The Muscular System
OBJECTIVES
• identify and differentiate histologically the three different types of muscle tissue
• dissect the muscles of the cat and identify them by name
• gain a general knowledge of the origin, insertion, and action of the muscles dissected
MATERIALS
• prepared slides of skeletal, cardiac, and smooth muscle
• compound light microscope
• immersion oil
• colored pencils
• cat cadaver, triple injected (order without skin attached)
• mayo dissecting scissors
• probe
• 1 ? 2 thumb forceps or Adson tissue forceps
• #4 scalpel handle with blade
• rubber gloves
Introduction
The muscular system is closely tied to the nervous system.
This is illustrated by the fact that animals can consciously control the contraction of certain muscles. These muscles are classified as voluntary muscles. Other types of muscle that move independently of conscious thought are called involuntary muscles. Skeletal muscle, as you may remember, is striated and voluntary. Cardiac muscle in striated and involuntary, and smooth muscle is nonstriated and involuntary.147
Copyright 2010 Cengage Learning. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. Due to electronic rights, some third party content may be suppressed from the eBook and/or eChapter(s).
Editorial review has deemed that any suppressed content does not materially affect the overall learning experience. Cengage Learning reserves the right to remove additional content at any time if subsequent rights restrictions require it.
EXERCISE 8.1 MUSCLE HISTOLOGY
The purpose of this exercise is to demonstrate the microscopic anatomy of the three types of muscle tissue. It also illustrates the complexity of muscle anatomy, especially of skeletal muscle. As with previous chapters, obtain the recommended slide(s) and locate all the things you are instructed to view and that are labeled in the diagrams and photomicrographs.
Then, draw and label what you see in the space provided.Skeletal Muscle
Description: A muscle that is attached to bone is called a skeletal muscle. It is composed of multiple bundles of muscle tissue called fascicles (Figure 8.1). Each fascicle is surrounded by connective tissue known as the perimysium, which separates it from other muscle bundles. Perimysium is composed of reticular and collagenic fibers. The fascicles together make up the entire muscle and are surrounded by epimysium, which is composed of dense irregular connective tissue. These connective tissue layers contain blood vessels, nerves, and fat, which enable the cells to obtain nourishment, to receive nervous stimulation and contract, and to slide past each other with minimal friction. Fat deposits are visible in meat, and their appearance is called marbling. The epimysia of various muscles blend together to form the deep fascia, a coarse sheet of dense connective tissue that binds muscles into functional groups. The superficial fascia is less-dense connective tissue that connects subcutaneous tissue to the deep fascia.
Individual skeletal muscle cells are multinucleated and may be 3 or 4 cm long (depending on the species). The nuclei are locatedjust beneath the cell’s plasma membrane (the sarcolemma), which is called the hypolemmal position. A muscle cell is also called a muscle fiber. Inside the cell or fiber are numerous tubular bundles called myofibrils, which nearly fill the sarcoplasm (the cytoplasm of a muscle cell). These myofibrils are composed of even smaller threadlike structures called myofilaments. The myofilaments are composed largely of two varieties of contractile proteins, actin and myosin, that slide past one another during the contractile phase of muscular activity. Surrounding each muscle cell is the endomysium, made up of areolar connective tissue.
Slide: skeletal muscle, longitudinal section and cross section
On the longitudinal section slide, note the cross-striations; these represent the A, I, H, and M lines, bands, and zones of the sarcomeres (the contractile units) of the myofilaments.
The letters arejust labels; they do not refer to any specific name. In Figure 8.2 you can see the various lines, bands, and zones that are visible with normal light microscopy.The depiction of an electron micrograph in Figure 8.3A and the drawing in Figure 8.3B illustrate the arrangement of lines that gives striated muscle its appearance. The A band represents the thick myosin
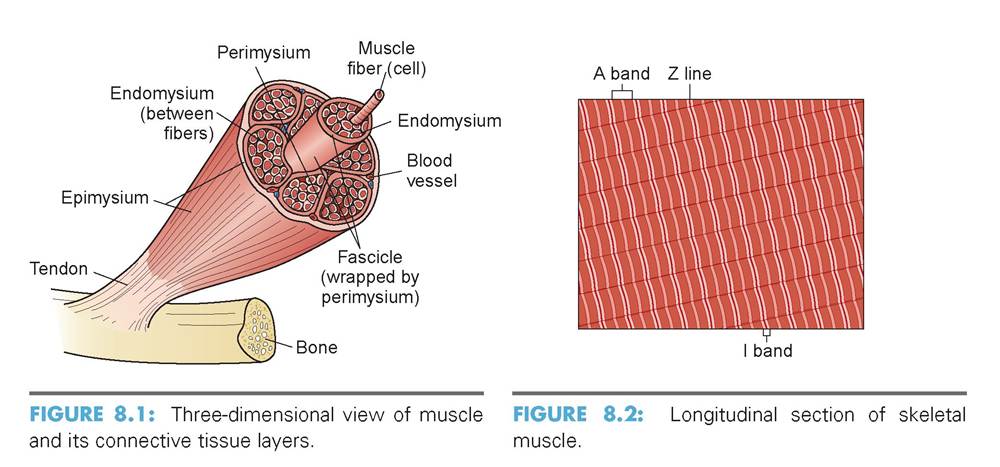
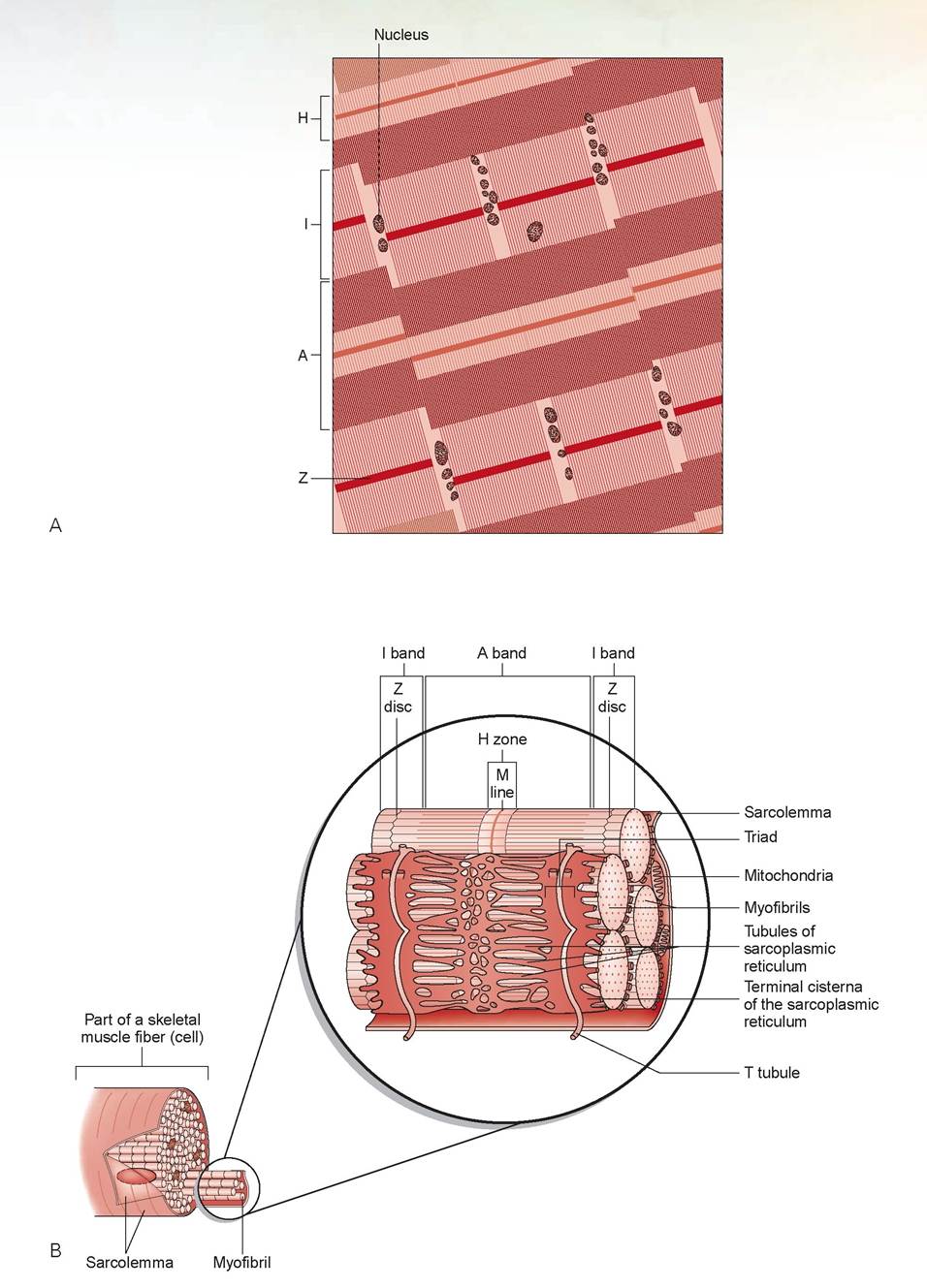
FIGURE 8.3: Skeletal muscle. A. Depiction of an electron micrograph. B. Microfibril structure with sarcoplasmic reticulum. Continued
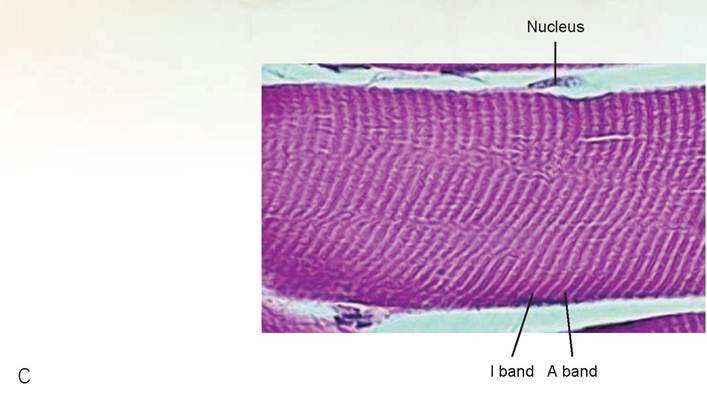
FIGURE 8.3, cont'd: Skeletal muscle. C. Skeletal muscle showing striated appearance.
