Slides for cytologic evaluation
Preparation
A direct smear from a well-mixed sample should always be prepared and evaluated to verify the electronic cell count. Effusions with low cellularity (class="lazyload" data-src="/files/uch_group75/uch_pgroup311/uch_uch7426/image/image907.jpg" alt=fig15.67.jpg>
Figure 15.67 This mesothelial cell has a cytoplasmic fringe (glycocalyx), coarse nuclear chromatin, and discrete nucleoli (Hemafix™, 1,000? magnification).
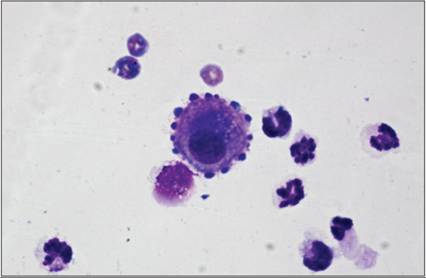
Figure 15.68 This mesothelial cell has a round nucleus with smooth chromatin and abundant cytoplasm with ear-like protrusions (Hemafix™, 1,000? magnification).
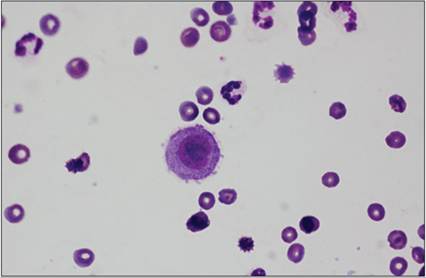
Figure 15.69 The nuclei of mesothelial cells can vary in shape and occasionally will be cleaved or bean-shaped (Hemafix™, 1,000? magnification).
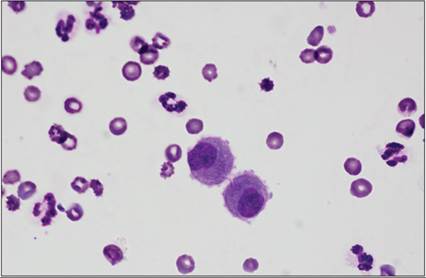
Figure 15.70 These mesothelial cells exhibit dense chromatin and prominent nucleoli (Hemafix™, 1,000? magnification).
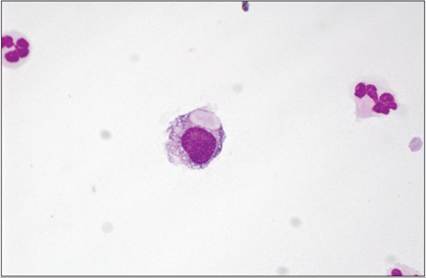
Figure 15.71 Mesothelial cells can occasionally have discrete cytoplasmic vacuoles (Hemafix™, 1,000? magnification).
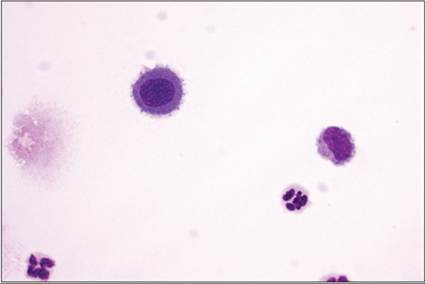
Figure 15.72 These mesothelial cells have discrete oval nuclei (Hemafix™, 1,000? magnification).
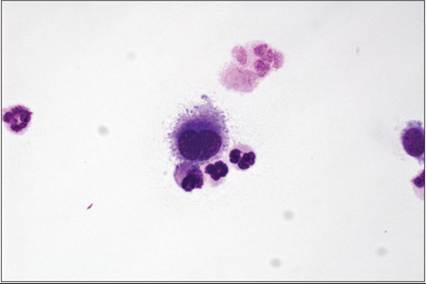
Figure 15.73 Mesothelial cells are commonly binucleate (Hemafix™, 1,000? magnification).
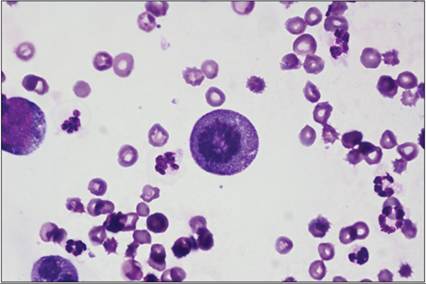
Figure 15.74 Mitotic figures are occasionally observed in the mesothelial population (Hemafix™, 1,000? magnification).
