Neoplasia
The presence of oral masses is one of the most common reasons for cytologic examination of the oral cavity. Oral neoplasia accounts for approximately 5% of all canine neoplasms and approximately 6–10% of all feline cancers (Munday et al., 2016).
Many are discovered when a patient is presented for reluctance to eat, excessive salivation, or periodontal disease. A review of oral masses revealed that while they grossly appear similar to neoplasms, many of the mass-like oral lesions in both dogs and cats were hyperplasic and/or inflammatory, demonstrating that microscopy and/or advanced diagnostics are needed for characterization and that a presumption of neoplasia is inappropriate in the absence of other supporting signs (Mikiewicz et al., 2019; Wingo 2018). Cytologic correlation with histologic diagnosis of oral neoplasms is high (Bonfanti et al., 2015). While many types of neoplasia can occur in the oral cavity, some of the most common and/or unique are described below. As with any location, in lesions with evidence for concurrent inflammation, dysplastic change induced by the presence of inflammatory cytokines should not be confused with neoplastic change.Melanoma
Melanoma is the most common malignant oral tumor of the dog, and melanocytic neoplasms comprise 30–40% of all canine oral tumors (Liptak, 2020; Smedley et al., 2022). The neoplastic cells are of neural crest origin and, as such, can have a pleomorphic appearance, exhibiting morphologic features of both epithelial and mesenchymal cells. These cells are readily identifiable when they are heavily pigmented and contain abundant green–black, seed-shaped, intracytoplasmic melanin granules. However, in poorly differentiated, amelanotic melanomas, these neoplasms can be misidentified easily. Nuclei are typically round to ovoid and often contain two similarly sized round nucleoli, giving the nucleus the appearance of a ‘pig’s nose’ or an ‘owl’s eye’ (Figures 6.18, 6.19, 6.20).
Immunostaining with immunocytochemistry using antibodies against cytokeratin, vimentin, and Melan A protein or immunohistochemistry with a panel of antibodies containing Melan-A, PNL-2, TRP-1, and TRP-2 may be helpful in identifying these neoplasms but may be cost prohibitive ( Przeździecki et al., 2015; Smedley et al., 2022). Although not all melanomas are malignant, those associated with the oral cavity are often biologically aggressive with frequent metastasis to the regional lymph nodes and lungs and with a metastatic rate dependent on site, size, and clinical stage (Liptak, 2020). Histologic examination of architecture is advised for prognostication (Smedley et al., 2022). 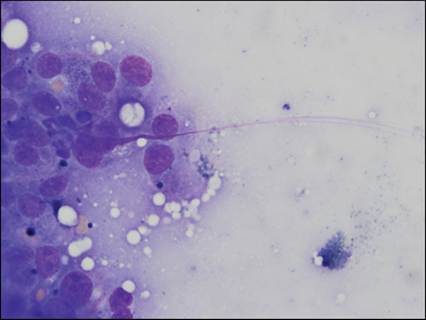
Figure 6.18 Oral mass from a dog. Melanoma. Multiple nuclei contain two prominent nucleoli, giving the appearance of a ‘pig’s nose. Low numbers of cells contain a faint black pigment dusting, and occasional aggregates of extracellular melanin granules are present. Cytoplasmic streaming from a disrupted nucleus is shown (modified Wright’s, 1,000? magnification).
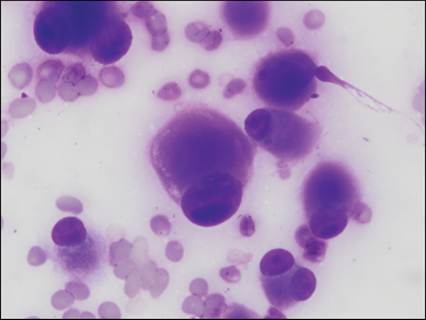
Figure 6.19 Oral mass from a dog. Amelanotic melanoma, confirmed with histopathology. Individualized round cells have an abundant amount of magenta-colored cytoplasm, which often stains lighter toward the periphery. Nuclei are ovoid and peripherally located typically with a single, prominent, deeply basophilic nucleolus. Two binucleated cells are seen. Anisocytosis and anisokaryosis are moderate to marked. No overt melanin granules are observed (Diff-Quik®, 1,000? magnification).
