Dermal and subcutaneous mesenchymal tumors
As previously mentioned, the dermis and subcutis contain supportive, connective tissues made up of resident mesenchymal/spindle cells and extracellular fibrillar and matrix materials.
These resident cells include fibrocytes/fibroblasts, adipocytes, endothelial cells, nerves, and muscle-associated cells, such as pericytes and myofibroblasts, which can be sites of tumor formation.Lipoma
Lipomas are one of the most common benign mesenchymal tumors in dogs and cats. Cytologic specimens of lipomatous masses are often grossly oily when material is prepared on a glass slide after FNA. They are also commonly acellular because the specimen can wash off during the staining process. When adipocytes from the lesion remain on the slide, they can appear individually and/or as small aggregates of cells with clear cytoplasm and large, clear vacuoles. The vacuoles cause marked distension of the cytoplasm and displace the small oval nucleus to the edge of the cell (Figure 4.40). Adipocytes from lipomas are cytologically identical to normal subcutaneous fat. Therefore, a diagnosis of lipoma can be supported by the clinical finding of a large, flocculent, subcutaneous mass coupled with the aforementioned FNA gross and cytologic findings.
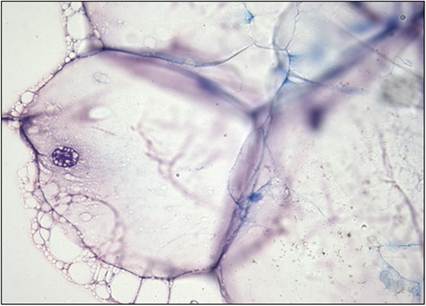
Figure 4.40 Aggregate of adipocytes in an FNA of a large, flocculent, subcutaneous mass from a dog. Cells are large and markedly distended by a single, clear, cytoplasmic vacuole. A small rounded vesicular nucleus can be seen in one of the cells (Wright–Giemsa stain, 500? magnification).
Soft tissue tumors
When spindle cells are present in increased numbers and display mild to marked atypia, there is increased concern for a spindle cell soft tissue tumor, particularly when there is an absence of inflammation (Masserdotti & Drigo, 2022).
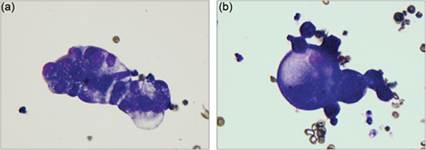
Soft tissue tumors comprise a heterogeneous population of neoplasms that range from benign to malignant and are often difficult to distinguish on cytology alone, requiring histopathology for grading (to predict biologic behavior) as well as immunohistochemical staining (for subclassification by tissue of origin and/or phenotype) (Avallone et al., 2007; Roccabianca et al., 2020).Examples of more benign soft tissue tumors (Figures 4.41a, b) include fibroma, myxoma, perivascular wall tumor, and some nerve-sheath tumors (i.e., neurofibroma). Some of these lesions have distinct cytologic features that may suggest the tumor type. For example, myxomas usually contain a thick, eosinophilic, proteinaceous matrix that entraps the spindle cells, which are a monomorphic population with relatively scant basophilic cytoplasm and a small oval nucleus (Figure 4.42); linear arrangements of cells in the specimen (windrowing) can also be seen due to the increased viscosity of the myxoid matrix. Cells from perivascular wall tumors and peripheral nerve sheath tumors often have very elongated, wispy cytoplasmic extensions, small and distinct cytoplasmic vacuoles, and a large oval nucleus (Figure 4.43a, b). Perivascular wall tumors can also contain multinucleate ‘crown’ cells (Figure 4.43b).
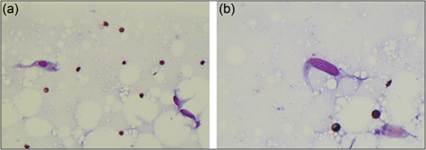
Figures 4.41a,b FNA of a subcutaneous mass on the sacrum from a 7-year-old Boxer. Small individualized mesenchymal cells are present with low numbers of erythrocytes in a thin basophilic proteinaceous background. Cells are small and spindle-shaped with light blue cytoplasm and a thin oval nucleus, most consistent with a benign mesenchymal tumor (Wright–Giemsa: a, 500? magnification; b, 1,000? magnification).
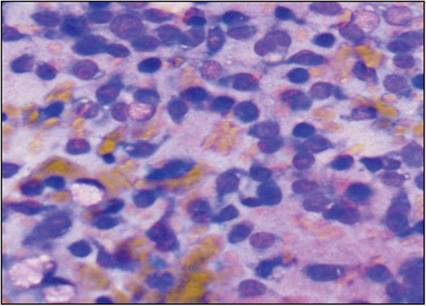
Figure 4.42 FNA of a subcutaneous mass on the right shoulder of an 11-year-old German Shorthaired Pointer.
Individualized spindle-shaped cells are entrapped in a thick eosinophilic proteinaceous extracellular matrix suggestive of a myxoma (Wright–Giemsa, 600? magnification).