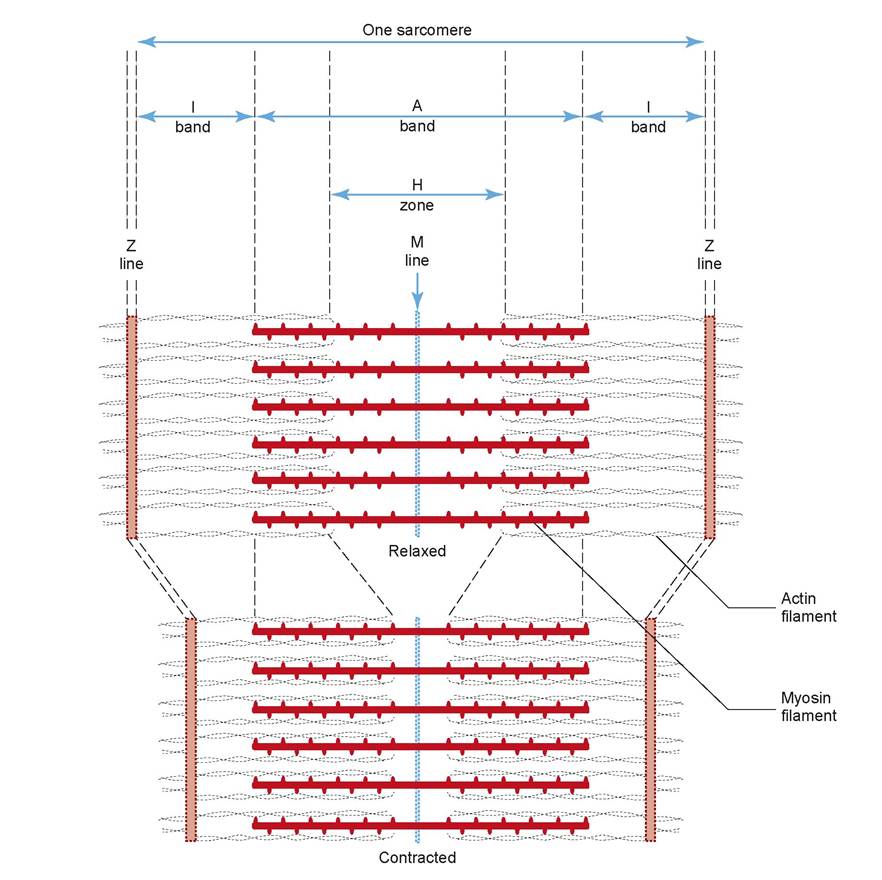
FIGURE 8.4: A sarcomere.
filament; it does not change in length. The thin actin filaments slide across the myosin during contraction. Because these filaments are anchored at the Z line, the Z-to-Z distance shortens during contraction (see Figure 4.4). The space between the two Z lines is a sarcomere, which represents the contractile unit of striated muscle. The sarcomeres of each myofilament line up together within each muscle cell; thus each band also lines up together. During contraction, the H zone and I bands shorten proportionally as the length of the sarcomere shortens. The M line is thought to be caused by transversely oriented, slender filaments that hold the myosin in place. All sarcomeres contract simultaneously, causing the entire myofibril to shorten, in turn causing the entire muscle cell to shorten. At each junction of the A and I bands, the sarcolemma indents into the cell, forming a transverse tubule (T tubule) that runs deep into the muscle cell.
Surrounding each myofilament is a web-like system of cross channels that make up the smooth endoplasmic reticulum, which is called the sarcoplasmic reticulum. It is thickest where it touches the T tubules (Figure 8.4).On the slide, find the muscle cell/fiber; the nuclei; the endomysium; perimysium (and perhaps a blood vessel within); the A and I bands; the H-zone; and possibly the M line.
Draw a section of skeletal muscle in the space provided, and label the parts of the cells.
Cardiac Muscle
Description: Cardiac muscle is involuntary and striated. It is different from skeletal muscle in that its cells are generally uninucleated, may branch, and anastomose with one another using special cell-surface modifications called intercalated discs.
Slide: cardiac muscle
The striations on cardiac muscle cells are not as noticeable as they are on skeletal muscle; instead, they appear as multiple, fine-lined cross-striations on each cell. Find the intercalated discs, the nuclei, and an example of a branching cell (Figure 8.5).
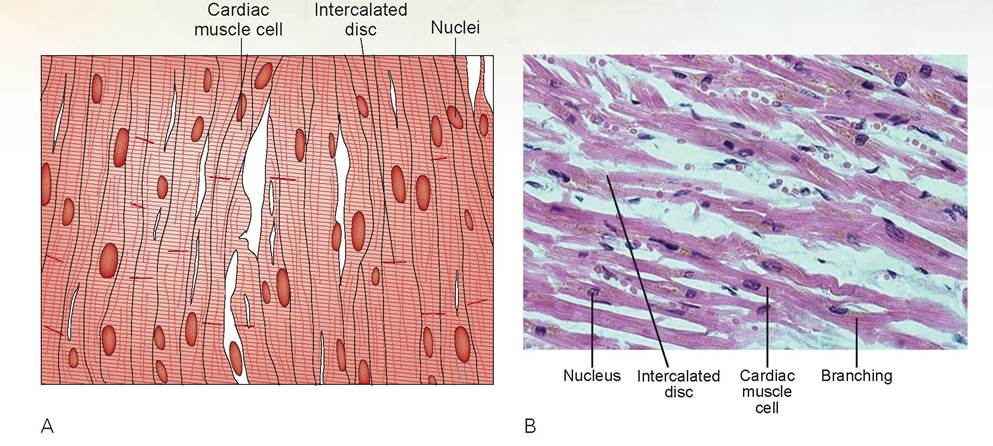
FIGURE 8.5: A. Cardiac muscle. B. Mammal cardiac muscle cells.
Draw a section of cardiac muscle in the space provided, and label the parts of the cells.
Smooth Muscle
Description: Smooth muscle is involuntary; it is found in organs that need to contract to move fluids, or it acts as a sphincter muscle to control the diameter of the opening in vessels and airways or between tubular organs. Smooth muscle cells are non-striated, have spindle-shaped cells with a central nucleus, and are arranged closely to form sheets. These muscle cells also contain actin and myosin, but smooth muscle does not have the orderly arrangement that skeletal muscle has.
Slide: smooth muscle or the intestinal tract
Smooth muscle cells are long and thin, tapered at both ends, and course in the same direction but are not perfectly parallel in configuration. The nuclei may appear rippled if the cell is contracting (Figure 8.6).
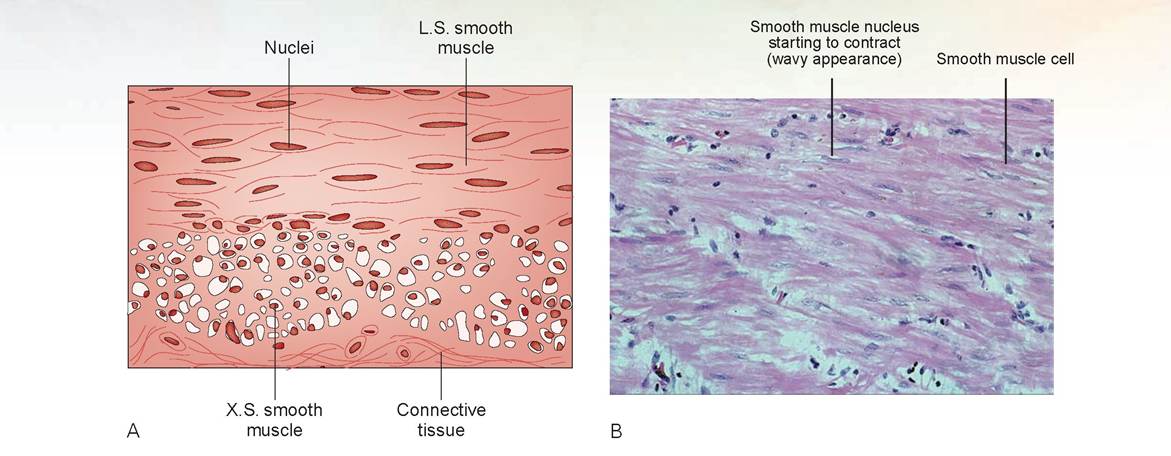
FIGURE 8.6: A. Smooth muscle. B. Mammal intestinal smooth muscle, longitudinal section.
Draw a section of smooth muscle in the space provided, and label the parts of the cells.
EXERCISE 8.2 DISSECTION OF THE CAT'S SKELETAL MUSCULATURE
The anatomical terms for the musculature of the cat differ from those used to name certain muscles in humans. Numerous cat-dissection manuals on the market use the analogous human muscles’ names, but these are used in human anatomy and physiology classes in the allied human health professions. The textbook used as the definitive veterinary source for naming these muscles is the Atlas of Feline Anatomy for Veterinarians by Hudson and Hamilton.
The important muscles to identify in this exercise are listed in colored bold print. If a muscle is mentioned prior to its dissection, it will be italicized. Also realize that there are many muscles in the cat that you will not dissect out; these are generally the smaller, deeper muscles.
Each muscle has an origin (the site of attachment to a fixed bone) and an insertion (the attachment to a more freely movable bone). As a muscle contracts, it pulls the insertion toward the origin. This is known as the action of the muscle. If you know a muscle’s origin and insertion, in most instances you can determine its action. Muscles may originate directly from the bone or from fascia above the bone, and they are often attached to their insertion by tendons. You will remember from your study of histology that tendons, ligaments, and aponeuroses are made of dense regular connective tissue, which are linear parallel bands of collagenous fibers.
Some muscles insert by means of an aponeurosis, a broad flattened sheet of tendon.In the following dissection guide, locate each muscle before making any incisions or attempting to transect the muscle. Clean the surface of each muscle by gently pulling off or cutting away superficial fat. With this method you should be able to see the direction of the muscle fibers. Generally, all the fibers of a muscle will run in one direction, and the fibers of the muscle that is adjacent or deep to it will run in a different direction.
As mentioned previously, muscles are separated from one another by sheets of fascia that envelop each muscle. Discovering these separations will enable the dissector to effectively isolate each muscle. A scalpel or knife can often create false separations; therefore, it is best to use blunt separation whenever possible. This is best accomplished using a probe, the blunt end of a scalpel, your fingers, or scissors (by continually spreading the tips open). Surgeons use scissors (or forceps) to spread tissues apart to minimize bleeding. When separating, leave the fascia that surrounds the muscle attached. This should ensure that the entire muscle is intact and that there are no artificial separations.
To examine the deep muscles, it is frequently necessary to cut through a superficial muscle. Do not bisect a muscle unless directed to do so. To bisect (or transect) means to cut into two parts. When bisecting a muscle, cut through it at right angles to the direction of the muscle fibers, halfway between the origin and the insertion, using scissors or a scalpel. To see the underlying muscles, reflect the superficial muscle: pull the ends back, one toward the origin and the other toward the insertion. If these directions are followed, the origin and insertion of the muscle will be retained.
Part 1: Superficial Muscles of the Chest
Complete the following steps in the dissection procedure.
1. Clean the fat off the surface of the muscles on the left side of the chest. We will not dissect the right side unless errors have been made on the left.
