Lymphocytic and lymphoplasmacytic inflammation
Often, lymphocytic inflammation is more regional and patchy within the liver; this has a negative effect on the sensitivity of FNA for lymphocytic inflammation. As in other locations, lymphocytic and lymphoplasmacytic inflammation is usually associated with an adaptive immune response and a more chronic duration (Figures 9.30a–c).
When chronic active hepatitis progresses to cirrhosis in the dog, FNA samples have decreasing amounts of lymphocytes and increasing amounts of biliary epithelial cells (Stockhaus et al., 2004). This finding fits with the expected resolution of inflammation and progression to fibrosis and hepatocyte drop-out. Care should be taken to avoid misdiagnosing lymphocytic inflammation with lymphoma (Otte et al., 2017). 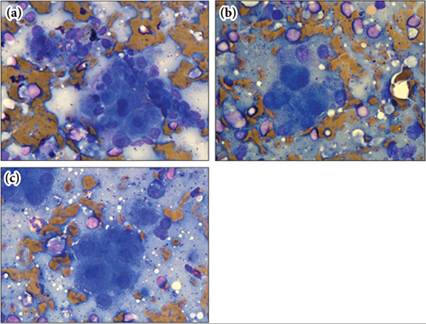
Figures 9.30a–c Nine-year-old Terrier-cross dog with a 6-month history of weight loss and recently elevated liver enzyme activity. (a) Clusters of hepatocytes and biliary epithelial cells are present. Mild anisocytosis and a single binucleate hepatocyte is present. There is a mixed lymphoid population with small lymphocytes predominant. Pigment consistent with ultrasound gel and hemosiderin is present. (b) Note the large number of mixed lymphoid cells surrounding, but not within, the hepatocyte cluster. (c) Mild anisocytosis is present in this cluster, which is surrounded by a mixed lymphoid population. A single plasma cell (upper right corner) and eosinophil (upper left corner) are found; both cell types were only rarely present throughout the slides. The cytologic interpretation for this sample was presumptive lymphocytic inflammation. Biopsy to confirm chronic active hepatitis and rule out lymphoma was recommended (Wright–Giemsa, 1,000? magnification). Clinically, the patient responded well to initial medical management and was lost to follow-up. (Same dog as in Figure 9.19.)