The Respiratory System
OBJECTIVES
• state the function of each component of the respiratory system
• describe the air flow from the nose to the alveoli of the lungs
• dissect the structures and organs of the respiratory system, and identify them by name
• identify the parts of the larynx and its cartilages
• describe the anatomy of the lungs of different species
• understand the flow of air between the air sacs and lungs of the bird and their connection to the pneumatic bones
• understand the various methods of measuring lung volumes and capacities
• understand the concept of dead space
MATERIALS
• cat cadaver, triple injected (order without skin attached)
• Mayo dissecting scissors
• probe
• 1 ? 2 thumb forceps or Adson tissue forceps
• #4 scalpel handle with blade
• bone cutting forceps
• rubber gloves
• model of the larynx
• spirometer
Introduction
The respiratory system can be divided into two parts: the upper respiratory system and lower respiratory system.
The structures of the upper respiratory system include the external nares, nasal cavity, sinuses, and larynx. The lower respiratory system includes the trachea, bronchi, bronchioles, and alveoli. The respiratory system performs ventilation and respiration. Ventilation is the process of breathing (also called pulmonary ventilation), which is the movement of gases in and out of the lungs. Respiration is a broader term that includes not only the act of ventilation but also the distribution of gases in the alveoli and the diffusion of oxygen into and of carbon dioxide out of the bloodstream. This exchange of gases in and out of the blood is called external respiration. Internal respiration is the exchange of gases between blood and tissues.In the exercises in this chapter the important structures are listed in colored bold print. If a structure is mentioned prior to its dissection it will be italicized.
Structures discussed prior to dissection may also be in bold print for special emphasis.237
EXERCISE 11.1 THE UPPER RESPIRATORY SYSTEM
The functions of the upper respiratory system are as follows:
1. conducting air (in and out)
2. cleansing air before it is used by the body
3. humidifying air before it is used by the body
4. transferring heat
5. making sounds (phonation)
6. maintaining acid-base balance
7. smelling (olfaction). The olfactory sensory receptors are neuroepithelial cells, which are chemical transducers. Contact with an odor molecule induces a chemical phenomenon that excites the cells to depolarize. This message is carried by the first cranial nerve (the olfactory nerve) to the olfactory bulbs, up the olfactory tracts, into the rhinencephalon (the olfactory brain, part of the telencephalon of the cerebrum), and is interpreted there as an odor. The sensory receptors are located in the posteromedial and posterodorsal parts of the nasal cavity.
Procedure
1. Examine the nose of the cat. The air enters the nasal cavity through the nares or nostrils. These openings vary in size and shape with each species. The horse’s nostrils are large and easily dilated, whereas the pig’s are small and rigid. The non-haired area of the nose is called the planum nasale (or planum nasolabiale in species with a large muzzle). The most rostral part of the nasal cavity is the nasal vestibule, which is the open chamber behind the nostrils that is lined with simple squamous epithelial cells.
The two nasal cavities, left and right, are separated rostrally by a cartilaginous septum. Each cavity is divided further by the nasal bone in the center and by the nasal turbinate bones projecting from the lateral wall of the nasal passage. The bony turbinates are scroll-like in appearance and are covered by nasal mucosa to form the nasal conchae. These effectively divide the flowing air into channels: the ventral meatus, middle meatus, dorsal meatus, and common meatus.
The mucosa is made up of pseudostratified ciliated columnar epithelial cells, goblet cells, and nasal glands. These channels increase air turbulence and thereby warm, moisten, and filter air as it passes through.The main sinuses are the maxillary and frontal sinuses, which are located within the bones for which they are named. Large animals also have a sphenoid sinus and a palatine sinus, except the horse, in which these two sinuses are fused into a sphenopalatine sinus. The cow and sheep have an additional sinus, the lacrimal sinus. These sinuses act as resonance chambers in phonation, and their mucosa, like that of the nasal cavity, warms and moistens the incoming air.
From the nasal cavity the air moves through the choanae (air passageway of the internal nares) and into the nasopharynx. On the dorsolateral wall of the nasopharynx are openings to the auditory or eustachian tubes. These act in pressure regulation with the middle ear, to which the tubes connect. (In the horse, each eustachian tube opens into a large ventral diverticulum within the nasopharynx known as the guttural pouch, which is located just lateral to the pharynx.) The nasopharynx is separated from the oropharynx by the soft palate. The position of the open epiglottis, either contacting the caudal edge of the soft palate or just beneath it, causes inhaled air to pass through the nasopharynx into the laryn- gopharynx (the area above the open epiglottis) and directly into the larynx (Figures 11.1 and 11.2).
2. Carefully remove the muscles from the ventral surface of the larynx in the neck to expose the cartilage (Figure 11.3).
The larynx is a hard tube made of cartilages. The thyroid cartilage is the large, ventral cartilage visible after removal of the ventral neck muscles. The cricoid cartilage is located caudal to the thyroid cartilage. This cartilage is shaped like a signet ring, with the small band located ventrally and an expanded portion located dorsally on both sides.
