Lymphoreticular Tumors
Large Granular Lymphocytic (LGL) Leukemia
This signature neoplasm occurs in Fischer 344, Wistar, and Wistar-Furth rats. It is a major cause of death in aging F344 rats. Neoplastic cells arise in the spleen and then spread to other organs.
Although once considered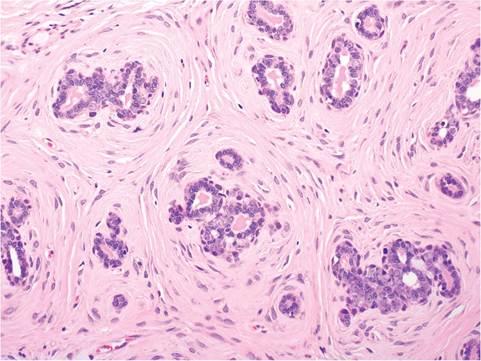
FIG. 2.83. Mammary fibroadenoma, demonstrating the relatively
well-differentiated epithelial cells lining acini and the prominent periacinar collagenous tissue.
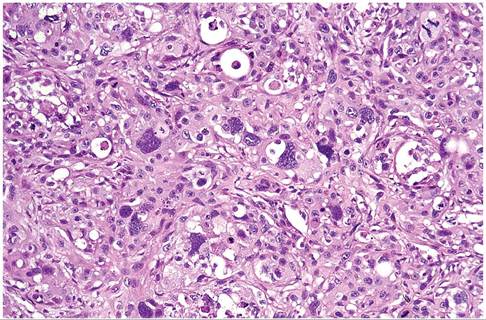
FIG. 2.84. Anaplastic mammary adenocarcinoma in an adult female rat. The neoplasm features anaplastic epithelial cells.
to be of natural killer (NK) cell origin, studies of cytotoxic activity and surface antigens suggest that these leukemias are of a heterogeneous lymphocytic cell origin. Clinical signs are characterized by weight loss, anemia, jaundice, and depression. LGL leukemia may be associated with elevated blood leukocyte counts of up to 400,000/ml3. Morphologically, leukemic cells resemble large granular lymphocytes. The spleen is typically enlarged, and there may be moderate to marked enlargement of the liver (Fig. 2.85) and lymphadenopathy. Petechial hemorrhages are frequently present on the lung and lymph nodes. Stained impression smears of tissues such as spleen reveal LGL cells that are 10-15 μm in diameter, with irregular-shaped, frequently indented nuclei, pale cytoplasm, and azurophilic cytoplasmic granules (Fig. 2.86). On histological examination of tissue sections, there is diffuse infiltration with LGL cells in spleen, lymph nodes, liver, and lung. There is

FIG. 2.85.
Abdominal viscera from a Fischer 344 rat with large granular lymphocyte (LGL) leukemia. There is marked splenomegaly and hepatomegaly. (Source: T.R. Schoeb, University of Alabama, Tuscaloosa, Alabama. Reproduced with permission from T.R. Schoeb.)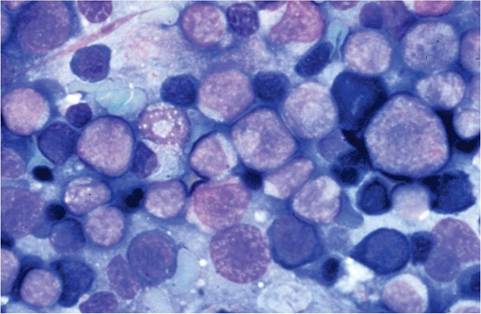
FIG. 2.86. Impression smear of spleen from a case of LGL leukemia. There are large numbers of neoplastic lymphocytes intermixed with hematopoietic elements.
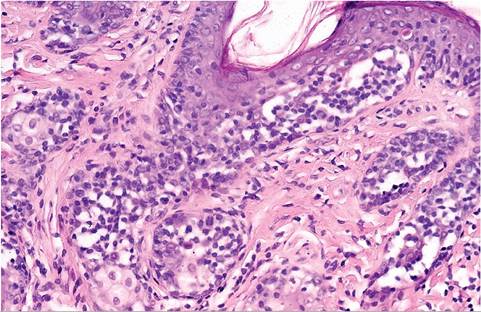
FIG. 2.88. Skin from an adult rat with epitheliotropic lymphoma. Note the infiltrate of relatively well-differentiated lymphocytes at the dermoepidermal junction.
frequently marked depletion of lymphoid follicles in the spleen and diffuse infiltration of leukemic cells in the sinusoids. Hepatocellular degeneration commonly occurs, probably a result of the concurrent anemia and neoplastic infiltrates. Erythrophagocytosis may be evident in the liver and spleen. There is usually a concurrent, immune-mediated hemolytic anemia, with thrombocytopenia and clotting abnormalities suggestive of disseminated intravascular coagulation.