Classically, we have considered lesions composed of abundant neoplastic spindle cells that display mild to moderate criteria of malignancy in the integument as ‘soft tissue sarcomas’ because most of them display similar biologic behavior (locally invasive with low to moderate recurrence rate and low metastatic rate); however, there is increasing evidence that differences in presentations and outcomes may exist among the different types of soft tissue sarcomas (Roccabianca et al., 2020).
Figures 4.43a,b FNAs of perivascular wall tumors. (a) Several wispy individualized mesenchymal cells are present. Cells have a moderate amount of lightly basophilic cytoplasm and an ovoid nucleus. Nuclei have dense chromatin. Small distinct cytoplasmic vacuoles are present in a few of the cells. Mild to moderate anisocytosis and anisokaryosis are observed (Wright–Giemsa, 1,000? magnification). (b) Multinucleate neoplastic cells have nuclei forming a ring around the periphery of the cell, consistent with ‘crown’ cells (Wright–Giemsa, 500? magnification).
Sarcomas
Cytology samples from sarcomas contain spindle cells with more significant criteria of malignancy (Figure 4.44). Examples of malignant spindle cell tumors that can occur in the subcutis include fibrosarcoma, myxosarcoma, liposarcoma, osteosarcoma, and hemangiosarcoma. These sarcoma subtypes have different biologic behaviors and can require different treatment strategies. As with the more benign spindle cell tumors, most sarcomas cannot be differentiated from one another cytologically, but sometimes distinctive characteristics are present that allow pathologists to provide a more specific provisional diagnosis, some of which are discussed below.
Histiocytic sarcoma is described with the round cell tumors. 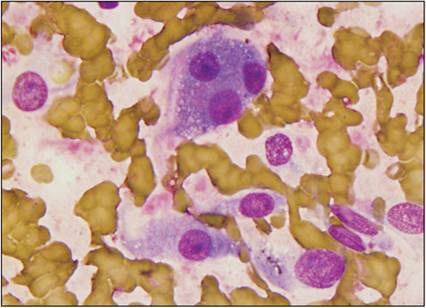
Figure 4.44 FNA of a subcutaneous mass on the hindlimb of a 9-year-old Labrador Retriever. There are moderate numbers of individualized spindle-shaped cells and moderate numbers of erythrocytes in a thin eosinophilic extracellular matrix. Cells have variable amounts of lightly basophilic cytoplasm and one or more large ovoid nuclei. Nuclei have stippled chromatin with one to two prominent nucleoli. A trinucleate cell is shown. Marked anisocytosis and anisokaryosis were noted. This sample is most suggestive of a sarcoma (Wright–Giemsa, 1,000? magnification).
Fibrosarcoma and myxosarcoma
Cytologic samples from fibrosarcomas have atypical mesenchymal cells frequently admixed with variably thick fibrillar pink matrix material (collagen) (Evans et al., 2018b). Occasional multinucleate tumor cells may also be seen. Keloid fibroma/fibrosarcoma is an uncommon variant in which the neoplastic cells occur in association with abundant amounts of eosinophilic, glassy, thick bands of hyalinized collagen (Raskin & Conrado, 2023; Figure 4.45). The myxoid variant of fibrosarcoma (myxosarcoma) can have similar thick proteinaceous background material and windrowing of cells as in myxomas (Figure 4.42). Samples from myxosarcomas contain large, spindle-shaped, mesenchymal cells with an oval nucleus and exhibit several characteristics of malignancy (Figures 4.46a, b). The myxoid matrix material is Alcian blue (pH 2.5) positive (Roccabianca et al., 2020).
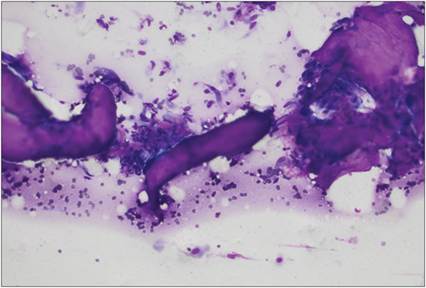
Figure 4.45 FNA of a mass near the hip of an adult dog. There are several individualized to aggregated spindle-shaped cells that display mild to moderate atypia and are often adhered to thick eosinophilic material (most consistent with keloid) (Wright–Giemsa, 500? magnification).
Figures 4.46a,b FNA from a subcutaneous mass on the third digit of the right hind foot of a 5-year-old Labrador Retriever. Several wispy individualized mesenchymal cells are associated with a thick eosinophilic extracellular matrix. Cells have a variable amount of lightly basophilic cytoplasm and an ovoid nucleus. Nuclei have stippled chromatin and one or more prominent nucleoli. Moderate anisocytosis and anisokaryosis are observed. A binucleate cell is present in 4.46a. The sample is most consistent with a myxosarcoma (Wright–Giemsa, 500? magnification).