2. Locate the pectoralis muscles, the large group that covers the ventral chest. The group originates from the sternum and inserts on the humerus, or close to it. Locate the muscles in this muscle group (discussed in the following steps) by comparing the cadaver’s muscles with Figure 8.7. The action of this muscle group is to adduct the limb medially.
3. The pectoralis descendens muscle (M. pectoralis descendens) (name used in previous cat dissection guides is the pectoantebrachialis) is the most superficial muscle of this group. It is approximately 0.5 in wide and extends from the manubrium of the sternum to insert on the fascia of the forearm. The cranial edge of this muscle is about 0.3-0.5 in from the beginning of the entire pectoralis group. It is a thin muscle and must be carefully dissected from the pectoralis transversus. Separate this muscle from the underlying fascia and muscle.
4. The pectoralis transversus muscle (M. pectoralis transversus) (previous cat dissection guides use the terms pectoralis major or superficial pectoral) is the portion of the pectoralis group deep to the pectoralis descendens and cleidobrachialis. It originates on the upper part of the sternum and inserts along much of the humerus. It can be difficult to dissect from the more caudal (and caudolateral) pectoralis profundus and may appear to have two bodies or sections. The key to this dissection is to note that the fibers of the pectoralis transversus course in the same direction or slight craniolaterally (especially in the caudal part) as those of the pectoralis descendens. There is a slight separation in the fascia where the pectoralis transversus and the pectoralis profundus meet. This muscle is also not very thick, and as you start bluntly dissecting this muscle from the deeper pectoralis profundus, you will see that the deeper muscle’s fibers actually run cranially under the pectoralis transversus. Also loosen this muscle away from the cleidobrachialis at its cranial border. Note its wide insertion on the humerus.
5. The pectoralis profundus muscle (M. pectoralis profundus) (known in previous guides as the pectoralis minor) lies caudal and deep to the pectoralis transversus. It originates on the middle portion of the sternum and inserts near the proximal end of the humerus. In the cat, this muscle is larger than the pectoralis transversus. The caudal part of the pectoralis profundus muscle was once dissected as a separate muscle and in older dissection manuals was labeled the xiphihumeralis. It need not be
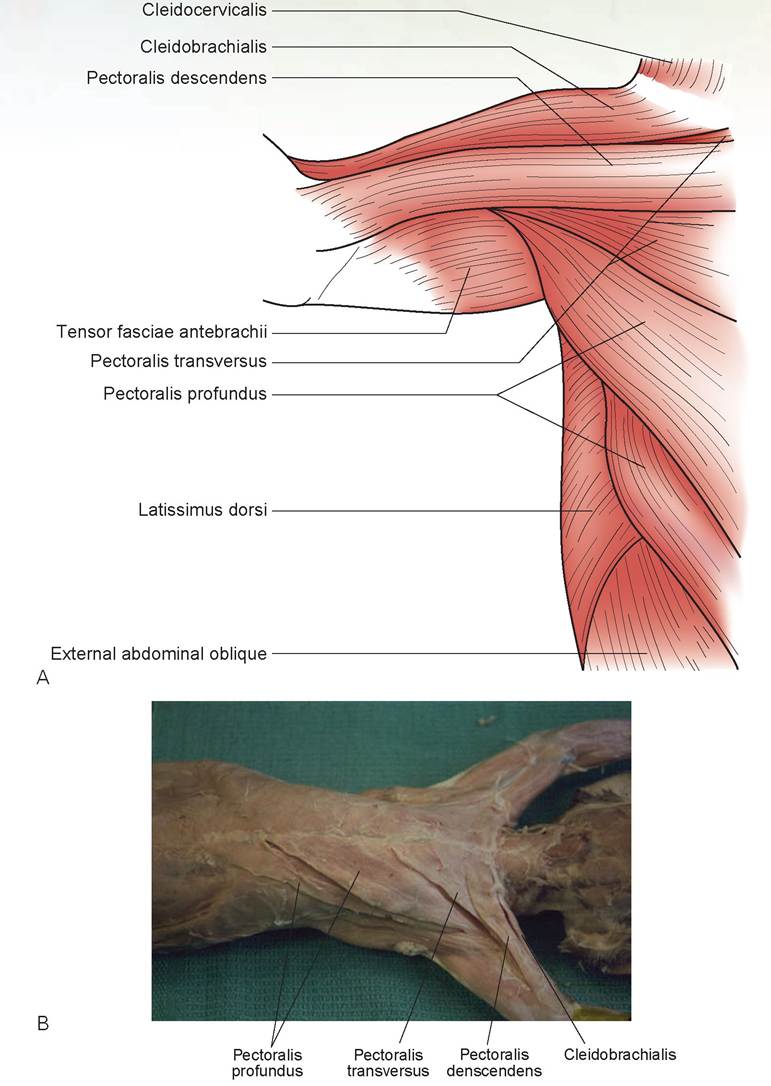
FIGURE 8.7: A. Ventral view of chest musculature. B. Ventral view of chest musculature of a cat.
separated as shown in Figure 8.7. Start caudally at its origin and work cranially, undermining and separating the caudalateral margin from the fascia and latissimus dorsi muscle. The muscle becomes a tendinous-appearing band as it passes deep to the pectoralis transversus and inserts on the humerus.
6. The muscle on the shoulder cranial to the pectoralis descendens is the Cleidobrachialis muscle (M. cleidobrachialis) (the clavodeltoid in previous guides). By blunt dissection, separate the cleido- brachialis from the connective tissue deep to it. Palpate the clavicle on the underside of the medial end of this muscle (toward the neck). The cleidobrachialis originates on the clavicle and inserts on the ulna with the pectoralis descendens. It appears as a continuation of the cleidocervicalis on the shoulder. Its action is to help draw the limb forward.
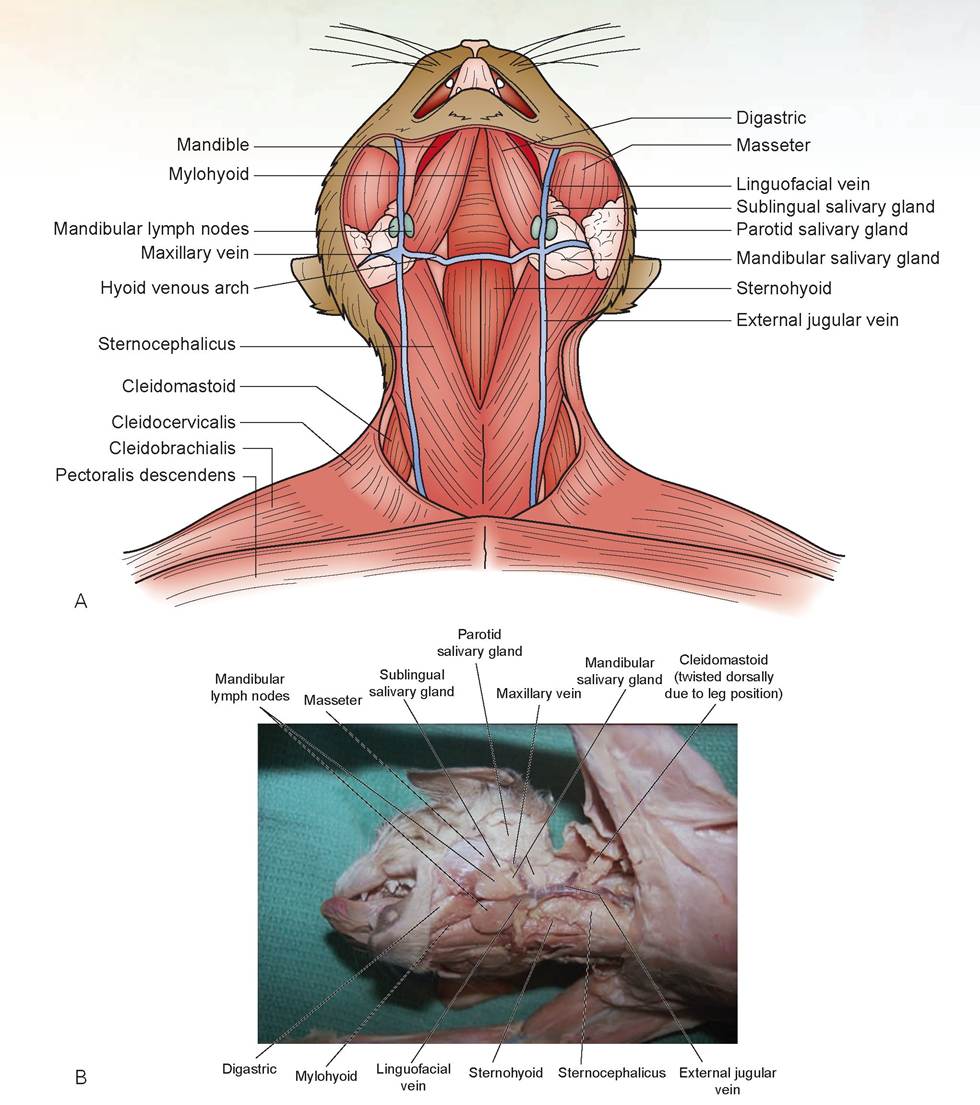
FIGURE 8.8: A. Ventral view of the neck musculature. B. Ventral view of the neck musculature of a cat.
Part 2: Superficial Muscles of the Neck
1. Remove additional skin from the left side of the neck up to the base of the ear. Be careful not to cut or damage the external jugular veins or the hyoid venous arch. The external jugular is the large vein that lies on the ventral surface of the neck, and the hyoid venous arch connects the right and left external jugular veins at the level of the larynx. At this time, free these veins from the underlying muscles. (Refer to Figure 8.8 during this dissection.)
2. Remove any excessive superficial connective tissue or fat from the back of the left shoulder and from the ventral and lateral surfaces of the neck. Do not remove the fascia in the midline of the back because it is part of the origin of the trapezius muscle.
3. The Sternocephalicus muscle (M. Sternocephalicus) has two parts, mastoid and occipital, known as the Sternomastoid and sterno-occipitalis muscles. They are difficult to separate by dissection, and it is easier to just identify the main areas of these muscles by their thickness and shape. They originate as a unit from the manubrium sterni and course diagonally to insert on the mastoid part of the temporal bone and the dorsal nuchal line of the occipital bone of the skull (see Figure 8.8). The sternomastoid muscle is the ventral portion and separates as a thick, elliptical bundle that unites with the cleidomastoid as a strong tendon at its insertion. Both parts of the muscle pass deep to the external jugular vein. The sterno-occipitalis is the broad, thinner, dorsal segment that lies immediately cranial to the cleidocervicalis. The action of this muscle is to turn and bend the head. Separate both borders of this muscle.
4. Next, locate the sternohyoid muscles (M. sternohyoideus). These are a narrow pair of muscles that are connected together along the midline, just superficial to the trachea in the middle of the neck. The caudal ends are covered by the sternomastoid. The sternohyoids originate from the first costal cartilage of the sternum and insert onto the hyoid bone. Its action is to pull the basihyoid bone and tongue caudally.
