The Cardiovascular System
OBJECTIVES
• name and describe the layers of the heart and the layers of an artery
• understand how the heart is positioned in the chest and how that relates to the sites used to auscultate the heart sounds
• understand and describe the flow of blood through the heart
• name and locate the major anatomical structures of the heart using models, diagrams, and a sheep’s heart
• explain the operation of the atrioventricular valves and semilunar valves, and their relationship to the heart sounds
• dissect and name the arteries and veins of the cat; identify the pulmonary, systemic, and portal systems of blood flow
• understand the pathway of electrical conductivity through the heart, and how this produces the electrocardiogram
• know the various intervals, segments, and deflection waves produced during the electrocardiogram, and understand their relationship to the electrical conductivity of the heart
• understand arterial blood pressure and how to measure it
MATERIALS
• cat cadaver (triple injected) without skin attached
• sheep heart
• Mayo dissecting scissors
• Probe
• 1 ? 2 thumb forceps or Adson tissue forceps
• #4 scalpel handle with blade
• bone cutting forceps
• rubber gloves
• model of the heart
• electrocardiograph
• doppler and sphygmomanometer
• electric clipper and #40 blade
• rubbing alcohol
• electrocardiogram gel
Introduction
The study of the cardiovascular system can be divided into two parts: the heart and the blood-vascular system.
The major function of the cardiovascular system is transportation, with blood as the transport vehicle. The blood carries oxygen, nutrients, cellular wastes, electrolytes, and many other substances and chemicals that are essential to life and to maintaining homeostasis in the body. The heart is a muscular pump that propels the blood through the vascular system. The vascular system is composed of a number of circulatory paths. The systemic circulation is the blood flow to and from most of the parts of the body (Figure 10.1).206
The pulmonary circulation is the blood flow to and from the lungs, during which the blood picks up oxygen and returns to the heart. The coronary circulation is the blood flow to the heart muscle itself, which provides it with the oxygen and nutrition it needs to do its job as a pump. The hepatic portal system is a venous system in which blood leaves the intestines and proceeds to the liver before returning to the heart. A portal system, by definition, is a series of vessels between two capillary beds. Also by definition, the venous system returns blood to the heart, and the arterial system carries blood away from the heart.
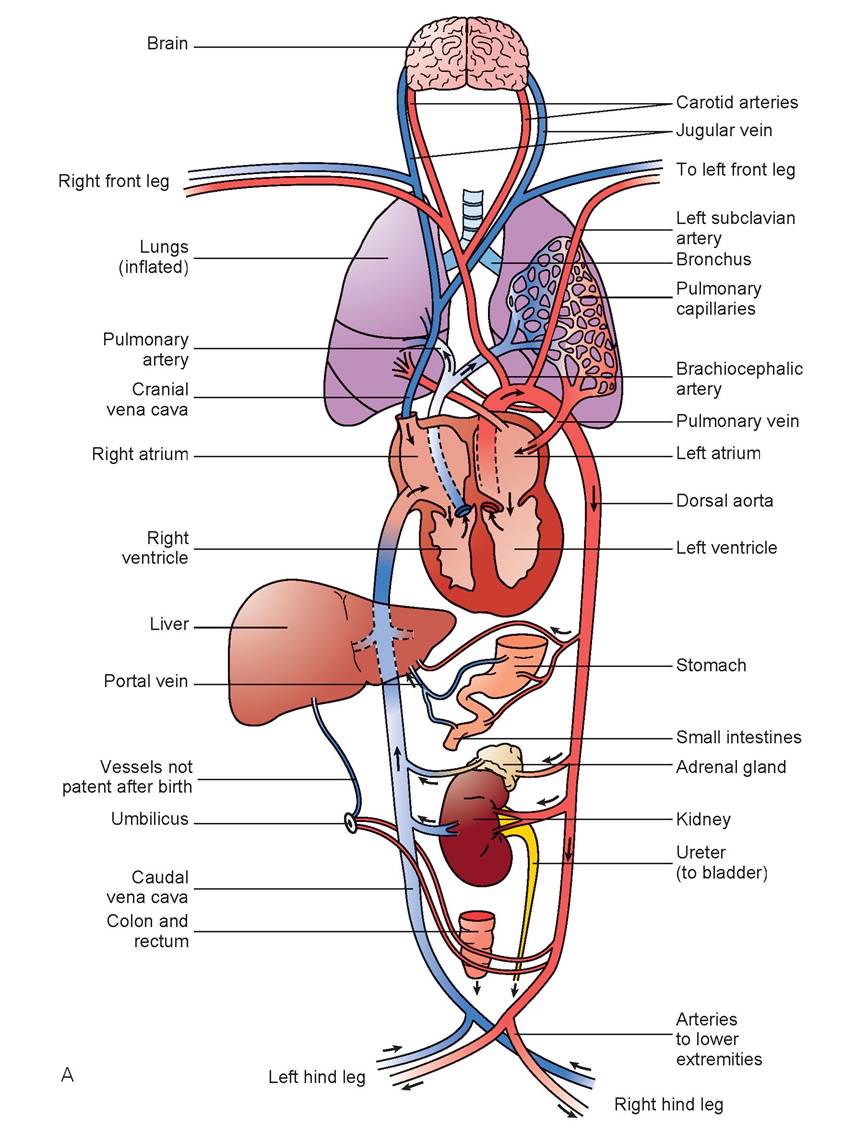
FIGURE 10.1: A. Plan of circulation in an adult animal. Red shading shows oxygenated blood and blue shading shows unoxygenated blood (opposite in the pulmonary system)
Continued
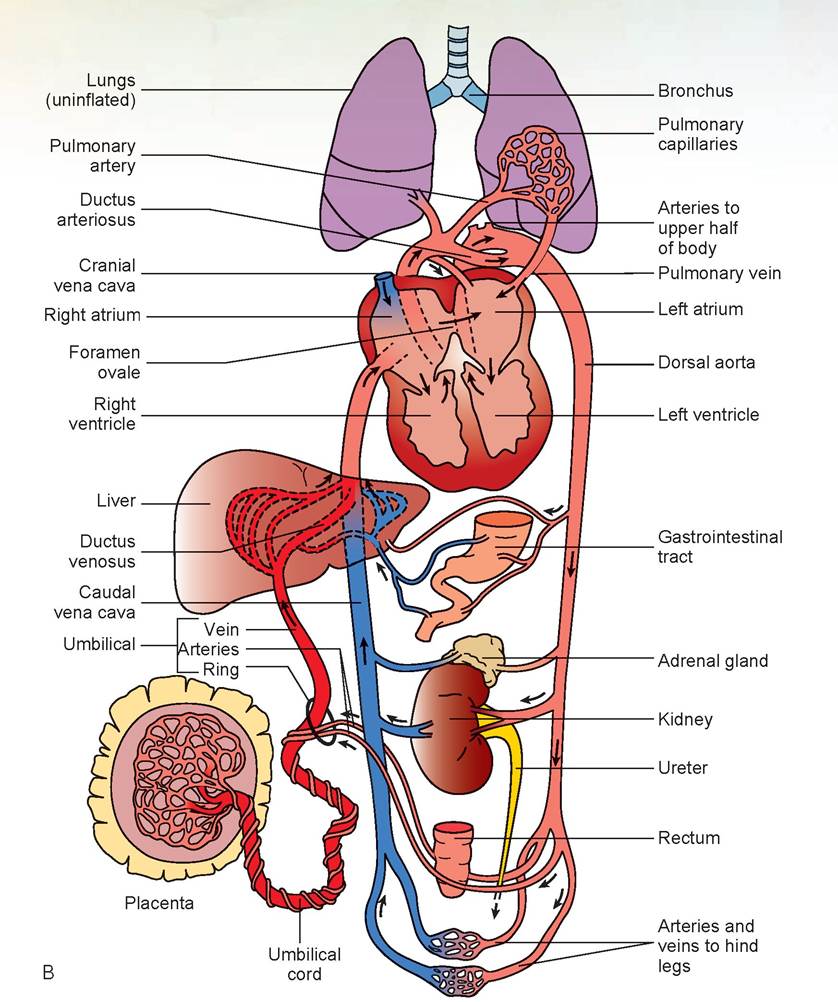
FIGURE 10.1, cont'd: B. Plan of circulation in a fetal animal. Red shading shows oxygenated blood and blue shading shows unoxygenated blood. The blood returning to the fetus via the umbilical vein has the highest oxygen content of all fetal blood
Part One: The Heart
The heart has two phases: contraction and relaxation. Contraction, or systole, is the active phase when energy is expended; relaxation, or diastole, is the resting phase. There are four chambers of the heart: the upper chambers are the right and left atria, and the lower chambers are the right and left ventricles (Figure 10.2).
Both atria contract at virtually the same time, as do both ventricles. The cardiac cycle is illustrated in Figure 10.3. The blood enters the atria while they are relaxed. The atrioventricular valves (between the atria and ventricles), also known as the AV valves, are open, and so blood flows rapidly into the ventricles.
Approximately 70% of the filling of the ventricles occurs during this phase. The atria then contract, which is called atrial systole, and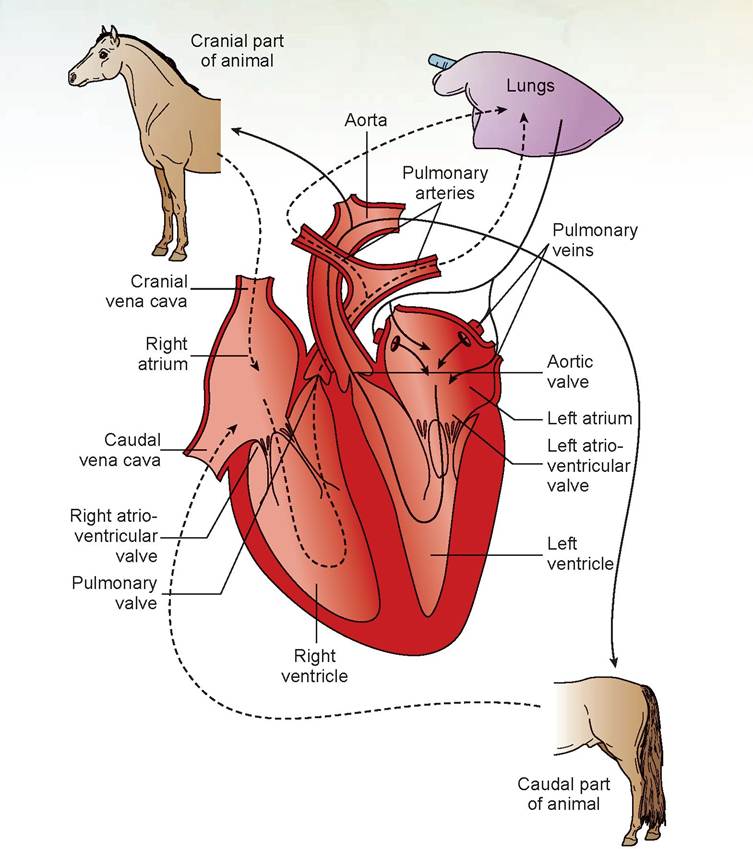
FIGURE 10.2: Diagram of the heart and the blood flow through it.
the ventricles fill completely. Next, both ventricles begin to contract, and the atrioventricular valves are forced closed, producing an audible sound; this is called the first heart sound (the lub of the lub-dub of the heartbeat). This phase is a period of isometric contraction. As contraction continues, the pressure within the ventricles overcomes the closed semilunar valvules (the valves to the large arteries that exit off the base of the heart); the valves open, and the blood is ejected into the pulmonary artery and the aorta (the large artery that begins the systemic circulation). This contraction is called ventricular systole. As blood moves into the two arteries, they stretch, and because of their elasticity, the pressure within these vessels becomes sufficient to cause the semilunar valves to snap closed. This is the second heart sound. The cycle is repeated, starting with the period
of relaxation of the heart called diastole. Figure 10.3 shows only the right side of the heart—the same cycle occurs simultaneously on the left side. The third heart sound is rapid ventricular filling, and atrial systole causes the fourth heart sound. The third and fourth heart sounds can normally be heard with an esophageal stethoscope (a tubular device placed within the esophagus, usually during anesthesia and surgery, that amplifies the heart beat and respiratory sounds). If these sounds can be heard with a normal stethoscope, there may be some cardiac problems, and the veterinarian should be alerted.
In the exercises in this chapter, the important structures are listed in colored bold print. If a structure is mentioned before its dissection, it is italicized.
Structures discussed before their dissection may also be in bold print for special emphasis.258" class="lazyload" data-src="/files/uch_group75/uch_pgroup311/uch_uch7427/image/image244.jpg">
FIGURE 10.3: Events of the cardiac cycle.
