Small intestine (duodenum, jejunum, and ileum)
Normal
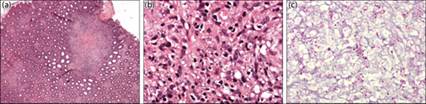
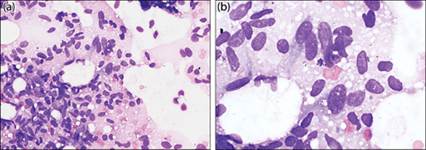
The epithelial layer is comprised of tall simple columnar epithelial cells with microvilli that function in absorption of nutrients (Figures 7.16a–c). Goblet cells are present and may be visualized in histologic and, occasionally, cytologic preparations.
The lamina propria layer contains lymphoid cells along with occasional globular leukocytes and Paneth cells, which participate in primary defense. Therefore, few lymphocytes and mononuclear cells may be present when sampling the intestine. 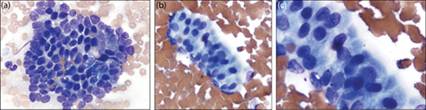
Figures 7.16a–c Normal small intestinal cytology, canine. (a) Duodenum; 500? magnification. (b) Jejunum; a row of uniform columnar epithelial cells with fine cilia; 500? magnification. (c) Jejunum; 1,000? magnification (Wright–Giemsa).
Hyperplastic lesions
In hyperplastic lesions of the intestine, diagnosis is usually presumptive and based on clinical history, diagnostic imaging, and identification of uniform populations of epithelial cells. Some cellular atypia may be present due to associated lesions such as inflammation, including chronic enteropathy (CE), or underlying neoplasia (Figure 7.17). Lymphoid follicular hyperplasia is also common and may occur secondary to infectious disease. Lymphoid hyperplasia of mucosal lymphoid tissue may even form mass-like lesions and thus be mistaken for lymphoma or CE (Figure 7.18). Therefore, similar to hyperplastic lesions of the stomach, intestinal hyperplasia is not a cytologic diagnosis and usually requires additional histopathology and investigation for an underlying disorder.
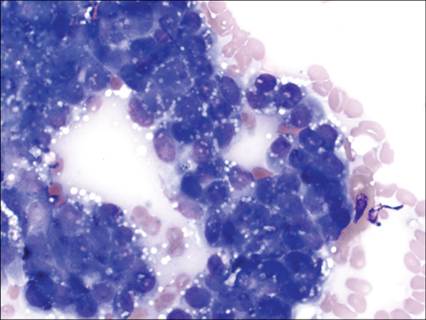
Figure 7.17 Small intestine, canine. Cytology of an FNA of intestinal epithelium overlying a sarcoma (same dog as in Figure 7.37).
Note the epithelial cells display moderate atypia including basophilia and more prominent nucleoli but are still generally uniform in shape and size. These changes were interpreted as dysplastic based on additional findings (Wright–Giemsa, 500? magnification).
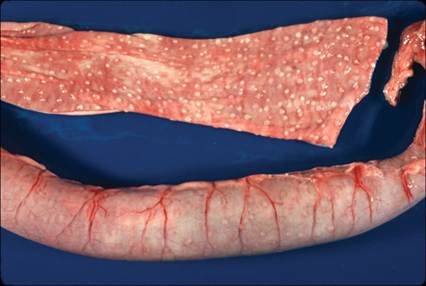
Figure 7.18 Gross image showing marked lymphoid hyperplasia in the intestine of a dog. (Courtesy Barry Cooper.)
Inflammatory lesions
In most inflammatory disorders of the GIT, diagnosis is a multistep process and typically includes additional diagnostics including fecal analysis, PCR or other assays for underlying infectious organisms, and, usually, tissue biopsy.
Foreign body reactions
Like foreign bodies at other sites, intestinal foreign bodies are usually diagnosed by a history of exposure or noted ingestion of an object along with diagnostic imaging. Cytology is usually only performed in lesions where no known history of foreign object ingestion is present and/or imaging is equivocal for an obstruction. Cytology may show the presence of chronic, usually pyogranulomatous, inflammation or may be unrewarding if significant fibrosis is present. Bacteria and clinical evidence of sepsis may be present.
Chronic enteropathy/chronic inflammatory enteropathy
Chronic enteropathies (CE) are a spectrum of disorders with three current categories recognized based upon response to treatment: immunosuppressive- (steroid) responsive (also called idiopathic inflammatory bowel disease), food-responsive, and antibiotic-responsive enteropathy (Dandrieux & Mansfield, 2019). The pathogenesis of these disorders is complex and likely involves immune system dysregulation, environmental factors, and genetic predisposition (Jergens & Heilmann, 2022).
Idiopathic, immunosuppressive-responsive CE is an immune-mediated disease process characterized by infiltration of inflammatory cells into the lamina propria layer (see Figure 7.3) of the intestine.
The pathogenesis of the disease is proposed to involve a loss of immunologic tolerance to normal antigens causing abnormal T-cell immune reactivity in the gut leading to chronic inflammation and injury (Cave, 2003). Inherited disorders are identified in numerous dog breeds including immunoproliferative enteropathy of Basenjis, familial protein-losing enteropathy and nephropathy in Soft-Coated Wheaten Terriers, and eosinophilic enteritis and granulomas in Siberian Huskies (German et al., 2003). In cats, heritable gastroenteropathies are questionable, although some studies have shown increased incidence in purebred cats (Dennis et al., 1992; Jergens et al., 1992).Food responsive CE in dogs and cats is evidenced by positive results of elimination diets (Guilford et al., 2001; Makielski et al., 2019). Affected dogs tend to be younger and may have less severe clinical signs than with other causes for CE (Jergens & Heilmann, 2022). Familial causes for these disorders include gluten-sensitive enteropathy in Irish Setters.
Antibiotic-responsive diarrhea (ARD; previously called small intestinal bacterial overgrowth) results in chronic GI signs in dogs. Idiopathic ARD has not been definitively identified in cats, although mild chronic enteropathy in cats may be controlled with antibiotic therapy alone. It is a diagnosis of exclusion where no underlying cause can be found but which is completely responsive to antibiotic treatment. However, this condition is currently debated as, despite initial response to antimicrobials, most patients will relapse post-discontinuation of treatment (Jergens & Heilmann, 2022). Additionally, overuse of antibiotics may also allow for disruption of normal enteric microbiota resulting in overgrowth of normal commensal organisms and resultant dysbiosis (Suchodolski, 2022). Affected dogs are typically young, large breeds, with German Shepherd dogs being overrepresented in many studies (Hall, 2011; Dandrieux & Mansfield, 2019). Clinical signs are typically due to chronic or recurrent small bowel diarrhea, although some dogs show signs of colitis.