5. The cleidomastoid muscle (M. cleidomastoideus) is a narrow band of muscle, of which the cranial part passes deep to, and the caudal part courses dorsolateral to the sternomastoid muscle (see Figure 8.8). It originates on the clavicle deep to the cleidocervicalis and inserts on the mastoid region of the temporal bone. Its action is to help draw the limb forward and also to fix the neck, holding the head in one position. Locate this muscle by looking between the sternomastoid and cleidocervicalis. Then separate the cleidomastoid along both borders.
6. The digastric muscle (M. digastricus) is a thin, superficial muscle that runs adjacent to the inner surface of the mandible (see Figure 8.8). It originates on the occipital and temporal bones and inserts on the mandible. Its action is to help open the mouth.
7. Inserting deep to the digastric and bridging the two sides of the mandible is the mylohyoid muscle (M. mylohyoideus). To see its fibers you must carefully remove the thin deep fascia that covers this muscle. The mylohyoid is a thin, sheet-like muscle with transverse fibers; it originates on the mandible and inserts on the median raphe (the connective tissue along the midline). Its action is to raise the floor of the mouth.
8. Note the large parotid salivary gland located ventral to the ear. The large muscle mass cranial to this gland at the angle of each jaw is the masseter muscle (M. masseter). It originates from the zygomatic arch and inserts onto the mandible. Its action is to close the jaw.
9. Other structures to find are the remaining salivary glands and the lymph nodes. Located inferior to the parotid salivary gland is the large mandibular salivary gland. Just cranial to this gland is the small sublingual salivary gland (monostomatic part). These glands are separated cranially and caudally by the maxillary vein, and lie deep and dorsal to the external jugular vein and caudal to the transverse jugular vein. The linguofacial vein is the cranial branch that feeds into the jugular vein; on either side are two small mandibular lymph nodes (see Figure 8.8).
Part 3: Superficial Muscles of the Shoulder and Back
1. The cranial extension of the cleidobrachialis muscle (dorsal to the clavicle) is the cleidocervicalis muscle (M. cleidocervicalis) (in previous guides called the cleidotrapezius). This is the broad muscle located on the back and side of the neck, dorsal to the sternocephalicus muscle. It originates from the occipital bone and the first few cervical vertebrae and inserts on the clavicle. The action of the cleidocervicalis is to elevate the clavicle.
2. The trapezius muscle covers much of the dorsal surface of the scapula (Figure 8.9). It is divided into two parts: the cervical part (in previous guides called the acromiotrapezius) and the thoracic part (in previous guides called the spinotrapezius). The cervical part covers the dorsal part of the scapula. It is a fan-shaped muscle that originates from fascia along the median dorsal line of the back and inserts on the cranial aspect of the scapular spine. The thoracic part of the trapezius group is a triangular sheet of muscle located caudal to the cervical part of the trapezius. It originates from the fascia above the spinous processes of the thoracic vertebrae and inserts on the caudal aspect of the scapular spine. Separate these muscles from underlying muscles and free their cranial and caudal borders. The action of this muscle group is to adduct the scapula.
3. The latissimus dorsi muscle (M. latissimus dorsi) is the large muscle caudal to the trapezius group (see Figure 8.9). It originates from the spinous processes of the thoracic vertebrae and the lum-
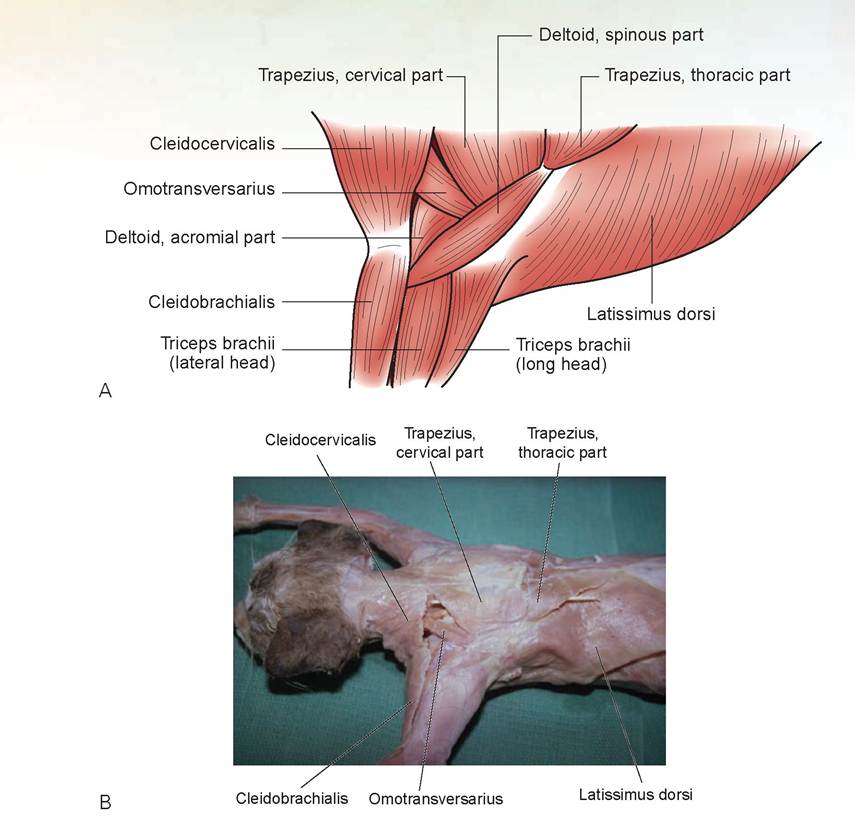
FIGURE 8.9: A. Superficial muscles of the shoulder and back. B. Superficial muscles of the shoulder and back in a cat.
bodorsal fascia. It courses Cranioventrally to insert on the proximal end of the humerus with the pectoralis profundus. Its action is to draw the trunk forward, depress the vertebral column, draw the limb against the trunk, and draw the limb caudally during flexion of the shoulder joint. Free the cranial and caudal borders of the latissimus dorsi. Part of the cranial border lies beneath the thoracic part of the trapezius.
4. The Omotransversarius muscle (M. omotransversarius) (in previous guides called the levator scapulae ventralis) in the cat is a strap-like band of muscle that originates from the atlas and the occipital area of the skull and passes caudally beneath the cleidocervicalis to insert on the acromion process of the scapula. Its action is to pull the scapula cranially (see Figure 8.9).
5. The deltoid muscle (M. deltoideus) consists of two parts: the acromial part (in previous guides the acromiodeltoid) and the spinous part (in previous guides the spinodeltoid). The spinous part of the deltoid is the most caudal portion. It originates along the caudal aspect of the spine of the scapula ventral to the insertion of the thoracic part of the trapezius. It runs almost parallel with the edge of the spine of the scapula and inserts on the proximal humerus. Separate and free the borders of this muscle. The acromial part of the deltoid originates from the acromion process of the scapula and inserts on the proximal end of the humerus. Free the edges of this muscle. The actions of the deltoids are to flex, extend, rotate, and abduct the humerus (Figures 8.9A and 8.10).

FIGURE 8.10: Deep muscles of the shoulder and superficial muscles of the upper front leg of a cat.
Part 4: Deep Muscles of the Shoulder and Back
1. To expose the deeper muscles of the shoulder and back, carefully bisect the cervical and thoracic parts of the trapezius muscles halfway between their origins and insertions (not at the midline of the back). Reflect the bisected muscles dorsally and ventrally.
2. The supraspinatus muscle (M. supraspinatus) fills the supraspinous fossa of the scapula cranial to the spine. The infraspinatus muscle (M. infraspinatus) fills the infraspinous fossa caudal to the scapula’s spine. Both muscles originate on the scapula and insert on the humerus (see Figure 8.10). The action of the supraspinatus extends the humerus, and that of the infraspinatus rotates it laterally.
3. The teres major muscle (M. teres major) originates on the dorsocaudal border of the scapula, caudal to the infraspinatus (see Figure 8.10). It inserts on the proximal end of the humerus with the latissimus dorsi. Separate the teres major from the infraspinatus. The action of this muscle is to extend and rotate the humerus.
4. Observe the dorsal rim of the scapula. A large muscle group originates from the spinous processes of the caudal cervical and cranial thoracic vertebrae. This is the rhomboideus group of muscles (M. rhomboideus), which contains three muscles (see Figure 8.10). The most caudal is the rhomboideus thoracic (M. rhomboideus thoracic) (in previous guides the rhomboideus major). It inserts on the dorsal caudal angle of the scapula.
Just cranial to this is the rhomboideus cervicis (M. rhomboideus cervicis) (in previous guides the rhomboideus minor). It inserts along the dorsal rim of the scapula. The division between these two muscles is somewhat obscure (difficult to see). As the rhomboideus thoracic inserts, it partially covers the dorsal aspect of the scapula. Follow the cranial edge of this insertion dorsally toward the spine, and you will find a natural separation in the fibers above the rim of the scapula, and thus the separation between the rhomboideus thoracic and the rhomboideus cervicis. The action of these two muscles draws the scapula dorsally and rotates it.
The rhomboideus capitis (M. rhomboideus capitis) is the most cranial muscle of this group. It is a narrow, thin, ribbon-like muscle that originates from the occipital bone and inserts on the cranial edges of the scapula just ventral to the dorsocranial angle. Its action is to draw the scapula cranially. Carefully dissect this muscle from the deeper muscles.
5. Deep to the rhomboideus capitis is a broad, flat muscle called the splenius muscle (M. splenius). It covers most of the dorsal and lateral surface of the neck. Its action is to turn the head.
6. Bisect the latissimus dorsi muscle at its center and reflect the halves dorsally and ventrally. This will allow you to see the deeper chest muscles. You will note a large, fan-shaped, serrated-appearing muscle called the serratus ventralis muscle (M. serratus ventralis). It originates from the ventral aspect of the ribs, passes medial to the scapula, and inserts on the medial dorsal border of the scapula (Figures 8.10, 8.11, and 8.12A). This muscle is also visible on the lateral surface of the body at its origin on the ribs. The action of this muscle is to pull the scapula forward and down.
7. The subscapularis muscle (M. subscapularis) fills the subscapular fossa of the scapula on its medial side. Thus, it originates on the medial scapula and inserts on the humerus. Its action is to rotate the scapula medially. Do not dissect this muscle.
Part 5: Muscles of the Front Leg
1. Clear away the superficial fat and fascia from the upper leg (also called the brachium).
2. The Tensor fasciae antebrachii muscle (M. Tensor fasciae antebrachii) is a thin, flat muscle that originates from the surface of the insertion of the latissimus dorsi, extends along the medial surface of the arm, and inserts on the olecranon process of the ulna. The long head of the triceps brachii lies deep and caudal to this muscle (Figure 8.13).