EXERCISE 10.1 ANATOMY OF THE HEART
The heart is positioned in the chest such that the base (the top part) is Iocatedjust inferior to the tracheal carina (tracheal bifurcation), and in most species it angles caudoventrally until the apex (the pointed end) is resting just superior to the last few sternabrae (in the horse the apex is located mid-sternum). Because the base of the heart is oriented more cranially than the apex, the valves of the pulmonary artery and aorta are more cranial than the valves that separate the atria from the ventricles.
The heart is enclosed within the pericardium or pericardial sac. The pericardium consists of the fibrous pericardium at the periphery, and a double-walled serous sac, the serous pericardium, between the fibrous pericardium and the heart. The parietal lamina of the serous pericardium intimately lines the fibrous pericardium, whereas the visceral lamina of the serous pericardium intimately covers the heart and becomes the epicardium. Between the two serous laminae is the pericardial cavity, which contains fluid that acts as a lubricant, allowing the heart to beat freely (Figure 10.4). The fibrous pericardium is covered by the pericardial pleura, the continuation of the mediastinal pleura. The mediastinal pleura was first noted when the chest was cut open in the dissection of the digestive system.
Complete the following steps in the dissection procedure using a cat’s heart and a sheep’s heart as indicated.
1. Using the cat, observe the pericardial sac surrounding the heart. Make a tiny incision in the sac at the apex of the heart. Using your scissors, cut up through the pericardial sac to the heart’s base and fold the sac above the heart and out of the way. Find on the cranial surface of the heart a red paraconal artery, which is a branch of the left coronary artery traversing the heart in the paraconal interventricular groove.
We look for these arteries in the cat’s heart because they are not injected with latex in the sheep’s heart (Figure 10.5).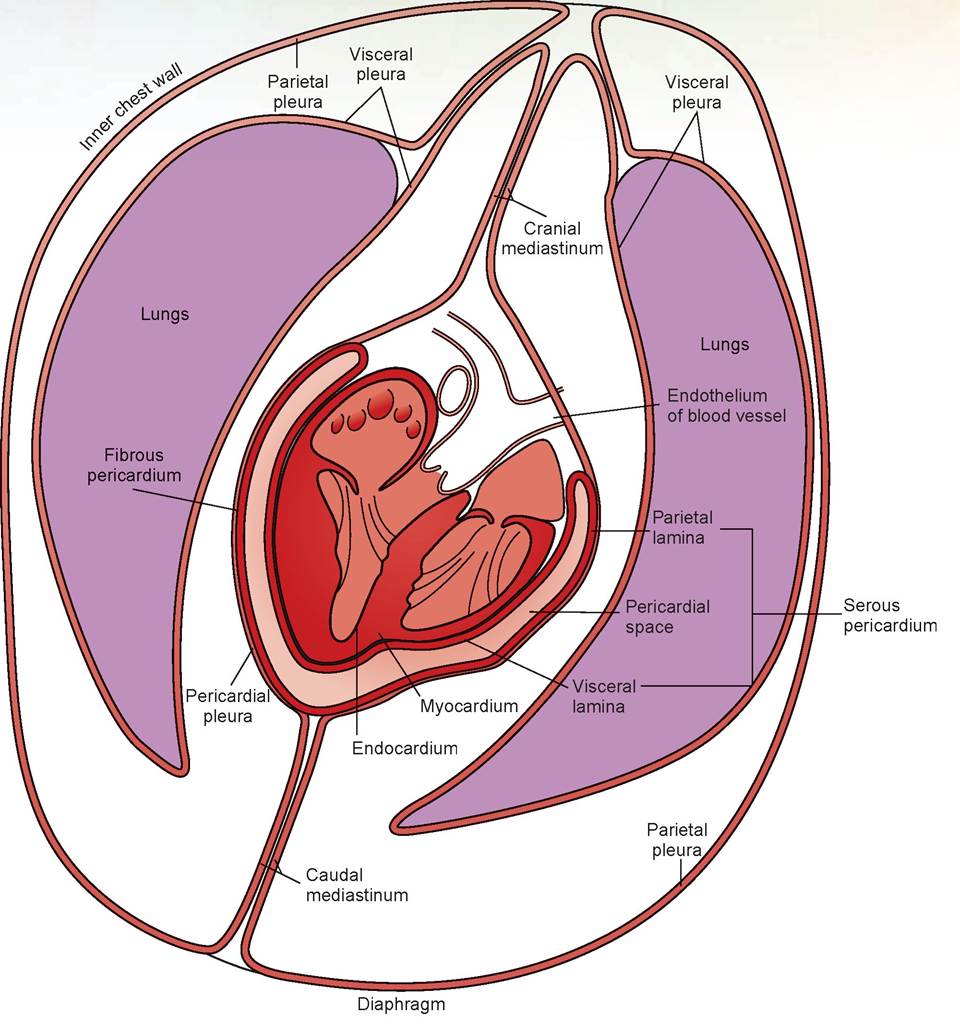
FIGURE 10.4: The pericardial sac and thoracic pleura.
2. Now obtain a sheep’s heart and rinse it in water to remove as much preservative as possible. If present, observe the pericardium around the sheep’s heart. Figure 10.6 illustrates all the layers of the heart and pericardium. The sheep’s heart will be used for the remaining steps in this exercise.
3. If the pericardium has not been removed, remove it from the heart, being especially careful to dissect it from the vessels at the base of the heart. If it has been removed, look for the remnants of this membrane attached to the large blood vessels above the heart.
4. There are three layers to the heart: the epicardium, myocardium, and endocardium (Figure 10.6). Separate a small portion of the epicardium (the visceral layer of the serous pericardium) from the myocardium (the muscle layer) by careful dissection with a scalpel. The third layer of the heart, the endocardium, will be visible when the heart is opened.
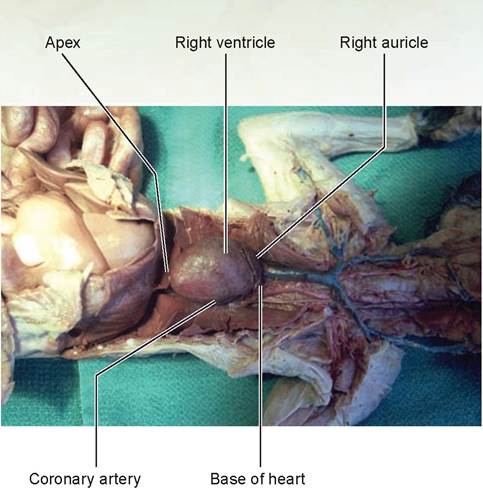
FIGURE 10.5: Heart position in the thorax of a cat.
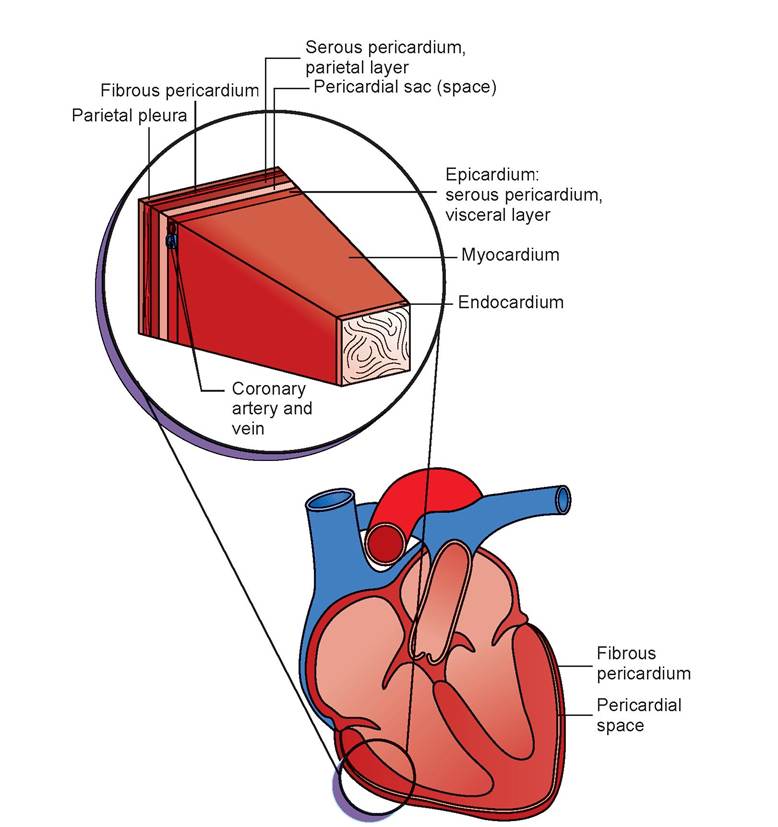
FIGURE 10.6: The layers of the heart.
5. Start the dissection by locating the pulmonary artery on the Cranioventral left surface of the heart (Figure 10.7A). This artery emerges from the cranial surface of the heart at the base, medial to the left auricle. The simplest method of identifying the ventral left surface of the heart is to look for the paraconal interventricular groove, which separates the right ventricle from the left ventricle. In this groove lies the paraconal artery, a branch of the left coronary artery.
Turn the heart over and look at the caudal surface. Another coronary artery runs down the middle and angles to the rightjust above the apex. This is the subsinuosal artery. This is where the coronary vascular system in domestic animals differs from species to species. In carnivores and ruminants, the subsinuosal artery is a branch of the left coronary artery (see Figure 10.7B). In the horse and pig, the subsinuosal artery arises from the right coronary artery (see Figure 10.7C). The right coronary artery can be located beneath the right auricle as that artery circles the heart.
The coronary venous system of the heart on the left cranial side includes the paraconal vein, which joins the great cardiac vein to enter the coronary sinus as it courses within the coronary groove beneath the left auricle. On the right lateral side is the subsinuosal vein. It lies in the subsinuosal interventricular groove and joins the coronary sinus as it courses toward the base of the heart. It does this in all species. Adjacent to the right coronary artery beneath the right auricle is the small cardiac vein.
6. Insert the handle end of a probe through the pulmonary artery and down into the right ventricle. Note that the distance to the bottom of this ventricle is approximately half the distance to the apex. There are several ways to know you are in the right ventricle: the chamber of the right ventricle does not go all the way to the apex; the myocardial wall is thinner when compared to the left ventricle; and within the chamber there is a cord that attaches the inner wall to the outer, called the trabecula septomarginalis (old name: moderator band) (see Step 15).
7. Using scissors, make a cut through the ventral wall of the pulmonary artery into the right ventricle. Continue the cut parallel to and 1 cm to the right of the paraconal interventricular groove (Figure 10.8). If you are too far from this groove, you will cut structures within the heart.
8. Continue the cut around the bottom of the right ventricle and up the opposite wall (still staying 1 cm from the edge of the wall) through the opening of the caudal vena cava (Figure 10.9).
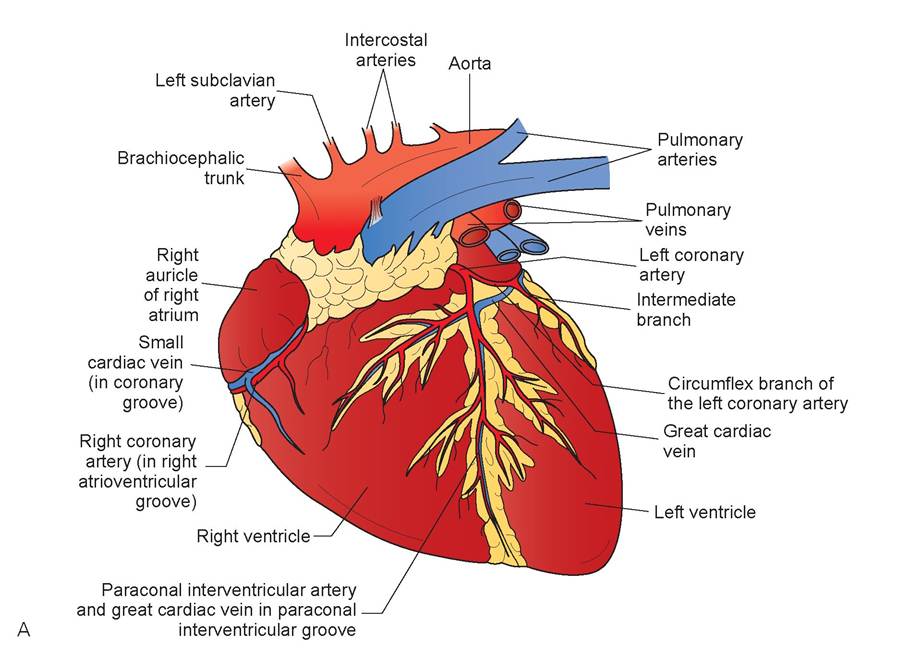
FIGURE 10.7: A. Left lateral view of the coronary circulation of the heart, all species.