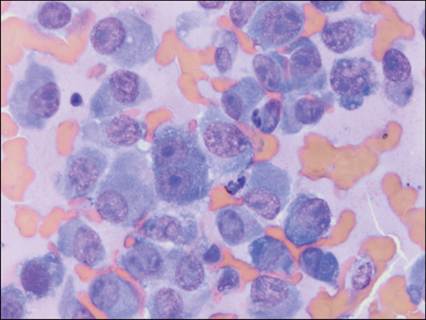
Figure 6.20 Oral mass from a dog. Amelanotic melanoma. Individualized spindle-shaped cells with moderate amounts of basophilic cytoplasm, that occasionally contains punctate vacuoles.
Nuclei are round to ovoid with coarse chromatin and often one or more prominent, deeply basophilic nucleoli. A binculeated cell resembling ‘eyes’ is noted centrally. No overt melanin granules are observed (modified Wright’s, 1,000x magnification).
Squamous cell carcinoma
Squamous cell carcinoma (SCC) is the second most common oral neoplasm in dogs and the most common oral cancer in cats, where it often occurs in the frenulum of the tongue (Andreasen et al., 2016; Liptak, 2020). Squamous epithelial cells are present throughout the oral cavity, as they cover most surfaces in the mouth, including the tonsil. Neoplastic squamous cells typically exhibit numerous criteria of malignancy. An increased N:C ratio can be difficult to detect, as ‘normal’ squamous epithelial cells typically contain an abundant amount of cytoplasm relative to nuclear size. As squamous cells mature, they lose their nucleus in conjunction with the keratinization process. Fully keratinized squamous cells stain bright blue with Romanowsky stain and the presence of a nucleus in a keratinized cell is indicative of nuclear to cytoplasmic maturation asynchrony, which is often associated with a neoplastic process. Additionally, neoplastic squamous cells often contain numerous distinct, nonstaining vacuoles, which occasionally aggregate, forming a ‘beard’ around the nucleus with an aggregate of vacuoles on one nuclear pole. Bizarre cell shapes, including round, angular, and ‘tadpole-shaped’ cells, are noted commonly (Figures 6.21–6.24). The cytologic diagnosis of neoplasia can be complicated by the fact that intralesional keratin often incites a marked neutrophilic inflammatory response, which might be interpreted erroneously as inciting dysplastic rather than neoplastic change in the epithelial population (Figure 6.25).The prognosis in dogs with SCC varies, depending on type and location. Subtypes of non-tonsillar SCC have been developed in dogs, based on the World Health Organization (WHO) classification system, with a suggestion that the papillary subtype has a lower rate of distant metastasis and, therefore, a more favorable prognosis, than other types of non-tonsillar oral SCC (Thaiwong et al., 2017).
Tonsillar tumors and lesions at the base of the tongue carry a worse prognosis than SCCs at other oral locations.The prognosis in cats with SCC is poor, due to the aggressive nature of local lesions and the metastatic potential (Liptak, 2020). Tonsillar SCC are reportedly 10 times more common in animals living in cities versus in rural areas, implying that environmental pollutants may play a role in tumor development (Reif & Cohen, 1971). 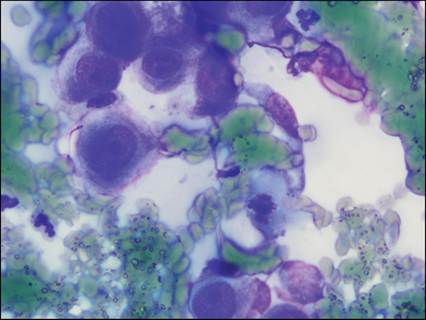
Figure 6.21 Mass at the base of a mandibular canine tooth from a dog. Squamous cell carcinoma. Individualized round to polygonal cells with a high N:C ratio. Nuclei are round to ovoid with coarsely clumped chromatin and one or more prominent nucleoli. Cytoplasm is deeply basophilic, consistent with keratinization. One mitotic figure is present. Anisocytosis and anisokaryosis are moderate (Diff-Quik®, 1,000? magnification).
