Cytology
Otitis externa is a multifactorial disorder affecting the quality of life of 10% to 20% of dogs and 2% to 6% of cats presenting to veterinarians.1-3 Although a common problem, management of otitis externa is frequently challenging.
Seemingly simple cases can become complicated by treatment failure, recurrence, and progressively worsening physical changes. Successful management of otitis requires accurate identification and management of both the primary cause (e.g., atopy, adverse food reaction, parasites, neoplasia) and concurrent perpetuating factors (e.g., bacterial or yeast infection, edema, glandular hyperplasia, loss of epithelial migration, otitis media).In addition to a detailed history and physical examination, otic cytology should be considered part of the minimum database for all patients with clinical signs of ear disease. Cytology is a simple, practical, and inexpensive diagnostic test that provides rapid results indicating the presence and numbers of bacteria and yeast. Preparation of a diagnostic-quality slide does not require any special skills or equipment, and the slide can be quickly and easily evaluated during a standard office examination. The immediate result allows for rational decision making at the time of the initial consultation, prior to return of culture and sensitivity results 48 to 72 hours later.
The value of cytology exceeds simple identification of organisms. Cytology can characterize the severity of overgrowth or infection; also, in cases of mixed infection, cytology assists in evaluating the relative significance of each organism, strengthening interpretation of culture and sensitivity data. When performed routinely on each subsequent visit, cytology provides an accurate method for monitoring the patient’s response to therapy.
Observation of quality and odor of exudates found during physical examination provides practitioners with a rough guide regarding potential organisms present in the external canal.
Classically, dry, grainy, black discharge is most often associated with Otodectes cynotis infestations; waxy, brown exudates indicate Malassezied; and yellow discharge indicates bacterial infection. Unfortunately these observations are not consistent or reliable.5,6 Veterinarians should not make a diagnosis or select therapy based on past experience, physical character of discharge, or odor. Instead, decision making should be based on cytologic evidence established by careful microscopic evaluation. Failure to do so may result in misidentification of the most relevant pathogen and inappropriate selection of antimicrobial therapy. The consequence is often poor case management, prolongation of treatment, or even treatment failure and progression of disease. Cytology should be viewed as a routine diagnostic test for every patient with clinically significant ear disease.Technique
In order to obtain the best diagnostic slide, be prepared to collect the sample prior to introduction of any cleaning agent or other therapy. In most cases, material obtained from the deeper horizontal canal is more clinically relevant than material obtained from the superficial vertical canal.5,7 In well-behaved or anesthetized dogs, the ideal sample is obtained by inserting a cotton-tipped applicator through a disinfected otoscopic cone positioned beyond the junction of the vertical and horizontal canals. The cone shields the swab from contents of the vertical canal, which may contain numerous, irrelevant commensal organisms. Once in position, the swab is extended beyond the cone and pressure is applied laterally against the epithelium, collecting the exudates; the swab is then pulled back into the cone and removed from the canal. Unfortunately, with an awake patient, safely inserting a swab into a painful deep horizontal canal can be challenging at best. The presence of stenosis, inflammation, and voluminous exudate makes the exercise difficult and potentially dangerous if the patient moves suddenly or unpredictably.
Overaggressive insertion of the swab into the patient’s ear canal in an effort to obtain the deepest possible sample may result in further damage to irritated epithelium, or worse, in accidental perforation of the tympanic membrane. To obtain consistent samples in awake or painful patients, veterinarians should aim for the junction of the vertical and horizontal canals, where the cartilage bends at a 75-degree angle. If the veterinarian avoids straightening the canal, the bend should prevent the swab from advancing too deeply and damaging the tympanic membrane. Veterinarians who are gentle, cautious, and quick can safely obtain a diagnostic sample from the majority of patients. In patients anesthetized for ear flush, otoscopy, or other procedures, time should be taken to collect an ideal specimen properly from the deep horizontal canal or in some cases the tympanic cavity.Although cotton-tipped applicators appear to be soft and gentle, when applied with pressure to inflamed epithelium, the surface of the swab is actually quite abrasive and can traumatize fragile tissue. An alternative to the swab is a rounded ear curette. The curette can be placed within the disinfected otoscopic cone positioned in the deep horizontal canal; the curette is advanced beyond the cone and gently scraped along the epithelium, collecting the exudate within the curette head. However, if a neoplasia is suspected, exfoliative cytology is preferred. The best sample for cytologic evaluation of a mass or polyp can be obtained by using a more traumatic surgical curette, using the same method described previously.