3. The cricothyroid ligament is the semi-transparent membrane in the space between the cricoid and thyroid cartilages.
Make a median longitudinal incision through these two cartilages on the ventral ridge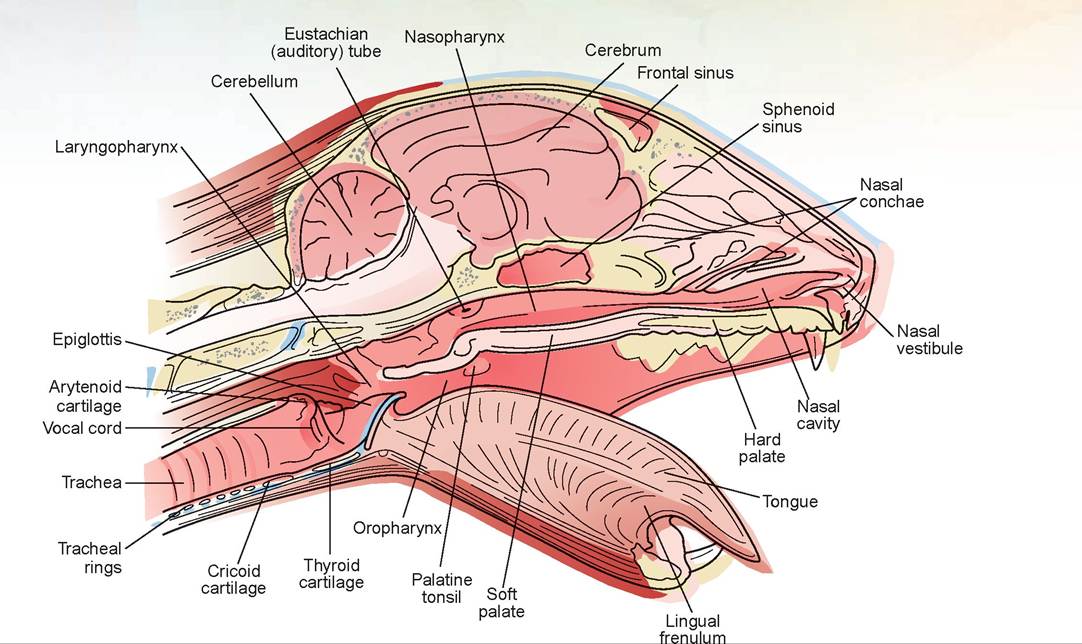
FIGURE 11.1: Sagittal view of the cat's head.
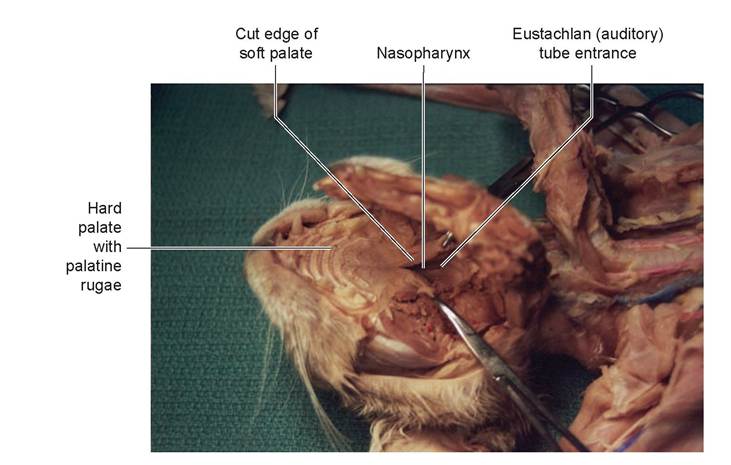
FIGURE 11.2: Nasopharynx and eustachian tube opening in a cat.
and through the basihyoid bone (the most ventral bone of the hyoid apparatus). Now find the two pyramid-shaped arytenoid cartilages on the dorsal surface of the larynx, cranial to the cricoid cartilage.
4. The epiglottis is the most cranial cartilage of the larynx and can be seen at the base of the tongue during the dissection of the mouth. This pointed, leaf-like cartilage is attached ventrally to the thyroid cartilage.
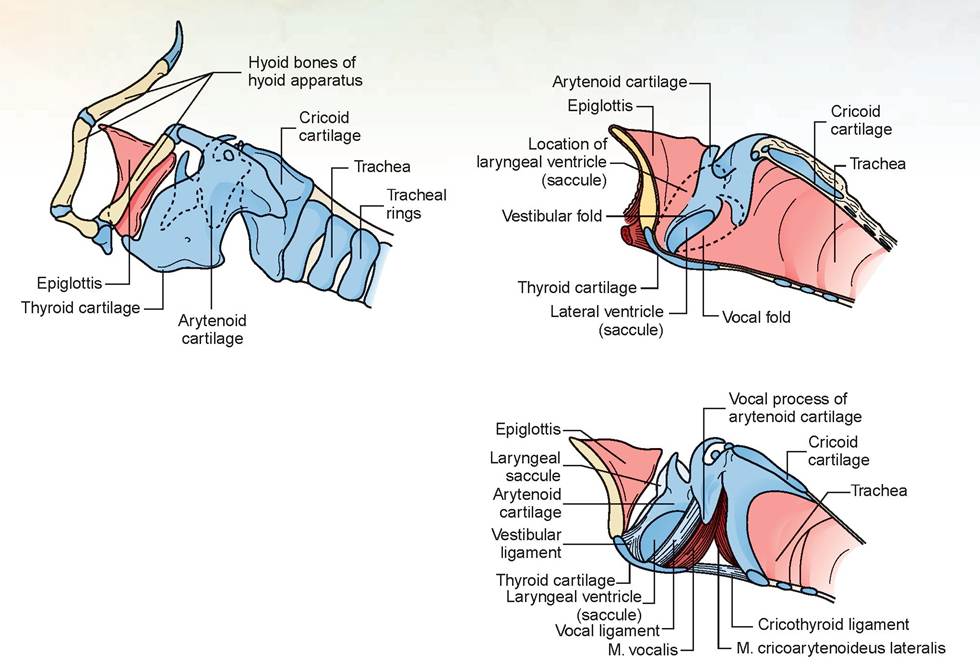
FIGURE 11.3: Laryngeal cartilages and the structure of the larynx (dog). A. Cartilaginous structures of the larynx and the hyoid apparatus. B. Structures of the larynx with mucosa attached. C. Structures of the larynx with mucosa removed.
