Other Bacterial Infections Corynebacterium kutscheri Infection: Pseudotuberculosis; Corynebacteriosis
Corynebacterium kutscheri is a Gram-positive bacillus that can infect mice, rats, and guinea pigs.
The organism is frequently harbored as an inapparent infection. The organism may be carried for several weeks in the oropharynx and adjacent lymph nodes in the absence of inflammatory lesions.
In clinical cases, hematogenous spread occurs from these sites, with resultant dissemination to the thoracic and abdominal viscera. Visceral abscesses will eventually heal by scarring and become culture-negative. Clinically, all age groups may be infected.Disease and mortality are usually associated with concomitant disease states, such as immunosuppression or nutritional deficiencies. Infections with viral pathogens such as rat coronavirus, Sendai virus, or parvovirus do not appear to alter the course of the disease experimentally.
Pathology
Weight loss, respiratory distress, and ruffled hair coat are typical clinical signs, when present. At necropsy, dark red encrustations may be present around the eyes and external nares, or there may be a mucopurulent exudate around the nose. In the lung, there are frequently raised pale foci of suppuration of variable size with a characteristic hyperemic peripheral zone (Fig. 2.36). Affected areas frequently coalesce with adjacent lesions. Raised foci may be present in other organs, particularly the liver and kidney (Fig. 2.37). Fibrinous exudate may be present on the pleura and/or pericardium.
Lesions most frequently occur in the lung. There are foci of coagulation to caseation necrosis, with leukocytic infiltration. Neutrophils are the predominant cellular infiltrates in the early stages. Subsequently, there are mononuclear cells composed of macrophages, lymphocytes, and plasma cells. Lesions arise hematogenously, and early lesions can be found in association with blood vessels (Fig. 2.38).
Adjacent pulmonary parenchyma may have interstitial pneumonia, with hypercellularity of alveolar septa, perivascular cuffing, and pulmonary edema. Some airways adjacent to affected areas may contain purulent exudate. Lesions of several days duration are suppurative in nature, with peripheral mononuclear cell infiltration and fibrosis. Large bacterial colonies are pathognomonic in lesions that have not resolved (Fig. 2.39), and appear as amorphous basophilic material in H&E stained tissue sections. Lymphoid hyperplasia is a frequent finding in chronic cases of
FIG. 2.36. Corynebacterium kutscheri infection (pseudotuberculosis) in an adult rat. Note the multiple foci of abscessation with peripheral reddening and consolidation in the lung.
Corynebacteriosis, and residual scars may be present in target tissues in recovered animals.
Diagnosis
The distribution and nature of the lesions require confirmation by bacterial culture of affected organs or oropharyngeal washings. Gram, Warthin-Starry, or Giemsa stains will reveal the diphtheroid appearance of the bacilli, with “Chinese letter” configurations. Detection

FIG. 2.37. Multifocal hematogenous renal abscesses in a rat due to Corynebacterium kutscheri infection.
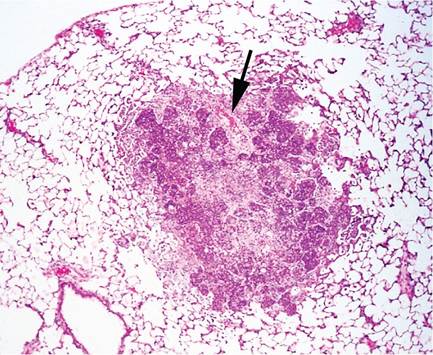
FIG. 2.38. Lung from a case of early Corynebacterium kutscheri dissemination. Note inflammation arising at the terminus of a small artery (arrow), indicative of hematogenous dissemination.
of carrier animals is best accomplished by culture or PCR of oropharyngeal washes or cervical lymph nodes. Serology is available for detecting seropositive rats. Differential diagnoses include pulmonary abscessation associated with advanced cases of chronic respiratory disease, acute to chronic pseudomoniasis, or diplococcal infections.