A separate cytologic specimen should always be prepared from both the right and the left ear canals, even if the patient presents for unilateral disease. Separate evaluation allows for comparison between the diseased ear and the normal ear, as well as early recognition of bacterial or yeast overgrowth in the less obviously affected ear. In patients with bilateral disease, clinically relevant differences in bacteria and yeast are common when comparing the two sides.8,9 Without independent evaluation, documentation, or monitoring of each ear separately, veterinarians may fail to make appropriate management decisions.
In the case of otitis media, systemic therapy and bulla infusions of antibiotics should be directed at organisms colonizing the middle ear rather than the external canal. In one study, isolates from the tympanic cavity differed from isolates from the horizontal canal in 89.5% of cases.8 In the same study, the tympanic membrane appeared to be intact in 71.1% of the ears with proven otitis media. If otitis media is suspected and the tympanum appears to be intact, sample collection should be performed by myringotomy—the intentional perforation of the tympanic membrane with a sterile swab, needle, or catheter. Because organisms from the middle ear may be coated in mucus, which prevents adequate uptake of stain, cytology from the middle ear should always be accompanied by a sample for culture and sensitivity obtained at the same time. In the external canal, cytology has been shown to be more sensitive than culture and sensitivity5,10; but this is not always the case in samples collected from the tympanic cavity.8
Once the sample is collected, roll the swab or curette onto a clean glass slide, evenly distributing a thin layer of material (Figure 3-1). Label each slide to identify correctly which ear was sampled. Alternatively, using one slide with a frosted end, holding the frosted end toward oneself, roll the sample from the left ear on the left part of the slide and the sample from the right ear on the right part of the slide. The precise method for marking slides is less important than consistency. Because cerumen has high lipid content, briefly heat the slide with an open flame to fix the material to the glass. This precaution will prevent loss of valuable information into the stain solvent. Avoid overheating the slide; excess heat will distort cells and organisms. Stain selection is a matter of personal preference; however, the same stain should be used for all samples in order to gain familiarity and produce consistent and reliable results.
A modified Wright’s stain, such as Diff-Quik (Baxter Scientific Products, McGraw Park, Illinois) is recommended. Modified Wright’s stains are designed for evaluation of peripheral blood smears; therefore, leukocytes will retain easily recognized characteristics. Both gram-positive and gram-negative bacteria, as well as yeast, will appear blue or purple. Performing a gram stain is necessary to obtain this additional information, but extra staining is often an unnecessary and timeconsuming task. In general, morphologically coccoid bacteria found in the ear canal are gram-positive organisms (e.g., Staphylococcus, Streptococcus, and Enterococcus) and the majority of rod bacteria are gram-negative (e.g., Pseudomonas spp., Proteus spp., coliforms). Only Corynebacterium, a gram-positive coccobacillus, and less common organisms such as Actinomyces and Nocardia spp. and filamentous grampositive rod bacteria do not follow this rule.Following staining, allow the specimen to air dry prior to microscopic examination. If desired, the slide can be permanently preserved by placing a drop of slide-mounting medium onto the stained material, applying a coverslip, then allowing the glue to set. Archiving of otic cytology is not always necessary if a detailed description is written into the medical record.
Scan the slide at low magnification to locate an area of interest. Cerumen and ointment-based medications do not take up stain and are of little interest. Avoid areas of thick, deeply stained debris, as the confluence will make characterization of individual organisms and cells difficult. Select a field containing thinly spread cellular or keratin debris for closer evaluation. Because different areas of the slide may yield different results, evaluate several fields to be sure all clinically relevant findings are discovered.
The high-dry, 40? objective (400? magnification) is adequate for identification of leukocytes, red blood cells, cornified epithelium, and neoplastic cells.