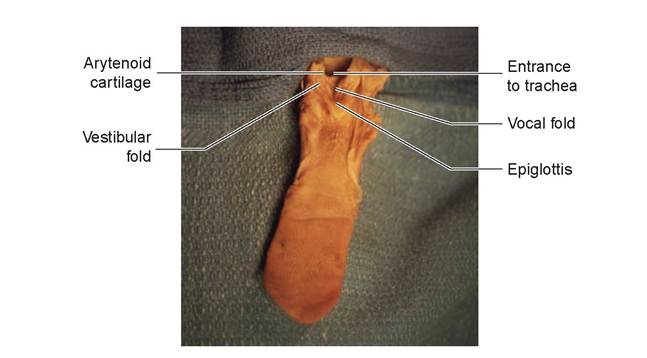
FIGURE 11.4: Isolated view of the tongue and laryngeal opening in a cat.
5. The most cranial and lateral folds of mucous membranes extending across the larynx are the vestibular folds; the caudal, large pair of folds are the vocal folds or vocal cords. Note in Figure 11.4 that these structures form a V in the center ventrally. This is how you would view the entrance to the larynx prior to inserting an endotracheal tube. The median longitudinal cut you made through the ventrum of the larynx splits the apex of the V. Your view is upside down from the photo in Figure 11.4, but this does not alter the appearance of the structures studied. In fact, you can observe them more closely with the larynx opened.
The depression created between the vocal and vestibular folds is called the laryngeal ventricle (present in dogs, questionable appearance in cats). The vocal cord is actually a vocal fold of mucous membrane covering the internal vocal ligament. This ligament extends from the arytenoid cartilages to the thyroid cartilage.Just caudal to this ligament is the vocalis muscle (m. vocalis), the muscle that controls the tension on the ligament and thus the pitch of the sound that is produced. Sound production, of course, is the purpose of this structure. The glottis is the space outlined by the paired arytenoid cartilages and paired vocal folds that form the opening (the vestibulum) into the larynx.
EXERCISE 11.2 THE LOWER RESPIRATORY SYSTEM
The functions of the lower respiratory system are the conduction of air into the alveoli and the exchange of gases with the pulmonary blood.
Procedure
1. The trachea starts at the caudal end of the larynx and continues until it bifurcates just dorsal to the heart. Observe the large right and left common carotid arteries and small internal jugular veins on each side of the trachea. The vagus nerve is the white, flattened thread that courses adjacent to the common carotid artery. This nerve supplies many of the thoracic and abdominal organs.
2. Free the trachea laterally from the preceding blood vessels and nerves if this has not already been done. Find the esophagus, the muscular tube that runs dorsal and parallel to the trachea.
3. Locate the two thyroid glands. Each is a small, dark-tan, oval-shaped lobe attached to the trachea, on the right lateral and left lateral side just caudal to the cricoid cartilage.
4. Examine the interior of the thoracic cavity. It is divided by the mediastinum into two right and left pleural cavities. To reiterate from the previous chapter, the pericardial sac, which contains the heart, is made up of the fibrous pericardium and the serous pericardium. The latter consists of two laminae: the parietal lamina and the visceral lamina, also called the epicardium.
Thus, the walls of the heart consist of the epicardium, the most external layer; the myocardium in the middle; and the endocardium, the most internal layer. Between the two pericardial serous laminae is the pericardial sac, in which a small amount of lubricating pericardial fluid allows the smooth gliding of one over the other and helps the heart beat easily. The fibrous pericardium is overlapped by the pericardial pleura (Figure 11.5). This is an extension of the mediastinal pleura.5. The parietal pleura (like the parietal peritoneum) lines the thoracic cavity, while the visceral pleura covers the lungs. Both the parietal and visceral pleurae meet with the mediastinal pleura. The mediastinum is a connective tissue partition, which includes the symmetrical mediastinal pleurae and separates the right and left pleural cavities. Conventionally, the mediastinal area of the thoracic cavity is divided into a space cranial to the heart, called the cranial mediastinum; a space where the heart is located, called the middle mediastinum; and the space between the heart and the diaphragm, called the caudal mediastinum. However, dorsal and ventral to the heart are two more spaces, called the dorsal mediastinum and the ventral mediastinum.
6. Remove the heart to expose the bifurcation of the trachea; this is called the carina. Note the cuts you are making through the pulmonary arteries and veins. The pulmonary artery and its branches, plus the right side of the heart, contain blue latex (illustrating they carry deoxygenated blood), and the pulmonary veins and the left side of the heart contain red latex (illustrating they carry oxygenated blood); note that this color pattern is the opposite of what is found in arteries and veins throughout the rest of the body. Visualize the bifurcation of the trachea and the extrapulmonary main bronchi (Figure 11.6). Note how they divide and enter each lobe of the lungs.
