The Digestive System
OBJECTIVES
• state the overall purpose and function of the digestive system
• using diagrams, identify the structural anatomy of the alimentary canal wall
• dissect the structures and organs of the digestive system, and identify them by name
• describe and identify the teeth of a cat or dog, including their dental formula and eruption table
• identify the parts of a tooth
• know the methods used in dental charting and the Triadan system of numbering teeth
• using a model or diagram, identify the parts of the equine large intestine
• using a model or diagram, identify the parts of the ruminant digestive system, including rumen, reticulum, omasum, abomasum, and the large intestine
• differentiate between the ansa spiralis of the ruminant and the pig
• know the parts of the fowl digestive system
MATERIALS
• cat cadaver, triple injected (order without skin attached)
• Mayo dissecting scissors
• probe
• 1 ? 2 thumb forceps or Adson tissue forceps
• #4 scalpel handle with blade
• bone-cutting forceps
• rubber gloves
• models of the equine colon and ruminant forestomachs and stomach
• three dogs for blood analysis, and two of the three for fecal analysis
• 10-ml graduated cylinders
• blood chemistry machine, amylase and lipase tests
Introduction
The digestive system is made up of the structures of the alimentary tract and the accessory digestive organs.
Its purpose is to ingest, digest, and absorb food and to eliminate the undigested remains as feces. It provides the body with the nutrients, water, and electrolytes that are essential for health and growth.The alimentary tract or canal is a hollow tube extending from the mouth to the anus. The interior of the canal is technically outside the body because the contents within make contact only with the cells that line the canal.
These cells are mostly the simple columnar epithelial cells studied previously. They protect the inside of the body from the bacteria and by-products of digestion found within the alimentary canal. For the ingested food to be available, it first must be broken down into smaller, diffusible molecules. The steps in this process are prehension, or using the mouth and lips to grasp the food; mastication, or chewing, which mixes food with salivary enzymes to both physically and chemically break it down; swallowing, moving the food through the esophagus to the stomach; digestion and absorption, which take place in the stomach and small intestines; and elimination via the large intestines and anus.180
The accessory digestive organs empty their secretions into the alimentary canal to aid digestion and absorption. These structures include the salivary glands, gallbladder, and pancreas. The liver is also considered—among other things—an accessory digestive organ. It is the largest gland in the body and performs many metabolic roles, such as formation of plasma proteins, vitamin storage, removal of foreign substances via Kupffer cells (phagocytic cells, also called stellate reticuloendothelial cells), detoxification, carbohydrate metabolism, and storage of glycogen. The liver's role in digestion is to produce bile, which leaves the liver via the hepatic ducts and is carried to the duodenum through the bile duct. When bile is not being used, it backs up through the cystic duct into a small reservoir sac known as the gallbladder. Bile emulsifies fats; in other words, it breaks the large fat particles into smaller ones. This allows the lipase released from the pancreas to break down the fat molecules into fatty acids for absorption.
The Structural Anatomy of the Alimentary Canal
The alimentary canal walls have four layers, or tunics. From the lumen outward, these are the mucosa, submucosa, muscularis (muscularis externa), and serosa (adventitia). Each of these layers is composed of a predominant tissue type and has a specific function in the digestive process (Figure 9.1).
The mucosa (mucous membrane) consists of surface epithelium (which in most cases is simple columnar epithelium), a layer of lamina propria (consisting of areolar connective tissue), and the muscularis mucosae (a thin layer of smooth muscle
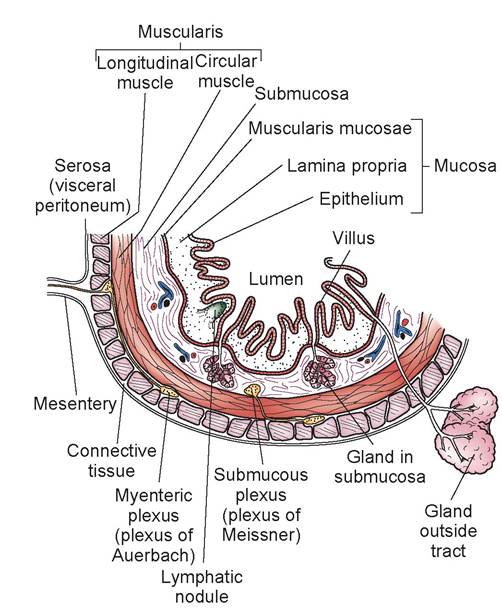
FIGURE 9.1: Basic structural pattern of the alimentary canal wall.
that enables local movement of the mucosa). The major functions of the mucosa are secretion (of enzymes, mucus, and hormones), absorption (of digested foodstuffs), and protection (against bacterial and endotoxin invasion). Each layer of the alimentary canal wall may be involved in one or more of these three functions.
The submucosa is composed of moderately dense irregular connective tissue and contains blood and lymph vessels, scattered lymph nodules, and nerve fibers. The layer’s intrinsic nerve supply is called the submucosal plexus. The submucosa’s major functions are movement of absorbed nutrients into the bloodstream, structural support for the canal, and protection. When a veterinarian places sutures in the wall of the intestinal tract, this is the layer that has the holding power.
The muscularis externa consists of two layers: an inner circular layer and an outer longitudinal layer, both composed of smooth muscle. Between the two layers is another intrinsic nerve plexus, the myenteric plexus. The muscularis externa and its nerve plexus are responsible for the gastrointestinal (GI) motility of the organ.
The serosa is composed of visceral peritoneum, which histologically is simple squamous epithelial tissue, and a thin layer of areolar connective tissue. In areas outside the abdominal cavity, the serosa is replaced by adventitia, a layer of coarse fibrous connective tissue that binds organs, such as the esophagus and rectum, to the surrounding tissues. The serosa, with its smooth surface and lubricating peritoneal fluid, reduces friction during contractions of the GI tract.
The adventitia anchors and protects the surrounding organs of the GI tract.Teeth
There are four types of teeth, classified according to their shape, function, and time of eruption.
The front teeth are called incisors (I) and are used cutting; the fang teeth are the canines (C), which are used for grasping; the next set of teeth are the
premolars (P); and caudal to the premolars are the molars (M). The premolars and molars are used for chewing, and since the molars have a flatter occlusal surface, they have a grinding function. The first set of teeth an animal grows are the deciduous teeth; these fall out and are replaced by the adult permanent teeth. As you can see from the dental formulas, only the incisors, canines, and premolars are deciduous.
Dental Formulas
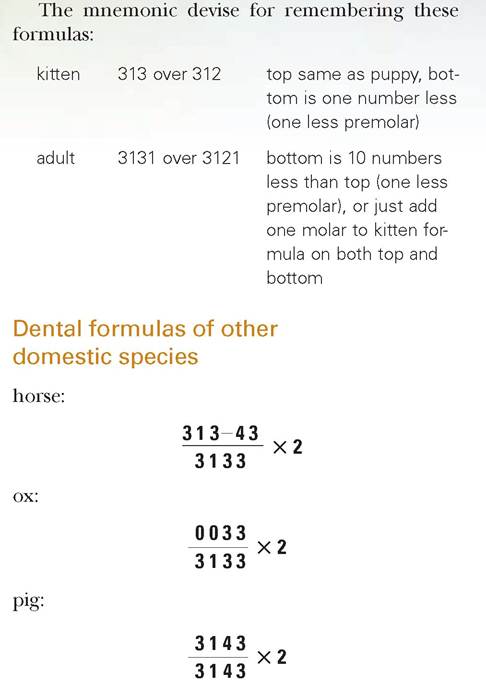
Students should know at least the dental formulas for the dog and cat, which are listed in the following paragraphs. The dental formulas for the other main domestic animals are listed at the end of this section.
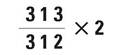
Dental formulas can be written in two ways. The first is with the numbers of teeth of each type on the upper arcade written over the numbers of teeth of each type on the lower arcade. For example, the adult dental formula for dogs is as follows.
The second method of writing this is to know that the order written is incisors, canines, premolars, then molars. Then you simply list the numbers of teeth of each type.
We multiply by two because you must consider both the left and right sides of the mouth to calculate the correct total number of teeth.
Using this same method, the dog deciduous formula is:
A mnemonic devise for remembering these formulas: It is easier to remember one number than many (i.e., it is easier to remember 313 than 3, 1, 3 in the dog deciduous formula).
Try remembering the formulas this way:puppy 313 over 313 top same as
bottom
adult 3142 over 3143 bottom one number
greater than top (translates to one more molar on the bottom)
Here is the formula for a cat’s deciduous teeth:
Similarly, the adult cat formula is as follows: 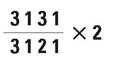
Aging a Dog or Cat
A student should learn to age a dog or cat using the eruption table shown in Table 9.1. Note that this is a simplified version showing the median age for the incisors. The figures in parentheses are the documented ranges.
The cat has approximately the same eruption table as the dog, except it has no upper P1, no lower P2 and P3, and no M2 or M3.
TABLE 9.1: Permanent Teeth Eruption Ages in the Dog
| Tooth | Age |
| I1 | 3 mos. (2-5 mos.) |
| I2 | 4 mos. (2-5 mos.) |
| I3 | 5 mos. (4-5 mos.) |
| C | 6 mos. (5-6 mos.) |
| P1 | 4-5 mos. |
| P2 | 5-6 mos. |
| P3 | 5-6 mos. |
| P4 | 5-6 mos. |
| M1 | 5-6 mos. |
| M2 | 6-7 mos. |
| M3 | 6-7 mos. |
Copyright 2010 Cengage Learning. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. Due to electronic rights, some third party content may be suppressed from the eBook and/or eChapter(s).
Editorial review has deemed that any suppressed content does not materially affect the overall learning experience. Cengage Learning reserves the right to remove additional content at any time if subsequent rights restrictions require it.
After the permanent teeth come in, aging an animal is an estimate based on tartar on the teeth, amount of wearing of the teeth, graying of the muzzle, and the overall condition of the dog or cat.