Microscopic evaluation of fecal samples from affected animals usually shows a mixed population of commensal bacteria although indication of changes in the normal microbiota (AKA dysbiosis) may be noted cytologically by apparent overgrowth of a particular population. Culture of fecal bacteria does not always correlate with bacterial numbers or species in the intestines, nor does culture indicate if bacterial toxins are produced (Weese, 2011; Suchodolski, 2022). Culture has therefore been largely replaced by molecular methods for organism detection. However, lack of standardization and variability in methodology between labs can make interpretation of results difficult (Suchodolski, 2022).Lymphoplasmacytic gastroenteritis
Regardless of the underlying cause, lymphoplasmacytic gastroenteritis (LPE) is the most common histopathologic finding for CE in both dogs and cats (Jergens, 1999; German et al., 2001; Maeda et al., 2017; Makielski et al., 2019). In LPE, the distribution of disease is primarily diffusely mucosal, with the lamina propria most severely affected. T cells predominate, but variable numbers of B cells, including plasma cells, can be identified (Figures 7.19a, b). Thus, CE is definitively diagnosed by histologic characterization, and full-thickness biopsy specimens are recommended to rule out underlying disorders causing secondary inflammation (Kleinschmidt et al., 2009; Freiche et al., 2021). However, infiltrates of inflammatory cells can be identified cytologically by aspiration of thickened mucosa or discrete lesions (Figure 7.20a, b). More severe forms may lead to ulceration and mixed inflammatory infiltrates, and multifocal disease is common. A concern exists that more severe lesions may progress to neoplasia. Indeed, lymphoma has been documented in both dogs and cats with a history of LPE (Jacobs et al., 1990; Hart et al., 1994; Roccabianca et al., 2006; Lingard et al., 2009). Furthermore, differentiating between a diagnosis of severe lymphoplasmacytic inflammation and low-grade, small-cell lymphoma is often difficult; therefore, a multistep approach incorporating histology, immunochemistry, and PCR analysis for antigen receptor rearrangement (PARR) is usually recommended to aid histologic diagnosis of both entities (Kiupel et al., 2011) (Figure 7.21).
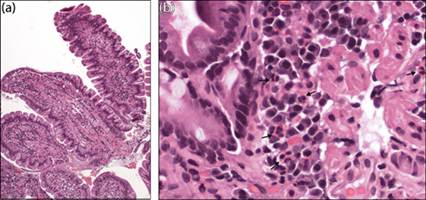
Figures 7.19a,b Small intestine, canine. Histologic section from a dog diagnosed with lymphoplasmacytic enteritis. (a) Note the marked expansion of lymphocytes in the lamina propria layer of the intestinal villi (H&E, 100? magnification). (b) At higher magnification, plasma cells, lymphocytes, and eosinophils (arrows) are more readily seen (H&E, 500? magnification).
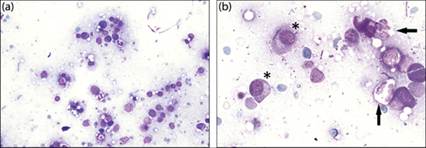
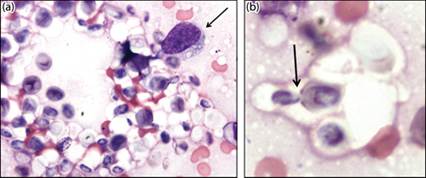
Figures 7.20a,b Intestine, feline. Aspirate from a thickened portion of ileum in a cat with lymphoplasmacytic gastroenteritis. (a) Mixed inflammation is present. Few erythrocytes and mixed bacteria are also present among eosinophilic proteinaceous background material (Wright–Giemsa, 400? magnification). (b) Small lymphocytes and numerous plasma cells (asterisks) and occasional neutrophils (arrows) are identified at higher magnification (Wright–Giemsa, 1000? magnification).
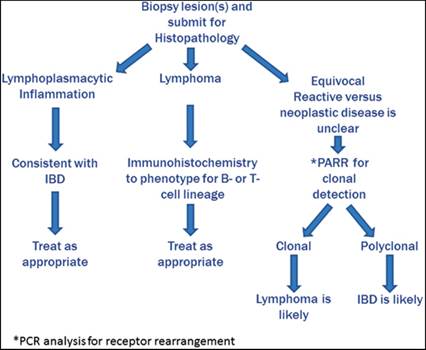
Figure 7.21 Diagnostic approach for lymphoproliferative disease in the gastrointestinal tract. Adapted from Kiupel M, Smedley RC, Pfent C et al. (2011) Diagnostic algorithm to differentiate lymphoma from inflammation in feline small intestinal biopsy samples. Vet Pathol 48(1):212–222.
Eosinophilic gastroenteritis
Eosinophilic inflammation can be seen with some underlying infectious causes (e.g. pythiosis and parasites described below) and as a paraneoplastic infiltrate secondary to neoplasia (see discussion under lymphoma below). However, primary idiopathic eosinophilic disease remains relatively uncommon in both dogs and cats. In cats, the disorder is poorly characterized. It may be associated with hypereosinophilic syndrome or food allergies, but often only mild increases in eosinophils are identified in the GIT of cats, even with food-responsive enteropathy (Guilford et al., 2001) (Figures 7.22a, b, 7.23).
When present, however, clinical signs are often more severe, clinicopathologic and histopathologic changes are more evident, and peritonitis may even be present (Figure 7.24) (Tucker et al., 2014). A unique condition, ‘feline gastrointestinal eosinophilic sclerosing fibroplasia’, is described (Craig et al., 2009; Weissman et al., 2013; Linton et al., 2015). Affected cats typically develop a focal, ulcerated intramural mass at the pyloric sphincter, ileocecocolic junction, or colon. Lesions are characterized by eosinophilic inflammation and fibrosis and cats may also have eosinophilic lymphadenitis and peripheral eosinophilia. Lesions are often associated with microabscesses and bacterial infection. On histopathology, mast cells are also seen but this is not consistently reported in cytologic specimens (Linton et al., 2015). Furthermore, aspiration of these lesions may be unrewarding due to fibrosis. The cause of this disorder is unknown. 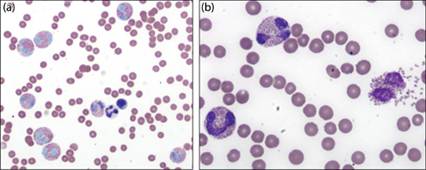
Figures 7.22a,b Jejunum, feline. Aspirate of a thickened region of intestine. Marked eosinophil infiltration is present (Wright–Giemsa: a, 500? magnification; b, 1,000? magnification).