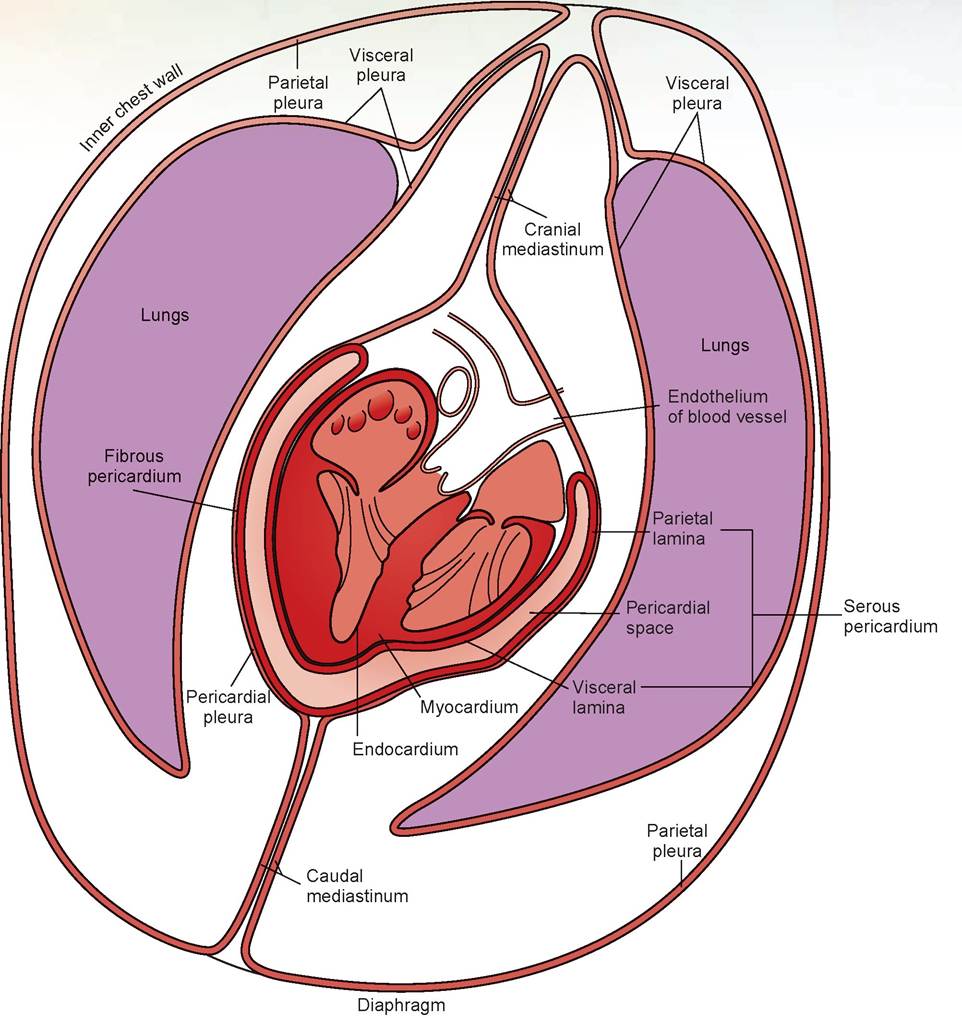
FIGURE 11.5: The pericardial sac and thoracic pleura.
7. Examine the lungs on either side of the thorax. Each lung is divided into lobes. There are four lobes on the right side: the cranial, middle, caudal, and accessory lobes; and there are two lobes on the left: the cranial and caudal lobes (Figures 11.7 and 11.8). Note in Figure 11.7B that the horse has a single right and left lung lobe, and a smaller accessory lobe of the right lung.
These lobes were formerly known as the apical (cranial), cardiac (middle), diaphragmatic (caudal), and intermediate (accessory) lobes. Many veterinarians learned them by these names, which are still used in older textbooks. See Table 11.1 for a comparison of the lungs in different species.
Tease away the medial surface of the cranial or middle lobes to observe the branching of the bronchi and blood vessels. Observe the lobar bronchus that runs the length of each lobe and the branches off of it.
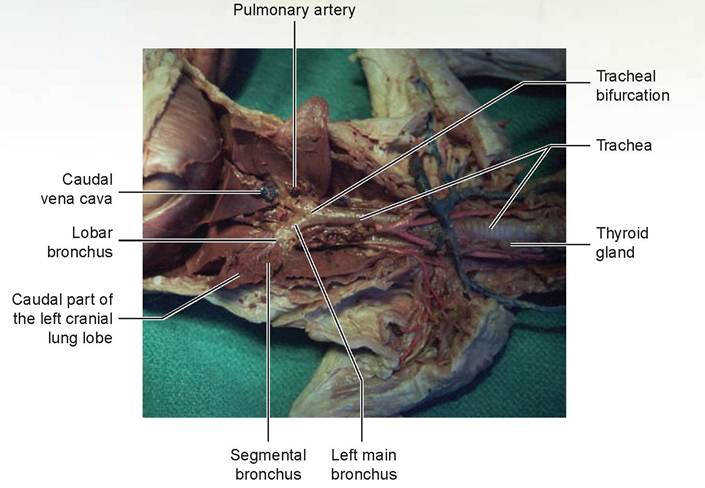
FIGURE 11.6: Arrangement of the lungs and bronchial tree within the thoracic cavity—in situ.
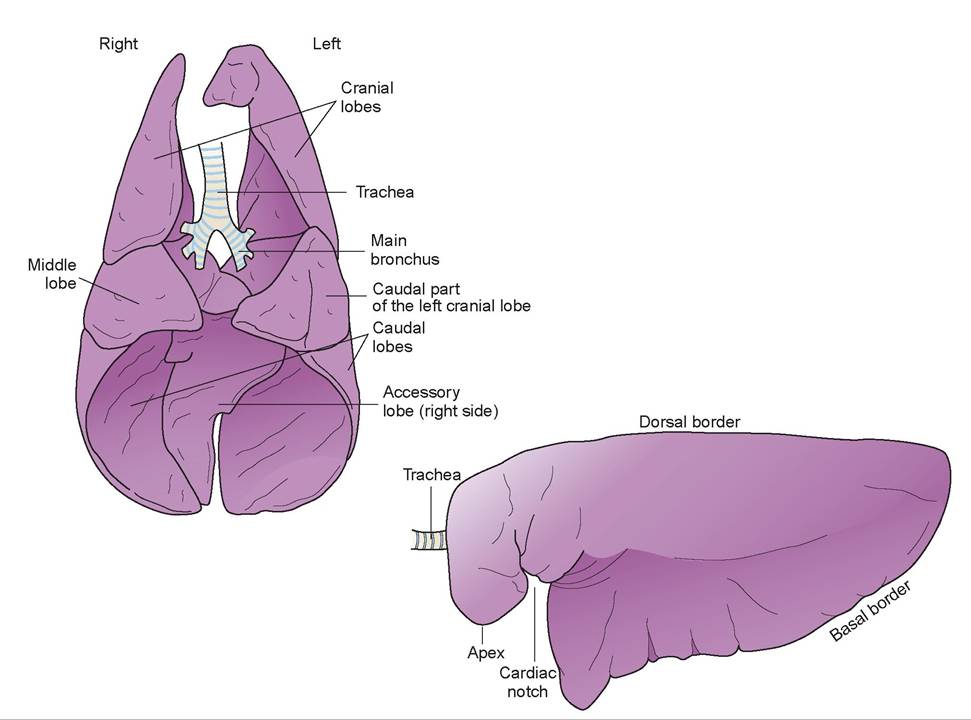
FIGURE 11.7: A. Lobes of the lung in a cat. B. Lobes of the lung in a horse.