Dental Charting
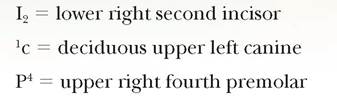
Currently there is no standardized method of tooth identification in veterinary medicine. Human dental insurance carriers have helped to standardize nomenclature for human teeth by using a numerical system. Veterinarians have been using a form of dental shorthand for years to identify a specific tooth and its corresponding quadrant. The letters indicating the type of tooth are the same as those used in the previously discussed dental formulas. Adult teeth are designated by capital letters, and deciduous teeth by lower-case letters. A number in superscript or subscript to the left or right of the letter indicates the quadrant the tooth occupies, and this is always based on the veterinarian viewing the animal from the rear.
For example:
Triadan System
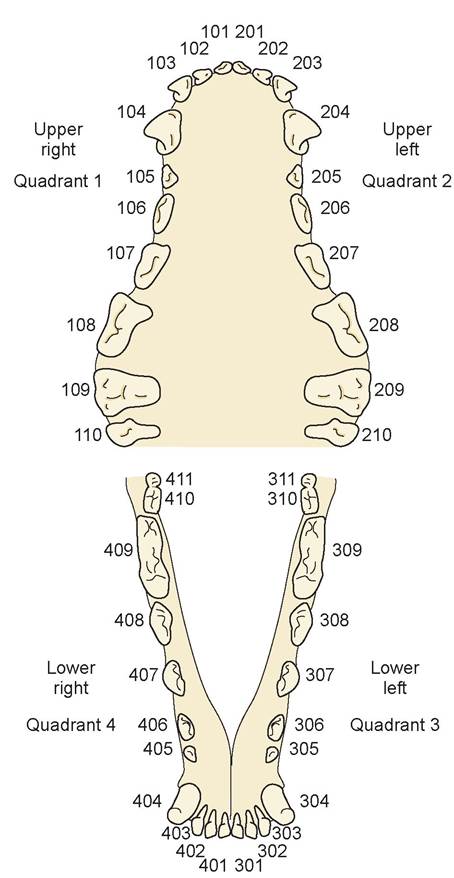
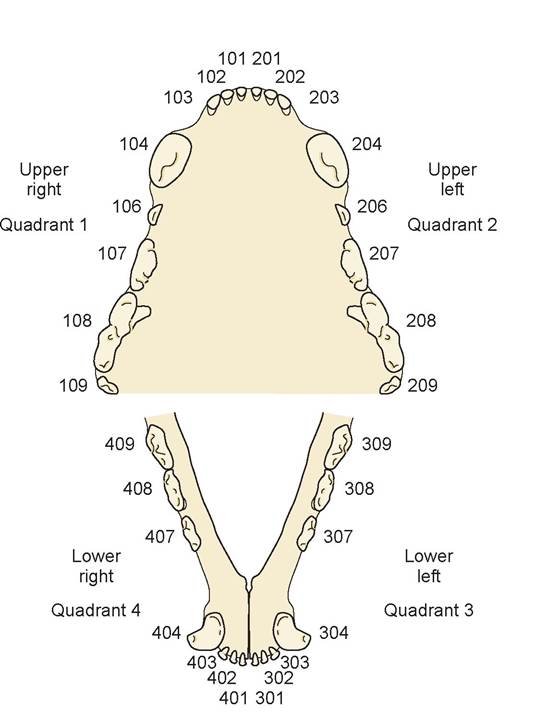
Most veterinary dentists are now using the Triadan system in which each tooth has a three-digit number. The first number represents the quadrant, starting with 1 on the animal’s upper right side and continuing clockwise (as viewed from the front of the animal’s head) to 4 on the lower right side. See Figure 9.2 for additional information. Quadrants for deciduous teeth are numbered 5 through 8.
Triadan Dental Numbering System - Dog
Triadan Dental Numbering System - Cat
FIGURE 9.2: Triadan system of tooth identification.
Copyright 2010 Cengage Learning. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. Due to electronic rights, some third party content may be suppressed from the eBook and/or eChapter(s).
Editorial review has deemed that any suppressed content does not materially affect the overall learning experience. Cengage Learning reserves the right to remove additional content at any time if subsequent rights restrictions require it.
Individual teeth are represented by the second and third digits. For example, all canines are numbered 04, and all first molars are numbered 09.Thus, the four canine teeth would be 104 to 404, starting on the upper right (104), upper left (204), lower left (304), and lower right (404). The same numerical pattern is used for each first molar, 109 to 409. This system works for both dogs and cats and takes into consideration that cats have fewer teeth than dogs. Cats have three premolars on the upper jaw and two premolars on the lower jaw, so in the Triadan system tooth 05 on the top and 05 and 06 on the bottom are not present. If you look at the shape of the cat’s teeth in comparison to the dog’s, it makes sense to identify the teeth by this method.
The Structure of a Tooth
Each tooth consists of a crown, neck, and root (Figure 9.3). The crown is the portion of the tooth that is visible above the gum, or gingiva. This portion of the tooth also can be called the clinical crown. The entire area covered by enamel is called the anatomical crown, and it extends a short distance into the neck area. The neck is the portion of the tooth between the gum line and where the gum attaches to the tooth, and it is associated with a slight constriction in the shape of the tooth. The root is the area below the neck that extends into
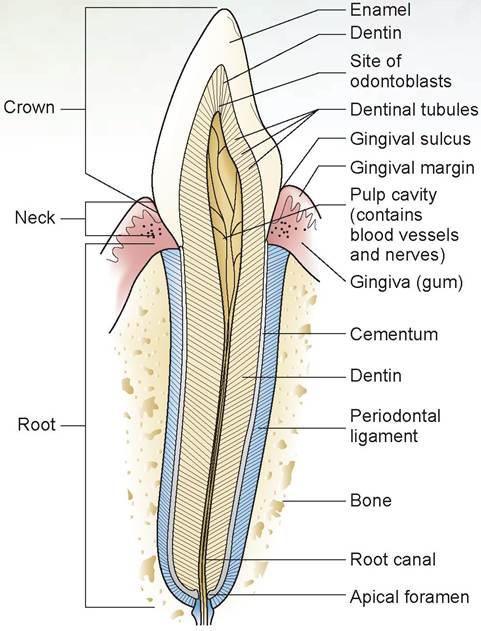
FIGURE 9.3: The structure of the tooth in a dog or cat.
the bone.
The crown is covered by enamel, which is the hardest substance in the body but is also fairly brittle. It is 95 to 97% inorganic calcium salts (chiefly CaPO4). The crevice (or space) between the margin of the gingiva and the limit of the anatomical crown (i.e., the enamel) is called the gingival sulcus, and its border is the gingival margin. The outermost surface of the root is covered by cementum, which is similar to bone in composition and less brittle than enamel. The cementum attaches the tooth to the periodontal ligament, which is the connective tissue that holds the tooth in the alveolar bone. The periodontal ligament also has a cushioning effect on the tooth.
The inner part, which is the bulk of the tooth, is called the dentin. It also is composed of a bonelike material. In the center of the tooth is the pulp cavity, which contains the pulp, a connective tissue containing blood vessels, nerves, and lymphatics. This provides the nutrients and sensation to the tooth. The odontoblasts, located on the outer margins of the pulp cavity, produce the dentin. The pulp cavity extends into the deep portions of the root and becomes the root canal. An opening at the root apex, called the apical foramen, provides a route of entry into the tooth for the structures found in the pulp cavity.
Teeth are either for cutting (shearing) or grinding. In all animals the incisors are used for cutting or shearing. Depending on whether an animal is a carnivore, an omnivore, or an herbivore, the premolars and molars have different amounts of grinding surface. A carnivore’s premolar and molar teeth have a relatively small amount of grinding surface, whereas omnivores and herbivores have a greater amount of grinding surface. In the dog and other canines, only the molars have a grinding occlusal surface; the same is true for the cat, but in the cat the molars are small and fewer (only one in each quadrant). Teeth that have a short crown are called bradydont teeth, while those with a long crown are known as hypsondont teeth.
EXERCISE 9.1 DISSECTION OF THE DIGESTIVE SYSTEM
Complete the following steps in the dissection procedure. The important organs and tissues to identify are listed in colored bold print. If a structure is mentioned before its dissection or its definition, it is italicized.
1. In the previous chapter you dissected the left side of the head and neck to expose the major salivary glands and lymph nodes of the cat. If any of the glands were destroyed during the dissection of the musculature, remove the skin on the right side of the neck and dissect out these structures. The salivary glands produce saliva, which is carried to the mouth via salivary ducts that pass through the head and neck musculature.
2. The largest salivary gland in the cat is the parotid salivary gland, which is located ventral to the pinna (Figure 9.4). This gland can be recognized by its lobular texture. The duct of the parotid crosses the masseter muscle and enters the oral cavity opposite the last upper premolar tooth. This is one of the reasons this tooth often has a lot of tartar buildup in older dogs. Two branches of the facial nerve also cross the masseter, dorsal and ventral to the parotid duct.
3. The mandibular salivary gland, which has the same lobular texture as the parotid gland, lies caudal to the angle of the jaw, ventral to the parotid gland (see Figure 9.4). The maxillary vein passes over this gland. This gland’s duct opens into the floor of the mouth near the lower incisors.
4. The smaller sublingual salivary gland (monostomatic part) is located rostral to the mandibular gland and the maxillary vein, and it is just superior to the mandibular lymph nodes. This gland also has a lobular appearance. Do not confuse this gland with the mandibular lymph nodes (which are smooth and elliptical in shape) located on either side of the linguofacial vein (which feeds directly into the jugular vein).
5. The cat has two additional salivary glands, the molar salivary gland, which lies near the angle of the mouth, and the infraorbital salivary gland on the floor of the orbit beneath the eye. They are hard to locate, and both, especially the latter, require difficult dissection.