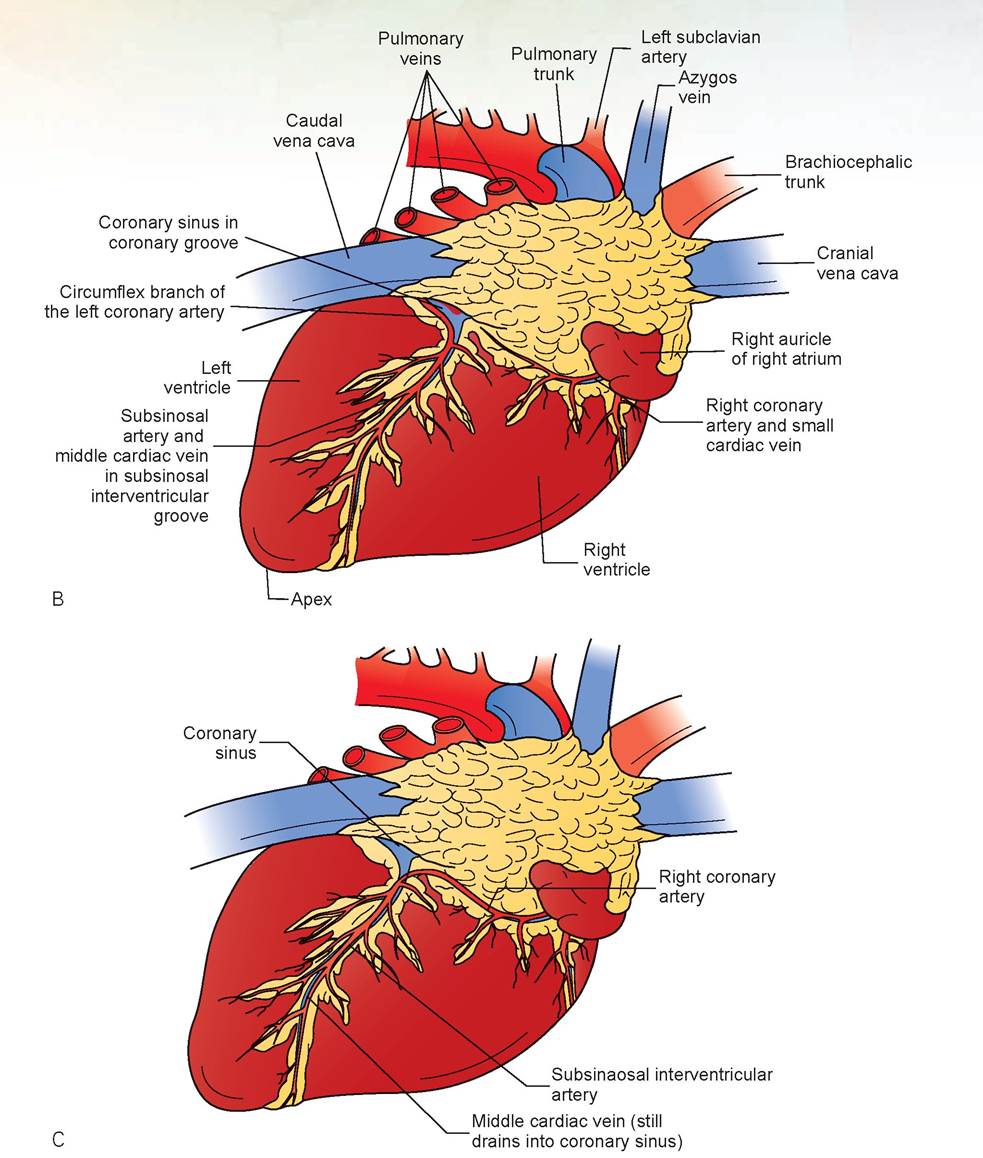
FIGURE 10.7, cont'd: B. Right lateral view of the coronary circulation of the heart in carnivores and ruminants. The subsinuosal artery is a continuation of the circumflex artery (a branch of the left coronary artery). C. Right lateral view of the coronary circulation of the heart in horses and pigs. The subsinosal artery is a continuation of the right coronary artery rather than the left coronary artery.
9. Pry open the pulmonary artery and observe the pulmonary valve. It should have two intact crescentshaped semilunar valvules, with the third incised by the cut you just made (see Figure 10.8).
10. From the caudal opening of the caudal vena cava, insert your finger or probe into the right atrium dorsally and caudally and find the opening of the cranial vena cava. These two large vessels are
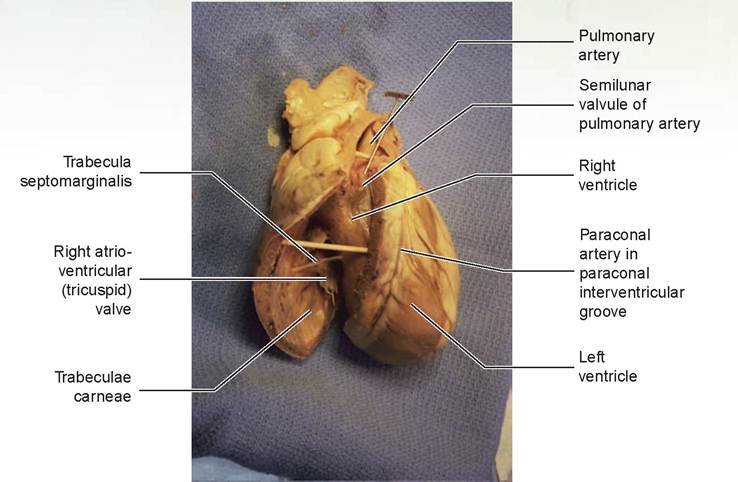
FIGURE 10.8: Proper cut through the pulmonary artery and right ventricular wall in a sheep heart
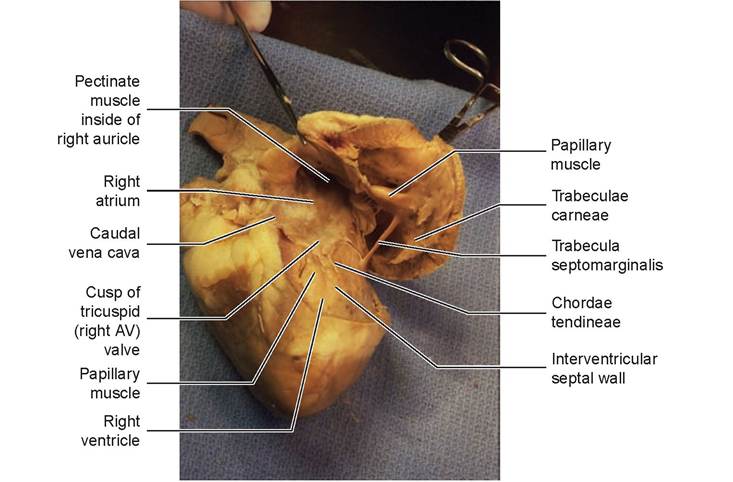
FIGURE 10.9: Right atrium and ventricle. The previous cut is continued around the ventricle and dorsally to join the entrance of the caudal vena cava.
the routes for blood returning to the heart from the cranial and caudal halves of the body(see Figure 10.9).
11. Open the right ventricle as shown in Figure 10.9, and look into the area of the right atrium and auricle. First observe the internal structure of the right auricle, the flap-like or ear-like (auricle means ear) structure seen from the exterior of the heart. The web-like arrangement of muscles on the interior of the auricle is made of multiple pectinate muscles, so called because they resemble a comb (pecten).
12. Locate the orifice of the coronary sinus, just below the caudal vena cava. It is a small canal-like tube that courses around the heart between the atria and the ventricles in the groove just under the auricles.
13. Examine the tricuspid valve, or right atrioventricular (AV) valve, between the right atrium and right ventricle. Count the number of cusps, or flaps, that make up this valve. From the name, you should determine that it has three cusps.
14. Locate the papillary muscles and the attached chordae tendineae in the wall of the right ventricle. The papillary muscles exert tension on the cusps of the valve during the contraction of the ventricles, thereby preventing the valves’ eversion into the atria.
15. Find the trabecula septomarginalis crossing the lumen of the right ventricle. This is thought to prevent overdistension of the ventricle. Also note the trabeculae carneae, myocardial ridges projecting mainly from the outer wall and running toward the apex (in both ventricles).
16. Find the aorta. This is the large, thick-walled vessel coming from the left ventricle. It can be found by inserting the handle of the probe into the remaining large vessel at the base of the heart and on into the left ventricle. Insert one side of the scissors deep into the aorta and down into the ventricle. If you encounter resistance, pull out slightly and reposition the scissors (because you probably have slipped into one of the cusps of the aortic valve). With your opposite hand, rotate the pulmonary artery out of the way, position the visible side of the scissors under this artery, and make a longitudinal cut through the aorta and ventricle to the apex (Figure 10.10).
17. Try to find the pulmonary veins entering the left atrium. This may be possible in hearts that have the pericardium still attached, but if it has been removed, often there is just a large hole in the dorsum, or top, of the atrium where these vessels once entered the heart.
18. Locate the most ventral and lateral of the pulmonary veins, or the most ventrolateral point on the opening into the left ventricle. Make a longitudinal incision through this pulmonary vein or
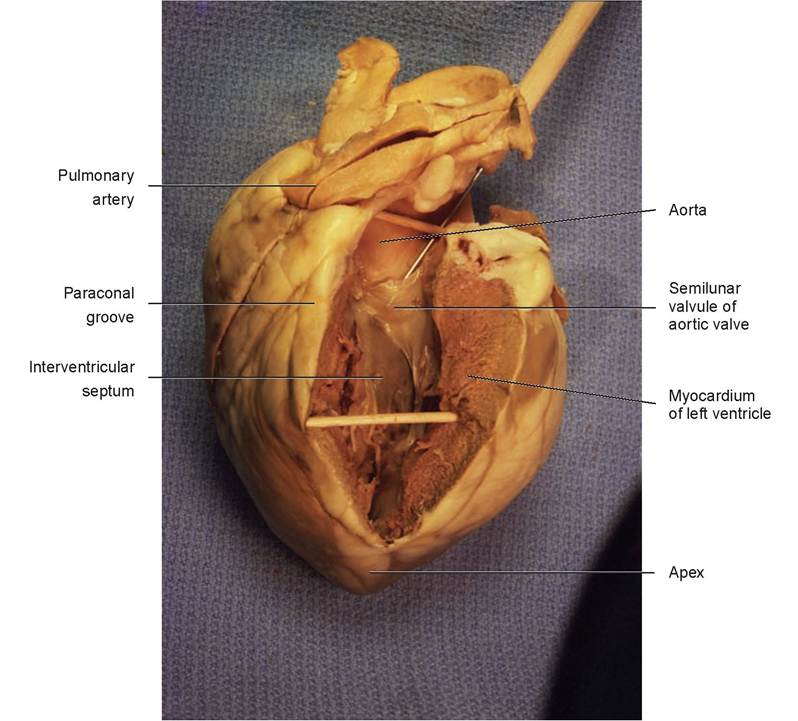
FIGURE 10.10: Proper cut through the aorta and left ventricular wall.
Copyright 2010 Cengage Learning. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. Due to electronic rights, some third party content may be suppressed from the eBook and/or eChapter(s).
Editorial review has deemed that any suppressed content does not materially affect the overall learning experience. Cengage Learning reserves the right to remove additional content at any time if subsequent rights restrictions require it. opening, staying at least 2 cm from the previous cut (which was actually through the left lateral wall of the heart). Continue this incision through the wall of the left atrium and the left ventricle to the apex, where it should join the previous cut (Figure 10.11).
19. Spread open the left side of the heart (see Figure 10.11). Compare the wall thickness of the left ventricle with that of the right. Observe the bicuspid valve, or left atrioventricular (AV) valve. This valve has two major cusps; hence the name bicuspid valve. Veterinarians often call it the mitral valve. Note that this ventricle also has chordae tendineae and papillary muscles, but no trabecula septomarginalis.