3. On the caudal aspect of the front leg is the triceps brachii group of muscles (M. triceps brachii) (see Figures 8.10, 8.11, and 8.12). The name triceps indicates the presence of three main muscles in this group, although the dog and cat have four when the small accessory head is considered. These encompass most of the caudal and lateral surfaces. The long head of the triceps is on the caudal surface and is the largest of the three muscles. It originates from the scapula caudal to the glenoid cavity and inserts on the olecranon process. The action of the triceps group of muscles is to extend the elbow joint. Free both borders of the long head.
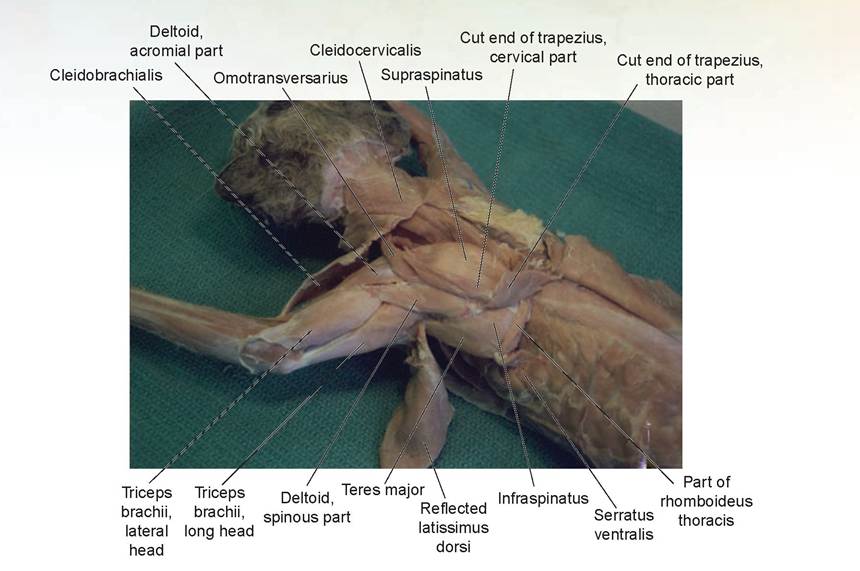
FIGURE 8.11: Deep muscles of the upper shoulder and back in a cat.
4. The lateral head is located just cranial to the long head on the lateral aspect of the leg. It originates from the proximal end of the humerus and inserts on the olecranon process. Free the cranial border first; then free the caudal border, making a linear incision in the fascial attachment at its distal insertion, and continue it for approximately 1 cm down the olecranon process. This will enable you to reflect this muscle cranially. You may choose to bisect the muscle to view the medial head of the triceps. However, some students choose not to do this and instead reflect the muscle cranially to view the medial head. On the medial side of the lateral head is the accessory head. Try to separate it along the cranial border; sometimes a distinct separation can be found.
5. The long, narrow medial head is located beneath the lateral head and can be viewed by reflecting the lateral head in a cranial direction. It is located just caudal to the humerus. It also originates from the proximal end of the humerus and inserts on the olecranon process.
6. The anconeus muscle (M. anconeus) is a thin, flat, triangular muscle that lies deep to the distal insertion of the lateral head of the triceps. It can be seen once the fascia above the lateral aspect of the olecranon process is opened and the insertion of the lateral head of the triceps is reflected cranially (see Figure 8.12). The anconeus originates on the lateral epicondylar area and the distal shaft of the humerus, and inserts on the olecranon process. Even though this is a small muscle, it is important because it must be incised to perform surgery on the anconeal process in a pathological condition known as ununited anconeal process (elbow dysplasia). Just view this muscle; do not attempt to free its edges as it tears easily.
7. The brachialis muscle (M. brachialis) is located on the lateral surface of the humerus, cranial to the lateral head of the triceps (see Figure 8.12). It originates from the humerus and inserts on the proximal end of the ulna. The action of the brachialis is to aid in flexion of the elbow joint.
8. The biceps brachii muscle (M. biceps brachii) is found on the craniomedial surface of the humerus. Because much of this muscle lies beneath the insertion of the pectorals, it is best viewed by elevating the insertions of the pectoralis transversus, pectoralis profundis, and pectoralis descendens muscles. The biceps brachii originates on the scapula and inserts on the radius. This muscle’s action is to aid in flexing the elbowjoint (see Figure 8.13B).
9. Deep beneath the pectoralis muscles is the coracobrachialis muscle (M. coracobrachialis). To locate this muscle, the pectoralis transversus and pectoantebrachialis must be elevated, and the lateral border of the pectoralis profundus must be separated completely from the fascia of the insertion
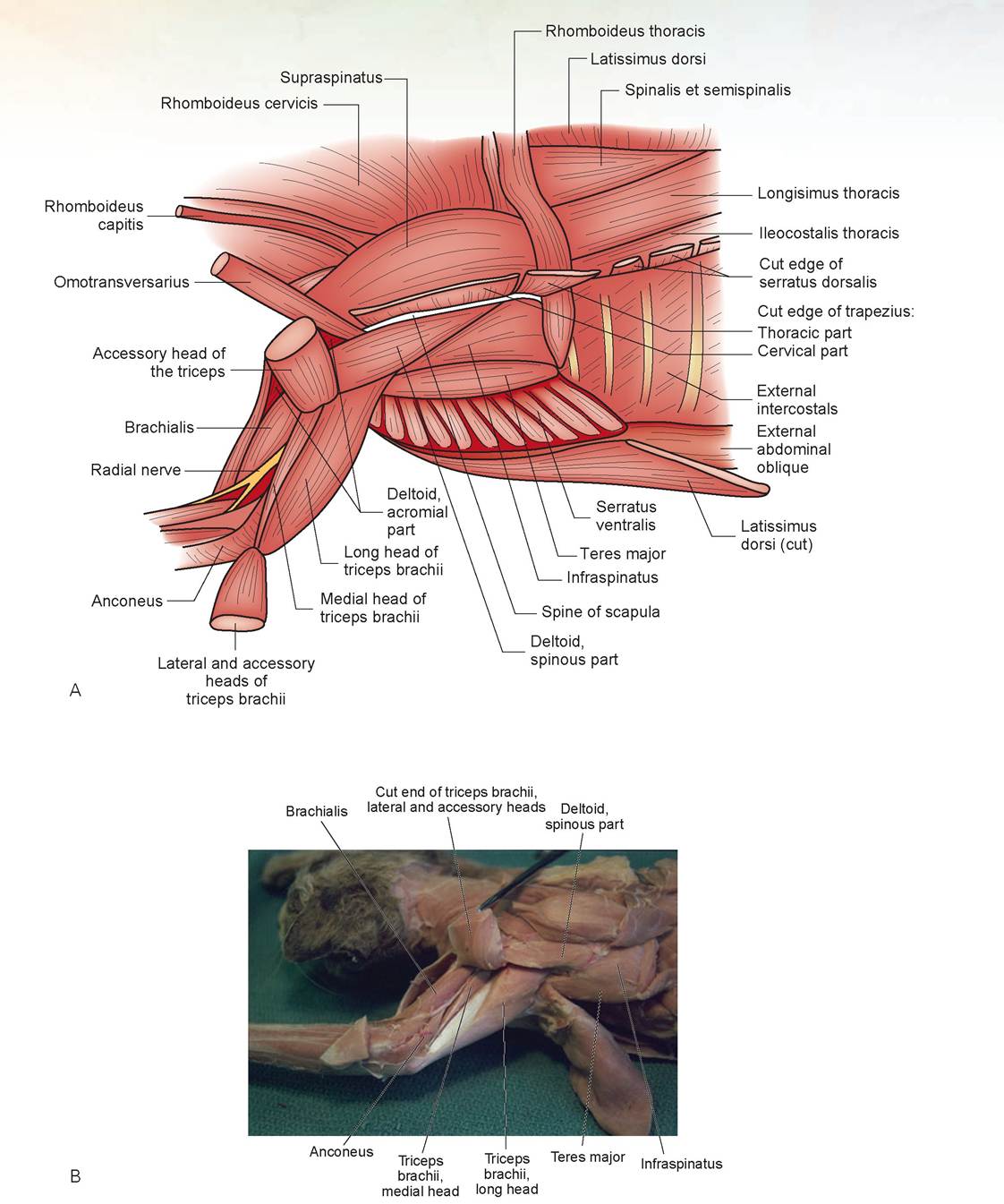
FIGURE 8.12: A. Lateral view of the deep muscles of the upper front leg. B. Lateral view of the deep muscles of the upper front leg of a cat.
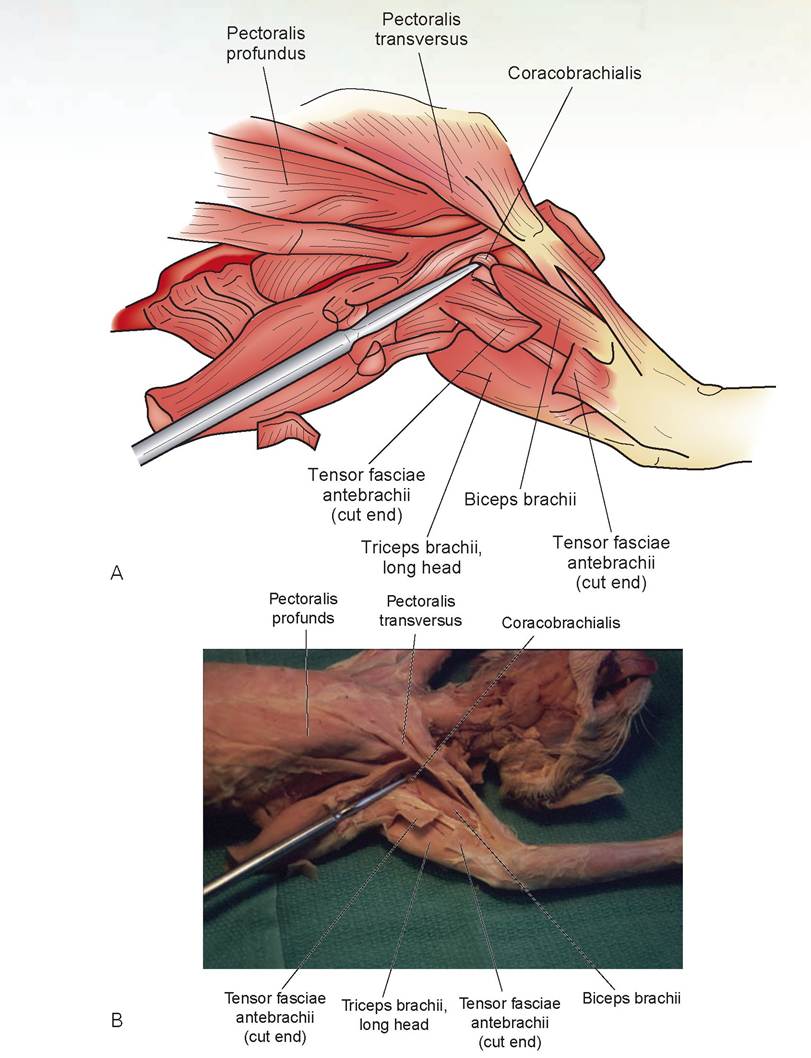
FIGURE 8.13: A. Medial view of the deep muscles of the front leg. B. Medial view of the deep muscles of the front leg of a cat.
of the latissimus dorsi and epitrochlearis. It should take only a few small snips with your scissors to make this separation. The coracobrachialis is found at the origin of the biceps brachii and is a short band of muscle approximately 4 to 6 mm wide. It runs at a 45° angle obliquely toward the body and away from the insertion of the biceps brachii. It originates from the coracoid process of the scapula and inserts on the proximal end of the humerus. Its action is to adduct the front leg.
