Round cell tumors
Round cell tumors affecting dogs and cats include lymphoma, plasmacytoma, and mast cell tumor, while histiocytoma and transmissible venereal tumor only occur in dogs. Cats can, however, develop a distinct cutaneous histiocytic neoplasm known as feline progressive histiocytosis (described below).
Round cell tumors typically exfoliate well, are highly cellular, and can display distinctive cytologic characteristics that often allow for a definitive diagnosis to be made from an FNA. Immunocytochemical staining can be used to confirm the diagnosis or to reach a definitive diagnosis if classic cytologic characteristics of the tumor are not present (Fernandez et al., 2005).Lymphoma
Cutaneous lymphoma can appear as plaque-like or nodular lesions and often multiple lesions are noted. They contain a monomorphic population of small, intermediate, or large lymphocytes. When composed of large lymphocytes, a diagnosis of lymphoma can be made on cytologic evaluation. Large lymphocytes have variable amounts of basophilic cytoplasm, a nucleus larger than a neutrophil in diameter, and one or more prominent nucleoli. Intermediate-sized lymphocytes have nuclei that are approximately the size of a neutrophil with scant to modest amounts of basophilic cytoplasm and a round or irregular nucleus with open chromatin and variably prominent nucleoli (Figure 4.59). Small-cell lymphomas are composed of small lymphocytes with condensed chromatin and can be difficult to distinguish from lymphocytic inflammation. Histopathology is important in discerning epitheliotropic (neoplastic lymphocytes infiltrate the epidermis and/or adnexa) and nonepitheliotropic cutaneous lymphoma (neoplastic lymphocytes infiltrate the dermis and/or subcutis), in addition to determination of phenotype with IHC, PCR for antigen receptor rearrangement, and/or flow cytometry. Most cutaneous lymphomas are T-cell lymphomas (Day, 1995).
If a cutaneous lesion consists of mostly small to intermediate-sized lymphocytes, cutaneous lymphocytosis may be another consideration. This is a very rare lymphoproliferative disease more commonly reported in cats than dogs, and it is still unknown whether it represents a reactive or neoplastic disease but it does share clinical and histopathologic similarities to cutaneous lymphoma. Biopsy with IHC and clonality testing may be helpful in making this distinction (Albanese, 2022). 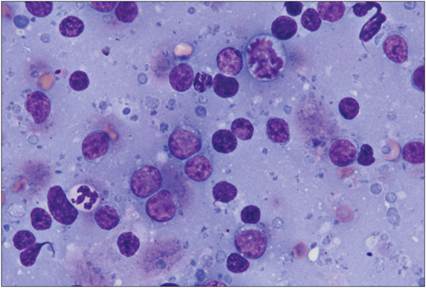
Figure 4.59 Cutaneous lymphoma. FNA of a dermal mass from a 10-year-old German Shepherd dog. The majority of the intact cells are intermediate to large lymphocytes, measuring approximately the same diameter as or slightly larger than a neutrophil. These cells have scant cytoplasm with more open chromatin and variably distinct nucleoli. There is a mitotic figure pictured (top off-center) and several lysed cells/bare nuclei and round basophilic cytoplasmic fragments. The size of the lymphoid population and homogeneity support a diagnosis of cutaneous lymphoma (Wright–Giemsa, 1,000? magnification).
Plasma cell tumor
Most cutaneous plasma cell tumors (plasmacytomas) of dogs and cats present as firm, raised dermal lesions and are benign neoplasms. FNA samples contain several round cells with abundant, basophilic cytoplasm, a perinuclear clearing in the area of the Golgi zone, and a round, eccentrically placed nucleus. Multinucleation (namely binucleation) is a common finding and a distinguishing characteristic of this tumor (Figure 4.60). Although rare, erythrophagocytosis has been reported in cases of plasmacytoma (Yearley et al., 2007). Malignant plasma cell tumors usually have several characteristics of malignancy. When multiple cutaneous plasma cell tumors are present, it may represent a more aggressive disease process (similar to multiple myeloma), and advanced diagnostics, such as serum and urine protein electrophoresis, assessment for lytic lesions, and bone marrow infiltration may be considered for staging (Moore A.R., 2023).