Liposarcoma
Liposarcomas are rare tumors of adipose tissue that contain cells with deeply basophilic cytoplasm, clear (often punctate) lipid-filled vacuoles, a large ovoid nucleus, and many characteristics of malignancy (Figures 4.47a, b). Hibernoma (brown fat tumor) can have a similar appearance to liposarcoma and staining with UCP-1 may help discern these two entities (Piccione & Dial, 2020). Other cytologic differentials could include xanthoma, balloon cell melanoma, meibomian or sebaceous adenocarcinoma, clear cell carcinoma, rhabdomyoma/rhabdomyosarcoma, granular cell tumor, and oncocytoma (Piccione & Dial, 2020; Sebastian et al., 2021). Positive Oil-Red-O staining can be used to help confirm adipocyte/lipocyte origin (Masserdotti et al., 2006).
Figures 4.47a,b FNA of a mass on the right lumbar region of a 1-year-old dog, suggestive of liposarcoma. (a) Spindle-shaped cells are closely associated with clear, round spaces consistent with lipid vacuoles. Binucleate cells, anisocytosis, and anisokaryosis are observed. (b) Cells have abundant basophilic cytoplasm filled with small, distinct, clear vacuoles. Nuclei are large and ovoid with stippled chromatin. A large prominent nucleolus is seen in some of the cells (Wright–Giemsa: a, 500? magnification; b, 1,000? magnification).
Osteosarcoma
Osteosarcomas can occur as de novo extraskeletal tumors secondary to trauma, foreign body, injections, certain infections, idiopathic, as well as metastatic tumors. This tumor often exfoliates well and contains several anaplastic osteoblasts: large ovoid to spindle-shaped cells with abundant basophilic cytoplasm, an ovoid nucleus, and one to three prominent nucleoli. In the more oval-shaped cells, the nucleus is eccentrically located and a perinuclear clear zone may be visible, resembling plasma cells. Neoplastic cells sometimes contain small, angular, eosinophilic, cytoplasmic granules (Figure 4.48a). Less commonly, erythrophagocytosis is seen in the osteoblasts (Barger et al., 2012). Many criteria of malignancy can be seen, including multinucleation and mitotic figures. There may be osteoclasts present (large multinucleated cells with an eosinophilic hue to the cytoplasm; Figure 4.48b). Bright, smooth, eosinophilic extracellular matrix (e.g., osteoid) may also be seen (Figure 4.48c).
Depending on the degree of cellularity and atypia, it can sometimes be challenging to distinguish osteosarcoma from osteoma or heterotopic ossification, such as can occur with ossifying myositis or osseous metaplasia of another epithelial or mesenchymal neoplasm, necessitating biopsy for further characterization (Roccabianca et al., 2020). Alkaline phosphatase staining can be useful in the diagnosis of osteosarcoma on cytologic preparations, where it is highly sensitive and specific when expressed by atypical spindle cells; however, it does not discern between reactive and neoplastic osteoblasts and is rarely expressed by non-osteoblastic tumors (Barger et al., 2005; Ryseff & Bohn, 2012).
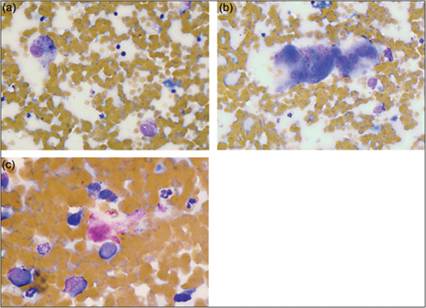
Figures 4.48a–c FNA of a subcutaneous mass on the left shoulder of an 8-year-old Rottweiler. (a) Two large osteoblasts are shown with abundant basophilic cytoplasm and an eccentrically located oval nucleus. Nuclei have stippled chromatin and a large prominent oval nucleolus. Cells contain several small irregular eosinophilic cytoplasmic granules. There is a moderate amount of blood in the background of the sample. (b) Two multinucleated osteoclasts are shown in a moderate amount of blood. (c) Bright eosinophilic extracellular material consistent with osteoid is often present in aspirates of osteosarcomas (Wright–Giemsa: a & b, 500? magnification; c, 1,000? magnification).
Hemangiosarcoma and lymphangiosarcoma
Hemangiosarcomas typically contain abundant blood with low numbers of very large, spindle-shaped, neoplastic, mesenchymal cells with an oval nucleus. The cells often contain small, distinct cytoplasmic vacuoles and may exhibit erythrophagia or contain blue–black pigment consistent with hemosiderin (Barger et al., 2012; Figures 4.49a, b). Some samples can have erythroid precursors and/or aggregates of blood leukocytes due to pooling in abnormal vasculature. Blood contamination of another sarcoma or hemangioma could appear similar cytologically. Lymphangiosarcoma is another rare neoplasm of the lymphatic vasculature that can occur anywhere on the body, but a common location is the ventral abdomen of cats. These lesions can have increased proportions of lymphocytes and atypical rounded to spindled cells (Azevedo et al., 2020). Endothelial cells should express CD31, while lymphatic cells can be distinguished using PROX-1 on immunocytochemistry (Roccabianca et al., 2020).