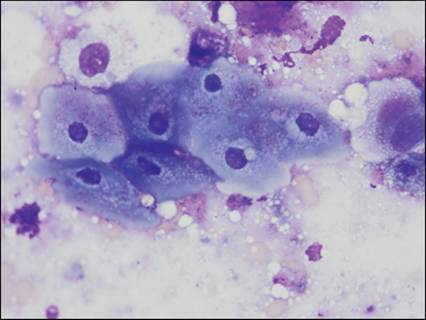
Figure 6.22 Mass on the zygomatic arch of a dog. Squamous cell carcinoma. Cohesive angular squamous epithelial cells exhibiting nuclear to cytoplasmic asynchrony, as keratinized cells should be anucleate. Aggregates of variably sized, nonstaining vacuoles surround the nucleus, forming a nuclear ‘beard’ (modified Wright’s, 1,000? magnification).
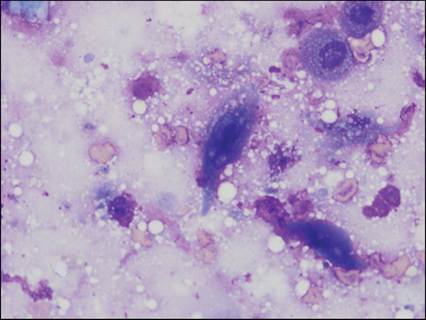
Figure 6.23 Oral mass from a dog. Squamous cell carcinoma. Individualized round to angular squamous epithelial cells exhibiting nuclear to cytoplasmic asynchrony are noted. The cell in the middle of the image tapers at one end, morphologically resembling a ‘tadpole’ (modified Wright’s, 1,000? magnification).
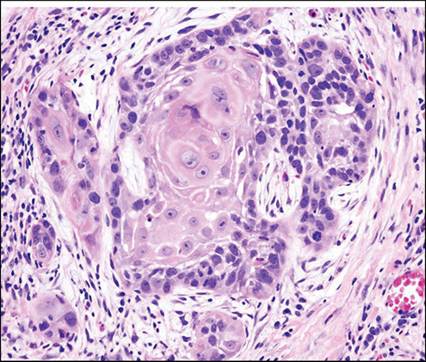
Figure 6.24 Histologic section of an oral mass from a cat.
Squamous cell carcinoma. Nests of pleomorphic squamous epithelial cells (keratin pearls) are surrounded by more basilar epithelium, adipose tissue, and fibrovascular stroma (H&E, 400? magnification).
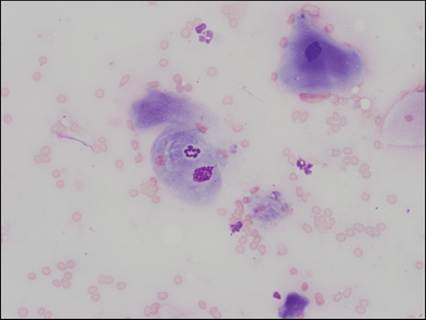
Figure 6.25 Digital mass from a cat. Squamous cell carcinoma. Squamous epithelial cells with blood and poorly preserved neutrophils. Either on or within (emperipolesis) the central squamous epithelial cell is a nondegenerate neutrophil (modified Wright’s, 500? magnification).
Fibrosarcoma
Oral fibrosarcoma is the third most common oral tumor of the dog and the second most common oral tumor of the cat (Liptak, 2020). This neoplasm often appears on the hard palate and, like other mesenchymal tumors, often exfoliates poorly, resulting in minimally cellular cytologic specimens. Therefore, a biopsy is often needed for diagnosis. When cells are present for evaluation, they typically have wispy cytoplasm with indistinct cellular borders, making assessment of anisocytosis and N:C ratio difficult. Nuclei are often ovoid with a coarse, open, chromatin pattern. There is a subset of oral fibrosarcomas with relatively benign looking morphology, exhibiting few criteria of malignancy, which are shown to be very biologically aggressive, with aggressive local invasion and a 30% metastatic rate (Cieckot et al., 1994; Munday et al., 2016). Therefore, even with minimal criteria of malignancy, there is suspicion for an aggressive lesion with the presence of proliferative mesenchymal cells (Figure 6.26).
