Techniques for sample acquisition
There are two ways in which to use a needle to obtain a sample of a tissue from a patient for subsequent dispelling of the needle contents onto a slide for smearing and then cytologic assessment: fenestration and aspiration.
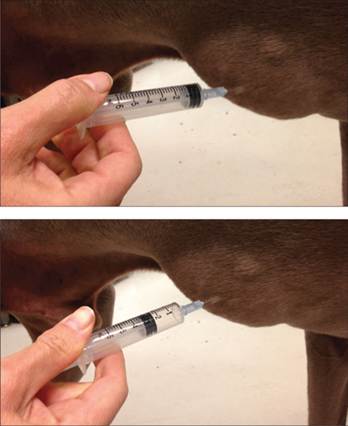
‘Fine needle aspiration’ (FNA) is typically the term used to describe either way of sampling, but the term ‘aspiration’ is often a misnomer, as fenestration, the easiest FNA technique and one that will provide a good sample the majority of the time, does not actually involve aspiration. With fenestration, the needle is rapidly inserted repeatedly into the tissue without drawing back on the plunger of an attached syringe to create negative pressure. The needle may be held and used on its own, or a syringe may be attached to the needle to act as an extension to allow for an improved grip. The syringe-attached fenestration technique is often used when sampling intrathoracic or intra-abdominal structures, as it not only creates an easier way to hold the needle but also maintains a closed system and prevents air from entering the body cavity. Preparation of the skin with clipping and scrubbing prior to FNA is almost never needed, the exception being if a culture is going to be obtained from the aspirate.For the fenestration technique without the syringe attached, first prepare the syringe that is laid out near the slides by drawing back the plunger so that there is 4–6 ml of air in the syringe. Having the syringe ready to dispel the needle contents as soon as the sample is obtained will help in creating an efficient process, thus keeping the sample from clotting. Next, the tissue to be sampled is held firmly with the non-dominant hand (Figure 1.2). The needle is inserted, using the dominant hand, through the skin and into the tissue. Then, the needle is rapidly moved back and forth, 4–8 times, into the tissue, keeping the needle under the skin at all times.
If the area to be sampled is large, the needle can be redirected in a fan shape during multiple fenestrations. Lastly, the needle is withdrawn, the syringe is attached, and the sample is expelled onto a slide (see Techniques for smearing samples onto slides). As mentioned earlier, if the tissue to be sampled is internal, a syringe with air in it may be attached to the needle and used simply as an extension without any negative pressure applied (Figure 1.3). 
Figure 1.2 Holding only the needle for the fenestration technique. Note the finger over the hub of the needle; this keeps fluid from squirting out in the case of a fluid-filled mass.