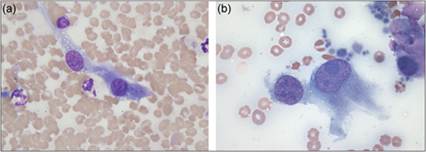
Figures 4.49a,b Hemangiosarcoma. FNAs of a subcutaneous mass on the prepuce of a dog. (a) Mesenchymal cells are large with abundant, spindle-shaped, basophilic cytoplasm and an oval nucleus with coarsely stippled chromatin. Small, distinct, clear cytoplasmic vacuoles and a prominent nucleolus are visible. Three neutrophils, a lymphocyte, and several erythrocytes are present in the background. (b) Marked characteristics of malignancy are observed within the mesenchymal cells in this sample. Anisocytosis, anisokaryosis, atypical nuclear shape, stippled chromatin, multiple prominent nucleoli, and variably sized nucleoli are shown. Erythrocytes, platelets, and a small amount of extracellular eosinophilic matrix (upper right) are present in the background (Wright–Giemsa, 1,000? magnification).
Injection-site sarcoma
More commonly reported in cats, but also rarely seen in dogs, are sarcomas secondary to injection or vaccination, often attributable to adjuvanted vaccines (such as rabies). The lesion is believed to arise from pluripotent mesenchymal stem cells, and histopathology commonly reveals fibrosarcoma but other sarcomas have also been documented (Roccabianca et al., 2020). Cytologic appearance, therefore, varies based on the type of sarcoma but contains atypical spindle cells with frequent multinucleation and rarely blue, blue–gray, or magenta adjuvant material. Current monitoring recommendations for injection-site sarcoma in cats involve the ‘3-2-1’ rule, whereby biopsy/excision of the lesion should be performed if a mass-lesion is present 3 months after injection, becomes >2-cm in diameter, or increases in size 1 month after injection (Hartmann et al., 2015).
Tumors of glandular structures
Sebaceous gland tumors
Neoplasia of the sebaceous gland can arise from germinative cells (basaloid reserve cells), sebocytes (sebaceous cells), or ductal cells. Tumors of the basaloid reserve cells include sebaceous epithelioma and epitheliomatous sebaceous carcinoma, and tumors of the sebocytes (and ductal cells) include nodular sebaceous hyperplasia, sebaceous (ductal) adenoma, and sebaceous carcinoma. Nodular sebaceous hyperplasia is the most common type of sebaceous tumor in dogs (Albanese, 2017; Mauldin & Peters-Kennedy, 2016).
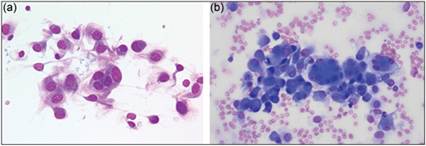
Lesions composed of sebaceous epithelial cells are usually benign in dogs and cats. Sebaceous hyperplasia and sebaceous adenomas appear cytologically similar. They contain cohesive clusters of round cells with abundant, highly vacuolated, basophilic cytoplasm and a small, centrally located, round nucleus with dense chromatin (Figure 4.50a, b). Sebaceous epithelial cells tend to be arranged in thick clumps, which create a kaleidoscope of vacuoles when the fine focus is adjusted on the microscope. Basaloid reserve cells may also be seen. These are small cells with small round nuclei and scant amounts of basophilic cytoplasm (Albanese, 2017). Sebaceous epitheliomas consist of a mixture of clusters of basaloid epithelial cells and scattered clusters of well-differentiated sebaceous epithelial cells (Figure 4.50b). Low numbers of well-differentiated squamous epithelial cells may also be seen (Raskin & Conrado, 2023). Sebaceous carcinomas are rare in dogs and cats and typically have several cytologic characteristics of malignancy.
Figures 4.50a,b (a) Sebaceous epithelial cells have abundant vacuolated cytoplasm and a small round nucleus with dense chromatin. Distinct basophilic cellular junctions are present (Wright–Giemsa, 1,000? magnification). (b) Sebaceous epithelioma with larger vacuolated sebaceous epithelial cells mixed with smaller, more basilar epithelial cells with scant cytoplasm (top and left) (Wright–Giemsa, 500? magnification).
Perianal gland tumors
Perianal gland tumors (also known as hepatoid gland or circumanal gland tumors) are common tumors in dogs, particularly intact males, and can be responsive to androgens. They originate from modified sebaceous gland epithelium within the dermis. These tumors can occur anywhere on the caudal half of the animal but are most frequently encountered around the tail and hindlimbs. Cytologically, tumor cells are present in clusters and resemble hepatocytes (hence the term hepatoid) with rounded, abundant, lightly basophilic cytoplasm that has an eosinophilic hue, and a round nucleus with a single prominent nucleolus (Figure 4.51a). Smaller numbers of epithelial cells with a high nuclear-to-cytoplasm ratio, scant cytoplasm, round nucleus with dense chromatin pattern (basal cell appearance, called reserve cells) are often closely associated with the clusters of perianal gland cells (Figures 4.51b, c). While increased numbers of reserve cells could be seen with perianal gland epitheliomas, the proportion of reserve cells does not appear to correlate with malignancy among perianal gland tumors (Evans et al., 2018a). Perianal gland adenocarcinomas are rarely reported and can appear well-differentiated to pleomorphic on cytology (McCourt et al., 2018). Therefore, histopathology is recommended to discern perianal gland hyperplasia and benign and malignant tumors (Goldschmidt & Hendrick, 2002). Due to androgen responsiveness, castration can help reduce perianal gland tumor size, potentially simplifying surgical removal.