20. Look into the left atrium and note that it also has pectinate muscles within the left auricle. Locate the interatrial septum, the wall that separates the two atria. This is best accomplished by grasping the heart with your thumb in the right atrium and your index finger in the left atrium (or vice versa); if you pinch your thumb and finger together, that will be where the interatrial septum is located. Now examine this septum from the interior of the right atrium. Locate the fossa ovalis, the oval-shaped depression ventral to the entrance of the cranial vena cava. At one time this was a portal through which the fetal blood (containing oxygen from the placenta) by-passed the pulmonary circulation and flowed into the left side of the heart to be pumped to the body (see Figure 10.1B).
21. Spread apart the cut made through the aorta into the left ventricle (see Figure 10.10). Note the valve between these two structures; like the pulmonary valve it also has three moon-like, crescentshaped valvules and is called the aortic valve.
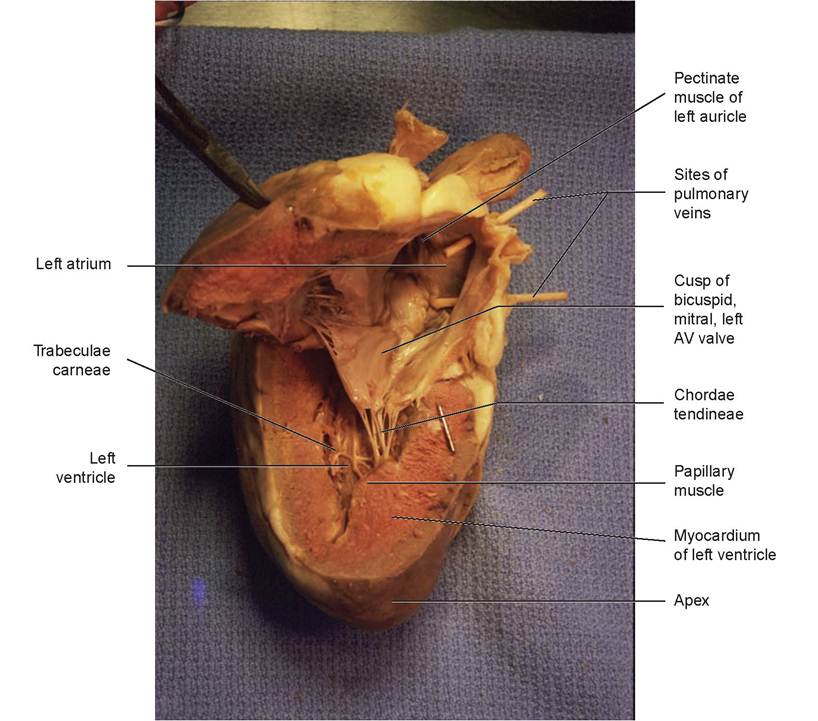
FIGURE 10.11: Left atrium and ventricle. The cut is made toward the apex through one pulmonary vein hole on the lateral side and connects with the previous cut at the apex of the heart.
Part Two: The Vascular System
The blood-vascular system is a closed transport system; blood leaves the heart in arteries and returns via veins. Veins contain venous blood, which is generally deoxygenated, and arteries contain arterial blood, which is generally oxygenated. There are two exceptions to this general rule for both the venous and arterial systems. In the venous system, the pulmonary vein(s) returning from the lungs contain oxygenated blood, as does the umbilical vein of the fetus, which returns oxygenated blood to the fetal heart. This oxygen is picked up from the mother as blood courses through the placenta (see Figure 10.1B). Conversely, in the arterial system, the pulmonary arteries taking blood to the lungs, and the umbilical artery taking blood to the placenta, contain deoxygenated blood.
The flow of blood through the vascular system starts with the arteries. As the arteries branch and enter tissues, they get smaller and become arterioles, which are the smallest arteries. From there they become capillaries, and a network of capillaries within tissue is called a capillary bed. This is the site of internal respiration, where the nutrients and oxygen enter the cells of tissues, and carbon dioxide (CO2) is removed to the blood according to the following formula:

Most of the CO2 combines with water to produce carbonic acid, which rapidly dissociates into hydrogen ions and bicarbonate ions. The hydrogen ions combine with the blood’s hemoglobin, which has released its oxygen to tissues, thus forming reduced hemoglobin that acts as a buffer. Most of the bicarbonate ions are carried inside the red blood cells, but some diffuses out into plasma, and chloride diffuses in. Approximately 21% of the carbon dioxide combines with the amino groups on hemoglobin to form carbaminohemoglobin. Another 7% is dissolved in plasma. Once the blood reaches the lungs, the reaction reverses itself, and CO2 passes from the capillary blood into the alveoli and then is exhaled. Simultaneously, oxygen enters the blood and is picked up by the red blood cells and hemoglobin within. This shows the close relationship between the blood-vascular system and the respiratory system.
Capillaries are microscopic tubes composed almost entirely of simple squamous epithelium. These were examined in the histology section of Chapter 5, Figure 5.3. Blood exits the capillaries and enters the smallest veins, called venules, which then unite to form larger veins and return the blood to the heart.
The walls of blood vessels, except for the capillaries, have three layers, or tunics (Figure 10.12). The tunica interna (or tunica intima) lines the lumen of the vessel and is composed of a thin layer of simple squamous epithelial cells, also called the endothelium (squamous cells underlain by a scant basal lamina). It is continuous with the endocardium of the heart. The cells of this layer fit closely together, forming an extremely smooth inner lining that helps to decrease resistance to blood flow.
The tunica media is the thicker middle layer of blood vessel walls and is composed primarily of smooth muscle and elastin. The smooth muscle is under the control of the sympathetic nervous system, a component of the autonomic nervous system. It plays an active role in regulating the diameter of the blood vessels, which controls the peripheral resistance and thus blood pressure.
The tunica externa (or adventitia) is the outermost tunic and is composed of areolar, or fibrous, connective tissue. Its function is basically support and protection.
In general, the walls of the arteries are thicker than those of the veins because their tunica media have more smooth muscle and elastin. Arteries and arterioles in tissue sections appear round, whereas the venules and veins are larger and can take on a variety of elliptical shapes during the sectioning of tissues. The larger veins have valves, usually two paired cusps placed at irregular distances along the vessels. They direct blood to flow only toward the heart and prevent backflow. Horses’ legs do not have valves in their veins—instead they depend on the pumping action of the horse’s weight and movement on the hooves to move the blood up the legs.
Arteries, because they are closer to the pumping action of the heart, must expand as blood is propelled into them and then recoil passively as the blood continues on its path into circulation during diastole. The systolic blood pressure is the pressure within the arterial system at the peak of systole and is controlled by two factors: (1) peripheral resistance (based on the diameter and elasticity of the vessel) and (2) stroke volume of the heart (how much blood is pumped out perheartbeat). Diastolic blood pressure (when the heart is relaxed) is controlled only by peripheral resistance. If arteries did not have elasticity (no elastin), were built similar to veins, and could not passively recoil, blood pressure would drop precipitously during diastole. Conversely, if arteries lose their elasticity (via sclerosis or hardening) and cannot stretch, blood pressure rises during both systole and diastole. This condition is known as hypertension. Excessively low blood pressure is known as hypotension.
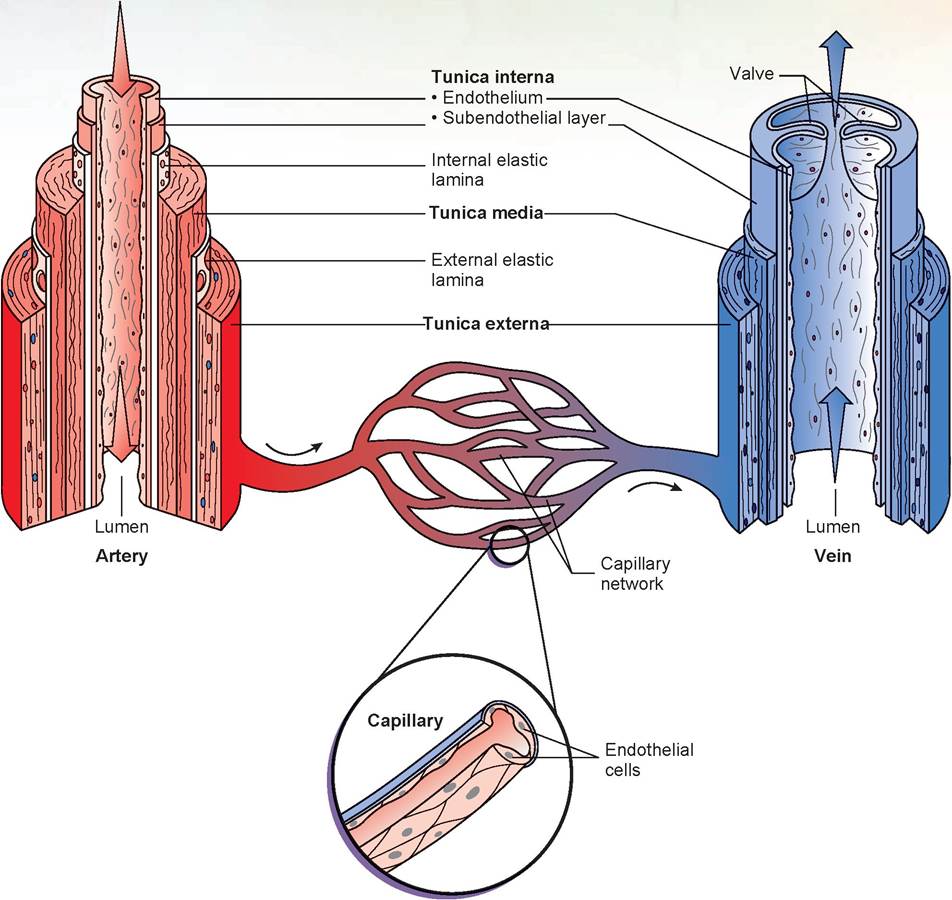
FIGURE 10.12: Structure of arteries, veins, and capillaries.
EXERCISE 10.2 DISSECTION OF THE ARTERIES AND VEINS
During this dissection, be careful to not damage the kidneys, ureters, uterus, ovaries, ductus deferens, or the vessels to these structures. Also take care not to damage any nerves. Use both the diagrams and the photos shown in the figures to determine the locations of the veins and arteries during your dissection. With the exception of the pulmonary veins, the veins will be injected with blue latex for ease of dissection and identification.
Part A: Dissection of the Veins
1. Using the cat, look at the pericardium surrounding the heart. After determining the location of its attachment, remove the parietal layer, the thymus gland, and any lymph nodes in the cranial thorax. Remember that the visceral layer of the pericardium forms the epicardium of the heart. Figure 10.13 illustrates the important veins that will be identified during dissection.
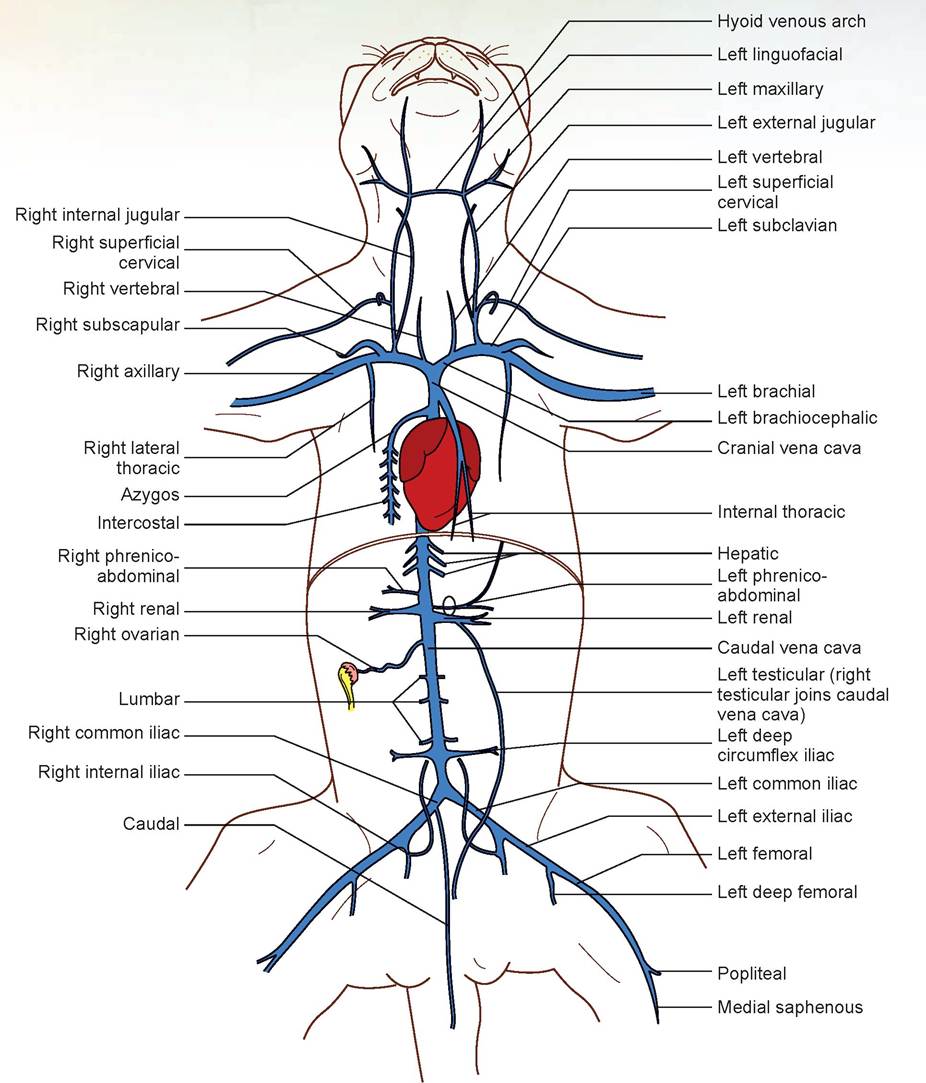
FIGURE 10.13: Venous system of the cat.