Figure 1.3 Ultrasound-guided aspirate, fenestration technique. The syringe is used solely as a handle for the needle. The syringe has air in it for ease of expelling the sample once obtained.
Alternatively, true aspiration can be used for sample attainment. In this situation, a 6 ml syringe, with the seal broken but all air expelled, is attached to the needle, and the needle is inserted into the tissue of interest with the syringe held in the dominant hand (Figure 1.4). Once the opening in the beveled part of the needle is completely inserted, so that negative pressure is obtained with aspiration, the plunger on the syringe is drawn back 1–3 ml and released rapidly 3–5 times (Figure 1.5). Be sure to release the suction on the syringe prior to withdrawing the needle from the tissue. Once the needle is withdrawn from the lesion, the needle is removed from the syringe, and 4–6 ml of air are aspirated into the syringe. It is critical to remove the needle prior to drawing air into the syringe, or the sample will be pulled into the syringe and the amount expelled will be poor. The sample is then expelled onto a slide (see Techniques for smearing samples onto slides).
Figures 1.4,1.5 FNA performed with aspiration technique. (1.4) The needle is attached to the syringe prior to entering the mass. (1.5) Once the needle is inserted, the plunger is pulled back to obtain 2–3 mL of negative pressure.
For internal organs or lesions, if a mass can be felt, it can generally be aspirated blindly. However, for lesions that cannot be palpated, or for lesions near critical structures such as major blood vessels, ultrasound (Figure 1.6) or computed tomography (Figures 1.7, 1.8) can be useful for guiding FNAs.
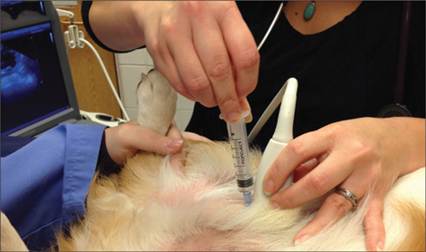
Figure 1.6 Ultrasound can be used to guide the sampling of internal lesions. In this example the aspiration technique is shown.
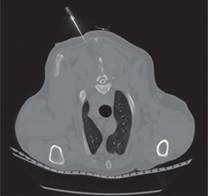
Figures 1.7 The needle is just entering the patient.
CT-guided FNA of a bone lesion.
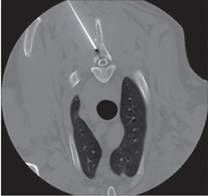
Figures 1.8 The needle is entering the lesion.
Fenestration versus aspiration
The greatest advantage of fenestration is the ease of sample collection. For most lesions, it is easier to handle only a needle as opposed to the more cumbersome syringe with a needle, and for all solid tissues, rapidly ‘poking’ the tissue several times is less difficult than holding a needle still and having to pull back and release the syringe plunger repeatedly. For very small areas of interest (e.g. feline lymph nodes [Figure 1.9], small masses), aim is improved with decreased volume of equipment and distance of the dominant hand from the sampling site with fenestration. Additionally, there may be higher cellularity and less blood contamination with the fenestration method (Leblanc et al., 2009).
The aspiration technique can be of advantageous in situations where the mass is extremely firm and does not release cells with the fenestration technique. In these cases, the added force of the negative pressure generated in the syringe may pull firmly attached cells into the needle. Note, however, that most firm masses will exfoliate very well with the fenestration method. Another situation in which aspiration is of benefit is in areas to be sampled that are extremely sensitive or painful, such as an inflamed digit or the tongue (Figure 1.10), or near a critical structure that should not be punctured, such as the eyelid margin (Figure 1.11). Entering the tissue with the needle only once and holding the needle still while aspirating with a syringe can be less uncomfortable than multiple fenestrations and is less likely to cause the needle to enter a tissue that is contraindicated. Two recent studies evaluated lymph node aspiration in dogs and cats. One study used ultrasound guidance and found that aspiration, rather than fenestration, resulted in more cellular samples (Whitlock et al., 2020). The second study evaluated canine lymph nodes and found no difference between the two techniques (Karakitsou et al., 2022).

Figure 1.9 Fenestration technique used to sample the mandibular lymph node in a cat. The lack of bulky equipment makes sampling small targets easier.

Figure 1.10 Lingual melanoma in a lightly sedated patient. This small, sensitive area can be better sampled with aspiration than with fenestration.

Figure 1.11 A mast cell tumor at the medial canthus in a Siamese cat. Aspiration of a lesion in this location in an awake patient may be less irritating and safer than fenestration.
For internal organs, fenestration is generally the preferred technique, but is usually performed with the needle attached to the syringe to prevent air from entering a body cavity through an open needle hub. Complications associated with FNA of internal organs are rare; hemorrhage from the liver or spleen or pneumothorax in cases with severe lung disease is very unlikely, but is a potential sequela to discuss with owners (Wood et al., 1998; Reichle & Wisner, 2000; Bonfanti et al., 2004; Zekas et al., 2005; Barrouin-Melo et al., 2006; Ballegeer et al., 2007; Watson et al., 2011; Bahr et al., 2013; Feeney et al., 2013; Glinska-Suchocka et al., 2013; Crain et al., 2014).