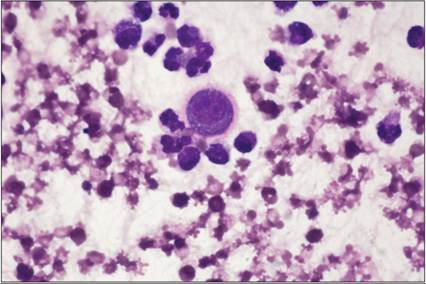
Figure 15.75 A mesothelial cell surrounded by degenerate neutrophils, with a round nucleus and cytoplasmic fringe (Hemafix™, 1,000? magnification).
Low numbers of neutrophils are present in almost all effusions, and the number of neutrophils increases with inflammation. Neutrophils can be differentiated into nondegenerate and degenerate forms:
· Nondegenerate neutrophils (Figures 15.79–15.81) resemble those seen in peripheral blood, with basophilic clumped chromatin and segmented nuclei. They are suggestive of nonseptic inflammation. Hypersegmentation and pyknosis of the nucleus is a common finding in aging neutrophils (Figures 15.82, 15.83). Aging neutrophils and nuclear remnants are often phagocytized by macrophages.
· Degenerate neutrophils (Figures 15.1–15.4) have undergone hydropic degeneration induced by bacterial toxins, which alter membrane permeability. Water diffuses into the cells and nuclei and causes swelling of the nucleus, which fills more cytoplasm. Nuclear chromatin becomes homogeneous and stains pink.
Macrophages (Figures 15.84–15.86) are also present in effusions and resemble tissue macrophages. They are large round cells with a bean-shaped amoeboid nucleus with a condensed reticular chromatin pattern. Cytoplasm is pale gray, often vacuolated, and might contain phagocytized material.
Small well-differentiated lymphocytes are commonly seen in small numbers in all effusions, except in lymphatic/chylous effusions where they are often the predominant cell type (Figures 15.10, 15.18). They are similar to lymphocytes in peripheral blood, with a round nucleus with a dense chromatin pattern and a small blue cytoplasmic rim. Reactive lymphocytes are slightly larger; the cytoplasm is deep blue, more abundant, and can show ear-like projections. These cells are common in inflammatory effusions. Occasionally, plasma cells can be found (Figure 15.87).
Eosinophils (Figures 15.88, 15.89) are readily recognized as they resemble those in peripheral blood. They can be increased in neoplastic disease (mast cell tumors, lymphoma), parasite infestation, or allergic reactions. Repeated removal of fluid from body cavities might also cause an influx of eosinophils.
Mast cells are inflammatory cells and can be found in low numbers in body cavity effusions. They are round cells with a round centrally positioned nucleus, which is often obscured by magenta to purple colored granules. In mast cell tumor-associated effusions, they occur in high concentration and can also exhibit high variability in size and granularity (Figures 15.31, 15.32, 15.34, 15.35, 15.63).
Erythrocytes are also present in effusions due either to hemorrhage or contamination. They deteriorate and hemoglobin degradation products such as hematoidin (orange rhomboid crystals; Figure 15.13) or hemosiderin (blue to greenish pigment; Figure 15.15) are formed and can be detected within macrophages. Bacteria (Figures 15.5, 5.90, 15.91) and parasites (Figure 15.92) can also be detected by microscopic examination. Phagocytized bacteria are more readily detected in the feathered edge or margins. Their staining properties in Romanowsky stains vary from blue to pinkish and do not reflect their Gram staining properties.
Neoplastic cells of all types can be observed in effusions. Carcinoma and adenocarcinoma of various origins (Figures 15.45–15.51), mesothelioma (Figures 15.42–15.44), and round cell tumors such as lymphoma (Figures 15.27–15.30), mastocytoma (Figures 15.31, 15.32, 15.34, 15.35, 15.63), multiple myeloma (Figures 15.36, 15.37), and malignant histiocytosis (Figures 15.38, 15.39) or ectopic thyroid carcinomas (Figures 15.93, 15.94) readily exfoliate into body cavity effusions. Mesenchymal tumors such as hemangiosarcomas (Figures 15.40, 15.41) may shed only a few cells and the associated effusions are usually hemorrhagic; thus tumor cells can be easily overlooked.