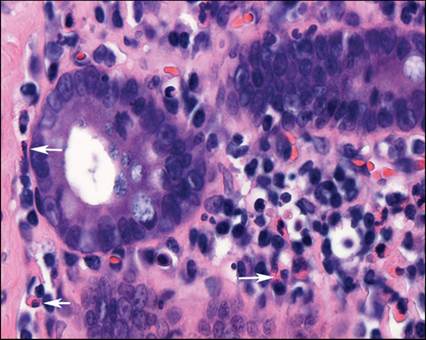
Figure 7.23 Histologic section from a cat with eosinophilic enteritis. Eosinophils are indicated by the arrows (H&E, 1,000? magnification).
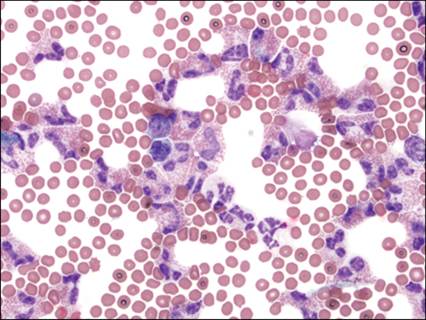
Figure 7.24 Peritoneal fluid, feline. Mixed inflammatory cells predominated by eosinophils are found in the abdominal effusion from a cat diagnosed with eosinophilic gastroenteritis (Wright–Giemsa, 700? magnification).
In dogs, breed-associated eosinophilic disease has been described in the Rottweiler and Cavalier King Charles Spaniel (German et al., 2002; Lyles et al., 2009). This disorder may be associated with granulomas in the esophagus, stomach, and small and large intestines (see Figure 7.52). The pathogenesis of these lesions is unknown, but several pathogenic mechanisms are speculated, including parasitic and allergic reactions (Johnson, 1992; Lyles et al., 2009).
Infectious causes of enteritis
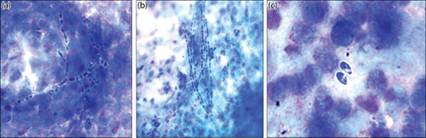
Like primary gastric infections, small intestinal bacterial infections are relatively uncommon in dogs and cats. Mycobacterium spp. are well-known pathogens that typically result in systemic disease. Both classic tuberculosis (including M. tuberculosis, M. bovis, and M. microti) and opportunistic mycobacteriosis (including M. fortuitum) have been described in dogs and cats, although clinical disease is inconsistently reported in these species (Kukanich et al., 2013; Pesciaroli et al., 2014). In animals infected with M. avium subspecies paratuberculosis (MAP), chronic enteritis and colitis are common clinical signs. However, MAP-specific DNA can be identified within the intestinal and nodal tissue of dogs and cats that do not have pathologic lesions or clinical signs of GI disease (Glanemann et al., 2008; Kukanich et al., 2013). In clinically affected animals, infection with MAP typically induces granulomatous inflammatory infiltrates with variable degrees of lymphocytic and/or suppurative inflammation. The organism can usually be identified as nonstaining linear structures both in macrophages and extracellularly on Romanowsky-stained slides (Figures 7.25a–c). The organisms can further be visualized with the use of an acid-fast stain (Figure 7.25d). PCR for MAP DNA is necessary for speciation of the organism (Glanemann et al., 2008).
Viral gastroenteritis
Numerous viral organisms are implicated in the development of gastroenteritis in dogs and cats. These include viruses that cause direct mucosal injury (e.g. parvovirus and coronavirus), as well as organisms that cause enteric signs secondary to immunosuppression (e.g. FIV) from T-cell infiltration and/or disruption of normal regulatory cell populations (Hartmann, 2011). Although histology of GIT biopsies may be diagnostic for some viral infections, cytology is rarely useful and antemortem diagnoses are usually reliant on viral ELISAs, serology, and PCR. An exception may be lesions induced by feline infectious peritonitis, where aspiration of large granulomas or infiltrated tissues (e.g. kidney or liver) may be useful in supporting a diagnosis in clinically affected cats (Figure 7.26) (Giordano et al., 2005).
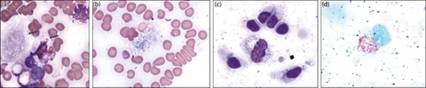
Figures 7.25a–d FNA from a region of intestinal thickening in a dog. (a, b) A mixed inflammatory infiltrate is present with numerous negative-staining linear structures (arrows) consistent with Mycobacterium spp. found in the macrophages (a) and throughout the background of the sample (b) (Wright–Giemsa, 1,000? magnification). (c) Same patient with organisms identified in an associated abdominal lymph node (Wright–Giemsa, 1,000? magnification). (d) Organisms stain red with an acid-fast stain (Ziehl–Neelsen, 2,000? magnification).
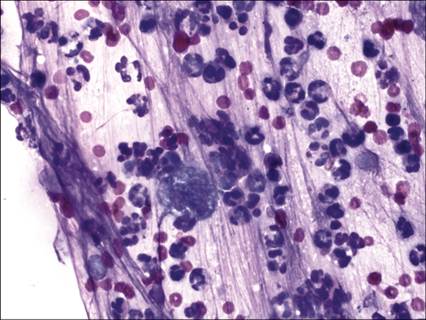
Figure 7.26 FNA from a mass in the intestine of a cat with feline infectious peritonitis (FIP) (confirmed post-mortem). Large numbers of nondegenerative neutrophils and occasional macrophages are found among thick fibrillar, eosinophilic, proteinaceous background material. The presence of granulomatous or pyogranulomatous inflammation without visible infectious organisms may be noted in lesions associated with FIP (Wright–Giemsa, 500? magnification).