2. Find the cranial vena cava, the large blue vessel entering the cranial aspect of the right atrium. This vein returns blood from the head, neck, and front legs.
3. Lift up the heart and cranial vena cava and carefully dissect away any tissue found beneath the cranial vena cava. The azygos vein can be seen entering the dorsal surface of the cranial vena cava immediately cranial to the heart (Figure 10.14). Lift up the right lung; the azygos vein is now visible on the right side against the vertebral column. The tributaries of the azygos vein are the intercostal veins from the body wall, the esophageal veins, and the bronchial veins. It is difficult to find the esophageal and bronchial veins if they are not injected with latex, which they may not be.
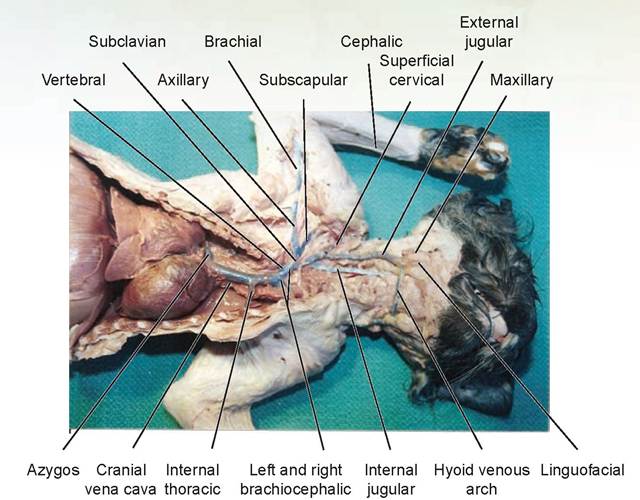
FIGURE 10.14: Cranial venous system of the cat.
4. Trace the cranial vena cava forward; note that it is formed by the union of the two brachiocephalic veins (see Figures 10.13 and 10.14).
5. The cranial vena cava also receives the internal thoracic vein from the ventral chest wall. The right and left internal thoracic veins unite shortly before they empty into the cranial vena cava. In some cats the right vertebral vein from the brain might enter the dorsal surface of the cranial vena cava, but in most cats it enters the right brachiocephalic vein (see Figures 10.13 and 10.14).
6. Trace both brachiocephalic veins forward. The left brachiocephalic vein receives the left vertebral vein. The vertebral veins come from the vertebrae and thus can be traced only a short distance dorsally in your dissection. Both brachiocephalic veins are formed by the union of the external jugular veins, which drain the head, and the short subclavian veins, which drain the front legs (see Figures 10.13 and 10.14).
7. Start tracing the external jugular vein toward the head. The first branch is the smaller internal jugular vein, and it joins immediately above the point of union of the external jugular with the subclavian. The internal jugular vein, which drains the brain, lies next to the left common carotid artery near the trachea. Another vessel, which is often difficult to locate, is the thoracic duct. It is a large lymphatic vessel that originates in the cranial portion of the sublumbar region and courses ventral to the vertebral column into and through the thorax between the aorta and azygos vein, specifically on the right dorsal border of the aorta and ventral border of the azygos vein. It empties into the external jugular at the point of union of the external jugular with the subclavian. Sometimes this duct may appear blue, if latex was forced into it, or brown and beaded (because of its valves) if it is empty. Continue tracing the external jugular vein toward the head. The large superficial cervical vein (formerly known as the transverse scapular vein) empties into the external jugular (see Figures 10.13 and 10.14).
8. The external jugular vein is formed by the union of the maxillary vein (the dorsal branch) and the linguofacial vein (the ventral branch)just caudal to the point of the mandible. The hyoid venous arch can be seen connecting the two external jugular veins at this point (see Figures 10.13 and 10.14).
9. We will use the left side of the cat to dissect the vascular system, and the right side for the nerves. If both the arteries and veins on the right side have superior latex injection (as was the situation in the photo of the cat in Figure 10.14), use that side. However, if on one side the arteries are better injected and on the other the veins are better injected, use both sides for the dissection. Just be sure not to damage any nerves as you do this.
Trace the left subclavian vein through the chest wall. It receives the subscapular vein from the shoulder a short distance from the site where it joins with the external jugular. Distal to where the subscapular vein joins, the continuation of the subclavian is called the axillary vein. When the axillary vein attaches to the muscles of the front leg, it becomes the brachial vein. The cephalic vein lies on the cranial surface of the foreleg, coursing up the leg and dividing at the elbow joint (see Figure 10.14). It continues up the cranial surface of the upper leg as the cephalic vein, whereas the other branch, the superior brachial vein, passes medial to the humerus to course adjacent to the superficial brachial artery and join the brachial vein (see Figures 10.13 and 10.14). The cephalic vein may join the superior cervical vein or enter the external jugular on its own.
10. Raise the apex of the heart and spread the lung lobes apart so you can find the caudal vena cava. Trace this vessel from the diaphragm cranially to where it drains into the right atrium. This large vein drains the lower part of the body.
11. Continue to trace the caudal vena cava caudally through the diaphragm and into the abdominal cavity, where it lies to the right of the aorta. To see this vein and its tributaries, dissect away the peritoneum because the caudal vena cava and the aorta are retroperitoneal. The tributaries usually accompany the arteries of the same name.
12. The hepatic veins drain blood from the liver into the caudal vena cava. To locate these veins, use a probe or a scalpel blade to gently scrape away tissue on the right cranial surface of the liver. Several hepatic veins may be located in this manner.
13. The phrenicoabdominal veins (formerly known as adrenolumbar veins) drain the adrenal glands and the body wall. The right vein drains into the caudal vena cava, and the left may either drain into the caudal vena cava or into the renal veins. These veins may be located by examining the dorsal muscle wall cranial to the kidney (see Figures 10.13 and 10.15).
14. Locate the renal veins, which carry blood from the kidneys into the caudal vena cava. Note that the right kidney, and thus the right renal vein, is more cranial than the left one. Do all the dissection on the left kidney, leaving the right kidney intact under the peritoneum for later dissection. Also note the white ureters exiting from the kidney and traversing retroperitoneally toward the bladder. Find these, but do not cut them (see Figures 10.13 and 10.15).
15. Caudal to the renal veins are the long, thin, paired ovarian veins or testicular veins. They are most easily located by tracing the vessels from the gonads back toward the caudal vena cava. If the cat is a female, locate the ovaries, small oval bodies near the cranial ends of the uterus, below the kidneys. The ovarian artery and vein should be visible. If the cat is a male, the testicular vein, artery, and ductus deferens can be seen passing through the inguinal canal (the opening in the caudal abdominal body wall).Trace these blood vessels cranially toward the aorta and caudal vena cava. In the cat, the left testicular and ovarian veins enter the left renal vein; on the right they enter the caudal vena cava (see Figures 10.13 and 10.15).
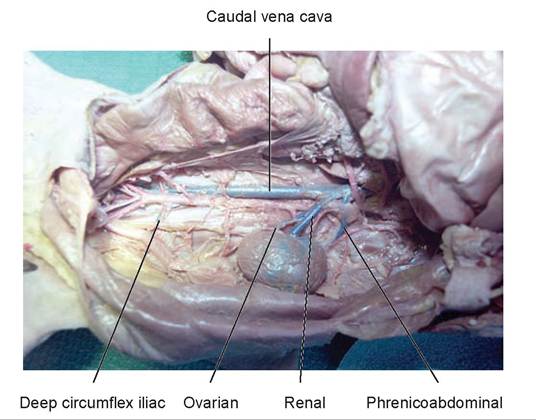
FIGURE 10.15: Veins of the mid-abdominal dorsal wall of the cat.
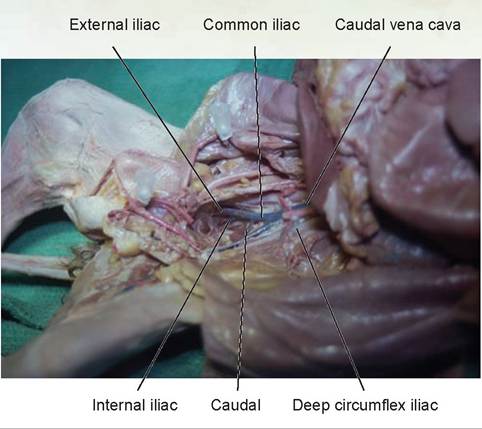
FIGURE 10.16: Veins of the caudal abdomen of the cat.
16. Several pairs of lumbar veins enter the dorsal surface of the caudal vena cava at intervals in the abdominal cavity. Spread the dorsal median musculature apart and lift the caudal vena cava gently to reveal these veins.
17. The right and left deep circumflex iliac veins (formerly known as iliolumbar veins) enter the caudal vena cava near its termination. These vessels drain the abdominal wall muscles (see Figures 10.13 and 10.15).
18. The common iliac veinsjoin to form the caudal vena cava (see Figures 10.13 and 10.16).Trace the route of the common iliac veins toward the hind legs. On the left side, the first vessel joining this vein is the internal iliac vein, which drains the rectum, bladder, and internal reproductive organs. The common iliac vein continues distally from this point as the external iliac vein. When it passes out of the body wall, it is the femoral vein. There is a slight variation on the right side; the first vein to join the common iliac is the caudal vein, a short distance from the caudal vena cava (see Figures 10.13 and 10.16). Trace the femoral vein to its formation by the medial saphenous vein superficially and the popliteal vein from deep between the muscles (see Figures 10.13 and 10.17). If this vein were to be traced to the lateral side of the leg, you would note that it is formed by the cranial tibial vein and the lateral saphenous vein.
19. The hepatic portal system may or may not be injected; if it is, it will be injected with yellow latex (Figure 10.18). A portion of the portal vein was dissected in a previous chapter with the digestive system (see Figure 9.19 in Chapter 9). As mentioned previously, a portal system is a vessel between two capillary beds—in this case, between the capillaries of the digestive organs and those of the liver. Thus, the portal veins carry blood from the digestive organs to the liver. As you follow the portal vein caudally, note that it is formed by the union of the splenic vein (formerly known as the gastrosplenic vein) from the stomach and spleen, and the larger cranial mesenteric vein coming in caudally from the small intestine. Two veins join the cranial mesenteric just dorsal to the mid-pancreas area: the pancreaticoduodenal from the pancreas and duodenum, and the caudal mesenteric from the colon.
Part B: Dissection of the Arteries
With the exception of the pulmonary arteries, the arteries will be injected with red latex for ease of dissection and identification.
1. Locate the pulmonary artery emerging from the cranioventral surface of the heart. Because it is attached to the right ventricle, it will be filled with blue latex. Trace its path to the lungs, noting that it branches into the right and left pulmonary arteries. Figure 10.19 illustrates the important arteries identified during dissection.
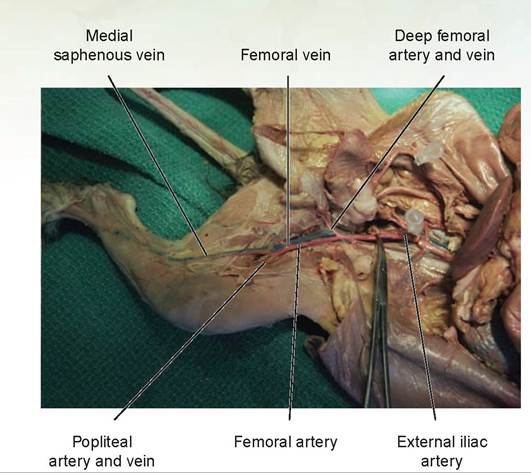
FIGURE 10.17: Medial view of the vessels of the hind leg of a cat.