6. On the side opposite the dissection of the salivary glands and lymph nodes (should be the animal’s right side), use a scalpel to incise through the masseter muscle from the corner of the mouth to just ventral to the parotid salivary gland. Then, using bone cutters, cut through the ramus of the
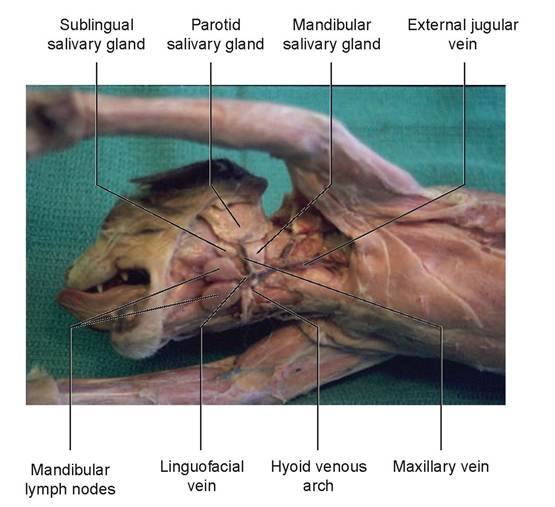
FIGURE 9.4: Salivary glands of a cat. mandible. As you start to pry open the oral cavity, use scissors to cut through the caudal tissue on the same (right) side all the way to the epiglottis. When you are done, the entire mouth and throat of the cat will be exposed, yet the structures of one side will be completely intact (Figure 9.5).
Locate the following structures in the oral cavity.
a. The vestibule is the area between the teeth and cheeks and lips.
b. The hard palate is the bony structure covered by tissue arranged in transverse ridges called the palatine rugae, and it makes up the roof of the mouth.
c. The soft palate extends caudally as a membranous continuation of the hard palate.
d. The fauces (a “space” bordered on each side by the palatoglossal arches, ventrally by the base of the tongue, and dorsally by where the soft palate starts) is the opening between the oral cavity and the oropharynx.
e. The two small palatine tonsils are masses of lymphatic tissue located on the dorsolateral wall of the oropharynx, about 1 cm caudal to the cranial edge of the glossopalatine arches.
f. The lips can be found on both the dorsal and ventral portions of the mouth.
g. The labial frenulum is the mucous membrane attached to each lip, upper and lower, at the midline.
7. The tongue lies on the floor of the oral cavity. Underneath the tongue is the lingual frenulum, the tissue covered by mucous membrane that anchors the tongue to the bottom of the mouth.
8. The dorsum of the tongue’s surface is covered with many papillae of four different types (Figure 9.6). The filiform papillae are the most numerous; they are hard, pointed, spinous projections with which the cat grooms its fur. The filiform papillae are located on the front half of the tongue. The fungiform papillae are small, more rounded, mushroom-shaped, and are located between and behind the filiform papillae. The vallate papillae are located on the top surface of the tongue laterally toward the base. There are only two or three of these on each side. Each is large and rounded and is surrounded by a circular groove (like a moat around a castle). The vallate papillae are difficult to see in a preserved cat. The last type are the foliate papillae, which are leaf-like projections located both at the base of the tongue and along the lateral sides. Microscopic taste buds are located on all the papillae except the filiform type.
9. Examine the teeth of the cat and number them using the Triadan system.
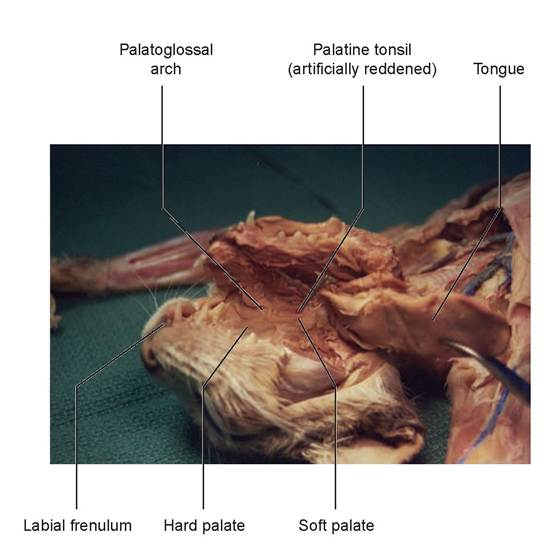
FIGURE 9.5: Dissected oral cavity of a cat.
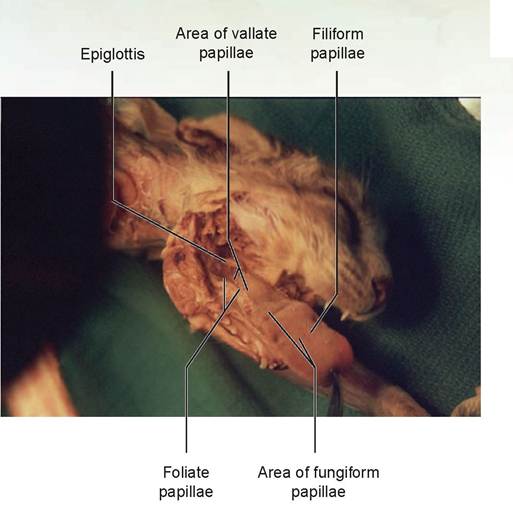
FIGURE 9.6: Tongue and epiglottis of a cat.
10. To expose the nasopharynx, make a small slit in the middle of the soft palate (see Figure 11.2 in Chapter 11). If you remember your skull anatomy, there is a depression just behind the internal nares bordered by the pterygoid bones. Inhaled air goes through the nasal cavity, exits through the internal nares, and enters the nasopharynx before proceeding to the larynx and into the trachea. In the dorsolateral wall of the nasopharynx are two small holes: the nasal openings of the auditory tubes or Eustachian tubes. These tubes go to the middle ear and help maintain the correct pressure within.
11. The oropharynx and nasopharynx are separated by the soft palate. Next, locate the Iaryngophar- ynx, or the part of the pharynx cranial to the larynx and dorsal to an open epiglottis. This part of the pharynx opens into the larynx and esophagus.
12. Locate the epiglottis, the pointed cartilage covered with mucous membrane,just in front of and below the larynx, caudal to the base of the tongue (see Figure 9.6). It closes the larynx and prevents fluids or food from entering during the swallowing process.
13. To study the remaining digestive organs, you must open the abdominal and thoracic cavities. First, locate the center of the pubic bone ventrally and make a small incision (large enough to permit entry of the blunt end of your scissors so you do not accidentally cut any organs). Open the abdominal cavity by cutting along the linea alba to the xiphoid process, just caudal to the sternum on the ventral midline. At this point, continue the cut cranially just to the left of the sternum (the animal’s left side), cutting through the costal cartilages up to the manubrium. Do not sever the blood vessels supplying the ventral body wall.
Observe the thin, transparent membrane dividing the chest cavity into two halves; this is the mediastinum. On the right side, locate where the diaphragm (the large, flat, muscular membrane that separates the abdomen from the thorax) meets the ventral chest wall. Using scissors, make two cuts about 2 cm apart: First feel with your index finger where the diaphragm attaches to the wall; then cut caudodorsally at an angle past your finger, making certain you are slightly caudal to the attachment of the diaphragm the entire distance of the cut. Make a second cut parallel to the first, only this time cut on the cranial side of the diaphragm (Figure 9.7). When you are finished, make these cuts on the left side in the same way. Now the abdomen and caudal thorax are visible, and both sides of the diaphragmatic attachments have been preserved.
14. Spread the chest wall so the heart and lungs are visible. Move the caudal lobe of the left lung out of the way and locate the esophagus, which runs along the dorsal wall of the thoracic cavity. It is best seen caudal to and behind the heart, just before it penetrates the diaphragm (Figure 9.8). The
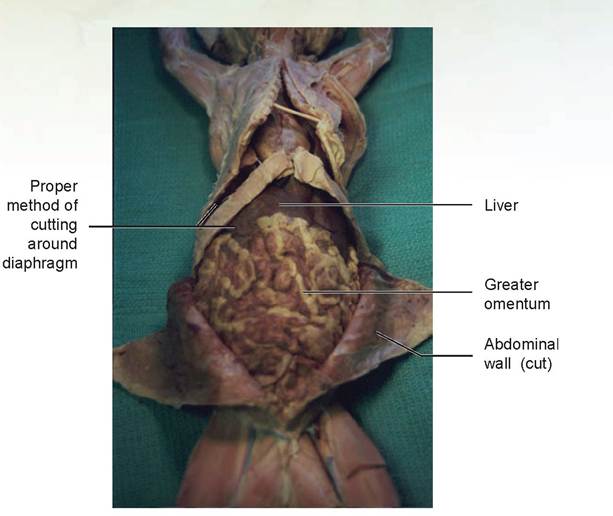
FIGURE 9.7: Proper method of cutting the abdominal wall and around the diaphragm of a cat.
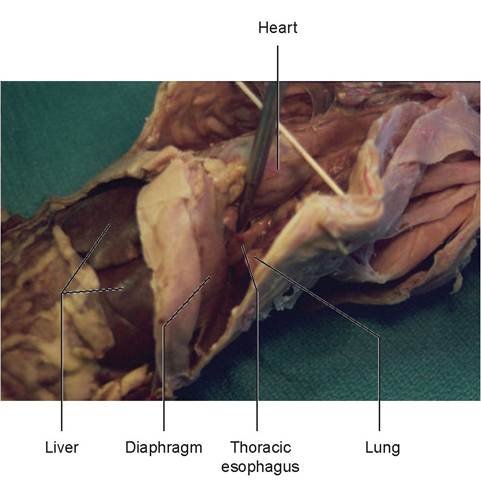
FIGURE 9.8: Thoracic esophagus, cranial to the esophageal hiatus, in a cat.
hole through the diaphragm where the esophagus penetrates is called the esophageal hiatus. The esophagus is the muscular tube connecting the Iaryngopharynx to the stomach. Try to visualize where the esophagus passes through the diaphragm.
15. Observe the greater omentum, the lacy structure containing adipose tissue, and covers and protects the ventral abdominal organs (see Figure 9.7).