Fungal gastroenteritis
Fungal infections of the GIT are generally less common than bacterial or viral infections. A few dimorphic fungi may colonize the GIT in specific environmental regions. Histoplasma capsulatum, for example, is commonly associated with chronic enteritis and colitis in infected individuals (Bromel & Sykes, 2005). Histoplasma spp. are small, 2–4-μm diameter yeasts with a central body surrounded by a thin clear capsule. Organisms may be identified via impression smears or aspiration of masses and/or associated lymph nodes (Figures 7.27a, b). Impression smears from endoscopic or full-thickness biopsies are also diagnostic for identifying organisms in infected tissues (Figures 7.28a–c).
Figures 7.27a,b FNA of a region of thickened intestine from a dog with chronic diarrhea and weight loss. (a) Numerous small yeast organisms are identified in a degenerating macrophage. The yeasts are consistent with Histoplasma capsulatum. (Wright–Giemsa, 1,000? magnification). (b) Organisms (arrow) are also identified in an adjacent abdominal lymph node. (Wright–Giemsa, 500? magnification).
Figures 7.28a–c Histologic section from the intestine from the same dog as in Figure 7.27. (a) The intestinal mucosa is thickened by infiltrating macrophages with lesser numbers of neutrophils and a large granuloma (H&E, 100? magnification). (b) Severe granulomatous to pyogranulomatous inflammation is present secondary to large numbers of intralesional yeast identified as Histoplasma capsulatum (H&E, 700? magnification). (c) Periodic acid–Schiff stain assists identification of small intralesional yeast (700? magnification).
Occasionally, infection by environmental fungi or overgrowth of commensal species may develop in individuals with compromised GI health. Some studies analyzing the small intestinal content from healthy and diseased dogs from different geographic locations have detected a high prevalence and diversity of fungal DNA in both healthy dogs and dogs with chronic enteropathies. In cases of fungal-associated disease, the organisms are highly antigenic and typically result in marked granulomatous and pyogranulomatous inflammatory infiltrates. Eosinophils may also be noted in some patients. Depending on the infection, spores, yeast, or hyphae may be identified in fecal smears, often surrounded by degenerating cellular constituents. Evidence of associated bacterial overgrowth may also be noted.
Candida, Cryptococcus, and Aspergillus spp. have all been reported to cause GI disease in animals (Schultz et al., 2008; Suchodolski et al., 2008; Uchiumi et al., 2014; Johnston et al., 2021). Cryptococcus spp. is ubiquitous and can result in disseminated disease in animals. It is found as large budding yeast surrounded by a thick nonstaining capsule (Figures 7.29a, b). As seen with other fungal infections, inflammation is usually granulomatous to pyogranulomatous in nature.
In human and veterinary medicine, the role of Candida spp. in antibiotic-associated diarrhea is controversial. Since Candida spp. exist physiologically in the GIT, the presence of small numbers of these organisms in stool is considered normal and, therefore, nonpathogenic. Individuals at risk for serious disseminated disease are more likely to be immunosuppressed, such as patients with cancer or secondary to GI perforation (Bradford et al., 2013). In tissue samples, Candida spp. are recognized as small, oval to elongated, segmentally constricted pseudohyphae with occasional buds (Figures 7.30a–c).
Figures 7.29a,b FNA from an intestinal mass in a cat diagnosed with cryptococcosis. (a) Extracellular round yeast organisms (approx. 5–15 in diameter) surrounded by variably thick clear-staining capsules are present along with a single macrophage (arrow). (b) Organism showing characteristic narrow-based budding (arrow) typical of Cryptococcus spp. (Wright–Giemsa, 1,000? magnification).
Figures 7.30a–c FNA of a mass associated with the ileum of a dog with candidiasis (C. albicans confirmed by culture). (a) Neutrophils, eosinophils, and a few macrophages are noted along with degenerating cellular debris. (b) Moderate numbers of fungal hyphae/pseudohyphae are present. Organisms are septate and branching with thin nonparallel walls. (c) Budding and spores are frequently seen (Wright–Giemsa, 1,000? magnification).
Like candidiasis, disseminated aspergillosis has been linked to immunosuppression. The German Shepherd dog is overrepresented in most studies, which may be attributed to dysfunction of normal mucosal immunity in this breed (Schultz et al., 2008; Olsson et al., 2014). Organisms are found as septate and branching hyphae in infected tissue and, like other fungal infections, are associated with marked inflammation and cellular degeneration (Figure 7.31). Therefore, in most cases of fungal-associated gastroenteritis, evidence of systemic illness and chronic debilitation is usually present.
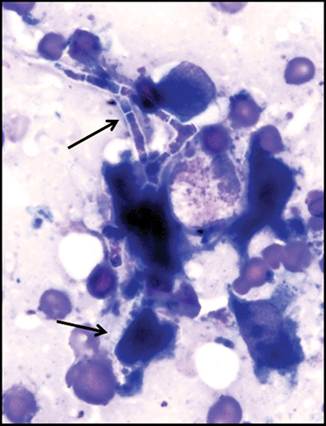
Figure 7.31 Aspergillus spp. infection in a dog. Long fungal hyphae (arrows) are found with associated pyogranulomatous inflammation and cellular degeneration in an intestinal lesion near the pancreas. Hyphae are septate and branching with thin clear cell walls. Disseminated disease was present in this patient (Wright–Giemsa, 1,000? magnification).
‘Pseudofungi’
Algae and oomycetes such as Prototheca, Pythium, and Lagenidium spp. are often referred to as ‘pseudofungi’ based on their morphologic appearance and tendency to induce marked pyogranulomatous inflammatory infiltrates.
Protothecosis in animals is due to infection with a unicellular achlorophyllic algal organism (Masuda et al., 2021). These organisms are opportunistic pathogens, which are ubiquitous soil saprophytes and typically found in moist environments in manure, water, and sewage. Despite worldwide distribution and prevalence in nature, they only rarely cause clinical signs of disease. Like opportunistic fungal infections, protothecosis has been linked to both localized and systemic disease in canine and feline patients. GI signs, usually colitis, are more common in dogs and are attributed to infection with Prototheca zopfii (Masuda et al., 2021). More discussion on the identification and diagnosis of protothecosis is provided under large intestinal inflammatory disorders (see Figure 7.56).