The remaining steps (10-12) are optional.
10. Note the thick layer of fascia covering the foreleg muscles. Remove this fascia so that the muscles can be identified. Observe the tendons of these muscles at the carpus, and separate the superficial muscles of the foreleg. Do not bisect any of these muscles. Compare your dissection with Figures 8.14 and 8.15 and identify each of the labeled muscles. The cranial group of muscles, in general, extends and supinates. The caudal group of muscles are flexors and pronators.
11. On the cranial side, the most cranial muscle at the elbow joint is the brachioradialis muscle (M. brachioradialis). Proceeding caudally, you will encounter the extensor carpi radialis (M. extensor carpi radialis) longus and brevis, extensor digitorum communis (M. extensor digitorum communis), extensor digitorum lateralis (M. extensor digitorum lateralis), and the ulnaris lateralis muscle (M. ulnaris lateralis). Deep to the tendons of the previously mentioned muscles, running obliquely from caudodorsal to cranioventral, is the adductor pollicis longus muscle (M. adductor pollicis longus)
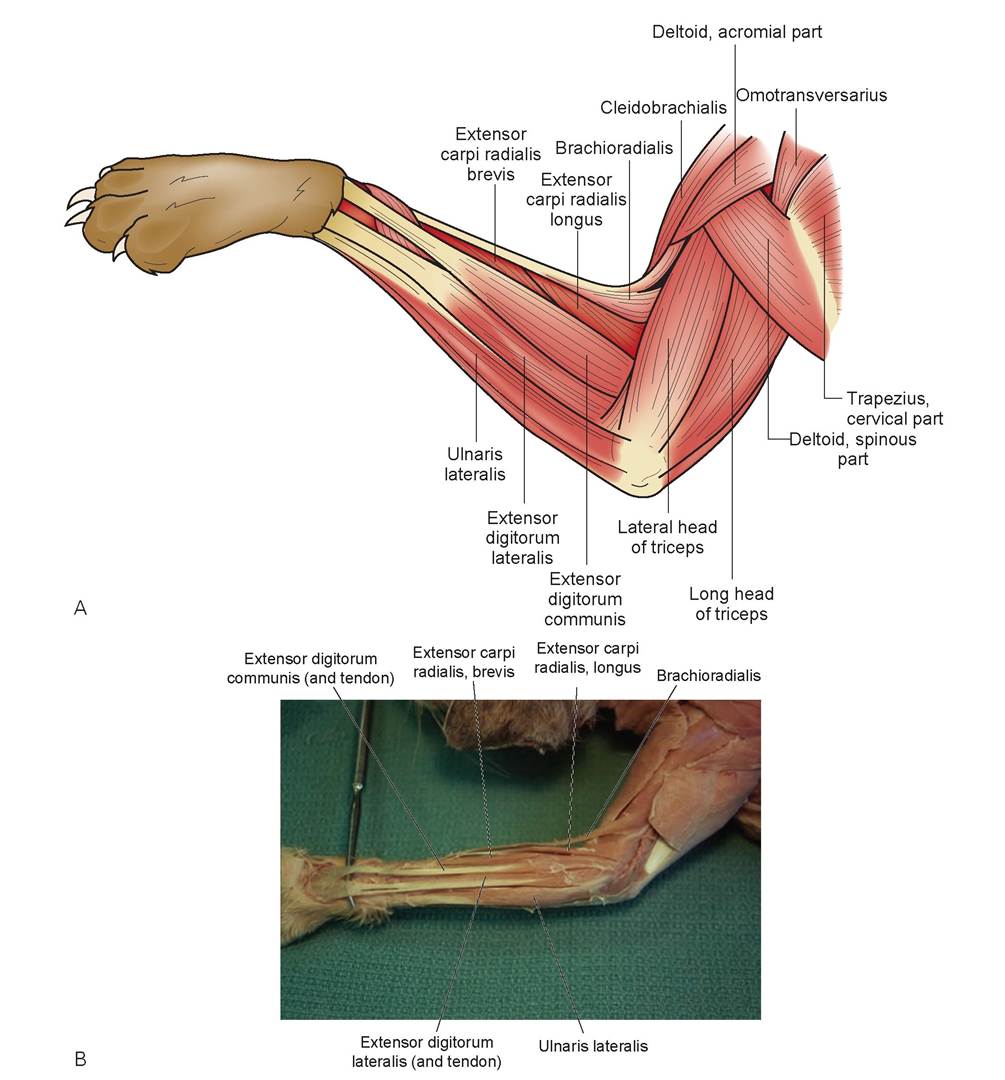
FIGURE 8.14: A. Craniolateral view of the muscles of the foreleg. B. Craniolateral view of the muscles of the foreleg of a cat.
(not shown in Figure 8.14). These muscles, as a group, are called the extensors and are innervated by the radial nerve.
12. On the caudal side is another muscle that angles across the proximal foreleg, the pronator teres (M. pronator teres). Just caudal to this muscle is the flexor carpi radialis muscle (M. flexor carpi radialis), followed caudally by the flexor digitorum superficialis (M. flexor digitorum superficialis) and the flexor carpi ulnaris (M. flexor carpi ulnaris). If these three superficial muscles are removed, the flexor digitorum profundus (M. flexor digitorum profundus) with its three heads can be viewed (not shown in Figure 8.15). The radial head appears most cranially, then the humeral head, followed by the ulnar head.
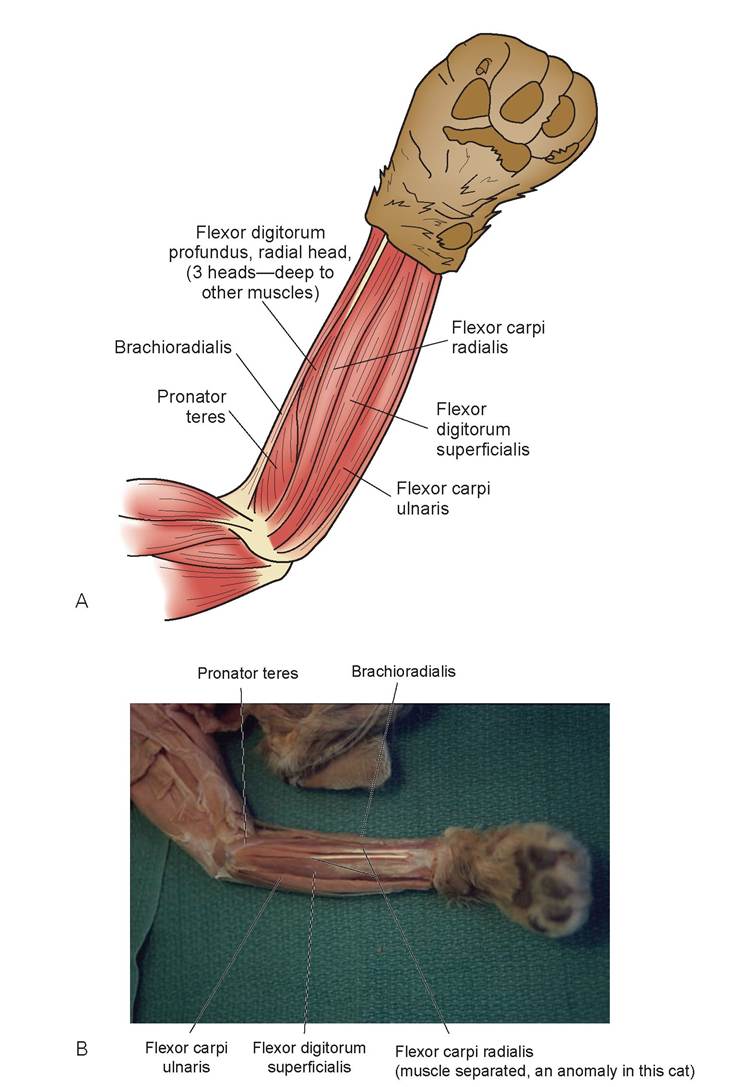
FIGURE 8.15: A. Medial view of the superficial muscles of the foreleg. B. Medial view of the superficial muscles of the foreleg of a cat.
Part 6: Abdominal Wall Muscles
1. Remove the fat and superficial fascia from the ventral and lateral surfaces of the left side of the trunk between the pectoralis profundus and the pelvic area. Note the Iumbodorsal fascia, the wide sheet of white-colored fascia covering the lumbar region of the back.
2. The lateral abdominal wall of the cat is composed of three layers of muscle. These abdominal muscles are very thin, each no greater than 1 mm in thickness; therefore, be extremely conservative in your dissection and cut through only one layer at a time.
3. The action of the lateral abdominal wall muscles is to compress the abdomen. This is important in forced expiration, defecation, micturition, and parturition. The muscles are also important in dorsal, ventral, and lateral flexion of the trunk.
4. The external abdominal oblique muscle (m. obliquus externus abdominis) forms the most superficial layer of the lateral abdominal muscles (Figure 8.16). It originates on the posterior ribs and the lumbodorsal fascia, beneath the caudal edge of the latissimus dorsi muscle, and inserts as fascia on the ventral midline. Make a cut in the middle of this muscle parallel to the muscles fibers and separate the opening you have formed. Once this muscle layer is isolated, bluntly dissect between this muscle and the internal oblique. Separate it and extend the opening ventrally to the ventral fascia. The top layer of this fascia is a broad sheet of connective tissue called the aponeurosis of the external oblique. Notice that the muscle fibers terminate about 1 inch before the linea alba (also called the white line; the mid-ventral line formed by the union of the aponeuroses of the lateral abdominal wall muscles). The aponeurosis is superficial to the rectus abdominis muscle.