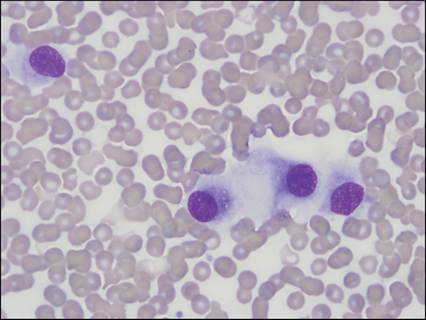
Figure 6.26 Mass on thorax of a dog. Fibrosarcoma. A poorly exfoliating neoplasm with a large amount of blood. Individual cells have wispy, indistinct, basophilic cytoplasm. Nuclei are round to ovoid with a coarse chromatin pattern and indistinct nucleoli (modified Wright’s, 1,000? magnification).
Lesions formerly known as epulides
Epulis (plural = epulides) is a nonspecific term used to refer to a growth of the gingiva. Epulides cannot readily be distinguished cytologically from gingival hyperplasia (Munday et al., 2016; Gelberg, 2021). Historically, at least four types of epulides (acanthomatous, fibromatous, giant cell, ossifying) were recognized; some of these lesions contain inflammatory cells and/or osteoclasts, making interpretation difficult (Figure 6.27). Classification of these tumors has been simplified. Lesions formerly classified as acanthomatous epulides, which arise from the remnants of dental lamina in the gingiva (rests of Serres), are now termed acanthomatous ameloblastomas whereas all other subtypes are termed peripheral odontogenic fibromas (Wingo, 2018; Liptak, 2020). Bone in peripheral odontogenic fibromas is consistent with osseous metaplasia, eliminating the need for the term ‘ossifying epulis’ (Munday et al., 2016). As squamous epithelial cells cover the mesenchymal gingiva, cells of mixed morphology are often noted in these lesions (Figure 6.28). Histologic examination of architecture is needed to characterize and further classify these lesions. While most exhibit benign biological behavior, acanthomatous ameloblastomas are often locally aggressive and invade the underlying bone of the maxilla or mandible. There is no report of distant metastasis, often allowing for management with aggressive local therapy (Liptak, 2013).
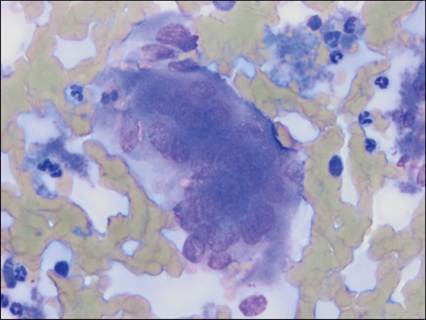
Figure 6.27 Hard palate mass from a dog. There is a single, large multinucleated cell, morphologically compatible with an osteoclast.
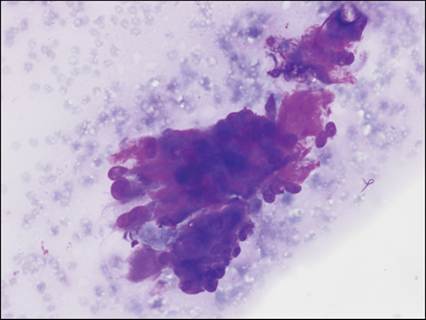
Figure 6.28 Gum mass from a dog. Peripheral odontogenic fibroma (formerly fibromatous epulis). Clusters of uniform, tightly cohesive, round-shaped epithelial cells with high N:C ratios and indistinct cell borders. Abundant brightly eosinophilic matrix material surrounds more pleomorphic, wispy, mesenchymal cells (modified Wright’s, 500? magnification).
Viral papillomatosis
Lesions associated with viral papillomatosis are horizontally transmitted between dogs and are caused by the DNA virus canine papillomavirus (CPV)-1 (Newkirk et al., 2021; Liptak, 2020). Multiple viral-associated masses often arise on the tongue, lips, or oropharynx and exhibit a verrucous appearance (Figure 6.29). They occur most commonly in young dogs (less than 1 year old) and typically regress spontaneously within 1–2 months, although spread to other bodily locations, including the esophagus and haired skin, can occur (Higgins et al., 2001; Munday et al, 2016). These lesions are composed superficially of various stages of squamous epithelial cells overlying a mesenchymal (stromal) core, resulting in heterogeneous aspirates (Figure 6.30). Cytoplasmic viral inclusions can be seen occasionally. Papillomavirus-induced lesions in cats are rare, although sublingual masses in cats have been associated with the presence of Felis catus papillomavirus 1 (FcaPV-1) DNA (Munday, 2015a,b).