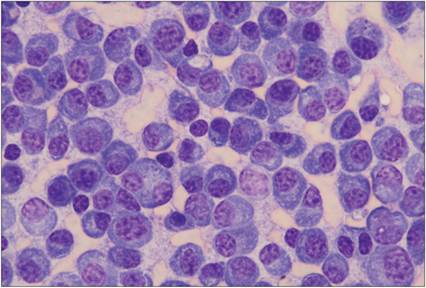
Figure 4.60 Plasma cell tumor. FNA of a dermal mass from a dog. The sample contains large numbers of individualized round cells and moderate numbers of erythrocytes. The round cells have a moderate amount of basophilic cytoplasm and frequently a pale perinuclear Golgi zone. They have an eccentrically placed rounded nucleus. A larger, binucleate cell is present (Wright–Giemsa, 500? magnification).
Mast cell tumor
The clinical appearance of mast cell tumors is variable. They can present as a firm, erythematous, cutaneous nodule, a deep, flocculent, subcutaneous mass, or anything in between. Mast cell tumors are composed of round cells with a rounded, centrally located nucleus that is often difficult to visualize because it is obscured by several small, distinct, metachromatic, cytoplasmic granules (Figure 4.61). Rarely, mast cells contain phagocytized erythrocytes (Barger et al., 2012). Eosinophils and/or large reactive fibroblasts may be present in large numbers and are more commonly observed in dogs compared with cats (Figure 4.61). In lesions with large numbers of fibroblasts, cords of extracellular eosinophilic matrix (collagen) are often observed.
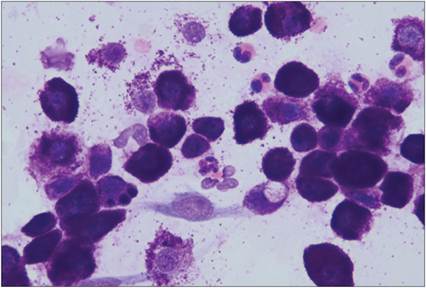
Figure 4.61 Mast cell tumor. Fenestration of a flocculent, subcutaneous mass from a dog. The sample contains large numbers of individualized round cells filled with numerous metachromatic, cytoplasmic granules. Anisocytosis is moderate. The nucleus is round, pale, and often obscured by the cytoplasmic granules. There are also a few eosinophils and reactive fibroblasts (Wright–Giemsa, 1,000? magnification).
The distinguishing feature of this tumor is the cytoplasmic granulation. However, mast cell granules do not always stain with Diff-Quik® stain, which may prevent diagnosis of the tumor (Figure 4.62).
A mast cell tumor should be suspected in lesions with large numbers of round cells that are associated with an eosinophilic infiltrate. Submission of an unstained slide to a diagnostic laboratory for Wright–Giemsa staining can confirm suspicion of a mast cell tumor. 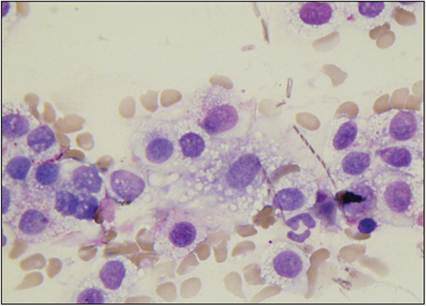
Figure 4.62 Mast cell tumor. FNA of a subcutaneous mass from a dog. There are several rounded cells with abundant cytoplasm and a centrally located round nucleus. Cells appear to contain vacuoles; however, a few metachromatic granules can be seen in some of the cells, allowing the diagnosis of a mast cell tumor to be made (Diff-Quik®, 1,000? magnification).
Histopathologic grading is regarded as the most consistent and reliable prognostic assessment in canine cutaneous mast cell tumors. Recently cytologic grading of Wright–Giemsa-stained slides has been attempted using some histologic criteria of malignancy. Cytologic findings associated with a poor outcome included poor granularity of the tumor cells or the presence of two or more atypical features, including anisokaryosis, mitotic figures, binucleation/multinucleation, nuclear pleomorphism, and reduced numbers of fibroblasts/collagen fibrils (Camus et al., 2016; Scarpa et al., 2016; Paes et al., 2022). Clinical stage is also important in assessing prognosis and can be achieved through cytologic evaluation of draining lymph nodes, spleen, and liver, although disease may be missed due to the small sample size of an FNA. Histopathologic evaluation of draining lymph nodes can also be assessed for a histologic node grade that has been shown to correlate with survival (Weishaar et al., 2014). Dogs with tumors affecting the prepuce, scrotum, and mucous membranes have been noted to experience a worse prognosis, while subcutaneous tumors seem to have a better prognosis (London & Thamm, 2020).