16. The liver is the largest organ in the abdominal cavity. It is the reddish-brown structure located immediately caudal to the diaphragm. Observe the ligaments of peritoneum attaching the liver to the diaphragm and ventral body wall. The ventral ligament is called the falciform ligament (which may have been partially cut while opening the body wall), and the cranial one is the coronary ligament (Figures 9.9 and 9.10). The coronary ligament can be seen by moving the liver caudally. This
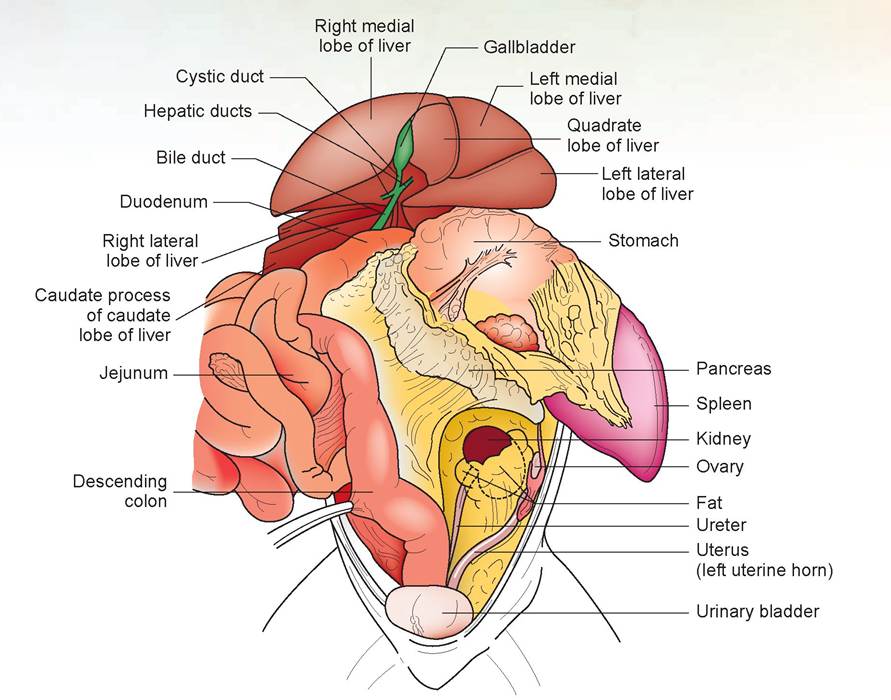
FIGURE 9.9: A cat's abdominal contents.
ligament is short and attaches the liver to the central tendon of the diaphragm (a sheet of connective tissue in the dorsomedial area of the diaphragm).
17. The falciform ligament divides the liver into right and left halves. Each half is subdivided into multiple lobes. These are named the right lateral and right medial lobes, the left lateral and left medial lobes, and the quadrate lobe (see Figures 9.9, 9.10, and 9.11). There is also a caudate lobe, which has two processes: The largest, located caudal to the right lateral lobe, is called the caudate process, whereas the smaller papillary process is located below the lesser omentum (Figure 9.12).
18. Observe the dark green gallbladder in a depression in the large right medial lobe (see Figures 9.9 and 9.10).
19. The largest part of the stomach lies mainly on the left side of the abdominal cavity. Separate the stomach and liver to observe the esophagus as it courses through the esophageal hiatus. There are four regions of the stomach (see Figure 9.11). The cardiac sphincter, or cardia, is the muscular valve that prevents esophageal reflux. The cardiac region is caudal to the cardiac sphincter and surrounds it for a short distance. The fundic region (or fundus) is the dome-like part of the stomach that projects dorsal to the cardia. The body of the stomach is the largest region and includes the majority of the greater curvature and lesser curvature. The pyloric region is distal to the body and extends from the level of the angular notch of the lesser curvature to the pylorus.
As noted previously, the shape of the stomach is such that it has two significant curvatures: the greater curvature, which is the larger outer curve located on the left lateral margin, and the lesser curvature, the smaller curve located on the inner medial margin of the stomach (Figures 9.12 and 9.13). The greater omentum is a double-membraned sac attached to the greater curvature, and the lesser omentum is attached to the lesser curvature. Because the greater omentum is a double-layered structure, there is a cavity, called the omental bursa, between the superficial and deep walls. To verify this, make a small, shallow tear in the omentum and insert your finger between the two layers.
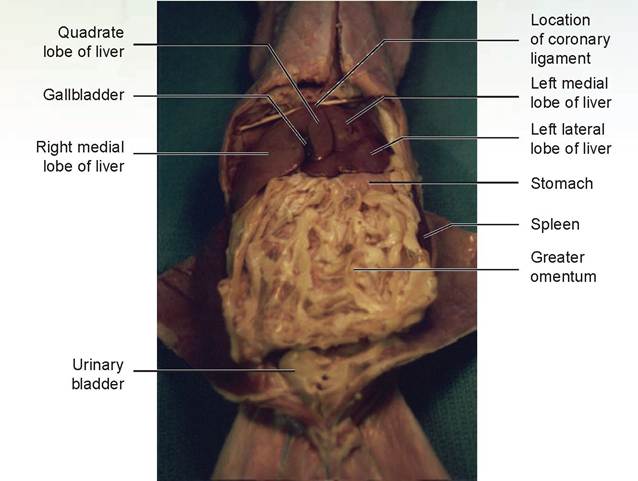
FIGURE 9.10: Ventral view of the lobes of the liver in a cat.
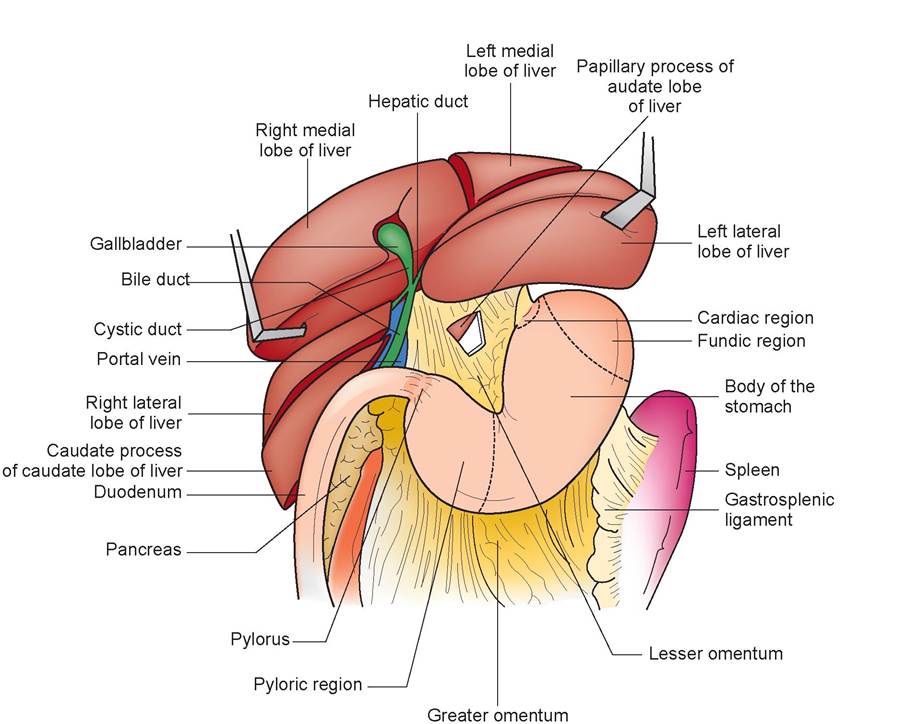
FIGURE 9.11: A cat's upper abdominal contents and underside of the liver.
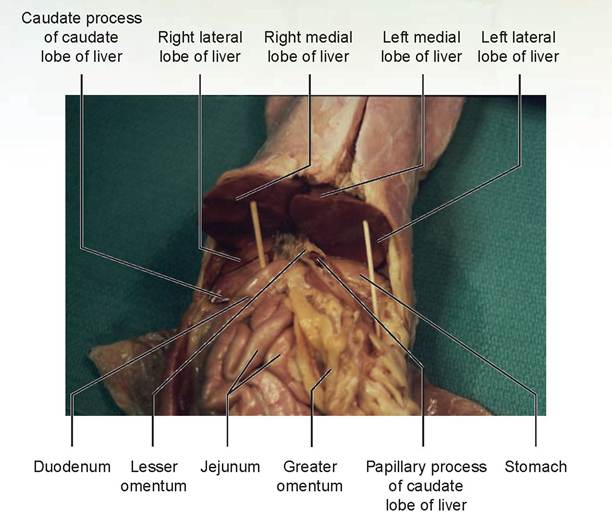
FIGURE 9.12: Underside of the liver in a cat.
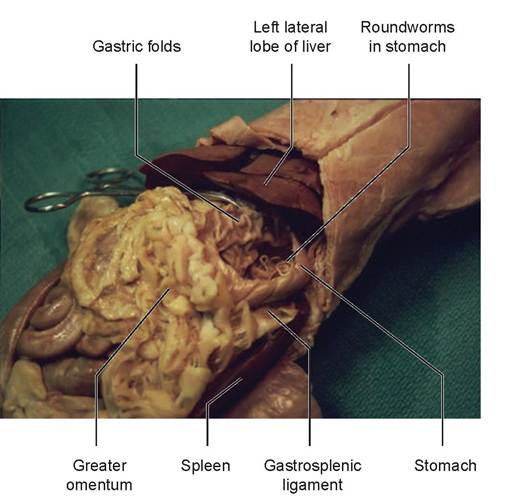
FIGURE 9.13: Stomach and spleen of a cat.
20. Make a longitudinal incision through the stomach wall, beginning in the esophageal region and continuing to the duodenum. Wash out the stomach’s contents. From the interior, observe the cardiac sphincter at the opening between the esophagus and stomach. Also look at the pyloric sphincter, which is between the stomach and duodenum. Notice the longitudinal gastric folds of the wall of the stomach called rugae.
21. Locate the spleen, the large reddish-brown organ to the left of the stomach and attached to it via the gastrosplenic ligament (see Figure 9.13).