Figure 6.29 Canine viral papillomatosis. Numerous verrucous masses covering the tongue, the lips, the labial tissue, and the hard palate (courtesy Dr. David Driemeier).
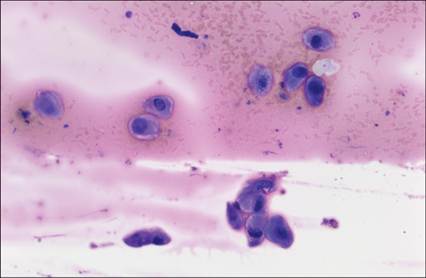
Figure 6.30 Toe mass from a dog. Canine papillomatosis. Aggregates of variably sized round to angular squamous epithelial cells with variable N:C ratios embedded in a brightly eosinophilic extracellular material (modified Wright’s, 100? magnification) (courtesy Dr. Elena Gorman).
Granular cell tumor
Granular cell tumors are relatively uncommon, typically benign neoplasms and may appear on the larynx, tongue, lips, palate, and gingiva (Munday et al., 2016). They have also been reported on the skin and in the central nervous system (Gross et al., 2005). The term ‘granular cell tumor’ is descriptive, as the cell of origin is unknown (Munday et al., 2016). Cytologically, granular cell tumors typically contain individualized round to polygonal cells with abundant pale pink cytoplasm, which contains numerous small, distinct, eosinophilic granules (Figure 6.31). Transmission electron microscopy has demonstrated that the granules are large, membrane-bound lysosomes. Granules are diastase resistant with periodic acid–Schiff stain (Figure 6.32; Higgins et al., 2001; Liptak, 2020). Nuclei are generally small and round and may be obscured by the granules. Occasionally, a spindloid morphology is observed. Biological behavior is unpredictable, but lesions are often locally aggressive (Higgins et al., 2001, 2016).
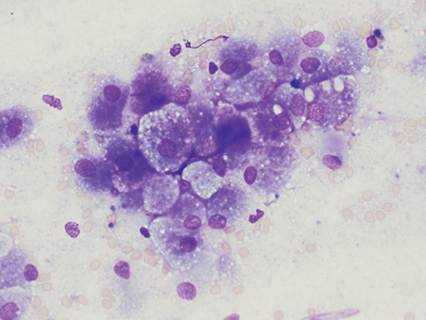
Figure 6.31 Laryngeal mass from a dog. Granular cell tumor. Cluster of loosely cohesive round-shaped to angular cells with an abundant amount of basophilic, vacuolated cytoplasm that typically contains a faint dusting of eosinophilic granules. Nuclei are round and centrally located with fine granular chromatin (modified Wright’s, 500? magnification).
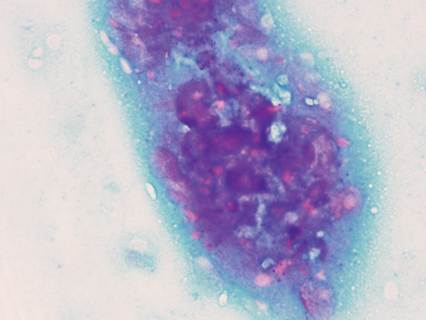
Figure 6.32 Cells from granular cell tumor in Figure 6.31 staining for periodic acid–Schiff (PAS) are brightly eosinophilic. (PAS, 500? magnification)
Other tumors
Many other malignancies have been reported in the oral cavity and lesion location in the mouth should not preclude an appropriate cytologic diagnosis (Figure 6.33). Lymphoma, morphologically identical to that diagnosed at other locations, is the most common tonsillar neoplasm (Figure 6.34). Mast cell tumors, plasma cell tumors, and transmissible venereal tumors, with their distinct morphologic features, can be diagnosed in the mouth and on surrounding mucous membranes (Figures 6.35–6.37; Hostetter, 2023). Dental tumors (e.g., odontomas) may arise and typically surround or replace the dental arcade. These tumors are named based on their cell or tissue of origin and the degree of odontogenesis, and appropriately applying naming conventions requires experience examining these lesions (Gelberg, 2021).