In cats, mast cell tumors often present as small, solitary, raised, white, hairless nodules.
If solitary, these are typically benign and complete surgical removal is curative. However, if multiple are present or there is suspicion of splenomegaly, evaluation of splenic mast cell neoplasia would be warranted as this would carry a worse prognosis (London & Thamm, 2020). Atypical cutaneous mast cell tumors have been reported in young cats histologic sections correlate with a poor prognosis (Strefezzi et al., 2003; Romansik et al., 2007; Elston et al., 2009; Sabattini & Bettini, 2010; Sabattini & Bettini, 2019).Histiocytic neoplasms
Histiocytoma
Histiocytoma is a common benign neoplasm of dogs. Tumors often are described as smooth, round, raised, mildly erythematous, cutaneous nodules with alopecia. Typically, the tumors spontaneously regress within a few months of diagnosis, although inflammation or infection can delay this. Surgical removal is recommended if the lesion persists to prevent progression to a malignant histiocytic neoplasm. These tumors are made up of Langerhans dendritic cells, which cytologically appear as round cells with lightly basophilic cytoplasm that becomes paler toward the edges of the cell. Nuclei are ovoid or bean-shaped and tend to be eccentrically placed with or without an indistinct nucleolus. Mitotic figures can be seen and there is a basophilic proteinaceous background. An infiltrate of small lymphocytes is seen as these tumors begin to regress and helps distinguish histiocytomas from plasma cell tumors or poorly granular mast cell tumors (Figures 4.63a, b). This infiltrate can become the predominant cell type and may complicate the diagnosis of histiocytoma.
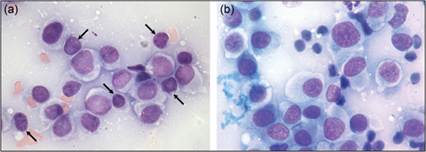
Figures 4.63a,b Histiocytoma. FNAs of hairless, raised, dermal lesions on the distal extremities from two dogs. The cells are individually arranged. They are rounded with abundant, lightly basophilic cytoplasm that becomes wispy and paler at the outer edge of the cell.
Cells have a large ovoid nucleus that is often eccentrically located and has a slightly open chromatin pattern. The samples also have a basophilic proteinaceous material and contain low numbers of erythrocytes. (a) Several small lymphocytes are present (arrows) (Wright–Giemsa, 1,000? magnification).
Cutaneous Langerhans cell histiocytosis
Cutaneous Langerhans cell histiocytosis is a rare condition of dogs (the Shar Pei breed is overrepresented) in which multiple cutaneous histiocytomas occur in the skin at the same site or at distant sites. It can also progress into a multisystemic disease involving the lymph nodes, lungs, and other internal organs. The cells are morphologically similar and have the same immunophenotype as those found in cutaneous histiocytoma (Sharma et al., 2021; Moore P.F., 2023). Animals present with multiple skin lesions that may respond to treatment with lomustine (CCNU), but they typically recur (Moore, 2014). The overall prognosis of these diseases is guarded due to lesion ulceration and recurrence. Immunocytochemistry can be used to help differentiate these lesions from cutaneous lymphomas.
Histiocytic sarcoma
Histiocytic sarcomas (HS) originate from neoplastic histiocytes (usually interstitial dendritic cells), and in the skin they occur within the dermis or subcutis. On cytology, the cells can be round and/or spindle-shaped, and marked atypia can be observed (Figures 4.64a, b). The cells have lightly basophilic cytoplasm, an ovoid to round nucleus which is often indented, and multiple, prominent nucleoli (Affolter & Moore, 2002; Albanese, 2017; Moore P.F., 2023). This tumor typically displays marked criteria of malignancy including frequent multinucleation and mitotic figures (Figures 4.64b). Phagocytized erythrocytes or cellular debris may be observed in the neoplastic cells (Barger et al., 2012). When spindle cells with marked cytologic atypia predominate in lesions, HS can appear similar to other high-grade sarcomas and undifferentiated pleomorphic sarcoma (also known as anaplastic sarcoma with giant cells, giant cell tumor of soft parts, and malignant fibrous histiocytoma), and immunophenotyping can be used to differentiate. Immunochemical identification of ionized calcium-binding adaptor molecule 1 (Iba1), lysozyme, vimentin, major histocompatibility (MHC) class II, CD11b, CD18, and CD204 expression by the neoplastic cells supports a diagnosis of histiocytic sarcoma (Yamazaki et al., 2014). Histiocytic sarcoma is the cause of death in approximately 14% of Bernese Mountain Dogs and Flat-Coated Retrievers (Erich et al., 2013). In cases of localized histiocytic sarcoma, cutaneous lesions on the limbs are frequently reported. Primary histiocytic sarcoma has also been reported in the spleen, lymph nodes, lungs, joints, and central nervous system.