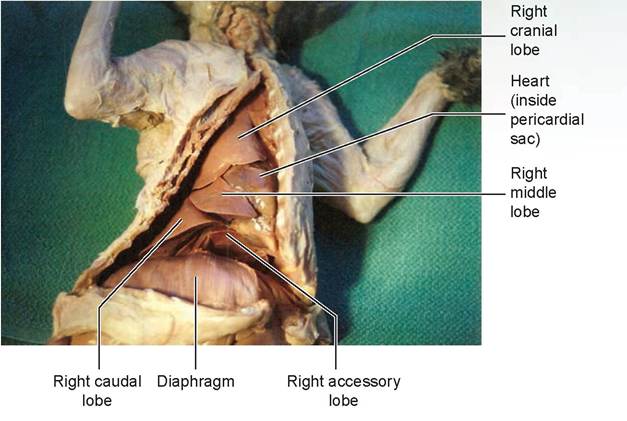
FIGURE 11.8: Lobes of the right lung of a cat.
TABLE 11.1: Lungs of Various Species of Domestic Animals
| Cranial (apical) | Middle (cardiac) | Caudal (diaphragmatic) | Intermediate (accessory) | |
| Horse | 1 lobe (right and left) | 1 right only | ||
| Ox | 1 left 2 right | 1 left and 1 right | 1 left and 1 right | 1 right only |
| Sheep | 1 left and 1 right | 1 right only | 1 left and 1 right | 1 right only |
| P∣g | 1 left and 1 right | 1 right only | 1 left and 1 right | 1 right only |
| Dog | 1 left and 1 right | 1 right only | 1 left and 1 right | 1 right only |
| Cat | 1 left and 1 right | 1 right only | 1 left and 1 right | 1 right only |
8. Note that the lungs are attached to other structures in the thorax only by the root. The root of the lung is formed by the branching of the bronchi, the pulmonary artery and veins, the nerves, and the lymphatic vessels and lymph nodes, all of which are encircled by pleura.
9. As the main bronchus enters the lungs, it becomes a lobar bronchus, which is the tube that courses the entire distance down the lung lobe (Figure 11.9). The branches from this are the segmental bronchi. Segmental bronchi have less cartilage than the main and lobar bronchi. The branches off the segmental bronchi are the terminal bronchioles, which are too small to be dissected and look like the tissue of the lungs. The trachea and the bronchial tree down to the first 2/3 of the terminal bronchioles is lined with pseudostratified ciliated columnar epithelium. The last 1/3 is simple ciliated columnar epithelium. Branching off the terminal bronchioles are the respiratory units, each of which consists of a respiratory bronchiole, an alveolar duct, an alveolar sac, and alveoli (Figure 11.10). This is called a respiratory unit because all the structures contain alveoli, which are where external respiration occurs.
10. In the mid-cranial area of the thoracic cavity, where the cranial mediastinum is located, is a large, fluctuant-appearing gland called the thymus gland (Figure 11.11). This gland, divided into lobules, is large in young cats but smaller in older ones. Just dorsal to this gland, within the cranial mediastinum, are the mediastinal lymph nodes.
11. Examine the interior of the wall of the thoracic cavity and locate the intercostal vein, intercostal artery, and intercostal nerve on the caudal border of each rib.
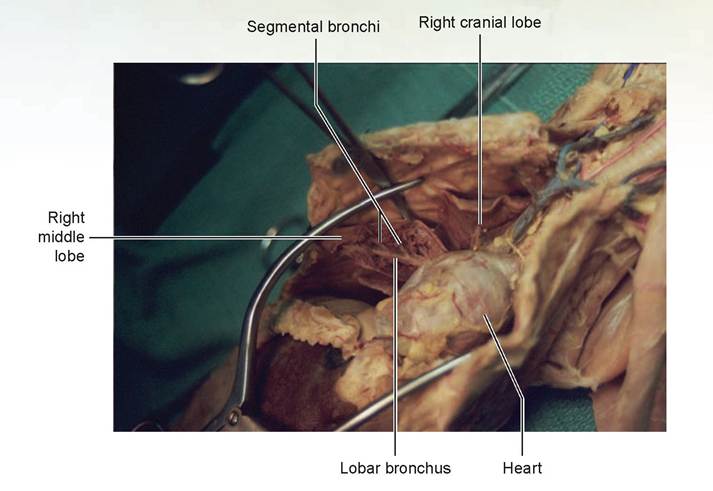
FIGURE 11.9: Lobes of the right lung of a cat.
border=0 id="Picutre 296" class="lazyload" data-src="/files/uch_group75/uch_pgroup311/uch_uch7427/image/image281.jpg">
FIGURE 11.10: Bronchiolar system of the lungs (all species).
12. The crura of the diaphragm (where it attaches to the dorsal wall) forms the caudodorsal area of the thoracic cavity. Find the phrenic nerves: white, thread-like structures directed caudally on each side of the pericardium to the cranial surface of the diaphragm (Figure 11.12). The phrenic nerves originate from the fifth and sixth cervical nerves.
