Rat Coronavirus Infection: Sialodacryoadenitis
Based upon past serological surveys, antibodies to rat coronaviruses were relatively common in both laboratory and wild rats, and outbreaks continue to occur sporadically in laboratory and pet rats.
The 2 naturally occurring prototype coronaviruses isolated from this species are Parker's rat coronavirus (PRC) and sialoda- cryoadenitis virus (SDAV). SDAV is a morphological term, and represents any and all subsequent coronavirus isolates that produce necrotizing inflammation of salivary and lacrimal glands (sialodacryoadenitis). PRC was first isolated from the lungs of rats. Intranasal inoculation of newborn and weanling rats with PRC produced rhinitis, tracheitis, and interstitial pneumonia, with focal atelectasis and high mortality in infants. PRC also induces salivary and lacrimal gland lesions, but these were overlooked in the original descriptions. SDAV isolates produce lacrimal and salivary gland lesions, but also produce pulmonary disease in young rats. These viruses should be considered part of a single biological grouping (rat coronaviruses). Nevertheless, this dichotomy and terminology continues because of historical precedent. Like mouse hepatitis virus (MHV), the rat coronavirus group is likely to contain numerous, constantly changing strains that vary in virulence.SDA is a disease of high morbidity and negligible mortality. Permanent ocular damage may occur in a small percentage of rats. Transient respiratory tract damage and hypersecretion may result in unexpected deaths in rats anesthetized during the acute stages of SDA. There is evidence that the virus has a significant additive effect in rats previously infected with M. pulmonis, and possibly the cilia-associated respiratory (CAR) bacillus. Behavioral changes and reproductive disorders including aberrations of the estrous cycle and neonatal mortality have also been associated with epizootics of the disease.
Active infection has also been found to precipitate graft-versus- host disease in the salivary and lacrimal glands of rats with allogenic bone marrow grafts.Epizootiology and Pathogenesis
Transmission is primarily through nasal secretions or saliva, and the virus spreads rapidly following introduction into a susceptible population of rats. In epizootics, there can be subclinical to high morbidity with virtually no mortality. Typical clinical signs associated with SDAV infection during the acute stages of the disease include sniffling, epiphora, blepharospasm, and cervical swelling. Dark red encrustations may be present around the eyes and external nares. These porphyrin-containing substances are released from damaged Harderian glands and emit a characteristic pink fluorescence under an ultraviolet light source. Other complications sometimes seen during the convalescent period include unilateral or bilateral ocular lesions. Reproductive disorders, including neonatal mortality and aberrations in the estrous cycle, have also been associated with SDAV. Prior exposure to the SDAV provides protection against the development of the disease upon reinfection for up to 15 months.
Pathology
Acutely infected rats may display excessive lacrimation or have red encrustations around the external nares and eyelids. Reflection of the skin of the ventral neck may reveal subcutaneous, periglandular, and interlobular edema of the parotid and/or the submandibular (submaxillary) salivary glands. In contrast to normal glands, affected glands are enlarged and blanched, with periglandular edema (Fig. 2.12). Similar changes are frequently evident in the Harderian, exorbital, and infraorbital lacrimal glands. Harderian glands often have blotchy brown pigmentation. During the acute stage of the disease, affected parotid and submandibular salivary glands and lacrimal glands have coagulation necrosis of the ductal epithelium, variable involvement of adjacent acini, with effacement of the normal architecture.
Interstitial edema, with mononuclear and polymorphonuclear cell infiltration, frequently occurs (Figs. 2.13 and 2.14). During the reparative stages of the disease, beginning at 7-10 d postexposure, there is nonkeratinizing squamous metaplasia of ductal and acinar structures of salivary (Fig. 2.15) and lacrimal glands, with reactive hyperplasia of cervical lymph nodes. Cellular infiltrates in affected glands at this stage are primarily lymphocytes, plasma cells, mast cells, and
FIG. 2.12. Sialodacryoadenitis virus (SDAV) infection of a rat during the acute stage of the disease. The submandibular salivary glands of the affected rat (a) are blanched and swollen (arrow), with periglandular edema, compared to an unaffected rat (b).
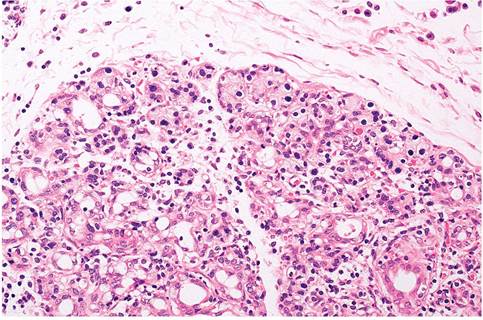
FIG. 2.13. Submandibular salivary gland from a rat during acute SDAV infection. Note the epithelial necrosis, leukocytic infiltration, and interlobular and periglandular edema.
' ł..