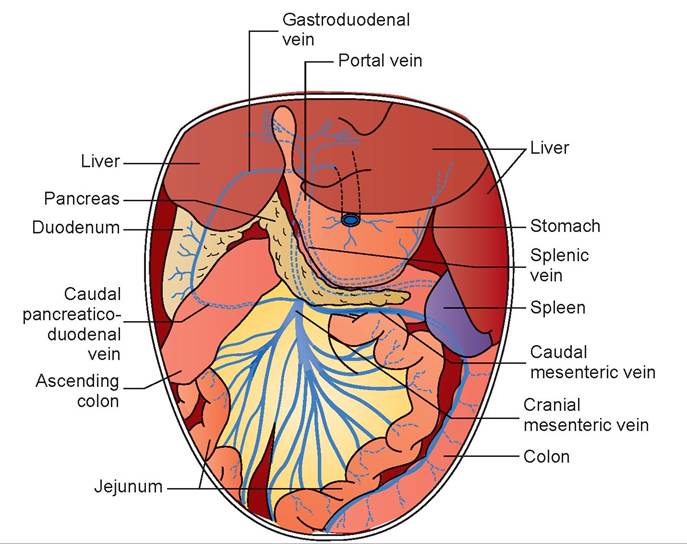
FIGURE 10.18: Hepatic-portal venous system in dogs and cats.
2. Move the right auricle to the right to see a large, white artery called the aorta emerging from the left ventricle and passing beneath the pulmonary artery; its path forms an arch that moves dorsally and to the left above the heart. The arch is known as the aortic arch. When the aorta becomes attached to the dorsal thorax, it is called the thoracic aorta. This is injected with red latex, but due to the thickness of the wall of the aorta, the color often cannot be seen (do not remove the wall of the aorta in your dissection).
3. The first major branch off the aortic arch is the brachiocephalic trunk, or brachiocephalic artery. Trace this vessel forward. The first branch off the brachiocephalic is the left common carotid artery; it then branches into the right subclavian artery and the right common carotid artery (Figures 10.19 and 10.20).
4. Follow the path of the left common carotid artery. It ascends cranially in the neck, coursing between the small internal jugular vein and the trachea. As you follow it cranially, you will note some small branches arising from this artery, such as the caudal thyroid artery, which is often hard to find and usually is not injected (see Figures 10.19 and 10.20). The first major branch to locate is the cranial
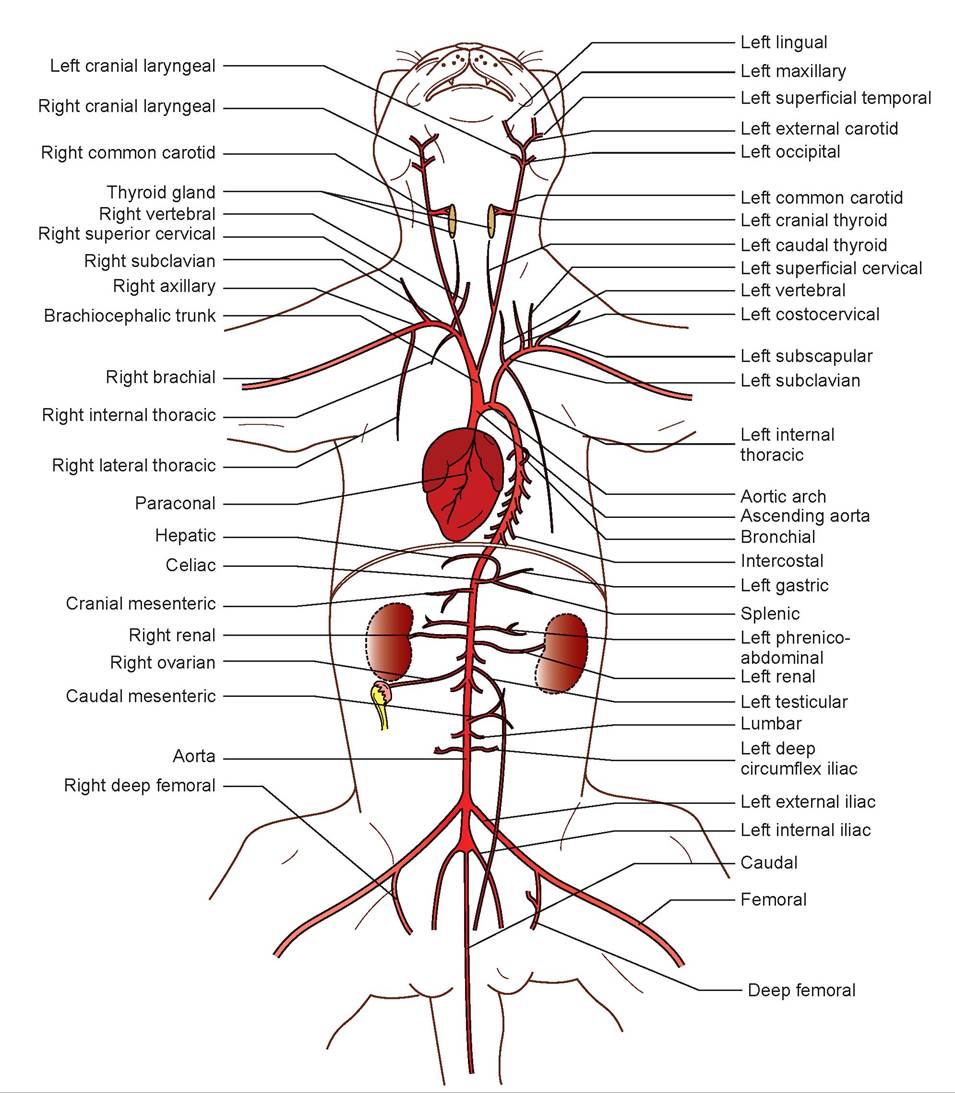
FIGURE 10.19: Arterial system of the cat.
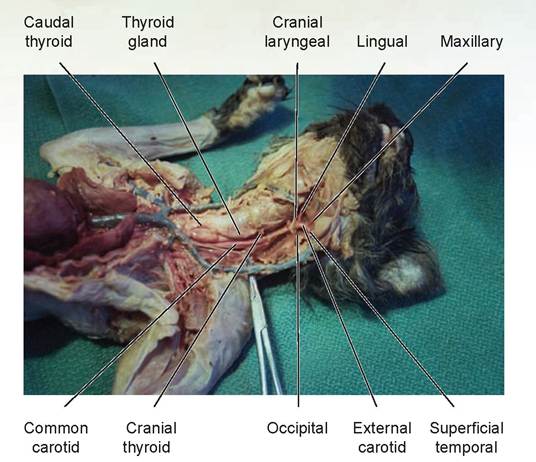
FIGURE 10.20: Cranial arterial system of the cat.
thyroid artery, which originates at the level of thejunction between the trachea and the cricoid cartilage. It supplies blood to the thyroid gland and muscles of the larynx. The next two branches off the common carotid are the occipital artery, which courses dorsally and supplies the back of the neck, and the cranial laryngeal artery, coursing ventrally to the larynx. The next branch is the lingual artery, which courses ventral and cranially. After this branch, the artery continues dorsocra- nially as the external carotid artery.
In the cat, the internal carotid artery is extremely small and need not be located. (It emerges from the common carotidjust cranial to the occipital artery and courses dorsally.) The external carotid divides into the superficial temporal artery, coursing dorsally and supplying the parotid salivary gland and local musculature, and the maxillary artery, coursing ventrocranially and branching into numerous other arteries that deliver blood to the maxilla and mandible (see Figures 10.19 and 10.20).
5. Return to the aortic arch and locate the left subclavian artery, the next branch off the aortic arch just to the left of the brachiocephalic artery. This artery supplies the left side of the chest and left front leg. Locate each of the following arteries. The left subclavian artery emits two branches, a ventrally oriented internal thoracic artery and a dorsocranial oriented vertebral artery. The next branch emitted also oriented dorsocranially is the costocervical trunk. The subclavian becomes the axillary artery as it proceeds ventrolaterally cranial to the first rib. The axillary artery then emits the ventrocranial oriented superficial cervical artery (see Figures 10.19 and 10.21). Its next major branch is the craniolateral oriented Left subcscapular artery.
6. The internal thoracic artery goes to the sternum and supplies blood to the ventral intercostal muscles. Note that it joins its corresponding vein. The left vertebral artery courses dorsally to the vertebrae and cranially to supply the brain, The costocervical trunk and the deep cervical artery (on occasion you may find this artery next to the costocervical trunk) supply most of the neck and some of the back muscles.
7. Next the superficial cervical artery, which ascends for a short distance and then branches, supplies some of the neck and shoulder muscles. The subscapular artery initially courses cranially but turns laterally to supply the muscles of the subscapular and caudal aspect of the scapula.
8. When the axillary artery becomes attached to the musculature of the front leg, it is known as the brachial artery. Follow the brachial artery until it branches to form the superficial brachial artery
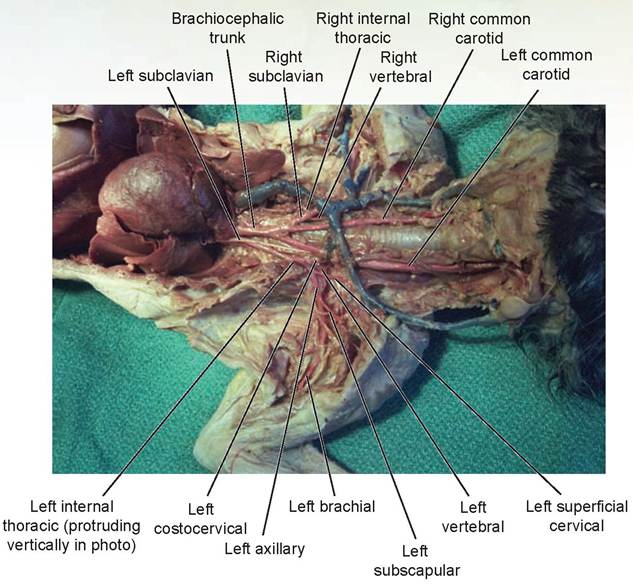
FIGURE 10.21: Cranial thoracic and appendicular arterial systems of the cat.
and the median artery. The superficial brachial gives off the collateral ulnar artery which courses toward the medial aspect of the olecranon process. Just distal to the elbowjoint on the medial aspect of the leg, the median artery gives off the ulnar artery which courses caudally and medial to the ulna. Just proximal to the carpus, the median artery gives off the radial artery, which courses medially across the carpal bones and continues caudally and medially to the accessory carpal bone. All of these arteries together supply the forearm. On the right side, the right vertebral artery emerges from the right subclavian just distal to the point at which the right common carotid artery emerges (see Figures 10.19 and 10.21). Also note the superficial cervical artery is the first branch off the axillary as it enters the axilla.
9. Returning to the aortic arch, trace the aorta caudally. Pull the viscera in the thorax to the right to expose the aorta in the thoracic cavity. As this vessel passes through the thorax it is called the thoracic aorta. Remove the pleura to expose this vessel in the thorax.
10. Note the intercostal arteries emerging from the thoracic aorta to supply the intercostal muscles. In addition, there are several bronchial arteries, which supply the lungs, and esophageal arteries, which supply the esophagus.
11. As the aorta emerges above the diaphragm, its first major branch from the abdominal aorta is the short celiac artery. Dissect away the fat and peritoneum that cover the cranial aspect of the abdominal aorta to locate this artery. The celiac artery divides into three branches: first is the hepatic artery, coursing dorsal to the stomach and to the liver; immediately distal to this is the left gastric artery, supplying the lesser curvature and cranial stomach; then the artery continues as the splenic artery, the largest of the branches, and goes to the spleen (see Figures 10.19 and 10.22). The hepatic artery branches into the right gastric, gastroduodenal, and cranial pancreatoduodenal arteries on its path to the liver. The hepatic artery was located previously in the lesser omentum, to the left of the portal vein, during the dissection of the digestive system (see Chapter 9, Figure 9.19).
12. A short distance caudal from the celiac artery is the cranial mesenteric artery (see Figures 10.19 and 10.22). It supplies the small intestine and a portion of the large intestine.