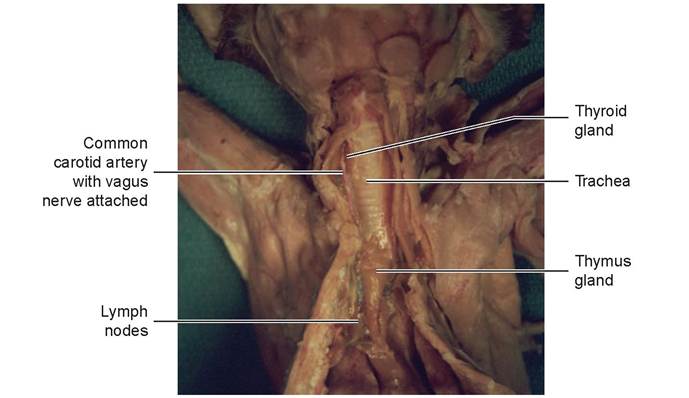
FIGURE 11.11: Thymus gland in the cranial thorax of a cat.
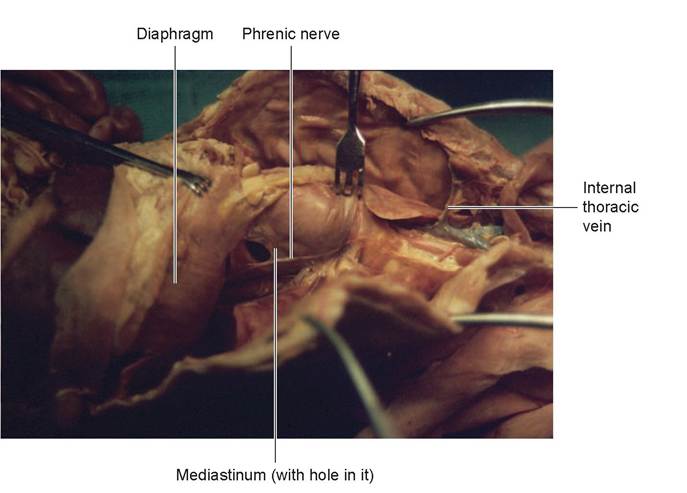
FIGURE 11.12: Mediastinum and phrenic nerve of a cat.
EXERCISE 11.3 THE LUNGS OF BIRDS
Procedure
Using Figure 11.13, find the structures of the respiratory system of the bird. Air enters the external nares through the nasal cavity, exits via the choanal slit, and continues through the glottis and larynx into the trachea. At the bifurcation of the trachea is the syrinx, or voice box. The trachea branches into bronchi, which pass through the ventral aspect of each lung. As these bronchi enter the lungs, they lose their
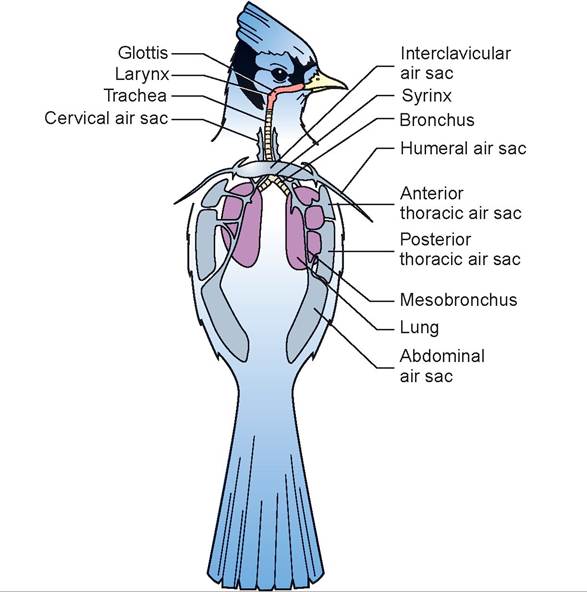
FIGURE 11.13: Avian lungs and air sacs.
reinforcing cartilage and are called mesobronchi. These give rise to between four and six ventrobronchi, then branch into smaller parabronchi, which are connected to the air capillaries. The air capillaries are surrounded by blood capillaries, and gas exchange occurs between these two groups. The mesobronchi also continue down through the lungs and connect to the abdominal air sac. There are nine air sacs: the paired cranial thoracic, caudal thoracic, cervical, and abdominal air sacs, and the unpaired inter- clavicular air sac. In birds, the mesobronchi are considered primary bronchi, and the ventrobronchi are considered secondary bronchi. These secondary bronchi, in addition to giving off parabronchi, also connect to the cervical, cranial thoracic, caudal thoracic, and interclavicular air sacs.
Two breaths, or respiratory cycles, are required to move one inhaled unit of air through the avian respiratory system (Figure 11.14). The first inhalation is made by expansion of the thoracoabdominal space (birds do not have a diaphragm), and most of the air moves directly into the abdominal air sacs. The first expiration pushes air into the lungs. This is where gas exchange with the blood occurs. The second inspiration moves the air into the cranial thoracic pairs of air sacs (anterior thoracic and posterior thoracic), and the second expiration moves the air out through the trachea. More than any other animal, birds truly receive fresh air during breathing because air flow is pushed into the lungs, not pulled.
Bird’s lungs are attached to the inside of the thoracic cavity, so holding a bird tightly can compromise air flow drastically. Air sacs also communicate with pneumatic bones. The interclavicular air sac extends to the humerus, sternum, syrinx, and pectoral girdle. The abdominal sac often extends to the legs and pelvic girdle.