Pythium insidiosum is a pathogenic oomycete found mainly in tropical and subtropical regions. Infection occurs mainly in horses, dogs, and humans and is rare in cats. The organism invades through small wounds via contact with water that contains motile zoospores or hyphae. Depending on the site of entry, infection can lead to different forms of disease including a cutaneous, vascular, ocular, GI, and, rarely, a systemic form (Gaastra et al., 2010). Signs of enteritis are common in dogs with pythiosis. Vomiting, weight loss, intermittent diarrhea, and palpable abdominal masses are frequently described. Peripheral eosinophilia and hyperglobulinemia have also been identified in infected dogs (Berryessa et al., 2008). Cytologically (and histologically), Pythium spp. can be challenging to detect. They form nonseptate, branched hyphae with irregular cell walls and stain poorly with Romanowsky stains (Figure 7.32). The infection frequently results in pyogranulomatous infiltrates similar to other fungal and algal organisms.
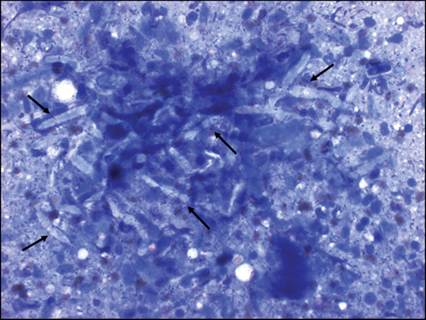
Figure 7.32 Impression smear from a gastrointestinal lesion from a dog with confirmed pythiosis. Aggregates of nonstaining hyphal structures with blunt rounded ends (arrows) are present among degenerating leukocytes (Wright–Giemsa, 700? magnification) (courtesy Mark Dunbar).
Lagenidium spp. are oomycetes closely related to Pythium. The pathogenic forms of lagenidiosis (L. caninum or L. karlingii) have clinical, epidemiologic, and cytologic characteristics similar to those of pythiosis in dogs, making them difficult to differentiate (Figure 7.33). Although enteric disease may occur with systemic infections, GI lesions are uncommon in animals infected with Lagenidium spp. (Grooters, 2003). The use of organism-specific antibodies or PCR is necessary for definitive diagnosis.
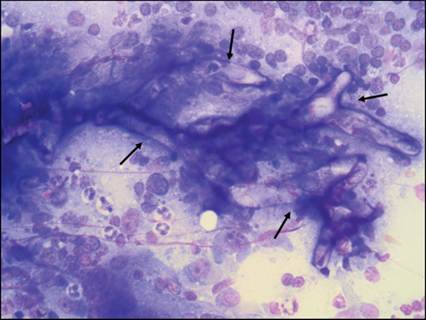
Figure 7.33 Gastrointestinal lesion from a dog. Similar to Pythium, Lagenidium spp. (arrows) stain poorly with Romanowsky stains (Wright–Giemsa, 700? magnification) (courtesy Mark Dunbar).
Neoplasms of the small intestine
Numerous tumor types are described in the intestinal tract of animals. Clinical signs are usually similar with vomiting, diarrhea, and/or anorexia frequently reported. On physical examination, poor body condition, a palpable mid-abdominal mass, pain, and thickened intestinal loops and/or ascites may be noted. Radiologic features of intestinal masses may reveal focal or diffuse changes depending on the tissue of origin. Many exhibit similar changes such as hypoechoic thickening of the intestinal wall, which may be noncircumferential and eccentric or circumferential, asymmetric, and eccentric (Laurenson et al., 2011; Willard, 2012; Freiche et al., 2021).
Epithelial tumors
Benign epithelial tumors of the small intestine are very rare in small animal patients. Malignant tumors, carcinomas and adenocarcinomas, are more commonly diagnosed in dogs and cats (Willard, 2012; Munday et al., 2017). In cats, adenocarcinomas are the second most common neoplasm of the GIT comprising approximately 7% of reported cases. They are most often found in the mid-lower small intestine. Siamese and male cats are overrepresented in many studies (Slawienski et al., 1997; Rissetto et al., 2011; Munday et al., 2017). Tumors frequently result in annular stenosis of a focal region of the intestine, but they may be more diffuse with circumferential thickening of the bowel. Metastasis to local lymph nodes and peritoneal surfaces is common in both species (see Case 1).
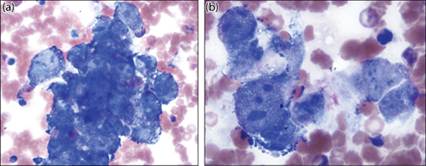
As described above, for the diagnosis of gastric tumors, the most successful results appear to be obtained by impression smears from biopsy specimens; however, FNA is usually successful as carcinomas typically exfoliate well. Carcinomas in all locations often appear similar. They are usually identified as cohesive clusters of atypical epithelial cells that display little resemblance to normal mucosa (Figure 7.16). Tumor cells frequently lose their normal columnar shape and often become more rounded to polygonal and frequently are found in ‘piled’ aggregates, indicating a loss of normal mucosal architecture. The cytoplasm is often deeply basophilic and the N:C ratio is typically increased, although cells may form variably sized cytoplasmic vacuoles which distort the cell. Nuclei often contain prominent nucleoli and nuclear molding may be observed. Moderate anisocytosis and anisokaryosis are usually present, and mitoses are often difficult to discern due to crowding (Figure 7.34).
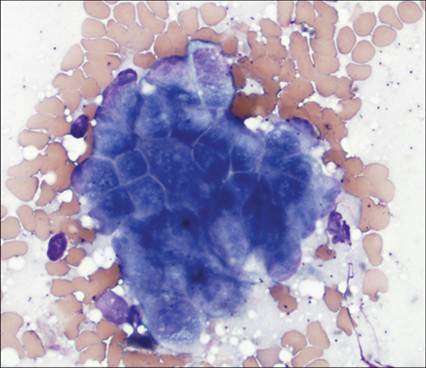
Figure 7.34 FNA from a mid-intestinal mass in a cat. A dense aggregate of neoplastic epithelial cells is present. Individual cells exhibit high N:C ratios, cytoplasmic basophilia, and prominent nucleoli characteristically found in intestinal adenocarcinomas (Wright–Giemsa, 500? magnification).