22. Lift up the greater omentum and fold it back over the stomach so that the small intestines are visible. There are three parts that make up the small intestines. The first part is the duodenum. It courses from
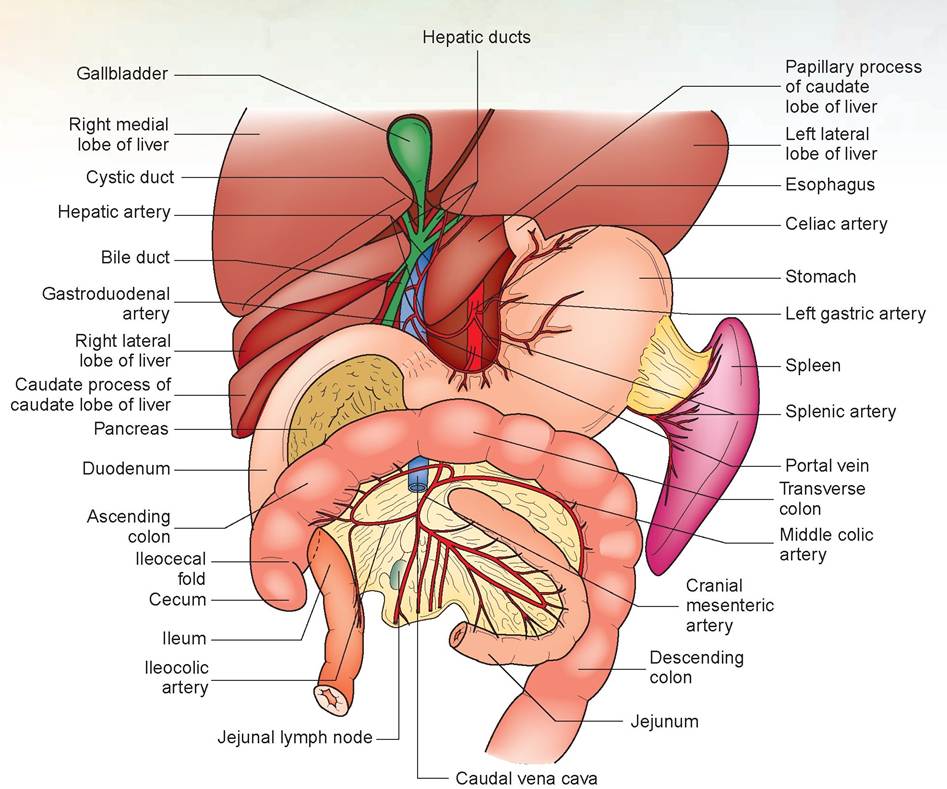
FIGURE 9.14: Ducts and vessels in the small and large intestines of the cat (most of the jejunum and part of the ileum have been removed).
the pylorus caudally on the right side (Figure 9.14). It ceases to be called the duodenum as it turns sharply around the root of the mesentery, which is the mesenteric extension of the parietal peritoneum from which the intestines hang when the cat is in its normal standing position (Figure 9.15).
23. Just medial to the duodenum and lying within its mesentery is the pancreas (see Figures 9.14 and 9.15). There are three parts of the pancreas: The body of the pancreas lies within the mesoduodenum and is attached to the duodenum; the left lobe is thicker and traverses across the abdomen between the layers of the deep wall of the greater omentum; and the right lobe is the free tip of the pancreas that separates from the duodenum. It can be recognized by its lobular appearance (similar to that of the parotid salivary gland, although darker in color).
Locate the sharp cranial flexure of the duodenum, found a short distance from the pylorus, where it curves caudally. Lift it up, view the dorsal side, and carefully dissect away the most cranial part of the body of the pancreas, just caudal to where the bile duct enters (the greenish duct connecting the liver to the duodenum; you will dissect this out in Step 30). By teasing apart the tissues, locate the main pancreatic duct in the interior of the pancreas. This is a white, thread-like duct carrying pancreatic juice to the duodenum. It attaches to the duodenum adjacent to the bile duct to form the hepatopancreatic ampulla at the exterior wall (Figure 9.16). The bile duct and the pancreatic duct continue within the wall of the duodenum and open to the mucosa at the major duodenal papilla. The sphincter of Oddi is a structure composed of smooth muscle that encircles the bile duct and main pancreatic duct as they traverse the wall of the duodenum. An accessory pancreatic duct may be found a short distance (approximately 1 cm) distal to the main pancreatic duct, and
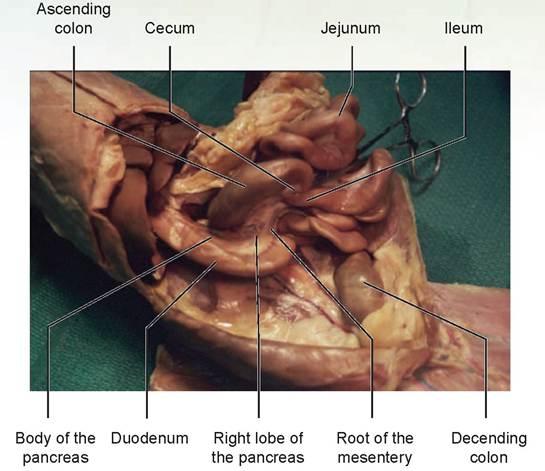
FIGURE 9.15: The small intestine of a cat.
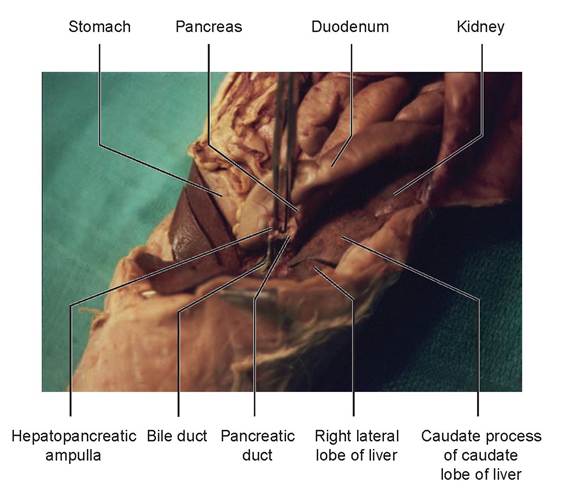
FIGURE 9.16: Main pancreatic duct of a cat.
forms the minor duodenal papilla. This papilla is present only in those cats with an accessory pancreatic duct (reported to be approximately 20% of cats); in the vast majority of cats you will not be able to locate it. These ducts carry the enzymes produced by the exocrine glands of the pancreas. (See Exercise 9.5 for more information on these enzymes.)
24. The second and largest part of the small intestine, the jejunum (Figure 9.17), is the next portion encountered; it makes up the majority of the length of this organ. The ileum is the last part of the small intestine; it opens into the large intestine. There is no gross demarcation between the jejunum and ileum except for a thin mesenteric ileocecal fold. Open the jejunum or ileum. The velvety appearance in the interior is due to the presence of numerous microscopic villi, which are fingerlike projections that aid in the absorption of food.
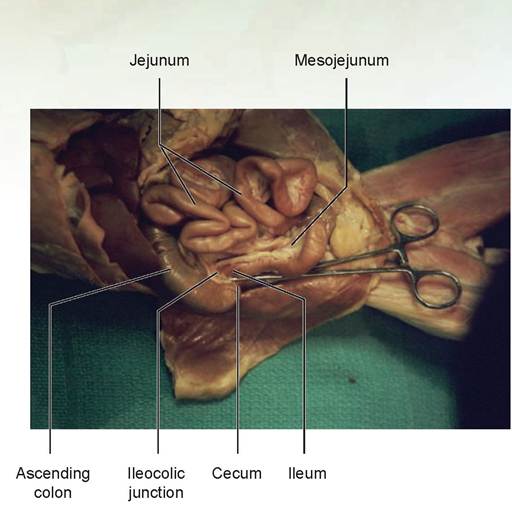
FIGURE 9.17: The ileum and the ileocolic junction of a cat.
25. Trace the ileum to where it enters the large intestine. This is approximately 0.5 to 1.0 cm from the tip of the cecum. This connection is called the ileocolic junction, a sphincter at thejunction between the small and large intestines. Make a longitudinal incision through the wall of the colon in the region of the juncture of the two intestines (see Figure 9.17).
26. The large intestine starts as a blind pouch known as the cecum (see Figure 9.17). The large intestine continues cranially on the right side as the ascending colon, arches transversely as the transverse colon, and continues caudally as the descending colon (Figure 9.18). There is no distinctive division between the ascending, transverse, and descending colons. The next part of the large intestine, the rectum, is located within the pelvic canal and opens to the exterior. This external opening of the rectum is known as the anus.
27. Examine the interior surface of the abdominal wall. The shiny membrane over the muscles is called the parietal peritoneum. The visceral peritoneum is the shiny covering on all the abdominal organs inside the abdominal cavity. These two layers are connected by the mesentery. The visceral peritoneum is also called the serosa or serosal surface of the intestinal organs. The serosa is made up of visceral peritoneum and areolar connective tissue, which attaches it to the underlying intestinal smooth muscles.
28. Identify the urinary bladder (see Figure 9.18), the small ventral organ located just cranial to the pelvic cavity, and the uterus, if your specimen is a female.
29. The portion of the peritoneal cavity between the urinary bladder and the uterus is called the vesico- genital pouch in the female. The rectogenital pouch is the space between the uterus and rectum. In males, the above pouches still exist due to a genital fold, containing the ductus deferens, which lies between the urinary bladder and rectum. These pouches are lined by visceral peritoneum.
30. The lesser omentum (or gastrohepatoduodenal ligament) can be seen extending from the left lateral lobe of the liver to the stomach and duodenum. Three important structures are located in the lesser omentum: the bile duct, the hepatic artery, and the portal vein. The bile duct is formed by a convergence of the hepatic ducts from each liver lobe with the cystic duct coming from the gallbladder. If the ducts contain bile, they will be green in color; otherwise, they are colorless and difficult to see. The bile duct enters the duodenum about 3 or 4 cm from the pylorus.
Carefully dissect away the lesser omentum and locate the hepatic artery dorsal and to the left of the bile duct. This vessel should be injected with red latex. The portal vein is located under the duodenum and beneath the bile duct as the cat is viewed on the table. Lift the duodenum and observe the dorsal surface of the lesser omentum and the duodenum to find this vein (Figure 9.19). It is a large vessel entering the liver. If it is not injected with yellow latex, it will be dark brown from the presence of coagulated blood. The portal vein is thin-walled and may be damaged during dissection.