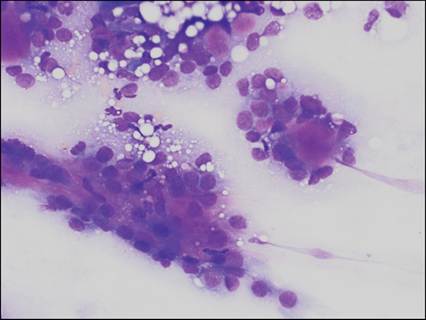
Figure 6.33 Salivary gland mass from a dog. Adenocarcinoma. Basilar-type salivary epithelial cells with high N:C ratios often form clusters and acini surrounding a bright eosinophilic extracellular secretory product. Anisocytosis and anisokaryosis are mild, making histologic confirmation necessary (modified Wright’s, 500? magnification).
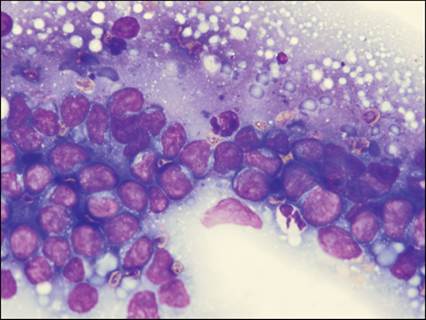
Figure 6.34 Laryngeal mass from a cat. Lymphoma. There is a monomorphic population of large lymphocytes with occasional indistinct nucleolar rings. Scattered lymphoglandular bodies are present in the background (modified Wright’s, 1,000? magnification).
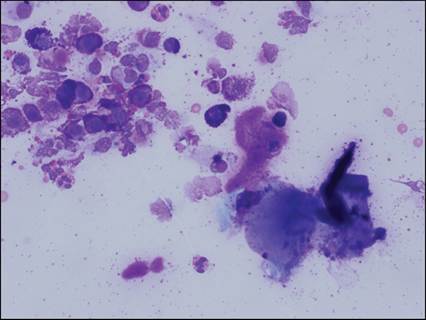
Figure 6.35 Oral mass from a dog. Mast cell tumor. Individualized round cells with abundant metachromatic intracytoplasmic granules. Nuclei are round and often do not take up stain. Eosinophils and free mast cell granules are in the background. Keratinized squamous epithelial cells with adherent Conchiformibius spp. organisms indicate oropharyngeal origin or contamination (modified Wright’s, 500? magnification).
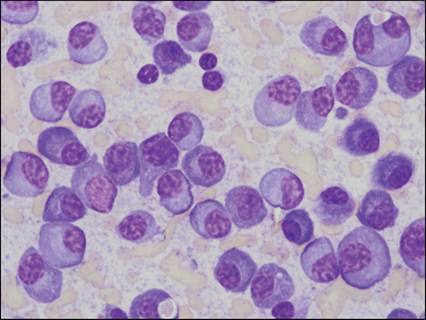
Figure 6.36 Lip mass from a cat. Plasmacytoma. Individualized round cells with a moderate to large amount of deeply basophilic cytoplasm that exhibits a perinuclear clear zone. Nuclei are peripheralized with a coarsely granular chromatin pattern. Occasional binucleated cells are seen and low numbers of erythrophagocytic plasma cells are present. Anisocytosis and anisokaryosis are mild (modified Wright’s, 1,000? magnification).
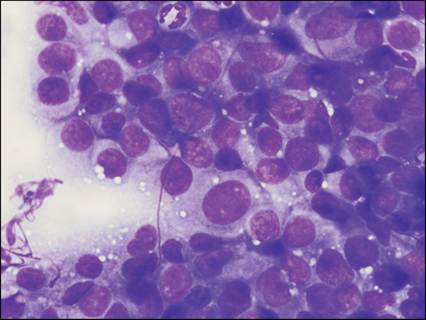
Figure 6.37 Labial mass from a dog. Transmissible venereal tumor. Aggregate of individualized round cells with pale, basophilic cytoplasm that occasionally contains discrete, nonstaining vacuoles. Nuclei are round to ovoid with finely granular chromatin. Anisocytosis and anisokaryosis are mild to moderate (modified Wright’s, 1,000? magnification).