Stromal/spindle cell tumors
Spindle cell tumors of the intestinal tract are generally uncommon in small animals, comprising approximately 10–30% of intestinal tumors in dogs (Russell et al., 2007). As noted above in the stomach, most spindle cell tumors were erroneously diagnosed as smooth muscle tumors (leiomyomas and leiomyosarcomas) prior to immunostaining techniques (see the examples of these tumors in the colon – Figures 7.61, 7.62). In dogs, spindle cell tumors located in the small intestine are most commonly diagnosed as GISTs; however, smooth muscle tumors are also reported in the small intestines (Frost et al., 2003; Russell et al., 2007; Gillespie et al., 2011; Hayes et al., 2013; Del Alcazar et al., 2021). In cats, intestinal smooth muscle tumors and GISTs are quite rare and typically limited to case reports and small case series (Barrand & Scudamore, 1999; Rissetto et al., 2011; Suwa & Shimoda, 2017).
Microscopically, leiomyomas and leiomyosarcomas are comprised of spindle-shaped cells with oval to cigar-shaped nuclei often forming bundles and streams (Figures 7.35a, b). Metastasis is uncommon but tumors can be locally invasive if poorly differentiated. GISTs are derived from the interstitial cells of Cajal (pacemaker cells) but cytologically often appear very similar to smooth muscle tumors (Figures 7.36a, b). Histologically, these are nonencapsulated cellular masses comprised of streams and short interlacing bundles of spindloid (‘storiform’ or ‘palisading’) to epithelioid cells. GISTs localize in the submucosa and muscularis but often expand transmurally and invade into the lamina propria. They are often associated with hemorrhage and necrosis. Metastasis to the liver, lymph nodes, and omentum may be more common with GISTs (Frost et al., 2003; Hayes et al., 2013).
Spindle cell tumors have variable exfoliation; therefore, FNA may result in limited cellularity. Cytologically, most appear similar with variable malignant criteria. Loose, noncohesive aggregates are also common with all forms including sarcomas; thus, more malignant forms may mimic poorly differentiated carcinomas (Figures 7.37a, b). As in all regions of the GIT, other sarcomas can occur in the small intestine and are usually metastatic lesions from other sites. These must be fully characterized by biopsy and immunohistochemical staining (Patnaik, 1990; LaRock & Ginn, 1997; Bonfanti et al., 2006; Rissetto et al., 2011).
Figures 7.35a,b FNA of an intestinal mass in a dog diagnosed as a leiomyoma. A dense aggregate of relatively uniform, spindle-shaped cells is found entrapped within eosinophilic matrix material. Individual cells have elongated nuclei and indistinct cell borders (Wright–Giemsa: a, 100? magnification; b, 500? magnification).
Figures 7.36a,b Cytology of a spindle cell tumor from the mid-intestinal tract of a dog. (a) Numerous disrupted spindle-shaped cells are identified at low magnification. This tumor was definitively diagnosed as a gastrointestinal stromal tumor via histology (Wright–Giemsa, 200? magnification). (b) At higher magnification (500?), spindle cells display only mild criteria for malignancy.
Figures 7.37a,b FNA of a mid-intestinal mass in a dog. Spindle to more oval-shaped cells are found in loose aggregates as well as individualized. Tumor cells in this lesion display marked malignant criteria including anaplasia. Hemangiosarcoma was suspected although not histologically confirmed (Wright–Giemsa: a, 500? magnification; b, 1,000? magnification).
Round cell tumors
Lymphoma
Lymphoma is the most common neoplasm of the feline GIT (Willard, 2012). Up to 70% of cats with lymphoma have GI involvement (Gabor et al., 1998; Richter, 2003; Louwerens et al., 2005) and small intestine location appears to be most common (Rissetto et al., 2011). Although lymphoma is considered the most common or second most common neoplasm in the canine GIT, it occurs less frequently in dogs than in cats, accounting for only 7% of all cases of canine lymphoma (Rassnick et al., 2009; Willard, 2012). In dogs, it is typically confined to the intestine but may rarely occur as a progressive stage of multicentric lymphoma (Frank et al., 2007).
As in other anatomic locations, the cause of intestinal lymphoma is unknown. A genetic influence based on clear breed predilections for certain subtypes of lymphoma has been reported. For example, Boxers are predisposed to T-cell lymphoma, while Miniature Dachshunds develop more B-cell lymphomas including alimentary forms in both breeds (Lurie et al., 2008; Pastor et al., 2009; Rimpo et al., 2022). Siamese cats are also overrepresented in some studies (Rissetto et al., 2011). Neoplastic transformation of lymphocytes in patients with lymphoplasmacytic enteritis has been reported (Jacobs et al., 1990; Hart et al., 1994; Roccabianca et al., 2006). As with the gastric form, infection with FeLV is not linked to formation of intestinal lymphoma in cats (Louwerens et al., 2005; Krick et al., 2008; Lingard et al., 2009; Freiche et al., 2021).
Clinical signs of intestinal lymphoma are similar to signs seen in other chronic disorders of the GIT. Hypoalbuminemia is a common biochemical abnormality (Frank et al., 2007; Couto et al., 2018; Freiche et al., 2021). Hypercalcemia is uncommon (Willard, 2012).
Different morphologic variants of lymphoma, including the intestinal forms, have been described in dogs and cats (Vezzali et al., 2010). These features, along with differentiation of the immunologic phenotype, have been shown to be important predictors of tumor behavior, progression of disease, response to therapy, and overall median survival time. For example, in both species, large T-cell lymphoma, also referred to as enteropathy-associated T-cell lymphoma (EATL) type 1, tends to be aggressive, quickly growing, and produces severe, progressive clinical signs (Willard, 2012). Low-grade intestinal, small-cell (EATL-type 2) lymphoma also occurs and is described most commonly in cats (Lingard et al., 2009; Briscoe et al., 2011; Moore et al., 2012). Dogs may uncommonly develop this latter, low-grade form (Couto et al., 2018; Lane et al., 2018). In both species, this small-cell variant appears to have a more favorable outcome with greater survival times post-therapy (Lingard et al., 2009; Couto et al., 2018; Lane et al., 2018; Freiche et al., 2021). Staging post-diagnosis is also an important prognostic step in intestinal lymphoma as, regardless of phenotype, metastatic spread is common.