5. The internal abdominal oblique muscle (M. obliquus internus abdominis) lies deep to the external oblique, with its fibers running in the opposite direction (ventrally and cranially). It originates on the lumbodorsal fascia, inserts with an aponeurosis on top of the transversus abdominus, and continues to the linea alba. Note where the muscle fibers terminate superficial to the tranversus abdominis before reaching the rectus abdominis muscle.
6. The muscle deep to the internal oblique is the transversus abdominis muscle (M. transversus abdominis). This may be viewed by making a second cut, in the same direction as the muscle fibers, through the internal oblique muscle. The transversus abdominis originates from the vertebral column, the lumbodorsal fascia, and the sacrum, and it inserts at the linea alba underneath the rectus abdominis muscle. Separate this muscle from the internal oblique and follow it as far ventrally as possible.
7. Carefully separate some of the fibers of the transversus abdominis. The shiny membrane visible beneath the muscle fibers is the parietal layer of the peritoneum, which should not be pierced.
8. The longitudinal band of muscle lying lateral and parallel to the linea alba on both sides is rectus abdominis muscle (M. rectus abdominis) (see Figure 8.16). To view this muscle, reflect the external oblique. The rectus abdominis originates from the cranial aspect of the pubis and inserts on the sternum and costal cartilages. Its action is to support the abdominal wall and ventrally flex the abdomen. Dissect only the lateral edge of this muscle from the underlying transversus abdominis for a short distance to enable you to see the direction of the muscle fibers.
9. In certain mammals, such as the pig, fat is deposited in the connective tissue layers between the muscles of the lateral abdominal wall such that fat and muscle alternate. This part of the pig is sold commercially as bacon. The small pieces of cartilage often found in bacon are pieces of costal cartilage from the lower ends of the ribs.
Part 7: Superficial Muscles of the Hind Legs
1. Remove the fat and superficial fascia from the dorsal surface of the back above the hind legs, around the groin region, and down the legs. Be careful during your dissection not to damage any muscles in the gluteal region, because the fascia adheres tightly to the gluteal muscles. Also, be careful not to remove any blood vessels or nerves from the inner thigh.
2. On the superficial craniomedial surface of the thigh (Figure 8.17) is the sartorius muscle (M. sartorius). It is a thin, band-like muscle, about 1 to 1.5 in. wide. Free both the cranial and caudal borders from the ilium to the tibia, and bisect this muscle at the middle. The action of this muscle is to adduct and rotate the thigh.
3. The gracilis muscle (M. gracilis) is the large (but thin), wide, flat muscle covering the caudomedial surface of the thigh, caudal to the sartorius. Free both borders of this muscle and bisect it in the middle. This muscle originates on the os coxae bone and inserts on the tibia and fascia of the knee area. Its action is to adduct the thigh.
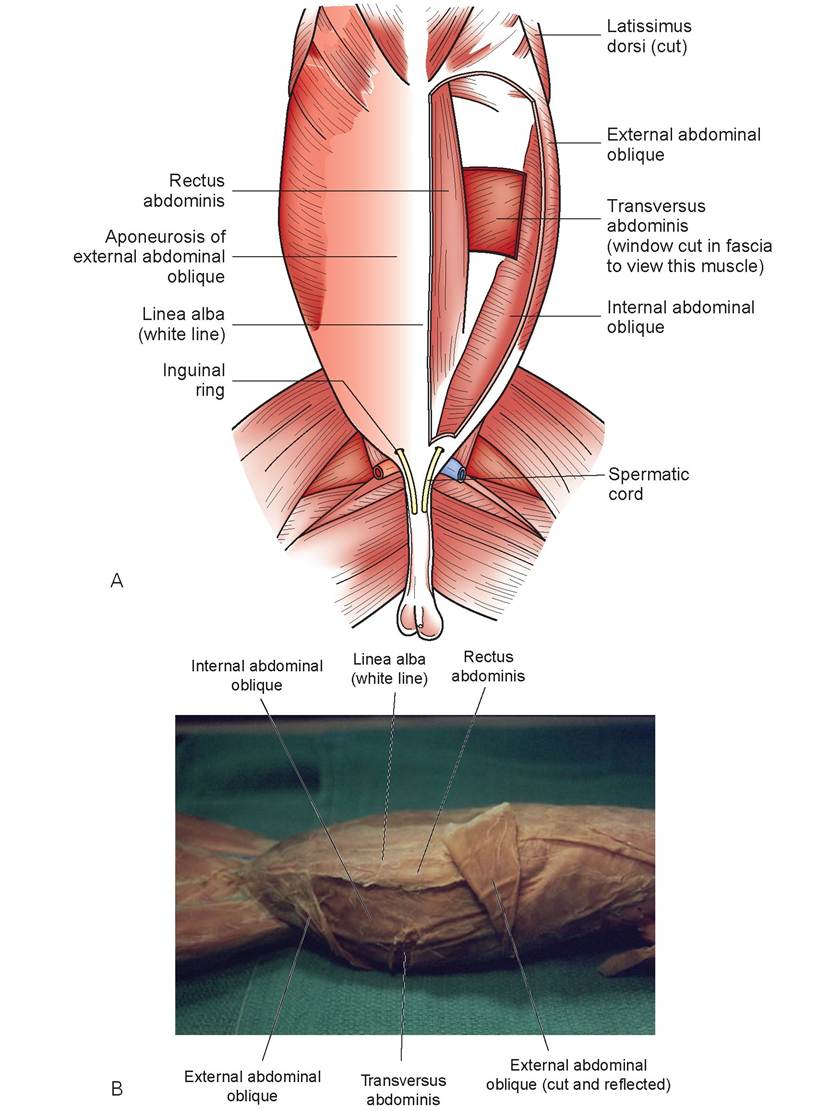
FIGURE 8.16: A. Muscles of the abdomen. B. Muscles of the abdomen of a cat.

4. Now turn the cat over so the lateral and dorsal areas of the rear leg are presented. Caudal to the sartorius on the lateral surface of the thigh is a tough, white sheet of fascia. This is the fascia lata (Figure 8.18). The fascia lata covers the biceps femoris, semitendinosus, and semimembranosus, and sends a lamina deep to the biceps. To free the lateral surface of the fascia from the underlying muscles, reflect the bisected sartorius muscle and pass your fingers caudally beneath the tough fascia. With your scissors or scalpel, separate the caudal border of fascia at the cranial border of the biceps femoris from the quadriceps femoris muscle. Bisect the fascia in the middle. When the proximal part of it is elevated, a triangular muscle, the tensor fasciae latae muscle
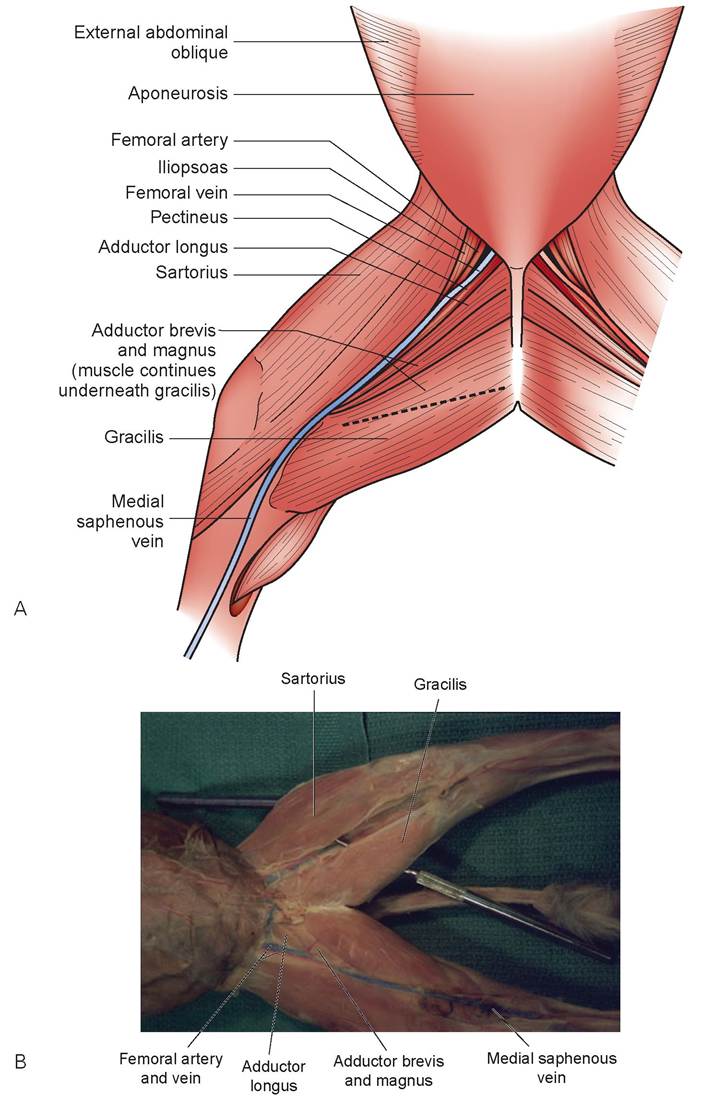
FIGURE 8.17: A. Ventral view of the superficial muscles of the upper hind leg. B. Ventral view of the superficial muscles of the upper hind leg of a cat.
(M. tensor fasciae latae), can be seen. The aponeurosis of this muscle is fused with the fascia lata. The tensor fasciae latae muscle originates from the ilium and inserts as the fascia lata. It acts as the tensor of the fascia lata and as an extensor of the lower leg. Free the caudal boundary between the tensor fasciae latae and the middle gluteal muscle.