Figures 4.51a–c FNA of a skin mass from the tail base of a dog. (a) Perianal gland tumor cells are large, uniform, hepatoid cells with abundant cytoplasm that is lightly basophilic and stippled with pale eosinophilic material. The nuclei are large with a single prominent nucleolus. The cell to the right of the image is binucleate. One free nucleus from a lysed cell is present to the far left of the image (Wright–Giemsa, 1,000? magnification). (b, c) Perianal gland tumor cells are closely associated with smaller reserve cells that have more rounded and condensed nuclei with scant cytoplasm (Wright–Giemsa, 500? magnification).
Apocrine gland tumors
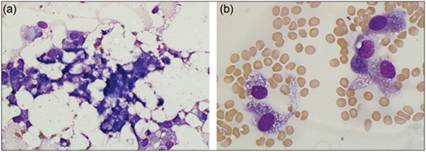
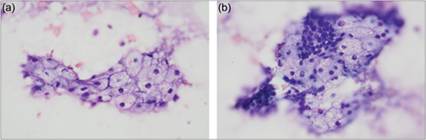
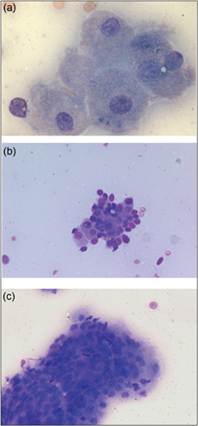
Apocrine gland anal sac adenocarcinoma (AGASACA) is an important aggressive, malignant tumor in dogs and rarely reported in cats. This tumor is often not detected until palpated during a rectal examination. It frequently metastasizes and can cause significant hypercalcemia due to the production of parathyroid hormone-related protein (Meuten et al., 1981; Rosol et al., 1990). On cytology, this tumor has a neuroendocrine appearance, characterized by numerous free nuclei within a lightly basophilic background of lysed cytoplasm (Figures 4.52a–c), which can be helpful in discerning an AGASACA from a perianal gland tumor; location of the mass is also very important in this distinction. Of note, AGASACA typically does not display significant criteria of malignancy on cytology despite its aggressive biologic behavior. Patients with suspected AGASACA should undergo staging, including abdominal ultrasound and evaluation of draining or enlarged lymph nodes, in addition to serum biochemical analysis for hypercalcemia (total and ionized, free calcium).

Figures 4.52a–c (a, b) FNA from a left anal gland mass of a 12-year-old Nova Scotia Duck Tolling Retriever. The sample contains large sheets of cells with indistinct cell junctions and a small round nucleus. Given the location of this mass, it is consistent with an adenocarcinoma of the apocrine gland of the anal sac. (b) Nuclei are arranged in small circles (acinar-like structures) in a few clusters of cells. (c) A second example of the sheets of cells that are observed in an apocrine gland tumor (Wright–Giemsa: a, 200? magnification; b & c, 500? magnification).
Apocrine tumors of the sweat gland can also occur elsewhere in the skin of dogs and cats (Conroy & Breen, 1972; Simko et al., 2003; Haziroglu et al., 2014). Apocrine gland adenomas are somewhat common in dogs but rare in cats, while apocrine gland carcinomas are relatively uncommon in both species. They can present as solitary, nodular lesions on the head, limbs, and abdomen. Adenocarcinomas are also rarely reported and less common sites include the clitoris, the vulva, and the eyelid in dogs (Hirai et al., 1997; Neihaus et al., 2010; Rout et al., 2016). Aspirates of apocrine gland tumors often contain clusters of columnar to cuboidal cells, occasionally with intracytoplasmic blue–gray secretory material, and sometimes basilar (ductal) cells. These lesions can have cystic portions (see ‘Apocrine cysts’).