Cytologic evaluation of an FNA is a commonly used and valuable method for diagnosing lymphoma in the intestine. The diagnostic accuracy of this method is high, provided the smear preparations are of good quality (Bonfanti et al., 2006; Ballegeer et al., 2007; Maeda et al., 2017). Although lymphocyte morphology may differ between variants, lymphoma is generally diagnosed by identifying a predominance of atypical lymphocytes associated with aspiration of a mass or thickened intestinal mucosa. Homogeneity, or a preponderance of one type of lymphoid population (e.g. large or intermediate-sized atypical lymphocytes), is highly suggestive of lymphoma (Figure 7.38 a, b). Diagnosis may be hindered by cell rupture, which is common in lymphoid disease in all locations due to fragility of lymphocytes. This is particularly true of large, immature lymphocytes where slides commonly contain numerous bare nuclei and cytoplasmic fragments (Figure 7.38 a, b). Predominance of granular lymphocytes may be identified in a variant of intestinal epitheliotropic lymphoma (Krick et al., 2008; Roccabianca et al., 2006) (Figure 7.39). While uncommon, paraneoplastic infiltration of eosinophils can be seen in some forms of T-cell lymphoma and is typically associated with more severe clinical disease (Figure 7.40).
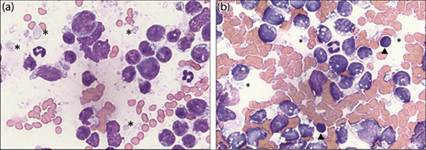
Figures 7.38a,b Cytology of intestinal lymphoma from a cat stained with both quick stain and Wright–Giemsa. A predominance of intermediate to large-sized lymphoid cells is identified via both staining modalities with frequent cytoplasmic fragments (asterisks) due to cell rupture. (a) Diff-Quik®, 1,000? magnification. (b) Few small, mature lymphocytes are present for size comparison (arrow heads) (Wright–Giemsa, 1,000? magnification).
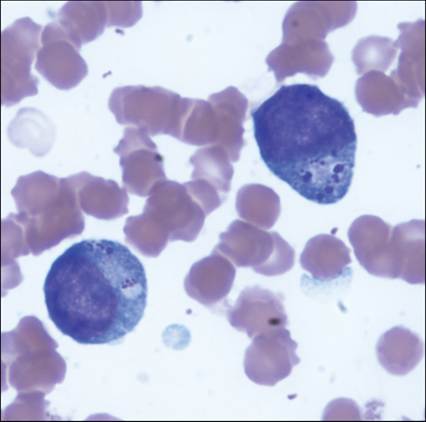
Figure 7.39 Cytology of an intestinal mass from a cat with granular lymphoma. Note the eosinophilic granules packeted on one side of the cell (Wright–Giemsa, 1,000? magnification).
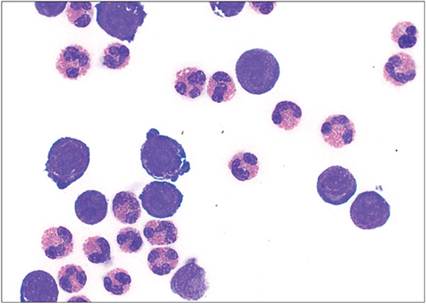
Figure 7.40 Cytology of abdominal fluid from a cat with large-cell lymphoma and paraneoplastic eosinophil infiltration. The cell count in the fluid was over 50,000/µL. Neoplastic cells are immature in appearance with large nucleoli (Wright–Giemsa, 500? magnification).
Differentiation of low-grade alimentary lymphoma from lymphoplasmacytic enteritis can be challenging cytologically and even by endoscopic intestinal biopsies, which sample only the mucosa and submucosa (Kiupel et al., 2011; Barrs & Beatty, 2012). Therefore, a multistep approach incorporating histology, immunochemistry, and PARR can be utilized to aid in the diagnosis of cases of suspected GI lymphoma in cats (Figure 7.21).
Determination of the immunophenotype of lymphoma cannot be reliably predicted by morphology of tumor cells alone; however, there are trends to suggest that most small to intermediate-sized variants of lymphoma tend to be of T-cell origin while large-cell, ‘lymphoblastic’ types can include both T- and B-cell phenotypes (Gabor et al., 1999; Sozmen et al., 2005). In cases of intestinal granular lymphomas (Figure 7.39), immunophenotypic analysis has shown that these are typically CD8+/CD3+ (cytotoxic T-cell) neoplasms (Roccabianca et al., 2006). There is some evidence that tumor location is predictive of both phenotype and prognosis in cats. For example, alimentary lymphomas are more likely to be of T-cell lineage when localized to the small intestine (Moore et al., 2012). Furthermore, small intestinal T-cell tumors may have a better long-term prognosis than B-cell tumors in cats (Lingard et al., 2009; Moore et al., 2012). In comparison, large-cell (‘lymphoblastic’) lymphoma and granular lymphoma are aggressive neoplasms with a poorer long-term prognosis in both dogs and cats regardless of location (Krick et al., 2008; Lurie et al., 2008; Willard, 2012).
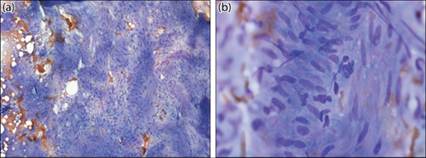
Immunophenotyping can usually be accomplished by supplying good quality, unstained cytology samples, preferably on positively charged slides (Caniatti et al., 1996) (Figures 7.41a, b). Alternatively, aspirates from the lesion may be placed into an EDTA tube with a milliliter of saline and submitted to the diagnostic laboratory within 48 hours for processing for either immunocytochemical staining or flow cytometry (Caniatti et al., 1996; Gibson et al., 2004; Sozmen et al., 2005). In cases of equivocal results due to a heterogeneous population of cells, a low cell yield, or low-grade lymphoma, additional diagnostic modalities may be necessary. This may include biopsy, where full-thickness biopsy is preferred to endoscopically acquired samples (Figure 7.42), and/or PARR (Avery, 2009; Kiupel et al., 2011; Barrs & Beatty, 2012). Indeed, PARR has been shown to be highly sensitive for detection of neoplastic (versus reactive) proliferation of lymphocytes and may even assist in staging and predicting prognosis of disease (Keller et al., 2004; Lana et al., 2006). However, clonal analysis alone may be misleading in some cases of lymphoma as both B- and T-cell receptors are frequently clonally rearranged but actual biphenotypic expression is less common (Sato et al., 2011; Weiss et al., 2011). Therefore, multimodal diagnostics are often necessary for full characterization of lymphoproliferative disorders, particularly in the GIT (see Case 2).