Malignant melanoma can also metastasize and form a tumor-associated effusion (Figures 15.95, 15.96). As mentioned above, differentiation between different types of carcinomas and mesothelioma is often impossible unless a primary tumor is identified or special stains are performed. Considering the high variability in the morphology of reactive mesothelial cells, at least four to five cytomorphologic criteria of malignancy as well as adequate cellularity should be present in a suspect cell population before an effusion is considered to be neoplastic. A few criteria of malignancy in a low number of cells, especially in combination with an inflammatory reaction, must not be overinterpreted. Absence of tumor cells in an effusion, as in any cytologic preparation, never rules out neoplasia. However, cytologic evaluation should never be omitted as a positive result provides a quick result and makes a substantial contribution to diagnosis. 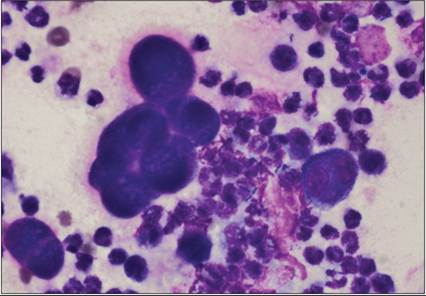
Figure 15.76 Reactive mesothelial cells from a septic exudate. The mesothelial cells have variability in the nuclear to cytoplasmic ratio, vacuolated cytoplasm, and anisocytosis (Hemafix™, 1,000? magnification).
Figures 15.77 Recurrent pericardial effusion from a Wire-haired Pointer. The mesothelial cells are reactive and pleomorphic with marked anisocytosis and anisokaryosis (Hemafix™, 400? magnification).
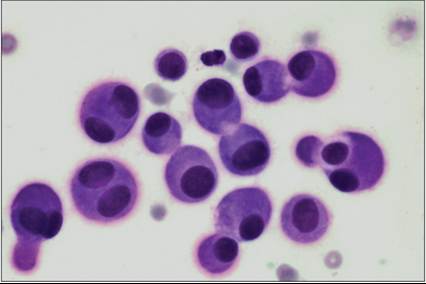
Figure 15.78 Recurrent pericardial effusion from a Wire-haired Pointer. Clusters of hyperplastic mesothelial cells exhibit anisocytosis and anisokaryosis but have a smooth chromatin pattern (Hemafix™, 1,000? magnification).
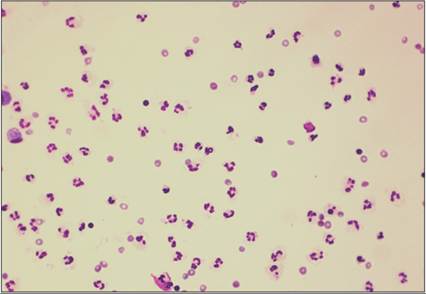
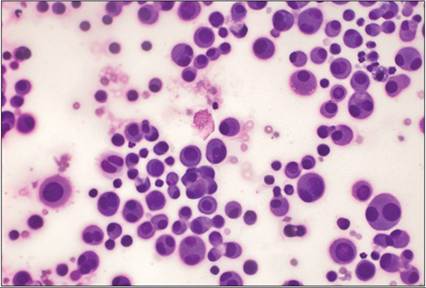
Figure 15.79 Cytospin preparation of a transudate.
Nondegenerate neutrophils are occasionally hypersegmented (Hemafix™, 400? magnification).
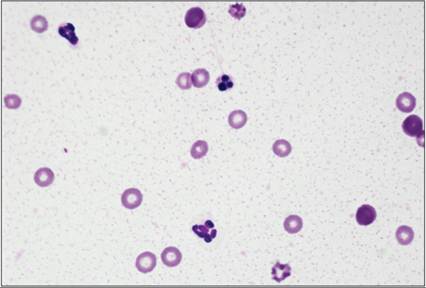
Figure 15.80 A pyknotic cell is pictured in the top center (Hemafix™, 1,000? magnification).
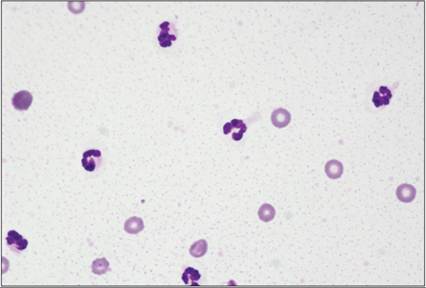
Figure 15.81 Cytospin preparation consisting of nondegenerate neutrophils (Hemafix™, 1,000? magnification).
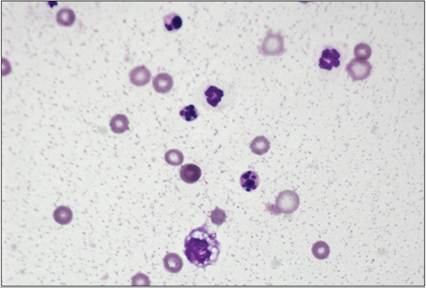
Figure 15.82 Aging neutrophils can appear as pyknotic and/or karyorrhectic cells (Hemafix™, 1,000? magnification).