Mammary masses
Mammary masses are common lesions in both the dog and the cat, particularly intact animals or those neutered later in life. Possible causes for mammary masses include cysts, inflammation/infection (i.e., mastitis), hyperplasia, and benign and malignant neoplasms. Cytology of mammary lesions can be challenging because they can have multiple components including cystic regions, inflammation, and neoplasia all in the same lesion, and even neoplastic lesions can contain both epithelial and mesenchymal elements (mixed tumors and carcinosarcomas). In addition, benign mammary epithelial neoplasia or hyperplasia may not be easily distinguished from carcinoma. In some cases, epithelial cells aspirated from malignant tumors/carcinomas may not have sufficient cytologic criteria of malignancy for an unequivocal cytologic diagnosis of malignancy. On the other hand, some tumors may display multiple criteria of malignancy in an FNA sample (appearing consistent with a carcinoma), and yet be diagnosed as benign tumors on histopathologic evaluation. Furthermore, aspirates from tumors with both epithelial and mesenchymal cells may not contain sufficient numbers of the different cell types for recognition of the mixed nature of the neoplasm. Cytology also cannot detect factors that are useful in histopathologic diagnosis of malignancy, such as invasion into lymphatic structures and enumeration of mitoses. Due to these factors, excisional biopsy and histopathologic evaluation are often recommended for mammary tumors where malignancy is suspected (such as feline mammary neoplasms or large masses). However, cytology of mammary lesions can be a good screening test to detect infection versus neoplasia or epithelial vs. mesenchymal vs. round cell tumor. Approximately 30–50% of canine mammary tumors and 80–90% of feline mammary tumors are malignant (Brodey et al., 1983; Goldschmidt et al., 2017; Seixas et al., 2011), and complete tumor removal with resection of the entire mammary chain and draining lymph nodes is indicated in many dogs and nearly all cats.
Canine mammary masses
Mammary gland tumors are the most common neoplasms diagnosed in intact female dogs (Dorn et al., 1968; Goldschmidt et al., 2017). Early ovariohysterectomy will reduce the chance of developing mammary neoplasia. Dogs spayed prior to their first estrus are much less likely to develop mammary neoplasia (0.5% chance during their lifetime), with an increasing chance of developing tumors in those dogs spayed after their first cycle (8% before the second estrus, and 26% before the third cycle, with no significant protective effect after the third cycle or after 4 years of age; Schneider et al., 1969; Sorenmo et al., 2020). Treatment with hormones also increases the risk of mammary gland tumor development, and treatment with low-dose progestins alone can result in an increased risk of benign tumors while combinations of estrogens and progestins have an increased risk of malignant tumors (Sorenmo et al., 2020). Mammary tumors are much less common in male dogs than in females (62 times more common in females), and mammary tumors in male dogs are usually benign lesions (Saba et al., 2007). Mammary tumors are most common in middle-aged or older dogs, with an increasing incidence from approximately 7 to 13 years of age (Sorenmo et al., 2020). Breeds with an increased risk of mammary tumors include Boxers, Poodles, Chihuahuas, Yorkshire Terriers, Maltese, English Springer Spaniels, Brittany Spaniels, English Setters, German Shepherds, Pointers, and Doberman Pinschers (Sorenmo et al., 2020).
Mammary gland tumors may arise from secretory or ductular cells, myoepithelial cells, or stromal cells. While cytology of mammary lesions has been previously reported to have good sensitivity, specificity, and correlation with histopathology, other studies have reported much lower diagnostic utility (Simon et al., 2009, Griffiths et al., 1984; Allen et al., 1986). Therefore, it is generally believed that in dogs, cytology cannot reliably distinguish between benign and malignant mammary neoplasia, and histopathology is still recommended if a mammary neoplasm is suspected. It can be useful, however, if mastitis or another neoplasm is occurring in the region of the mammary gland (i.e. round cell tumor).
Canine epithelial and complex mammary neoplasms
Tumors of the mammary gland may arise from epithelial (secretory or ductular) or myoepithelial cells. Epithelial cells can appear cuboidal, columnar, or rounded and may be present in clumps or forming papillary, trabecular, or even acinar-like arrangements (if glandular origin) on cytology (Allison & Walton, 2020). Myoepithelial cells can vary from rounded to cuboidal to more commonly spindled and should be differentiated from mesenchymal cells (Emanuelli et al., 2020). Cytologic criteria of malignancy (anisocytosis, anisokaryosis, prominent nucleoli, binucleation and multinucleation, and/or increased N:C ratio) may be utilized in the evaluation of epithelial cells from aspirates of mammary tumors (Figures 4.16a–c and 4.53–4.55a, b), but this can be problematic, as some malignant tumors lack significant criteria of malignancy for a definitive cytologic diagnosis of carcinoma, while some benign epithelial tumors may exhibit mild to moderate criteria of malignancy. The cytologic criteria of malignancy that have been statistically associated with mammary carcinoma include variable nuclear size (anisokaryosis), nuclear giant forms, high N:C ratio, variable or abnormally shaped nucleoli, and macronucleoli (Allen et al., 1986). Simple mammary tumors consist of neoplastic epithelial cells (either epithelial or myoepithelial), while complex tumors consist of both epithelial and myoepithelial cells. Benign mammary gland epithelial neoplasms in the dog include adenoma (simple and complex or adenomyoepithelioma), myoepithelioma, duct adenoma, and duct papilloma (intraductal papillary adenoma) (Sorenmo et al., 2020). Malignant mammary gland epithelial neoplasms are namely carcinomas, including simple, complex, squamous cell, among others.