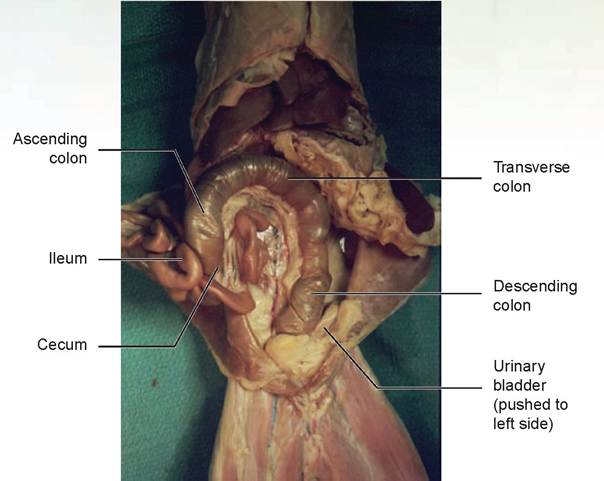
FIGURE 9.18: Large intestine, cecum, and parts of the colon of a cat.
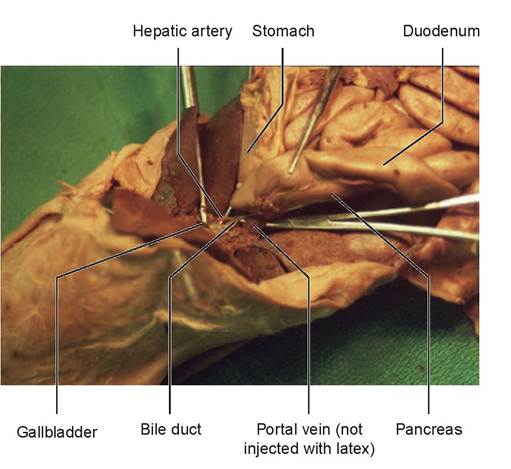
FIGURE 9.19: Bile duct, portal vein, and hepatic artery of a cat.
31. Lift a loop of the jejunum and find the large jejunal lymph node, located within the mesojejunum (see Step 32). Also note the arteries, veins, lymphatic vessels, adipose tissue, and other lymph nodes in the mesentery of the colon.
32. Each mesentery is named for the organ it supports; for example, the mesocolon is the mesentery attached to the colon, and the mesoduodenum is the mesentery attached to the duodenum. Locate and name these structures for each abdominal organ.
33. The kidneys and ureters are located dorsal to, or behind, the peritoneum. For this reason they are considered retroperitoneal.
EXERCISE 9.2 ANATOMY OF THE RUMINANT STOMACH
The process of digestion in the ruminants is classified as anterior fermentation; in other words, fermentation takes place anterior to the small intestine. The rumen is a fermentation vat in which bacteria and protozoa process cellulose and hemicellulose from ingested roughage and convert them to volatile fatty acids. These are absorbed by the ruminal papillae to produce energy. The volatile fatty acids provide more than 70% of the mature ruminant’s daily energy supply.
The rumen, reticulum, and omasum are considered the forestomachs, which are non-glandular and lined with stratified squamous epithelium. The abomasum is the true, or glandular, stomach. The reticulum and rumen are located on the left side of the animal, whereas the omasum and abomasum are located on the right. This is important when considering where the incision line will be so that the technician can clip the animal’s hair appropriately for an abdominal surgical procedure.
Procedure
Using Figure 9.20, find the following structures. Note that on the exterior, indentations are called grooves, whereas on the interior these grooves are called pillars.
1. rumen
a. esophageal sphincter
b. rumino-reticular orifice
c. rumino-reticular groove
d. ventral sac
e. dorsal sac
f. caudal dorsal and ventral blind sacs
g. caudal groove
h. right and left longitudinal pillar and/or groove
i. ruminal papillae
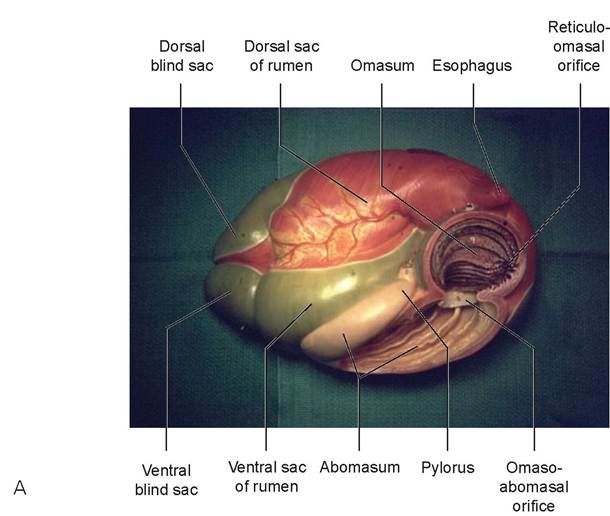
FIGURE 9.20: Ruminant stomach. A. Right side. (Courtesy of SOMSO Modelle, www.somso.de.)
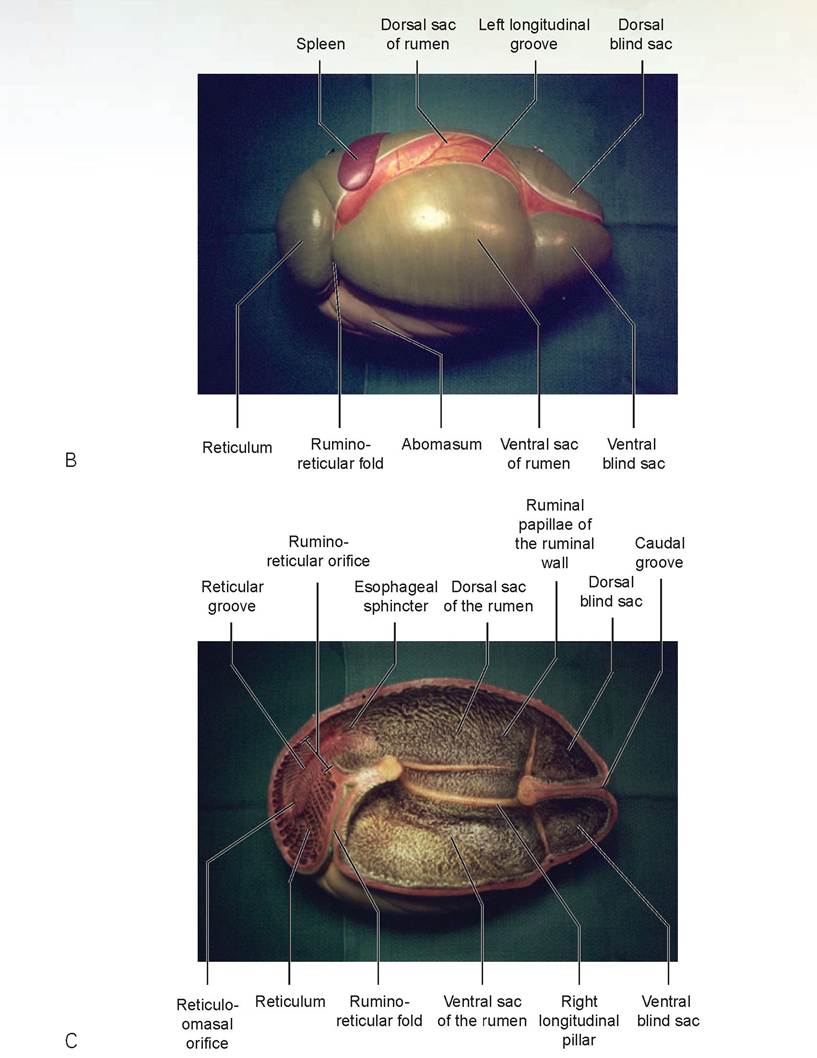
FIGURE 9.20, cont'd: Ruminant stomach. B. Left side. C. Interior view of the rumen and reticulum. (Courtesy of SOMSO Modelle, www.somso.de.)
2. reticulum
a. reticular groove or esophageal groove
b. reticulo-omasal orifice
c. honeycombed interior mucosal surface
3. omasum
a. studded laminae (aids to move food to the abomasum)
b. omaso-abomasal orifice
4. abomasum
a. cardiac region
b. fundic region
c. pyloric region
5. pylorus or pyloric sphincter
EXERCISE 9.3 COMPARATIVE ANATOMY OF THE LARGE INTESTINE
Locate the following structures (in bold or italic type) in the figures that follow.
Equines
Unlike the ruminants, the equine species is a posterior fermenter (i.e., fermentation takes place posterior to the small intestine). Because of this, the horse (and other equidae) has the largest and most complex large intestine of any domestic animal. For a large-animal veterinarian, knowledge of the horse’s extensive intestinal anatomy is crucial for the performance of a competent rectal palpation, and thus for an accurate diagnosis in a case of equine colic.
The cecum is large and comma-shaped and extends from the pelvic inlet to the floor of the abdominal cavity behind the diaphragm near the xiphoid cartilage. The ileum empties into the cecum, and from there the intestinal contents move to the great colon. This has four parts, and food moves through them
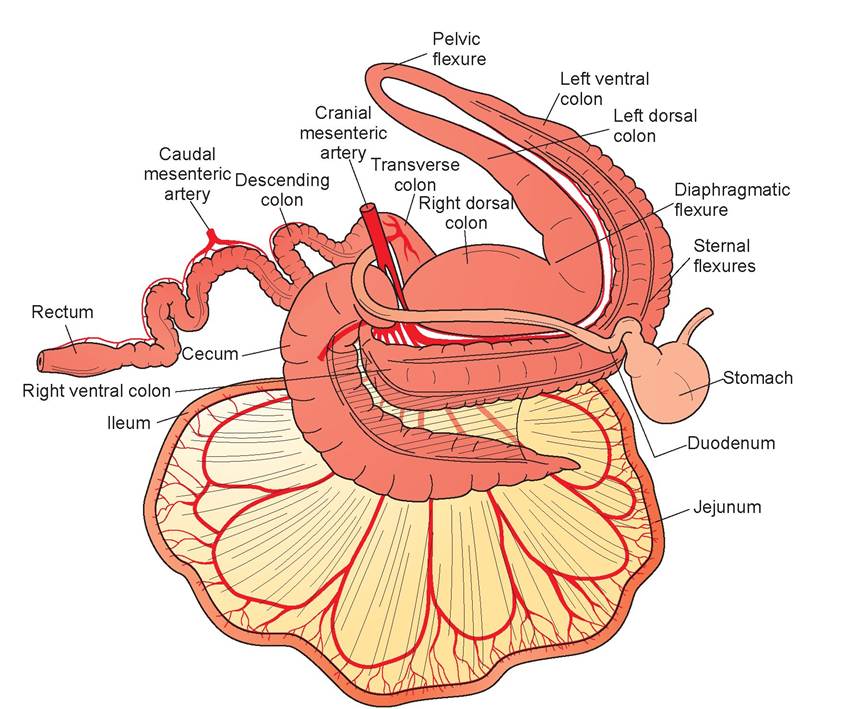
FIGURE 9.21: The gastrointestinal tract of the horse.
in the following order: (1) right ventral colon (bends at the sternal flexure); (2) left ventral colon (bends at the pelvic flexure); (3) left dorsal colon (bends at the diaphragmatic flexure); (4) and right dorsal colon (Figure 9.21). This then continues with the transverse colon, leading to the descending colon, then to the rectum. At the flexures and the entry to the relatively narrow transverse colon, foreign bodies may become trapped and cause problems. The large intestine in the horse is provided with sacculations and longitudinal bands. The former are separated by grooves, and the latter differ in number from segment to segment.