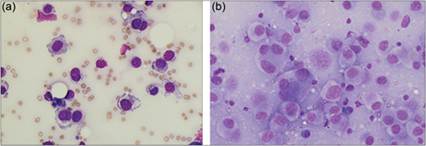
Figures 4.64a,b FNAs of histiocytic sarcomas. (a) FNA of a subcutaneous mass from a 12-year-old dog. Cells are rounded with abundant basophilic cytoplasm. Cytoplasmic vacuoles are observed. Nuclei are ovoid with coarsely stippled chromatin. Binucleate cells and anisokaryosis are noted. Multiple small, dark, prominent nucleoli are present in most of the cells (Wright–Giemsa, 500? magnification). (b) FNA of a mass on the right lateral thigh of a 9-year-old dog. Neoplastic cells display marked atypia including multinucleation, anisokaryosis, and karyomegaly (Wright–Giemsa, 500? magnification).
Feline progressive histiocytosis
In cats, there is a distinct entity of neoplastic dermal interstitial dendritic cells that can present as single or multiple cutaneous nodules and plaques, often found on the head or distal limbs. This can behave as a low-grade histiocytic sarcoma whereby lesions are typically slowly progressive and can spread systemically in the terminal stage (Affolter & Moore, 2006; Moore, 2014; Moore P.F., 2023). Cells have a histiocytic appearance with abundant lightly basophilic cytoplasm and an ovoid nucleus with stippled chromatin and are admixed with small T lymphocytes and neutrophils (Pinto da Cunha et al., 2014); cellular pleomorphism can increase with disease progression. Immunocytochemistry with CD1 is used in the diagnosis of this disease.
Transmissible venereal tumor
Transmissible venereal tumors (TVTs) are common in dogs from tropical and subtropical areas of the world. Cells that make up these tumors are canine-derived cells that have an aberrant number of chromosomes and contain a long interspersed nuclear element insertion near the oncogene c-myc (Murgia et al., 2006). The neoplastic disease can spread from affected to unaffected animals and is often observed around the genitals and muzzle. TVTs may become large, but they regress if there is an effective humoral immune response to the neoplastic cells (Goldschmidt & Hendrick, 2002). TVT cytology samples contain round cells that have moderate to abundant, lightly basophilic cytoplasm and a round, centrally located nucleus. Punctate, round, clear, distinct cytoplasmic vacuoles are the distinguishing feature of this tumor (Figure 4.65). A lymphocyte infiltrate (typically small lymphocytes) may also be seen and is reflective of an immune response to the tumor cells.
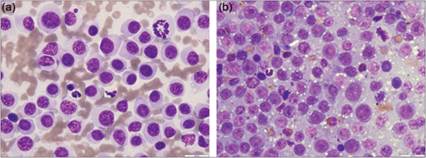
Figures 4.65a,b Transmissible venereal tumors. (a) FNA of a vaginal mass from a dog. The sample is highly cellular and consists of nucleated cells present in a bloody background. There are numerous individually occurring round cells with distinct cell borders and scant to moderate amounts of light basophilic cytoplasm. Low numbers of cells contain a few small distinct intracytoplasmic vacuoles. The nuclei are round and have a smooth to reticular to coarse chromatin pattern. Moderate anisocytosis and anisokaryosis are noted. A few neutrophils and small lymphocytes and occasional mitotic figures are also seen (Wright–Giemsa, 1,000? magnification). (b) FNA of a preputial mass from a dog. The sample is highly cellular and consists of nucleated cells present in a vacuolated background containing low numbers of red blood cells. There are high numbers of individually occurring round cells with distinct cell borders and scant to moderate amounts of light basophilic cytoplasm, often containing low numbers of small distinct intracytoplasmic vacuoles. The nuclei are round, have a reticular to coarse chromatin pattern and a single distinct nucleolus. Moderate anisocytosis and anisokaryosis are noted. A few neutrophils and small lymphocytes and occasional mitotic figures are also seen (Wright–Giemsa, 1,000? magnification).