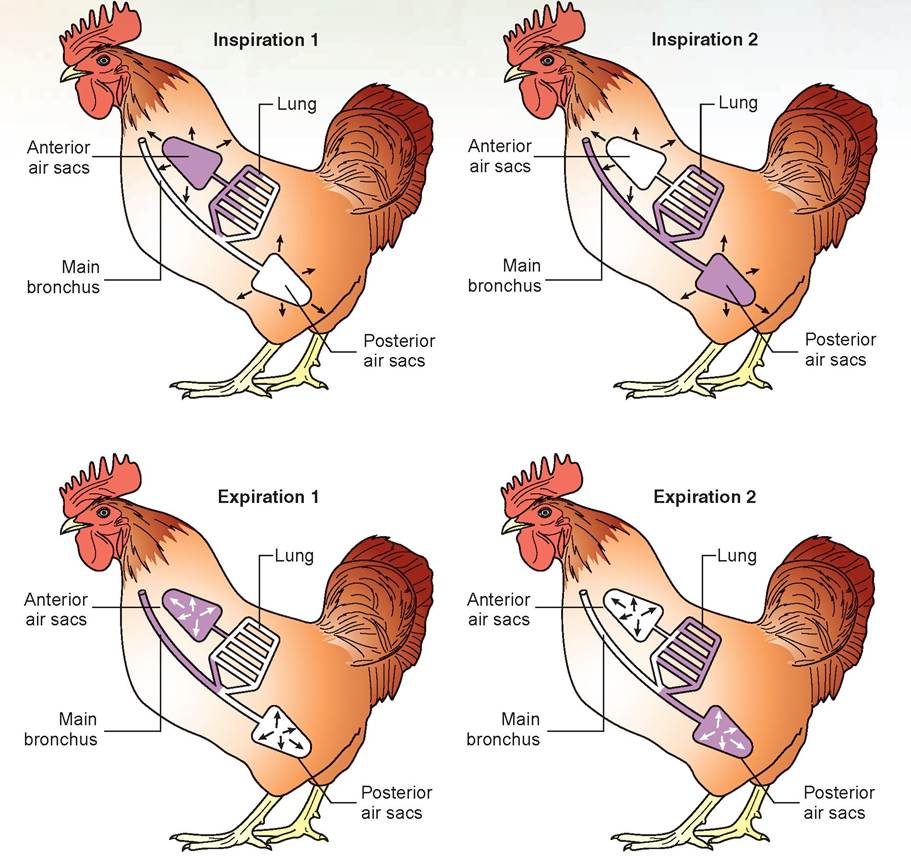
FIGURE 11.14: Air flow through the respiratory system of birds (white areas represent air flow).
Lung Volumes and Capacities
tidal volume (VT): Volume of air moving in (or out) during normal breathing.
inspiratory reserve volume: Volume of air it is possible to inhale after a normal inspiration.
expiratory reserve volume: Volume of air it is possible to exhale after a normal expiration.
residual volume: Volume of air in the lungs, even after maximum expiration.
vital capacity: The total volume of air that can be exhaled after a maximum inspiration.
functional residual capacity: The sum of the expiratory reserve volume and the residual volume. Functional residual capacity equals the volume of gas left in the lungs at the end of a normal expiration, and this remaining gas will mix with the next tidal volume. Functional residual capacity also shows that the alveoli do not fill with fresh air on each inspiration.
dead space: The space occupied by air at the end of an expiration. Dead space is also the volume of the respiratory system that takes no active role in external respiration; in other words, it is the volume of air that occupies the space between the nose and the respiratory unit. Only the respiratory unit has alveoli in which external respiration can occur. If an endotracheal tube is inserted and extends through the mouth, as in gas anesthesia, this added volume is added dead space.
EXERCISE 11.4 MEASURING LUNG VOLUMES AND CAPACITIES
Procedure
Because dogs and cats are reluctant to breathe into a hose on command, this exercise will use a spirometer with you as the subject. In the spaces provided, record the volume of air for each measurement.
1. Without using the spirometer, count and record the your normal respiratory rate (RR).
RR =______________ respirations/minute
2. Insert the disposable cardboard mouthpiece into the open end of the valve assembly of the spirometer. Practice exhaling though the spirometer instead of through your nose so an accurate measurement can be obtained.
3. Conduct the test three times for each required measurement. Write down each measurement and the average of the three.
4. Measure tidal volume (Vt). Inhale a normal breath, and then exhale normally into the spirometer mouthpiece. Record the volume and repeat the test twice more. (Normal human value = 500 ml)
trial 1: ml
trial 2: ml
trial 3: ml
average: ml
5. Compute the minute volume (Ve).
minute volume (Ve) = Vt ? RR
minute volume (Ve) =__________ ml ?____________ resp/min
minute volume (Ve) =__________ ml
6. Measure expiratory reserve volume (ERV). Inhale and exhale normally two or three times; then, after exhaling, insert the spirometer mouthpiece and exhale forcibly as much of the additional air in your lungs as you can. Record the result, and repeat the test twice again. (Normal human value = 1,000 to 1,200 ml)
trial 1: ml
trial 2: ml
trial 3: ml
average: ml
7. Determine vital capacity (VC). Breathe in and out two or three times; then bend over and exhale all the air possible. Next, as you raise yourself upright, inhale as fully as possible (you must strain to inhale the maximum amount). Quickly insert the mouthpiece and forcibly exhale as much as you can. Record your result and repeat the test twice again. (Normal human value = 4,500 ml or a range of 3,600 to 4,800 ml)
trial 1: ml
trial 2: ml
trial 3: ml
average: ml
8. Calculate inspiratory reserve volume (IRV) with the following formula. (Normal human value = 2,100 to 3,100 ml)

Question
1. How does your computed value compare with normal for each of the previous calculations?
Clinical Significance
Knowledge of the anatomy of the lung lobes is critical when considering the areas to auscultate. Most veterinarians start listening to the area of the chest wall just above the elbow joint, caudal to the scapula. This is where the trachea and carina are located. The sounds auscultated here are called bronchial sounds and are loudest because of the air turbulence created at this bifurcation. Listen to the lower end of the trachea in the neck area to learn what this sounds like.