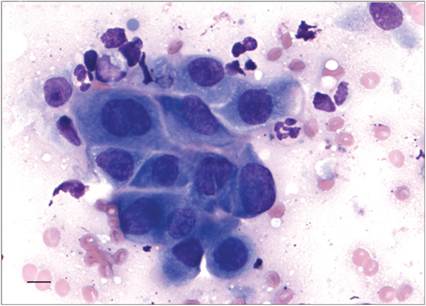
Figure 4.53 Epithelial cells from a mammary carcinoma in a dog. These are large, polygonal cells that exhibit several criteria of malignancy (anisocytosis, anisokaryosis, coarse chromatin, nucleoli, and binucleation with nuclear molding) (Wright–Giemsa, scale bar = 10 μm).
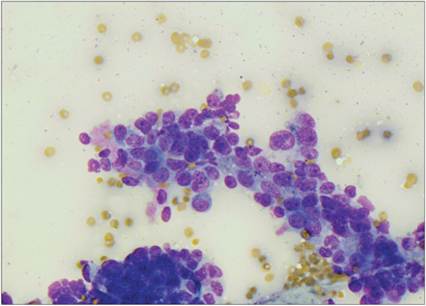
Figure 4.54 Small neoplastic epithelial cells from a 3 ? 5 cm firm fixed mass associated with the left fifth mammary gland of an intact female Miniature Poodle. The cells are densely clustered and have a high nuclear to cytoplasmic ratio, rounded nuclei, stippled chromatin, and a prominent nucleolus. Some irregularly shaped nuclei are noted. Moderate anisokaryosis is present. There is a small amount of eosinophilic extracellular matrix associated with the cells (Wright–Giemsa, 500? magnification).
Figures 4.55a,b FNA from a 2 ? 5 cm mass associated with the left fifth mammary gland of an intact female Golden Retriever. Poorly organized clusters of large, vacuolated epithelial cells with distended, deeply basophilic cytoplasm and a variably sized, round nucleus are seen. The sample is suspicious for a malignant mammary tumor (Wright–Giemsa, 1,000? magnification).
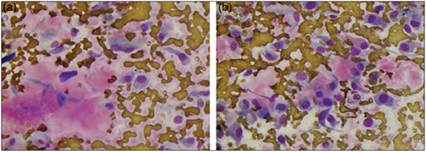
Canine mixed mammary tumors
Mixed mammary tumors exhibit proliferation of both epithelial and/or myoepithelial and stromal (mesenchymal) cells with usually cartilage and/or bone production (Im et al., 2014). Mixed tumors include benign mixed tumor and malignant mixed tumor (carcinosarcoma; Goldschmidt et al., 2011; Sorenmo et al., 2020). FNA cytology of mixed tumors will typically yield clumps of epithelial cells along with spindle cells, which may be associated with matrix material (Figures 4.56, 4.57a–d). Osteoclasts may be found in mixed tumors with bone formation or in mammary osteosarcomas (Figure 4.58).
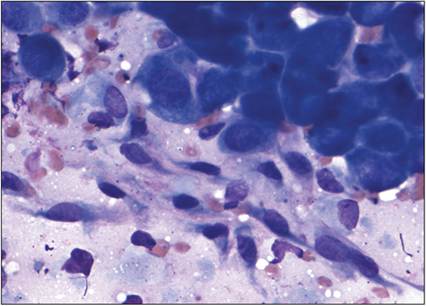
Figure 4.56 Epithelial cells and spindle cells from a mixed mammary tumor in a dog. The spindle cells are associated with pink matrix material. The epithelial cells exhibit several criteria of malignancy, including anisocytosis, anisokaryosis, prominent nucleoli, and coarse chromatin, concerning for a malignant lesion (Wright–Giemsa, scale bar = 10 μm).
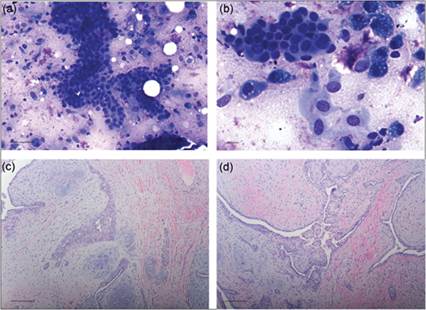
Figures 4.57a–d FNA (a, b) and biopsy (c, d) of a mammary mass in a 13-year-old, male Labrador Retriever. (a) The aspirates revealed numerous clumps of small epithelial cells with mild anisocytosis and anisokaryosis, along with a population of spindle cells and associated pink-staining matrix material (Wright–Giemsa, scale bar = 50 μm). (b) A higher magnification view of the FNA of the mass. This field includes epithelial cells, spindle cells, and foam cells (Wright–Giemsa, scale bar = 10 μm). (c, d) Histopathology of the mammary mass. Both epithelial and spindle cell elements are present as well as smooth, basophilic material, indicating production of cartilage within the lesion. The histologic diagnosis was benign mixed mammary tumor (H&E, scale bar = 100 μm).
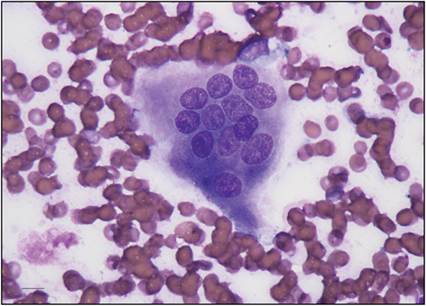
Figure 4.58 An osteoclast found in an aspirate of a mammary mass. Osteoclasts are large cells with multiple, uniformly sized nuclei and moderate to large amounts of basophilic cytoplasm with faint pink granulation. They may be found in tumors with osseous differentiation, such as mixed mammary tumors or osteosarcoma (Wright–Giemsa, scale bar = 10 μm).