Ruminants
In the ruminants, as in the horse and the pig, the ileum empties its content into the cecum. From there the material moves into the ascending colon, which consists of the proximal loop (ansa proximalis), the spiral loop (ansa spiralis), and the distal loop (ansa distalis). The spiral loop is coiled and makes up the bulk of the ascending colon (Figure 9.22). From the distal loop the ingesta enter the transverse colon, then the descending colon, and finally the rectum. In all ruminants, large and small alike, the large intestine is smooth; neither sacculations nor bands are present.
Pigs
In the pig the ascending colon is similar to that of the ruminants, with three exceptions: There is no proximal loop, the spiral loop is very different, and most of the segments of the large intestine have sacculations and bands similar to those in the horse. The biggest difference is that the spiral loop is not nearly as symmetrically coiled as in the ruminants (Figure 9.23).
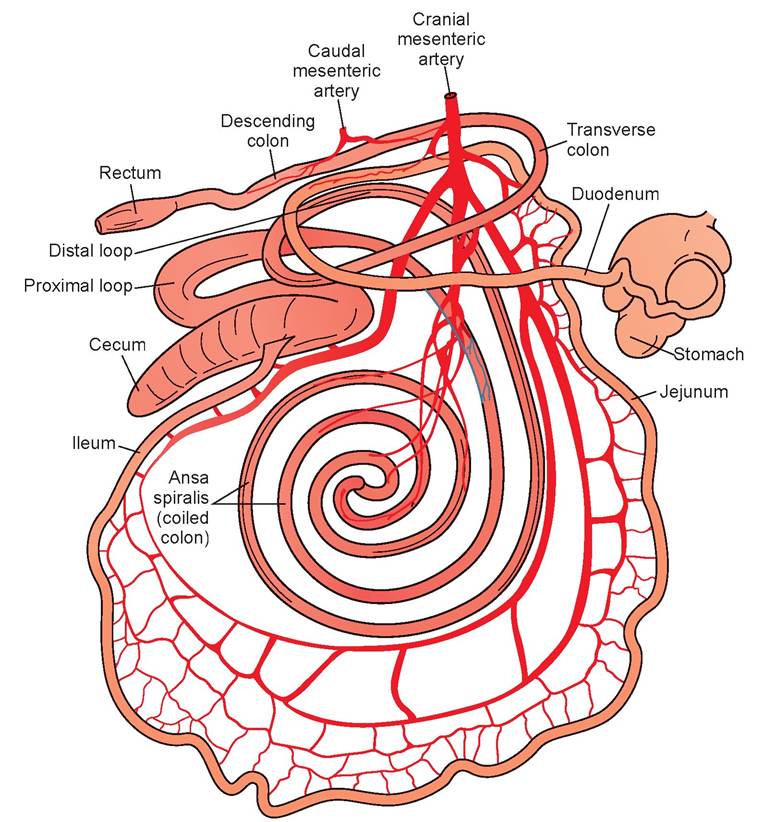
FIGURE 9.22: The gastrointestinal tract of an ox.
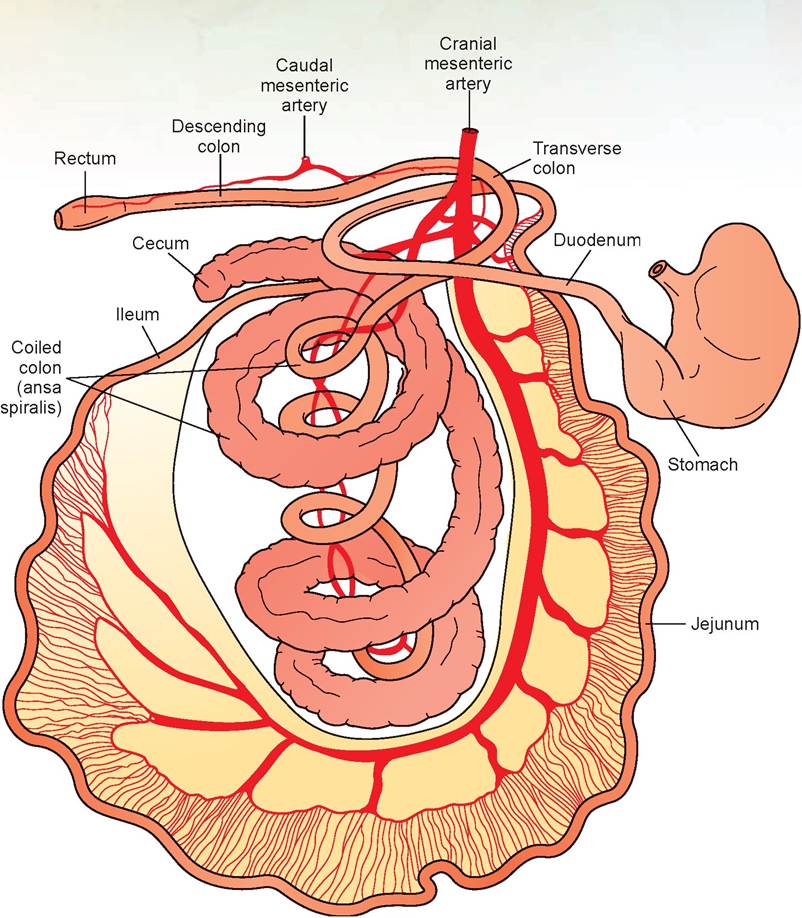
FIGURE 9.23: The gastrointestinal tract of a pig.
EXERCISE 9.4 DIGESTIVE ANATOMY OF THE FOWL
Locate the structures in bold type in Figure 9.24.
1. esophagus
2. The crop is a temporary food storage area where food waits until the proventriculus and gizzard empty. Enzymes that digest carbohydrates are secreted by the crop’s wall. Peristalsis moves food out of the crop and into the proventriculus.
3. The proventriculus has no storage function but mixes foodstuffs with pepsin, a proteolytic enzyme released from the cells within. Little acid is produced by this organ.
4. The gizzard macerates the food.
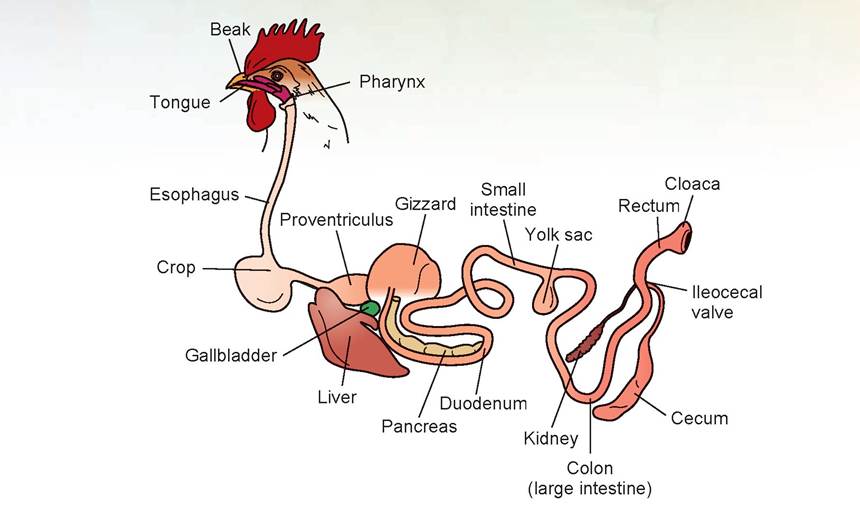
FIGURE 9.24: Digestive system of a chicken.
5. The small intestine has the same function as in other animals.
6. The large intestine also has the same function as in other animals.
7. The cloaca is the common opening for the gastrointestinal, urinary, and genital systems. In birds, the transit time for foodstuffs through the digestive system is very rapid. Feces begin to be formed 2 to 2.5 hours after food is ingested, and half the waste has been excreted within 5 hours.
EXERCISE 9.5 EXOCRINE PANCREATIC ENZYME ANALYSIS
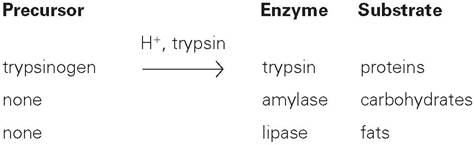
The pancreas is a mixed gland producing both enzymes and hormones. Enzymes are produced by the exocrine glands of the pancreas, and hormones are produced by the endocrine glands. As you may remember from Chapter 5, exocrine glands secrete their product onto an epithelial surface, whereas endocrine glands secrete directly into the bloodstream.
Two pancreatic enzymes are routinely assayed in dogs because their levels rise in cases of acute pancreatitis. These are amylase and lipase. A third enzyme, trypsin, can be assayed quantitatively or qualitatively in suspected cases of exocrine pancreatic insufficiency. The following list indicates the process by which these enzymes are produced by the pancreas, and the nutrients they digest.
Assays for Lipase and Amylase
The object is to quantitatively determine whether an animal’s pancreas is responding to the presence of fat and carbohydrates in the diet.
1. After three dogs (A, B, and C) have fasted overnight, draw blood from all three and perform the following:
a. Administer 3 ml/kg of corn oil to dog A.
b. Administer 3 ml/kg of 50% dextrose to dog B.
c. Keep dog C NPO (non per os, or no food taken in orally); this will be the control.