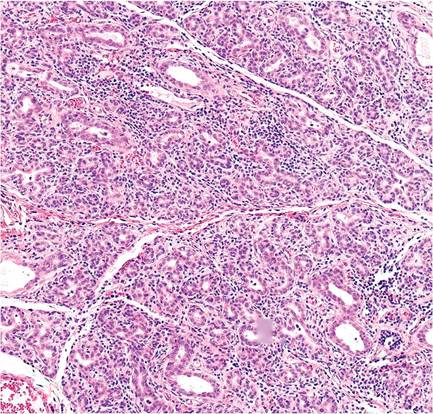
FIG. 2.15. Parotid salivary gland during early resolution of SDAV infection. Ducts and acini are lined by undifferentiated hyperplastic epithelium and the interstitium is infiltrated with mononuclear leukocytes.
macrophages. Squamous metaplasia is evident in salivary and lacrimal glands, and may be particularly marked in the Harderian glands (Fig. 2.16). In salivary glands, regeneration of acinar and ductal epithelial cells is usually complete by 3-4 weeks postexposure. There may be isolated ducts or acini lined by poorly differentiated epithelial cells, with scattered aggregations of mononuclear cells, including mast cells, but usually the salivary glands are essentially normal histologically at this stage. Focal residual inflammatory lesions associated with interstitial deposition of pigmented material may persist in the Harderian glands for several weeks.
Ocular changes are secondary to impaired lacrimal gland function, resulting in keratitis sicca, impaired intraocular drainage, hyphema, and megaloglobus (Fig. 2.17), with subsequent permanent damage to the eye.Necrotizing rhinitis, with mononuclear and polymorphonuclear cell infiltration, occurs during the acute stages of the disease. Both respiratory and olfactory
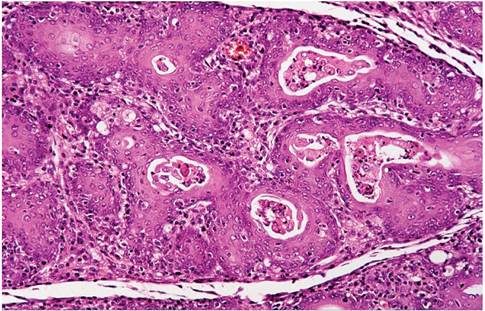
FIG. 2.16. Harderian gland from a rat during recovery from SDAV infection. There is marked squamous metaplasia of ducts and acini.
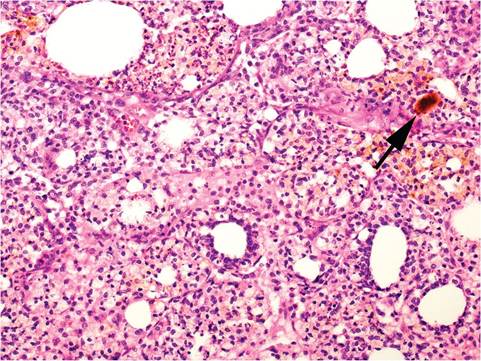
FIG. 2.14. Harderian gland from a rat during acute SDAV infection. There is necrosis of glandular epithelium. Note the inspissated brown porphyrin pigment (arrow).
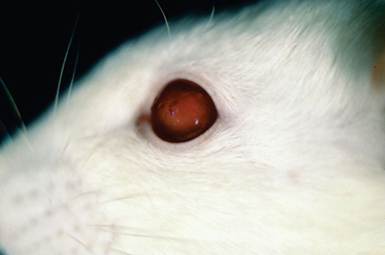
FIG. 2.17. Megaloglobus with hyphema as a sequel of SDAV infection.
epithelia are affected. The majority of the repair is complete by 14 days postexposure, although residual lesions may persist longer in specialized areas such as the vomeronasal organ. In the lower respiratory tract, there is transient tracheitis, and focal bronchitis and bronchiolitis, with leukocytic infiltration, hyperplasia of respiratory epithelial cells, and flattening and loss of ciliated cells. Focal alveolitis, when present, is characterized by hypercellularity of alveolar walls and mobilization of alveolar macrophages. Lesions in the lower respiratory tract are transient and usually have disappeared by 8-10 days postexposure.
Athymic nude rats are particularly susceptible to SDAV and develop chronic persistent infections and wasting disease. Chronic suppurative rhinitis, bronchopneumonia, and chronic inflammatory lesions in the salivary and lacrimal glands have been described. Viral antigen was evident in affected tissues, including epithelium of the urinary tract.
Diagnosis
The presence of the typical lesions of the salivary and lacrimal glands confirmed on microscopic examination is sufficient to make the diagnosis. Viral antigen may be present in the respiratory tract and affected salivary and lacrimal glands at 4-6 days postexposure, and PCR has been used for definitive diagnosis. Virus isolation is not a practical procedure in most circumstances. Serological testing is the recommended method to confirm prior exposure to SDAV. Differential diagnoses include nasal and ocular discharge associated with mycoplasma, Sendai virus, or pneumonia virus of mice (PVM) infections; subcutaneous edema of the head associated with Pseudomonas aeruginosa; ocular and nasal irritation associated with high environmental ammonia levels; and stress- associated chromodacryorrhea. The presence of porphyrin-containing red encrustations around the eyes and nose (chromodacryorrhea) are often present, but not diagnostic for SDA. Chronic disease states (e.g., chronic respiratory disease (CRD)) and stress-associated events may also result in the release of porphyrins from the Harderian glands.