Canine mammary gland sarcomas
Mesenchymal neoplasms of the canine mammary gland can include fibrosarcoma, osteosarcoma, chondrosarcoma, and hemangiosarcoma, with osteosarcoma being the most commonly diagnosed sarcoma (Goldschmidt et al., 2011; Sorenmo et al., 2020). Aspirates from these lesions will appear similar to these tumors in other tissues. These may sometimes be difficult to distinguish from mixed mammary tumors with FNA cytology, particularly in mixed mammary tumors where large numbers of epithelial cells are not aspirated.
Feline mammary lesions
Mammary gland tumors are less commonly encountered in cats than dogs and, similar to dogs, occur more frequently in intact females; however, unlike dogs, the majority of mammary tumors (85–95%) in cats are malignant (Hayes et al., 1981; Allen, 1973; Seixas et al., 2011). Mammary tumor risk has been reported to decrease by 91% if spayed before 6 months, by 86% between 7 and 12 months, and by 11% between 13 and 24 months, with no protective effect after 24 months (Sorenmo et al., 2020). Progestin use can also increase relative risk (overall 3.4, 5.3 for benign, and 2.8 for malignant tumors; Sorenmo et al., 2020). Mammary tumors are much less common in male cats than in females (Hayes et al., 1981; Viste et al., 2002). Mammary neoplasia is seen predominantly in middle-aged to older cats with a mean age at diagnosis of 10–12 years old (Zappuli et al., 2015). Epidemiologic studies have demonstrated an increased incidence of mammary carcinoma in the Siamese breed, with Siamese cats having twice the risk of developing carcinoma compared with other breeds (Hayes et al., 1981; Ito et al., 1996). There are too few studies comparing cytologic diagnosis of mammary tumors with histopathology results to discern the diagnostic utility of FNA in felines at this time.
Feline fibroadenomatous change
Fibroadenomatous change (feline mammary hypertrophy/fibroadenoma complex, feline fibroepithelial hypertrophy) is the most common cause of benign mammary tumors in cats (Allen et al., 1973). These hyperplastic lesions are the result of endogenous or exogenous progestin-induced proliferation of epithelial and stromal cells. Cats with fibroadenomatous hyperplasia have one or more enlarged (sometimes markedly enlarged) mammary glands. It is most common in young (up to 2 years old), intact, cycling queens or in pregnant cats (Rutteman & Misdorp, 1993). Neutered female cats with ovarian remnants can also develop fibroadenomatous change, and this condition has been documented in neutered female cats or in male cats that have been treated with progestins (megestrol acetate; Hayden et al., 1981; MacDougall, 2003). Fibroadenomatous change is a benign condition, and the masses will often regress spontaneously, after ovariohysterectomy, or termination of progestin treatment (Rutteman & Misdorp, 1993; Gimenez et al., 2010). If FNA cytology is performed on these lesions, findings should include clusters of uniformly sized, cuboidal epithelial cells, as well as a population of spindle-shaped stromal cells with associated pink-staining matrix (Solano-Gallego & Masserdotti, 2023).
Feline epithelial mammary neoplasms
Mammary epithelial neoplasms in the cat typically arise from epithelial cells with very rare proliferations of myoepithelial cells encountered. Benign neoplasms of the feline mammary gland are uncommon and could include adenoma, ductal adenoma, and duct papilloma (intraductal papillary adenoma) (Zappuli et al., 2020). The majority of feline mammary neoplasms are malignant and represent carcinomas of various histotypes, such as simple, solid, tubular, tubulopapillary, among others. Squamous cell carcinoma or carcinomas with squamous differentiation may also be found (Sorenmo et al., 2020). Considering the relatively high percentage of feline mammary neoplasms that are malignant, excisional biopsy and histopathologic evaluation are often recommended, even if the epithelial cells appear benign when examined by FNA cytology. Aspiration of regional lymph nodes to check for metastasis is recommended, as well as assessment of thoracic radiographs for metastatic lesions, because metastasis would indicate a shorter survival time (Ito et al., 1996; Seixas et al., 2011). Tumor size has been correlated with the prognosis of feline mammary neoplasms (Weijer & Hart, 1983; MacEwen et al., 1984; Ito et al., 1996). Cats with large tumors (>3 cm in diameter) were found to have a median survival time of approximately 6 months, while cats with tumors 2–3 cm in diameter had a median survival time of 2 years (MacEwen et al., 1984).
Feline mammary gland sarcomas
Mesenchymal neoplasms of the mammary gland are very rare, but the most common in the cat are fibrosarcoma and hemangiosarcoma (Zappuli et al., 2020). Again, these will appear cytologically similar to these tumors in other tissues.