2. Draw blood from A and B again one hour after administration of the corn oil and dextrose, respectively, and again at 3 hours post-administration from all three dogs.
3. Using a blood chemistry machine, measure amylase and lipase in each sample. Make a graph of the results, using time on the x axis and mg% (milligrams percent) of amylase and lipase on the y axis.
Questions
1. Should there be a rise in serum levels of these enzymes if these enzymes are being secreted from the pancreas into the intestinal tract?
2. Was there a change in the appearance of the serum of either dog A or dog B at one hour or three hours post-administration?
3. If any of the dogs were exhibiting signs of pancreatitis (painful abdomen, vomiting), what changes would you expect to see in the enzyme levels of the pancreas?
Discussion
There should be no significant absorption of lipase or amylase back into the bloodstream from the intestinal tract after these enzymes are released by the pancreas in a normal animal. However, in an animal with an inflamed pancreas, the administration of a large amount of fat or dextrose could further stress the pancreas and cause release of these enzymes into the blood, and thus both lipase and amylase levels would be expected to rise. The serum of dog A should have become lipemic (white, cloudy appearance) at either 1 hour or 3 hours post-administration. (This occurs both in normal and in clinically ill dogs.) There should have been no change in the appearance of the serum from dog B.
Qualitative Assay for the Presence of Trypsin Using the Fecal Film Test
The object is to diagnose which dog is trypsin deficient. This is an older test that has been replaced by more modern assay methods, such as the trypsin-like immunoreactivity (TLI) test. However, it is a simple test to run and will demonstrate the presence or absence of trypsin.
1. Your instructor will provide samples of feces from two dogs. Label them dog A and dog B.
2. For each dog’s sample, using a graduated cylinder, bring 9 ml of 5% sodium bicarbonate to 10 ml total volume by adding feces. Mix well with a stirring rod.
3. Place a 3/4-inch wide strip of undeveloped x-ray film into the test tube (cut the strip so that it sticks out the top of the test tube about 1 inch).
4. Incubate the test tubes at 37 degrees centigrade for 30 minutes.
5. Remove the film strip, rinse under running water, and examine whether the gelatin on the end of the strip has been removed (by enzymatic action). If it has, the end of the strip will be transparent.
6. If the gelatin has been removed, this indicates the presence of trypsin.
Questions
1. In dogs with acute pancreatitis, feces have an increased fat content. Why might this occur?
2. What might be a clinical sign of exocrine pancreatic insufficiency, in which the digestive enzymes of the pancreas are not produced?
Discussion
In acute pancreatitis, lipase is not breaking down the pieces of fat in the duodenum. Therefore fat cannot be absorbed, and it is excreted in the feces. Animals that cannot produce sufficient enzymes for digestion will have weight loss and will appear malnourished after a long period of time, in spite of having a good appetite. They may also have chronic diarrhea.
Clinical Significance
Topics that could be discussed in this section include crop burns after eating food that is too hot in hand-reared birds, differentiating between malabsorption syndrome and exocrine pancreatic insufficiency in hungry dogs that are losing weight, and periodontal disease in dogs and cats. However, placement of Cesarian section incisions will be our focus.
When considering where to make an incision for a Cesarian section on a cow, ewe, or doe, knowledge of the abdominal anatomy and the arrangement of abdominal organs is crucial. The gravid uterus lies just above, or dorsal to, the mid-to-caudal ventral belly wall. To access this structure, there are generally two approaches: a paramedian incision between the midline and left mammary vein, or a linear incision starting in the left paralumbar fossa and extending ventrally. The former is done with the animal in dorsal recumbency, and the latter with the animal standing or lying on its right side.
Each incision has its advantages and disadvantages, both during the operation and during the post-op recovery period. If the approach were to be made on the right side, the small intestine and ansa spiralis would make access to the uterus impossible; for this reason it is not done. On the left side, there is an area just caudal to the rumen where the uterus is accessible. As a technician, knowing how a particular veterinarian likes to do this surgery and knowing the animal’s internal anatomy will help you correctly clip and prep the animal for surgery.

λ really hated this type of emergency call. Geoff Spencer had called to tell me his horse had [J severe colic. He lived about halfway between my hospital and Willamette Ski Bowl—about
70 miles up a winding, two-lane highway. It was the dead of winter, with the temperature dropping about as fast as my enthusiasm for my chosen profession. I might not have minded it so much if they had night skiing; after I cured this horse I could relax with a few runs on the slopes. But it was already getting dark, the roads were icy, and my car's right defroster wasn't doing the job it should have.
I'm not sure maybe I was just nervous, scared, or both... about the drive and about whether I
could cure this animal. The horse was reported to be rolling, sweating, kicking at its side, and getting up and down: classic symptoms of a very painful abdomen. I told Geoff to start walking the horse and not to let it roll. We didn't want a twisted intestine to complicate matters.
Veterinarians classify colic into two categories: of gastrointestinal origin and of non-gastrointestinal origin. Causes of non-gastrointestinal colic are conditions such as peritonitis, hepatitis, uterine torsion, urinary tract disease, or parturition (giving birth). The clinical signs of a colicky horse are classified as mild or severe.
A horse with mild colic is restless, anorexic, has an anxious expression in its eyes, and may be sweating and looking at its side. The gastrointestinal signs of this type of colic are yawning, stretching the upper lip, grinding the teeth, and abnormal feces. Behavioral signs include groaning, pawing the ground, getting up and down, stretching, a desire to roll, and tail twitching. Pain is classified as slight and intermittent.
In severe colic all the previously listed signs are present but are more severe. In addition, the horse may be depressed, may want to vomit, and may have profuse diarrhea. Other more severe behavioral signs include rolling, kicking at the belly, disregard for self and handlers, walking in short circles, and falling or suddenly dropping to the ground in pain. We also see labored breathing and profuse sweating. Pain is classified as continuous.
The diagnosis of the nature and cause of the colic is made based on The Eight Ps of Colic: pain (how severe?), pulse (how high?), peristalsis (increased or decreased?), perfusion of the mucous membranes, passage of a stomach tube (to note ability to pass the tube and the stomach's contents), palpation (by rectum), peritoneal fluid assessment (normal or not?), and packed cell volume (the percentage of red blood cells).
In this case the diagnosis was not tremendously difficult. The horse's colic was severe. After taking the horse's pulse (78 beats per minute, which is high), temperature (102°F, also elevated), and listening to its heart, lungs, and gut sounds, I performed a rectal palpation. There was a huge, solid, hard mass caught at the entry to the pelvic flexure, and there was no way, short of surgery, to get to it. I recommended transferring the horse to an equine surgeon, but Geoff did not want to do this and requested that I put the horse down. I am sure that the pain this horse was exhibiting weighed heavily in his decision. We were also facing the prospect of hauling a colicky horse on icy roads in the dark—and that was provided he could have borrowed his neighbor's horse trailer. Under the circumstances, he did what he thought was best, and I euthanized his horse.
“Dr. Cochran, how much will it cost to find out what caused this problem?” Geoff asked.
If I don't know the cause of a problem, my natural curiosity compels me to find the source of the physical symptoms of my patient by performing a necropsy. I told him I was about to suggest that. If we didn't find out what the foreign body was that caused this horse's problems, one of his other horses might ingest something similar.
I opened the horse's left side, starting my cut at the dorsal aspect of the paralumbar fossa. I immediately found the pelvic flexure, where the left ventral colon becomes the left dorsal colon. The object was stuck solidly in this flexure. I cut open the wall of the colon, pulled out the object, and washed it off. At first I didn't recognize what it was, but as the fecal material washed away, its shape became uncommonly clear to me. It looked like a white, ankle-length gym sock—wrinkled at the ankle as if it had been sitting in an old locker for years. This sock had become completely mineralized. It must have lain in the bottom of the cecum for years.
This horse had been a range horse for a period of time in its life, eating off the ground and picking up some mineralized dirt with its food. Why the horse had eaten this sock and how it made it through the small intestine to the cecum is a mystery, but it happened, and then something caused it to be expelled from the cecum. It was even surprising that the sock had made it past the sternal flexure, considering its size and shape.
Now we knew what had caused this problem, and chances are, this is one I will never see again.
Summary
The dissection of the gastrointestinal system of the cat should provide you with a good knowledge of the anatomy of monogastric animals (those having one stomach). We examined the structures of the mouth, esophagus, stomach, small intestine, large intestine, and accessory digestive organs. If time permitted and the specimens were available, a detailed study of the equine, bovine, porcine, and avian digestive systems would be included rather than just diagrams of their structures. By matching specimens to the diagrams provided, a study of the digestive system structures of the aforementioned animals and the bird would be greatly enhanced.
REVIEW QUESTIONS
1. What is the difference between the digestive tract and the alimentary tract?
2. Name the accessory digestive organs.
3. What is the function of the Kupffer cells of the liver?
4. Name the four layers or tunics of the alimentary canal.
5. Name the layers of the mucosa.
6. What replaces the serosal layer outside of the peritoneal cavity, such as the area of the rectum?
7. Name the four types of teeth.
8. Write the dental formulas for the adult dog and the adult cat.
9. Using a shorthand method for dental charting and the Triadan system, identify the fourth upper premolar on the right side, and the left lower canine tooth.
10. Name the three main parts of a tooth.
11. What must be broken down in order to extract a tooth?
12. Where is a tooth’s nerve located?
13. Which is the largest salivary gland?
14. Name the two frenula (singular: frenulum) that are found in the mouth.
15. Name the four types of lingual papillae, and indicate which have taste buds.
16. Fill in the blank: The esophagus penetrates through the diaphragm at the
17. Name the two ligaments attached to the liver ventrally and cranially.
18. Name the regions of the stomach.
19. What percentage of cats has an accessory pancreatic duct?
20. Where is the sphincter of Oddi?
21. What is the difference anatomically in the locations of the cystic duct, the hepatic ducts, and the bile duct?
22. Why is the abomasum not considered a forestomach in the ruminants?
23. What is the difference between an anterior fermenter and a posterior fermenter?
24. What is the function of the crop in the fowl?
25. The cloaca is the common opening for which three systems?