Place the stethoscope head in the location discussed previously and listen for similar sounds. In large animals, this sound is heard only in a limited area of the chest because bronchial sounds are not conducted any distance in normal lung tissue. In the dog (in particular, in small breeds of dogs) and in the cat, bronchial sounds may be heard over a considerable part of the area of auscultation. Next, slide the stethoscope head ventrally to listen to the cranial lobe; then auscultate the middle and the caudal lobes in order. The normal sounds of the lung lobes are quieter and called vesicular sounds. They are best described as the sound produced if the letter F is whispered softly.
These sounds may change in various pathological situations. If the lung lobe (or part of a lung lobe) becomes consolidated with fibrin and fluid due to pneumonia, the sounds are called referred bronchial sounds. A good auscultator can discern accurately where the line of consolidation occurs across the ventral aspects of the lung lobes. Abnormal lung sounds produced by pathological processes within the tracheobronchial tree are termed adventitious sounds. The point of maximum intensity is usually near the diseased area.
Adventitious sounds may be either discontinuous (crackles) or continuous (wheezes). Crackles are characterized as either coarse or fine. Coarse crackles are bubbling or gurgling sounds, whereas fine crackles are often characterized as Velcro or cellophane-type sounds. One mechanism for causing coarse crackles is the bursting of bubbles of secretions within an airway, such as in pulmonary edema or bronchopneumonia. Fine crackles may occur when a closed airway opens suddenly during inspiration, as may occur in fibrosis, inflammation, or interstitial pulmonary edema. Wheezes are continuous musical or whistling sounds generated by air passage through a narrowed airway, as might be caused by stenosis, the presence of foreign bodies, bronchospasms, mucous plugging, or tumors.

-f ike was a 12-lb. “terror,” according to Mrs. Robertson. Corralling him long enough z∙∙—⅝ ∕∖∕ to administer his puppy shots was an impossible task for one person. I summoned ∖J~'.? V my best technician, who, by the way, can hold anything still for 10 seconds. Fortunately, I can administer a DHLPP in less time than that and can even manage to get the needle into the animal rather than my thumb... usually. Nike was a perpetual-motion poodle, with every body part moving simultaneously: squirming, wiggling, running, jumping, and going every direction at the same time. But running was his specialty! He would have been about 9 months old the day he ran full speed through an 8-cm wide opening in a wooden fence. Unfortunately, Nike's chest was just slightly under 10 cm in diameter. It was not the best day of his life.
Mrs. Robertson had seen the whole event. The neighbor's cat made it through the opening with no problem, with Nike in hot pursuit. With a howl of pain, he let his owner know he had made a huge error in judgment. Mrs. Robertson was frantic upon entering my office.
“He's having trouble breathing,” she exclaimed.
I listened to his chest and noted that the lung sounds on the right side were normal, but on the left side the vesicular sounds were diminished in the areas of the lower cranial and caudal lung lobes where they should have been audible. A quick x-ray revealed that his left lung was not inflating as much as it should, and fluid was accumulating in the pleural cavity. The thoracocentesis showed the fluid was fresh blood. This condition is known as a hemothorax.
Fortunately, I could not find any fractured ribs. The ribs had some give to them because of their ligamentous attachment at the vertebrae and the cartilaginous portion that attaches to the sternum. Nike's blood work-up revealed normal clotting times. After sedation, we drained the blood from his chest through a small catheter so as not to damage the lung tissues. Simultaneously, we treated him for shock.
It was necessary to drain his chest two more times that afternoon and evening. The next day we were still able to get blood from the chest, but the amount was diminishing. For that reason, a thoracotomy (a surgical procedure to open the thoracic cavity) was not performed. However, we placed a small-gauge chest tube in the thoracic cavity on his left side because we were concerned about the possibility of a large blood clot forming within the thoracic cavity. If this happened, a thoracotomy would be a necessity. We kept track of the total amount of blood drained from the chest and did repeated blood counts. We wanted to determine whether a blood transfusion would be necessary. By the next afternoon, we could no longer draw any blood through the chest tube.
The look of relief on Mrs. Robertson's face when she went home with Nike just made my day—for about 2 hours, that is, when she came rushing back in with Nike breathing hard again!
“I just let him out to go to the bathroom. I didn't think he'd try to run through the fence again!” she cried.
I looked at the poor little beast and just shook my head; we were going to have to do it all over again.
Summary
For a veterinarian or veterinary technician to perform a good physical exam on a patient's respiratory system, a detailed knowledge of the patient's anatomy is required. This includes the upper respiratory system as well as the lower respiratory system. Technicians, as part of their duties as veterinary anesthetists, routinely intubate patients using an endotracheal tube. To do this properly, knowledge of the internal anatomy of the larynx is needed.
In addition to the anatomical structures of the respiratory system, we also covered some of the physiological parameters that can be measured or estimated. Because much of the anesthesia performed on animal patients is gas anesthesia, an understanding of respiratory physiology is needed to understand the principles of anesthesiology. Key concepts in respiratory physiology include the movement of gases through the respiratory tree to the alveoli, the subsequent exchange of gases with the blood, and the concept of dead space. This chapter also introduced you to auscultation of the lungs and the normal and abnormal sounds that can be heard.
REVIEW QUESTIONS
1. Name the two parts of the respiratory system and the structures of which each is composed.
2. Differentiate between respiration and ventilation.
3. Differentiate between external respiration and internal respiration.
4. Name the six functions of the respiratory system.
5. What is the function of the sinuses?
6. What structure covers and thus closes the glottis during swallowing?
7. What structure alters the tension on the vocal ligament to change tones produced?
8. What structures combine to form the mediastinum?
9. Name the lung lobes on each side of the thorax in the cat.
10. How many cranial lobes does the ox have?
11. Name the branches of the bronchi from the trachea deep into the lung lobe.
12. Name the component structures of the respiratory unit.
13. In the bird, how many respiratory cycles are required to move one pocket of air through the lungs, and why?
14. Define tidal volume.
15. Define dead space.