Infectious organisms such as yeast and larger bacteria are also easily recognized. After examining several fields with the high-dry objective, switch to the high-magnification,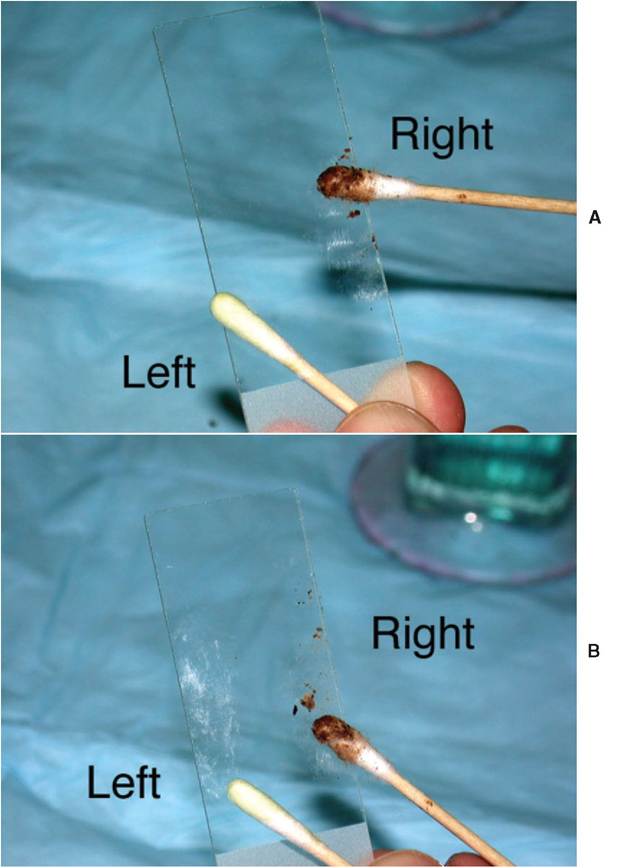
Figure 3-1
Technique for staining a cytologic specimen from the ear. A, Roll swab along glass slide. Swab with brown debris came from the right ear. Swab with purulent debris came from the left ear. B, Both specimens applied to the same slide, the right ear on the right side of the slide, the left ear on the left.
Continued
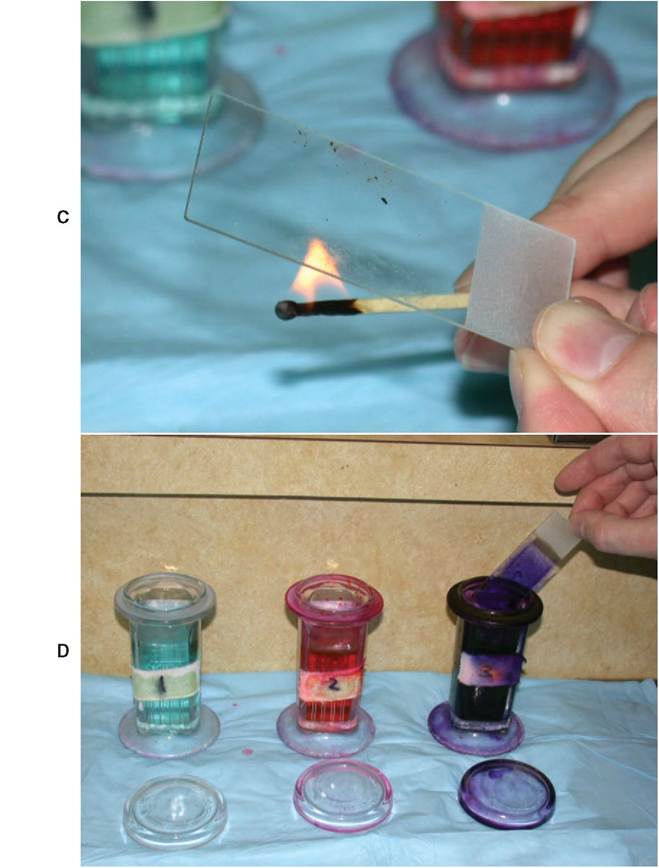
Figure 3-1—cont'd
C, Briefly heat-fix specimen to the slide. D, Stain with modified Wright's stain according to label instructions (Diff-Quik) shown.