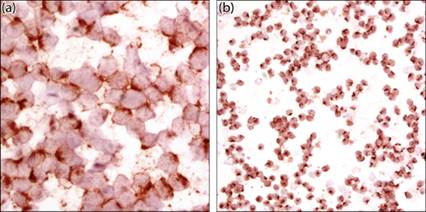
Figures 7.41a,b (a) Anti-CD79a antibody consistent with B-cell phenotype. (b) Anti-CD3 antibody consistent with T-cell phenotype (HRP polymer anti-rabbit IgG with Nova Red chromogen and hematoxylin counterstain: a, 1,000? magnification; b, 500? magnification).
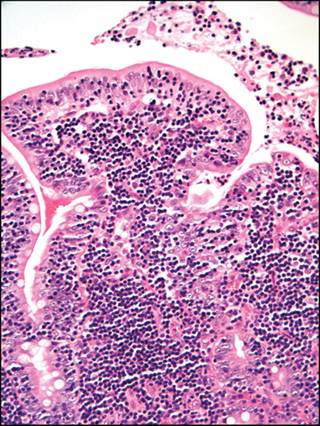
Figure 7.42 Histologic section of intestinal mucosa from a cat with lymphoma. Note the marked increase in lymphocytes within the lamina propria (H&E, 200? magnification).
Enteric mast cell tumors
Feline intestinal mast cell neoplasia is recognized as the third most common intestinal tumor in cats (Rissetto et al., 2011). Unlike lymphoma and adenocarcinoma, there are no breed predilections identified for the enteric form of this tumor (Rissetto et al., 2011. Barrett et al., 2018). Cytologically these tumors can display variable differentiation including poor granulation (Barrett et al., 2018; London & Thamm, 2020). Based on ultrastructural and histochemical features, enteric mast cell tumor is considered to be a separate entity from other visceral (e.g. splenic) mast cell neoplasms of cats. Tumors may occur anywhere along the intestinal tract; however, proximal and mid-intestinal locations are more frequently reported, whereas distal and large intestinal tumors appear to be less common. Interestingly, cats may also have concurrent intestinal lymphoma (Laurenson et al., 2011). A unique variant of feline intestinal mast cell tumor characterized by moderate to marked eosinophilic infiltrates and sclerosis has recently been described. This variant is commonly associated with lymph node and hepatic metastases and a high mortality rate (Halsey et al., 2010). Regardless of the variant, all cats with visceral mast cell neoplasia should be staged, as metastasis is common (Laurenson et al., 2011; Barrett et al., 2018; London & Thamm, 2020).
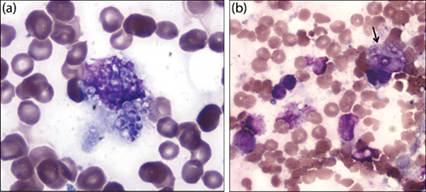
Clinical signs are typically vomiting, inappetence, and signs similar to other GI tumors. Anemia secondary to inflammation, chronic hemorrhage, or erythrophagocytosis by neoplastic mast cells is frequently identified (Figure 7.43).
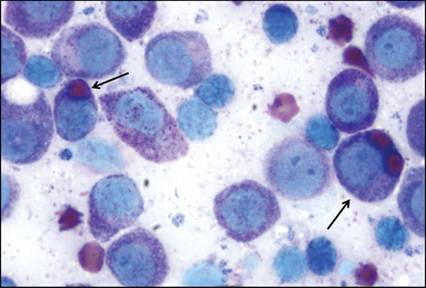
Figure 7.43 Erythrophagia by neoplastic mast cells in a cat with visceral mast cell tumor (arrows) (Wright–Giemsa, 1,000? magnification).
In dogs, high-grade cutaneous mast cell tumors frequently exhibit metastasis, particularly to the spleen, liver, and regional lymph nodes (Stefanello et al., 2009). Primary mucosal (including intestinal) mast cell tumors, however, are rare in dogs with only a few reports characterizing this disease (Takahashi et al., 2000; Ozaki et al., 2002; Kobayashi et al., 2012). Purebred male dogs of miniature breeds appear to have a higher prevalence of intestinal mast cell tumors. These are frequently of high grade and the prognosis is extremely poor (Takahashi et al., 2000).
Definitive diagnosis of intestinal mast cell neoplasia can usually be accomplished via cytologic evaluation of an FNA of the mass. Cells readily exfoliate and typically contain metachromatic granules. In cats, these granules are often smaller than those seen in other species and may not stain well with Diff-Quik® (Figure 7.44). However, caution is required when aspirating suspected visceral tumors, as mast cell degranulation may occur; therefore, pre-treatment with antihistamines is recommended (London & Thamm, 2020).
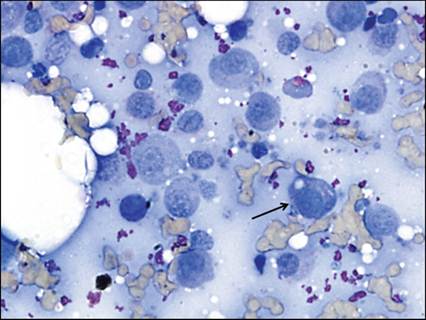
Figure 7.44 Enteric mast cell tumor in a cat. Faint eosinophilic granules can be made out in a few of the cells (arrow). The globular extracellular eosinophilic material is likely ultrasound gel (Diff-Quik®, 500? magnification).
Peritoneal effusions, occasionally containing eosinophils, along with a peripheral eosinophilia, have been documented as paraneoplastic syndromes associated with visceral mast cell disease in dogs (Figure 7.45) and cats (Peaston & Griffey, 1994). Mast cell tumors may, therefore, be misdiagnosed (even by biopsy) as eosinophilic enteritis (Howl & Petersen, 1995). Thus, the presence of eosinophils should remain as a potential indicator for underlying mast cell disease.
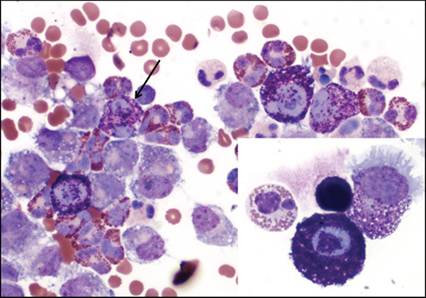
Figure 7.45 Eosinophils and neoplastic mast cells in peritoneal effusion from a dog with visceral mast cell neoplasia (Wright–Giemsa, 500? magnification; inset 1,000? magnification).