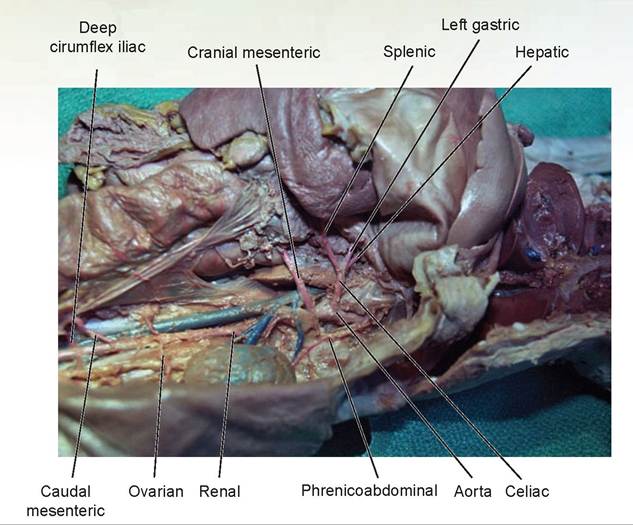
FIGURE 10.22: Mid-abdominal arteries in a cat.
13. The paired left and right phrenicoabdominal arteries (formerly known as the adrenolumbar arteries) course from the aorta to the dorsal body wall (see Figures 10.19 and 10.22). They supply the adrenal glands, diaphragm, and muscles of the body wall.
14. The next pair of arteries are the renal arteries, which supply the kidneys (see Figures 10.19 and 10.22).
15. Just caudal to the kidneys, off the abdominal aorta, the right and left testicular or ovarian arteries emerge (see Figures 10.19 and 10.22). These are small, thread-like arteries emerging from the ventral surface of the aorta. If your cat is a male, follow the testicular arteries from the inguinal canal to theaorta. The testicular artery supplies each testis. If your cat is a female, trace the ovarian arteries to the ovaries.
16. Push the descending colon to one side to see the single caudal mesenteric artery (see Figures 10.19 and 10.22). This arises from the ventral surface of the aorta a short distance from the previous testicular or ovarian arteries. It supplies the descending colon.
17. Lift the aorta gently to observe the lumbar arteries. There are approximately seven pairs of lumbar arteries emerging at intervals along the abdominal aorta in the cat. These supply the abdominal wall.
18. Another pair of arteries called the deep circumflex iliac arteries (formerly known as the iliolumbar arteries) emerge next and course laterally to the dorsal caudal musculature (see Figures 10.19 and 10.23).
19. The aorta terminates in a series of branches, first the paired external iliac arteries, then the internal iliac arteries (see Figures 10.19 and 10.23). The external iliac becomes the femoral artery as it passes out through the body wall (see Figure 10.17). It courses next to its corresponding vein and branches with it; the nomenclature for these branches is the same as for the veins. The internal iliac artery supplies the gluteal muscles, rectum, and uterus.
20. The aorta terminates by branching into the small caudal artery, which courses down the median ventral surface of the sacrum and enters the tail (see Figures 10.19 and 10.23).
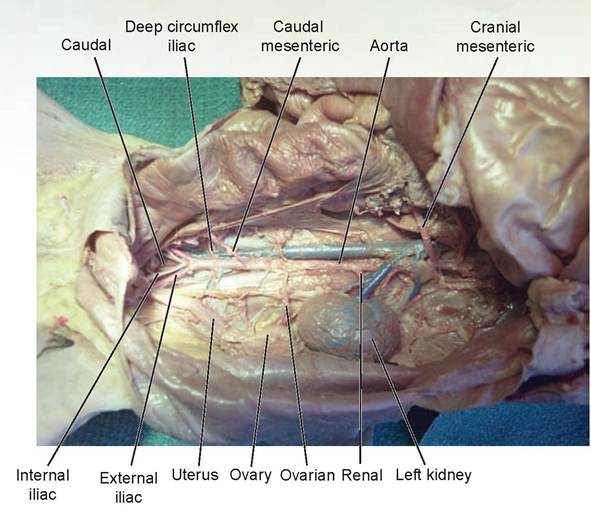
FIGURE 10.23: Caudal abdominal arteries in a cat.
The Electrocardiogram
An electrocardiogram is a recording of the electrochemical activity (depolarization waves) traveling through the heart immediately prior to each beat. The heart’s ability to beat is intrinsic, and thus it does not depend on impulses from the nervous system to initiate its contraction. The heart will continue to contract rhythmically even if all nerve connections are severed. However, because it is connected to the autonomic nervous system, this system has a controlling effect on the heart and can either increase or decrease the heart rate.
Within the heart is the intrinsic conduction system, or nodal system. This system consists of specialized noncontractile myocardial tissue, called purkinje fibers of the purkinje system, that conducts the wave of depolarization through the heart in an orderly, consistent, and sequential manner that enables the heart to beat as a coordinated unit. The definition of depolarization is the state of a neuron that occurs immediately after a sufficiently strong stimulus is applied and results in an influx of sodium ions. This changes the membrane potential from approximately —70 mV to +30 mV. Repolarization follows depolarization; during it, potassium
ions rapidly diffuse out of the neuron. This causes the membrane to return to its resting potential (see Chapter 15 for a more detailed explanation).
The sinoatrial node (the SA node), also called the pacemaker, has the highest rate of discharge and provides the stimulus to initiate the heartbeat. It also sets the rate of depolarization for the heart as a whole. The impulse then spreads across the both atria and is immediately followed by atrial contraction (atrial systole). The impulse then is picked up by the atrioventricular node (or AV node). At the AV node the impulse is momentarily delayed; in an animal with an average heart rate of 72 beats per minute, the delay is approximately 0.1 sec. It is shorter in animals with faster heart rates and longer in animals with slower heart rates. This allows the atria time to completely contract. From there the impulse passes through the AV bundle (or bundle of His) and splits into the right and left bundle branches as it travels down the interventricular septum. Branching off the bundle branches are numerous purkinje fibers attached to the myocardium, called terminal purkinje conducting fibers. The impulse passes through these fibers to initiate ventricular contraction (ventricular systole; Figure 10.24).
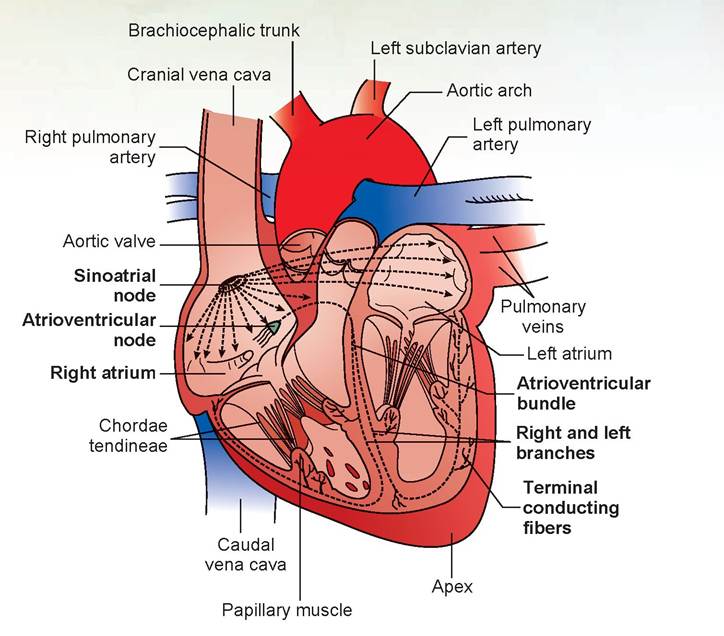
FIGURE 10.24: The intrinsic conduction system of the heart, all species.
The electrocardiograph records the electrical currents generated by the heart as they eventually spread through the body and are picked up by the machine’s electrodes. The electrocardiogram (ECG or EKG) records three main recognizable waves, called deflection waves. The first is the P wave, representing depolarization of the atria, which occurs immediately prior to atrial systole. The next is the QRS complex, representing ventricular depolarization, and it is immediately followed by ventricular systole. The third wave is the T wave, representing ventricular repolarization. A small atrial repolarization wave occurs at the same time as ventricular depolarization, and thus this wave is buried within the QRS complex (Figure 10.25).
The direction of the ECG deflection waves (up or down) depends on where the positive and negative electrodes are attached on the limbs of the patient. Traditionally, a dog lies in right lateral recumbency and has electrodes attached at the elbows and knees. The right knee is the ground electrode. Cats may be positioned like dogs or ster- nally. The electrocardiograph machine is able to change the polarity of the electrodes without having to move them. A typical ECG records three standard limb leads, three augmented limb leads,
and four or more chest leads. The three standard limb leads—Leads I, II, and III—record two of the electrodes during a reading. Lead I is positive on the left front leg and negative on the right front leg; Lead II is positive on the left hind leg and negative on the right front leg; and Lead III is positive on the left hind leg and negative on the left front leg. The augmented or unipolar leads, known as aVR, aVL, and aVF, compare the positive electrode to each of the standard limb leads. The chest leads are placed at various locations on the external chest wall.
In a normal animal, the lead that usually gives the P wave and R wave in a positive deflection is Lead II because of the heart’s position in the chest. As the wave of depolarization moves toward the positive electrode, it will record it as a positive deflection. If the wave moves directly toward the lead, it will be a strong positive deflection; if it is moving 45° obliquely toward the positive electrode, it will be a small positive deflection; if it is moving 90° to the positive electrode, the deflection will usually be minimal and be as much positive as negative. If the wave moves 45° away from the positive electrode and toward a negative electrode, it will be a small negative deflection; and finally, if the wave moves directly away from
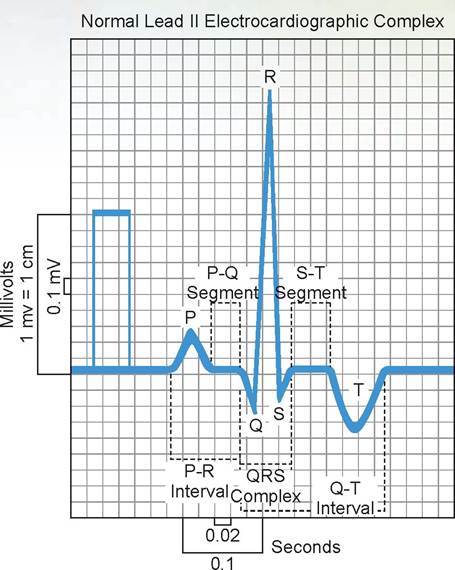
FIGURE 10.25: The normal Lead II electrocardiogram pattern. The machine appears standardized at 1 cm = 1 mV, and the tract would normally be recorded at 50 mm/sec paper speed
the positive electrode and directly toward the negative electrode, it will be strongly negative. If the QRS complex’s wave deflections are equally positive and negative, this lead is called the isoelectric lead. The size of the atria or ventricles also affects the size of the wave deflection, giving veterinarians an indication of whether there is heart enlargement. Therefore, measurements of the P wave and R wave are performed as follows (see also Figure 10.25). The units of the following are all in millivolts (mV).
P wave: Measure from the baseline to the top of the P wave.
R wave: Measure from the baseline to the top of the R wave. (Note: it is measured not from the bottom of the Q or S waves to the top of the R wave, but from the baseline.)
Along the horizontal axis of the ECG, certain measurements are taken. Remember, intervals include the wave deflections; segments do not. The units of the following are in seconds (sec).
P-R interval: Measure from the start of the P wave to the start of the Q wave. This interval is misnamed and should be called the P-Q interval, but it is so named because the Q wave is often absent. This represents the time for atrial depolarization.
P-Q segment: Measure from the end of the P wave to the start of the Q wave. This represents the time the wave is within the AV node.
QRS complex: Measure from the start of the Q wave to the end of the R wave. This represents the time for ventricular depolarization.
S-T segment: Measure from the end of the S wave to the start of the T wave. This represents the time period between the end of depolarization of the ventricles and the initiation of repolarization.
Q-T interval: Measure from the start of the Q wave to the end of the T wave. This represents the length of time for ventricular contraction and repolarization.
Note that the measure along the horizontal axis is time in seconds, and that the vertical is measured in millivolts (mV). The standard measurements are taken at 50 mm/sec, and 1 mV = 1 cm on the vertical axis. This makes each small box equal to 0.02 sec horizontally and 0.1 mV vertically.
EXERCISE 10.3 RECORDING THE ELECTROCARDIOGRAM
Procedure
1. Place a dog in right lateral recumbency on a table with a non-metallic surface (otherwise you may get 60 cycle-per-second interference), and place the electrodes on the skin as indicated on the electrode leads. Standard to the industry is that the white electrode is right front (RF) leg, the black electrode is left front (LF) leg, red is left hind (LH) leg, and green is right hind (RH) leg (note that green is the ground wire). The brown electrode is the chest lead, but we will not use this electrode. Place a small amount of electrode gel or alcohol at the connection sites.