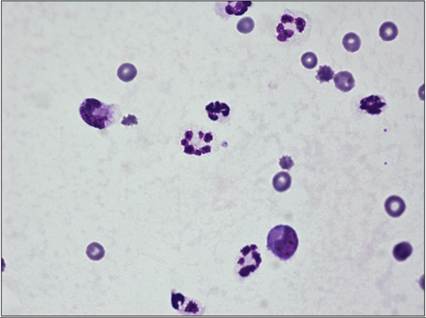
Figure 15.83 Hypersegmented neutrophils are arranged in a background of proteinaceous material and few red blood cells (Hemafix™, 1,000? magnification).
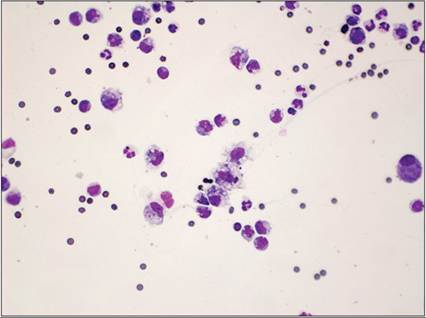
Figure 15.84 Activated macrophages have vacuolated cytoplasm (Hemafix™, 400? magnification).
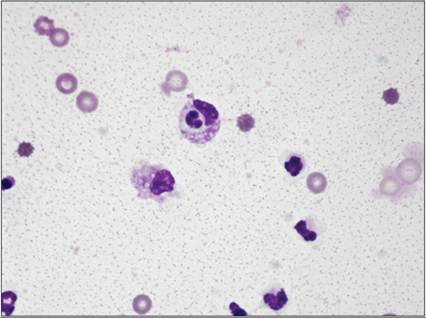
Figure 15.85 Activated macrophage that has phagocytized a neutrophil (leukophagia) (Hemafix™, 1,000? magnification).
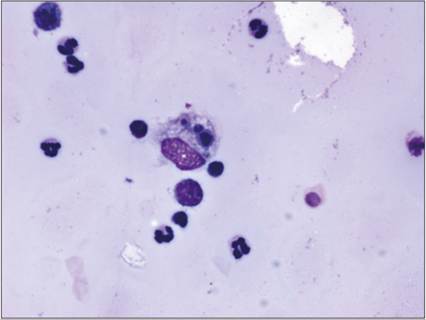
Figure 15.86 Macrophage phagocytizing pyknotic cells (Hemafix™, 1,000? magnification).
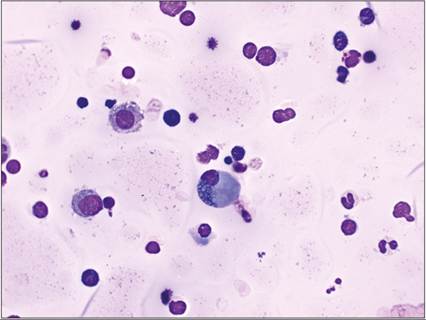
Figure 15.87 Pleural fluid from a cat. In the center is a Mott cell (Hemafix™, 1,000? magnification).
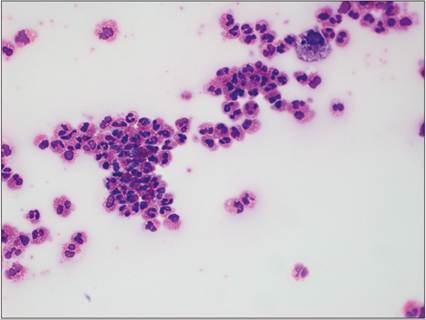
Figure 15.88 Abdominal fluid from a domestic shorthair cat. Activated macrophages and many eosinophils are observed (Hemafix™, 400? magnification).
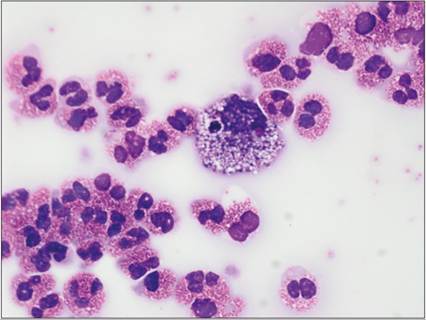
Figure 15.89 Abdominal fluid from a domestic shorthair cat. Many eosinophils and a vacuolated macrophage are pictured. The cat was diagnosed with intestinal eosinophilic granulomatosis (Hemafix™, 1,000? magnification).