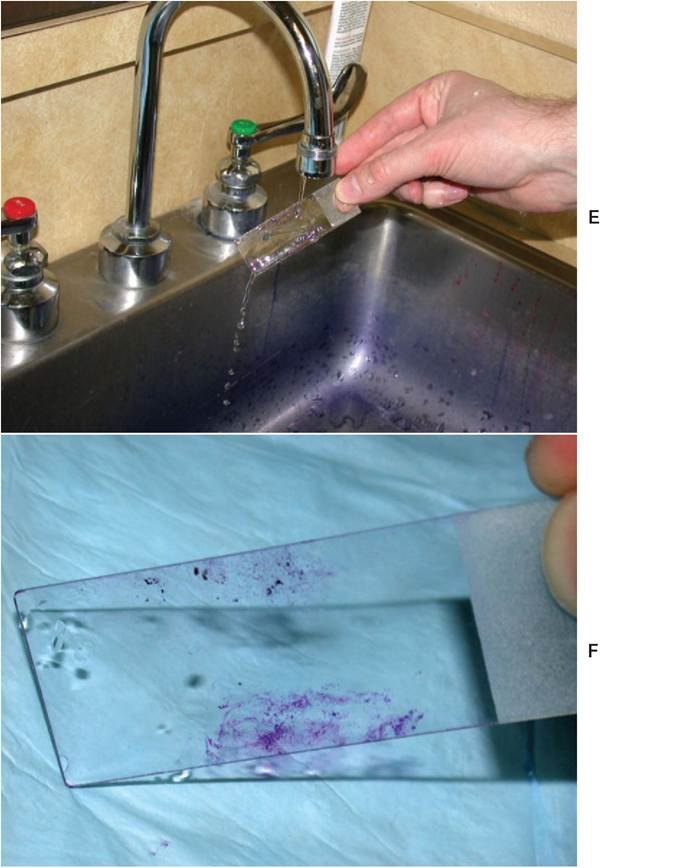
Figure 3-1—cont'd
E, Rinse slide by placing unstained side of slide under gentle water stream; this permits laminar flow of water to remove excess stain. F, Allow to air dry.
oil-immersion lens (100? objective, 1000? magnification) for detailed evaluation. The higher magnification is necessary to identify smaller or lightly stained bacteria that may be easily missed with the high-dry objective. The high-oil magnification also permits detailed evaluation of the cytoplasm of neutrophils and macrophages for phagocytized bacteria—another important indicator of that particular organism’s acting as a pathogen rather than a commensal.
In order to maintain consistency in cytologic evaluation, each specimen should be specifically evaluated for the presence, estimated number, and morphologic characteristics of three specific features: yeast, bacteria, and leukocytes. To estimate the numbers, evaluate five to 10 areas, and record the average count per high-powered field (Figure 3-2). A complete record of all three cytologic features is necessary to monitor progression of disease or response to therapy. Recording “bacterial otitis” alone does not supply sufficient information for later comparison. Each cytologic description should contain information regarding the morphologic characteristic of bacteria (cocci or rod), the presence or absence of Malassezia and leukocytes, whether bacteria were phagocytized by leukocytes, and a semiquantitative estimation of the relative numbers of each type of organism seen. This level of detail permits either the primary clinician or any colleague following the case to determine accurately whether the “bacterial otitis” is resolving, changing, or worsening.
In addition to bacteria, yeast, and leukocytes, veterinarians occasionally identify parasites such as Demodex or Otodectes cynotis on stained specimens prepared in this manner; however, this technique is unreliable for purposeful diagnostic evaluation for parasites. Instead, prepare a separate slide using a direct mineral-oil technique. Apply several drops of mineral oil to a clean glass slide. Collect a large quantity of otic exudate from any level of the canal with a clean cotton swab and transfer the debris to the mineral oil on the glass slide. Unlike stained cytology, debris from both ears can be pooled onto the same slide. Place a coverslip directly onto the mineral oil and examine the specimen with low magnification (4? or 10? objective). Examine the entire area defined by the margins of the coverslip, using a consistent back-and-forth sweep, similar to the technique used for fecal flotation specimens.
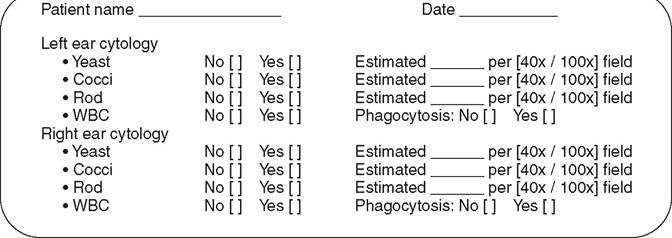
Figure 3-2
Suggested medical record insert for documenting cytologic findings.