2. Turn on the ECG machine and push the standardize button to be sure it deflects 1 cm at 1 mV. (If needed, adjust it so 1 cm = 1 mV.) Also make sure it is running at 50 mm/sec.
3. Record Leads I, II, and III for a short distance on the paper. If you would like to, you may also record AVF, AVL, and AVR at this time.
4. Reduce the paper speed to 25 cm/sec. Note the printed marks at the top of the ECG paper. Each little box is 1 mm square, and there are 75 little boxes between each mark, which we will call one section. If you do the math you will see that at 25 mm/sec it will take 3 seconds to traverse 75 boxes (one section), and 6 seconds for two sections. Counting the number of R waves in two sections and then multiplying by 10 gives you the heart rate, or beats per minute for the animal. (There are ten 6-second intervals in each minute; therefore, you multiply the beats counted by 10.)
5. Using the ECG, record the information in the following spaces and compare it to your instructor’s computations. Remember to label your units.

Questions
1. What would be the multiplier that is needed to determine the heart rate for two sections of ECG paper if the machine were run at 50 cm/sec?
2. If there were a delay or block in the impulse as it passed through the AV node, which two measurements would be increased?
Discussion
Regarding question 1, if the paper were running twice as fast as previously, half the number of R waves would be recorded. Therefore, the multiplier would have to be doubled to 20.
To answer question 2, because the impulse is in the AV node during the P-Q segment, this measurement would be increased in length. Also, because the P-R interval includes the P-Q segment, this too would be increased in length.
EXERCISE 10.4 BLOOD PRESSURE MEASUREMENT USING A DOPPLER
In humans, blood pressure is measured in a peripheral artery in the arm using a stethoscope and a sphygmomanometer, which consists of an inflatable cuff that circles the arm and a pressure manometer. Normally the blood flow through an artery is inaudible, but the inflated cuff causes blood flow in the artery to be turbulent, which is audible.
The cuff is inflated until the artery is completely compressed, with no flow of blood through it and thus no sound. As pressure is slowly released from the cuff, the manometer needle drops. At the point at which arterial blood pressure exceeds the pressure of the cuff, blood will flow through the artery and will be audible. This point is called the systolic blood pressure and represents peak systolic pressure at maximum ventricular contraction. As more pressure is released, pressure drops from the cuff and the artery; the point at which the blood flow again becomes inaudible is the diastolic blood pressure. This is the pressure within the vascular system when the heart is in diastole.
Animals do not have peripheral vessels of sufficient size distal to where a cuff could be placed to hear an audible pulse with a stethoscope. Therefore, devices such as dopplers must be used to hear the blood flow through the artery. Because the doppler records blood flow without turbulence, it is limited to systolic blood pressure measurement.
Procedure
1. Using an electric clipper and a #40 blade, clip away the hair on a dog between the carpal pad and metacarpal pad (or if necessary, clip on the dorsum of the hock).
2. Place a blood pressure cuff sized for a human infant or for a newborn (depending of the size of the dog’s leg) around the dog’s foreleg,just below the elbow (or hind leg just below the knee). Cuff width should be 40% of the circumference of the leg. Do not inflate it yet.
3. Put some ECG gel on the clipped area; in the areajust medial to the midline of the ventral aspect of the leg, place the doppler head and listen for the audible heartbeat. When it is consistently audible, inflate the cuff until the heartbeat becomes inaudible, then slowly release the pressure until it becomes audible once again. This point is the systolic blood pressure. Perform this three times and record your results below.

Question
1. Were all three measurements different, or were they the same each time?
Discussion
If the measurements were done correctly and the animal’s blood pressure was not affected by pumping the cuff, they should be the same each time. However, like humans, animals may get nervous and release epinephrine into their system, causing vasoconstriction, which increases peripheral resistance and increases blood pressure. Even though the act of measuring may hinder the accuracy of the measurement, the change is not so significant as to cause a misdiagnosis.
Clinical Significance
Auscultation of the heart valves is an important skill for both the veterinarian and the veterinary technician to learn. During dissection, when you made your cuts through the pulmonary artery and aorta, they were made through the cranial surface of the heart on the left side. It was mentioned that these two valves, because of the way the heart is positioned in the thorax, are cranial to the mitral valve, or left AV valve. It is thus logical that we would auscultate for these valves on the left side of the chest.
If the diaphragm of the stethoscope is placed just above the sternum on the left side of the chest and slid forward until the heart sound is clearly audible, it will be over the mitral valve. This should be the fourth or fifth intercostal space at the costochondral junction. Next, slide the stethoscope head a little dorsally and cranially and listen for the heart sounds in this location; this will be the aortic valve and should be the fourth intercostal space. Then, slide the stethoscope head cranially and ventrally one intercostal space and listen to the pulmonary valve, which should be at the third intercostal space at the costochondral junction.
On the right side, the right AV valve is found at the fourth intercostal space at the costochondral junction, or wherever it is best heard. Here is how to remember the order in which these valves are found: If the valves were labeled on the left outside chest wall, reading from cranial to caudal would form the word P-A-M (pulmonary valve-aortic valve-mitral valve).

λ n veterinary school, the seniors used to delight in making junior veterinary students look
_______ [J stupid. When I became a senior, I personally never, ever took advantage of the poor lower forms of life.
When I was a junior, the two senior students with whom I was assigned for my week of cardiology rotation had a lot of fun at my expense. The first game they played with me was “Find the Heart.” On Monday morning they took me out to the calf pens and told me there was something wrong with the calf's heart and, if I had any brains at all, I should be able to diagnose the condition within a few minutes. I got out my stethoscope and proceeded to listen for the heart sounds. I started on the left side, meticulously searching for the mitral valve. I searched and searched, listening intently, but I could not hear anything.
“Well, what do you hear?” Mutt (the tall one) asked me.
“Uh, nothing. I can't hear anything,” I replied, beginning to show a little red on my face.
“Come here,” said Jeff (the short one).
I walked over to him and, not being the brightest human on the planet at that moment, did not remove the earpieces of my stethoscope from my ears.
Grabbing the head of my stethoscope and tapping on it, he yelled, “Does this thing work?”
I jumped back in pain and pulled them from my ears.
“Well, that's not the problem. Listen to the other side of the chest; maybe the heart is over there,” he told me.
Dumbly, I did as he suggested. All the while, these two were trying to keep straight faces and glaring at me like I was stupid. I wasn't stupid, just ignorant. As I listened, I was thinking, because the heart is in the middle of the chest, how could I hear it on the right side if I couldn't hear it on the left? This time I moved the stethoscope up and listened to the lung sounds. Now I could hear the muffled sounds of a heart.
I stood up and looked at them. “The heart's not in the chest, is it?” I asked.
“What do you mean it's not in the chest?” Jeff replied.
“If it isn't in the chest, where would it be?” Mutt inquired.
I started listening to the cranial chest and palpated the neck. Deep in the neck, just in front of the thoracic inlet, I felt something beating and found a small heart.
“What's it called?” they asked.
“I don't know,” I replied.
“An ectopic cordis,” Mutt answered.
I had gotten the answer too quickly for them. Next I was guided to the small animal ward to play “Name the Murmur.”
“Listen to this heart and tell us the type of murmur you hear and its cause,” Jeff told me.
As I grasped the chest, I could feel the vibration of the heartbeat in my hand. Placing the stethoscope head against the chest, I immediately heard a whoosh-whoosh sound rather than the normal l ub-dub. I had been taught that murmurs were abnormal heart sounds, often heard between the first and second heart sounds, but being only a rookie at this, my experience was lacking. It sounded more like a washing machine than a heartbeat.
“I have no idea what this is,” I said.
“Well, is it systolic or diastolic?” Mutt asked me.
“I don't know. Both maybe?” I replied.
“That's an intelligent answer; you can do better than that, can't you?” Jeff remarked sarcastically. “Describe it to us,” Mutt demanded.
“Well, there's no first or second heart sound, just a loud whoosh, followed immediately by a second whoosh of a slightly lower pitch. Then it repeats itself continuously,” I said, gesturing with my hands and shrugging my shoulders.
They had given me up as hopeless, I thought.
“It's a machinery murmur of a patent ductus arteriosus,” Jeff told me.
“Better go read up on it before Dr. Frye asks you about it and you get it wrong,” Mutt said, shaking his head.
They sent me off to the vet school library to read about it. This is what I found out: The ductus arteriosus is a vessel present in fetal life that shunts blood from the pulmonary artery to the aorta, thus bypassing the lungs (see Figure 10.1B). In dogs and cats, it normally closes by muscular contraction sometime in the first eight days of life. When it does not close, the condition is known as a patent ductus arteriosus. Sometimes the vessel doesn't close completely and leaves a very small opening, and in those cases it usually causes no important hemodynamic changes. The female dog is most often affected, and there is a breed predilection in miniature poodles, German shepherds, Pomeranians, Shetland sheepdogs, and other toy breeds. When the ductus stays patent, most dogs develop severe clinical signs in first six to eight weeks of life. Cats with this condition rarely survive past a few weeks of age.
The pathophysiology is complicated and depends on the size of the patent ductus and the direction of the blood flow through it. The result is left and/or right heart failure. Animals with the condition generally have a history of coughing and exercise intolerance. On physical exam, a veterinarian may find a persistent machinery murmur, a pounding femoral pulse, and a precordial thrill (which is the vibration I felt when I placed my hand on the dog's chest). Diagnosis is made based on the clinical signs, radiography, ECG, ultrasonography of the heart, and angiography. If the blood flow is left to right, surgical ligation of the duct or implanting a plug (called an embolization coil) can help correct the problem. Because the condition may be hereditary, which has been confirmed in the miniature poodle, animals that survive should not be bred.
After reading up on the condition, I realized I had not done such a bad job in describing it. Later I found out I had secretly passed their test on both accounts, but they would never admit that to me.
Summary
In this chapter we covered the anatomy and physiology of the heart and the blood-vascular system. You learned that there are three main circulatory systems of the blood-vascular system: the coronary, pulmonary, and systemic circulations. You will learn in Chapter 13 that there is a small portal system between the hypothalamus of the brain and the pituitary gland. In addition to learning the parts of the heart and its intrinsic vessels, you learned the names of the main vessels in the body of the cat. These names are similar in most species.
The vascular supply of the equine leg is beyond the scope of this book, but many excellent texts cover this if you are interested. Some of the more important vessels in horses are the external maxillary artery as it crosses the mandible (for obtaining a pulse rate), the jugular veins in the jugular furrow (for intravenous injections and drawing blood), the carotid arteries (for avoiding them when working on the jugular veins), the common digital artery on the medial aspect of the leg (for obtaining a pulse rate), and the medial and lateral posterior digital arteries just below the fetlock joint (which may develop a prominent pulse in cases of laminitis).
Finally, knowing how to take blood pressure readings and what they mean, and knowing the significance of the wave forms on an ECG, are important skills every veterinary technician should learn.
REVIEW QUESTIONS
1. Into what two portions is the cardiovascular system divided?
2. Differentiate among the systemic, pulmonary, and coronary circulatory systems.
3. Define a portal system, and describe the hepatic portal system.
4. Differentiate between systole and diastole.
5. Name the four chambers of the heart and their associated valves.
6. What causes all four heart sounds, and which are audible with a stethoscope?
7. The pericardial sac is made up of what layers?
8. What structure consisting of a groove and an associated artery on the ventrocranial surface of the heart delineates the right and left sides of the heart?
9. What is the function of the trabecula septomarginalis?
10. Which veins contain oxygenated blood in the fetus? In the adult?
11. Which arteries contain non-oxygenated blood in the fetus? In the adult?
12. What is the function of the papillary muscles and chordae tendineae?
13. In fetal life, what is the function of the fossa ovalis?
14. What is the name of the smallest arteries and smallest veins?
15. What compound acts as a buffer in blood by combining with free hydrogen ions produced by the dissociation of carbonic acid?
16. Where is endothelium located?
17. Since a horse’s legs have no valves, how is stocking up (swelling) prevented?
18. What are the factors that control systolic blood pressure and diastolic blood pressure?
19. Define hypertension and hypotension.
20. Where is the thoracic duct found, and what does it carry?
21. Name the specialized non-contractile myocardial tissue in the heart.
22. What is the pacemaker of the heart?
23. What events are occurring during the P, QRS, and T waves of the electrocardiogram?
24. If the wave of depolarization is moving directly toward the positive electrode, will the deflection on the electrocardiogram be positive or negative, and will it be a strong deflection, a moderate deflection, or no deflection at all?
25. True or False: The P-R interval is from the start of the P wave to the start of the Q wave.