5. The huge muscle caudal to the fascia lata, covering the entire caudolateral surface of the thigh, is the biceps femoris muscle (M. biceps femoris) (see Figure 8.18). This muscle forms the lateral wall of the popliteal fossa, which is located caudal to the knee joint. It originates on the ischium and inserts on the distal femur, patella, and fascia of the lower hind leg. Its action is to extend the stifle and the
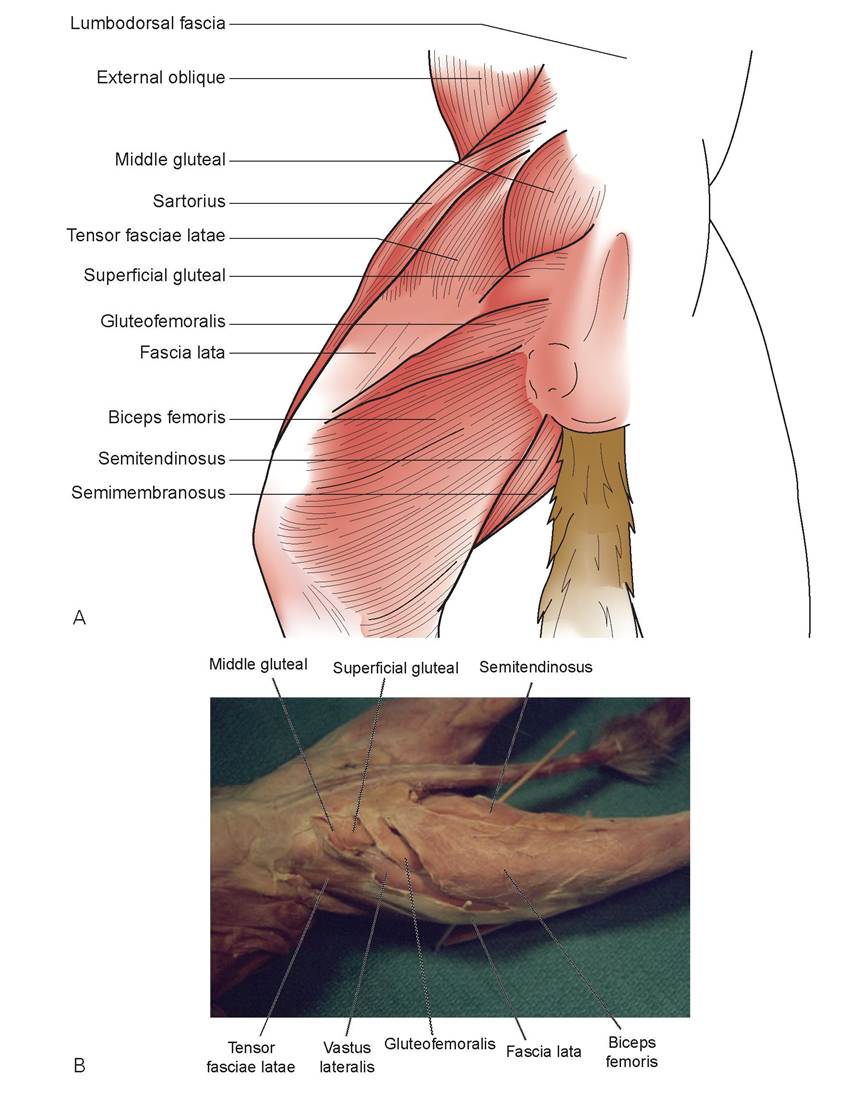
FIGURE 8.18: A. Dorsolateral view of the superficial muscles of the upper hind leg. B. Dorsolateral view of the superficial muscles of the upper hind leg of a cat.
hock when the leg is weight bearing, and it is also a propulsor and acts to abduct the thigh and flex the lower leg. Dissect the fat from the popliteal fossa and locate the superficial popliteal lymph node within (Figure 8.19C). Free both cranial and caudal borders of this muscle.
6. When freeing the cranial edge of the biceps femoris, begin near the knee joint and work upward, looking for a small, narrow muscle—the gluteofemoralis muscle (M. glutefemoralis) (previous name: caudo femoralis m.)—at the cranial edge (Figures 8.18 and 8.19). This muscle originates on the coccygeal vertebrae and inserts on the patella with a long, narrow tendon visible on the inner surface of the biceps femoris. Its action is to help adduct the thigh. It is not present in the dog, but is in the fowl and reptiles.
7. The superficial gluteal muscle (M. gluteus superficialis) is immediately cranial to the caudofemoralis (Figure 8.19A and B). Its fibers originate and extend laterally from the sacrum and coccygeal vertebrae and insert on the lateral aspect of the greater trochanter of the femur. Its action is to abduct the thigh.
8. The muscle that extends craniad and is located cranial to the superficial gluteal muscle is the middle gluteal muscle (M. gluteus medius). It originates on the lateral ilium and the sacral and coccygeal vertebrae, and it inserts on the greater trochanter of the femur, just craniomedial to the insertion of the superficial gluteal. Its action is also to abduct the thigh. The deep gluteal muscle is located beneath the middle gluteal and also inserts on the greater trochanter. In the Brown Approach to surgery of the hip joint, these tendons of insertion must be cut, and the muscles reflected, to perform surgery on this joint.
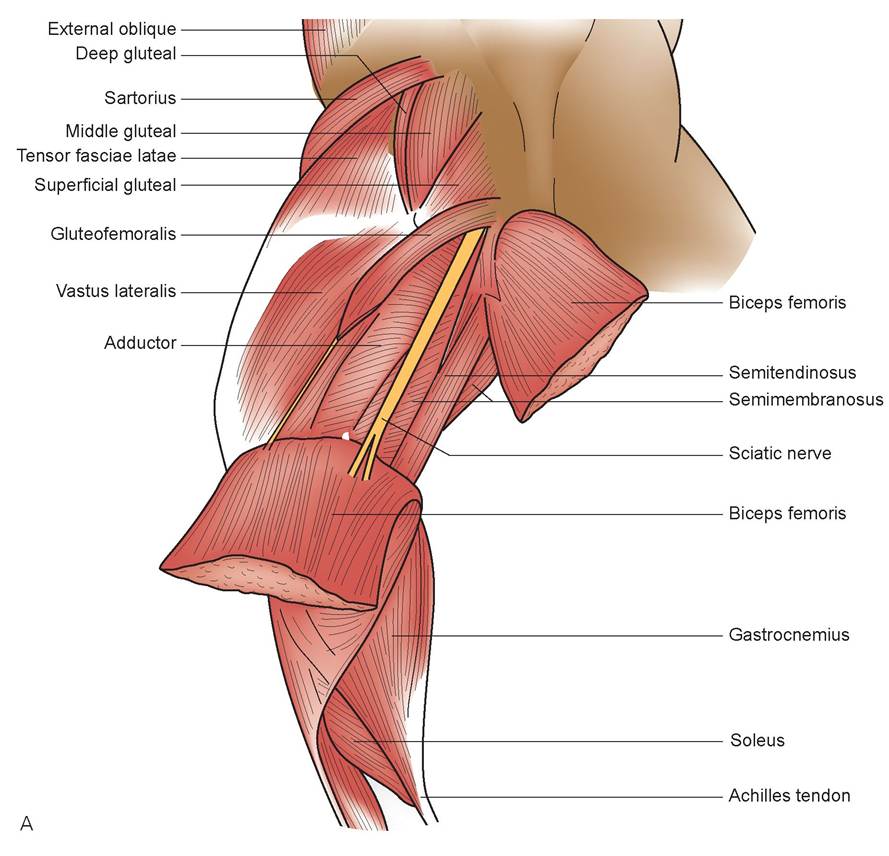
FIGURE 8.19: A. Dorsolateral view of the deep muscles of the upper hind leg.
Continued
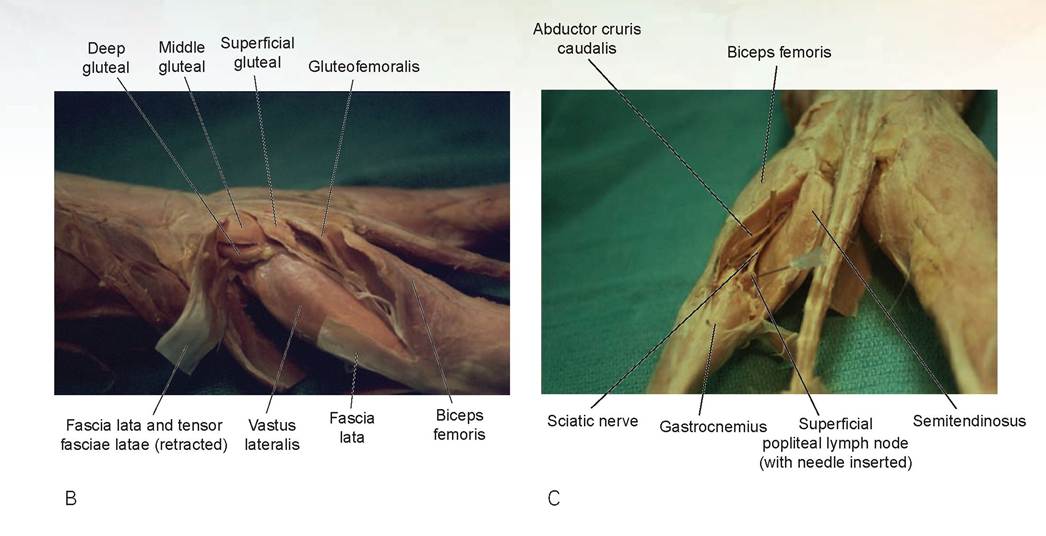
FIGURE 8.19, cont'd: B. Dorsolateral view of the deep muscles of the upper hind leg of a cat. C. Caudal view of the deep muscles of the upper hind leg of a cat. Needle is in the popliteal lymph node.
Part 8: Deeper Muscles of the Thigh
1. On the lateral side of the cat’s thigh, the caudal borders of the biceps femoris should be free. Gently lift up the biceps femoris, freeing it from the sciatic nerve and the abductor cruris caudalis muscle lying beneath. Carefully remove the fat in the popliteal fossa so the medial aspect of the biceps femoris can be viewed. Be careful not to bisect the sciatic nerve or this thin muscle (see Figure 8.19A and C).
2. The abductor cruris caudalis muscle is an extremely thin, long muscle lying beneath and attached to the biceps femoris and running parallel to the sciatic nerve. This muscle originates from the second caudal vertebra and inserts on the aponeurosis of the biceps femoris. Its action, similar to that of the biceps femoris muscle, is to abduct the thigh. It is easy to cut accidentally.
3. Turn the cat over so the medial aspect of the thigh is visible. Deep to the gracilis, four muscles are now visible. The most caudal is the semitendinosus muscle (M. semitendinosus) (Figure 8.20). It is a thick, strap-like muscle that originates from the ischial tuberosity and inserts on the proximal tibia. It forms part of the caudomedial border of the popliteal fossa. Its action is to flex the leg. Free both borders of this muscle.
4. Just cranial and medial to the semitendinosus is the semimembranosus muscle (M. semimembranosus). This originates on the ischium and inserts on the femur. Its action is similar to that of the biceps femoris and semitendinosus muscles to adduct the thigh.
5. Between the pectineus muscle cranially and the semimembranosus muscle caudally are three adductor muscles: a thin in the cat muscles adductor longus (M. adductor longus) cranially, followed by the small adductor brevis (M. adductor brevis) and the large adductor magnus (M. adductor magnus). All three adductor muscles originate from the pubis and ischium, and insert along most of the length of the femur. Their collective action is to adduct the thigh (see Figure 8.20A and B). Be careful not to separate the adductor magnus in the middle of the muscle belly; there is a slight fascial separation that can be mistaken for the caudal border of the adductor brevis.
6. Cranial to the adductor longus muscle is the pectineus muscle (M. pectineus). This is a tiny, thin muscle located below the femoral artery and vein. The pectineus originates on the pubis and inserts on the femur. Its action is to adduct the limb, flex the stifle, and extend the hip and hock joints (see Figure 8.20). Just proximal and dorsal to the pectineus is the iliopsoas muscle (M. iliopsoas), a
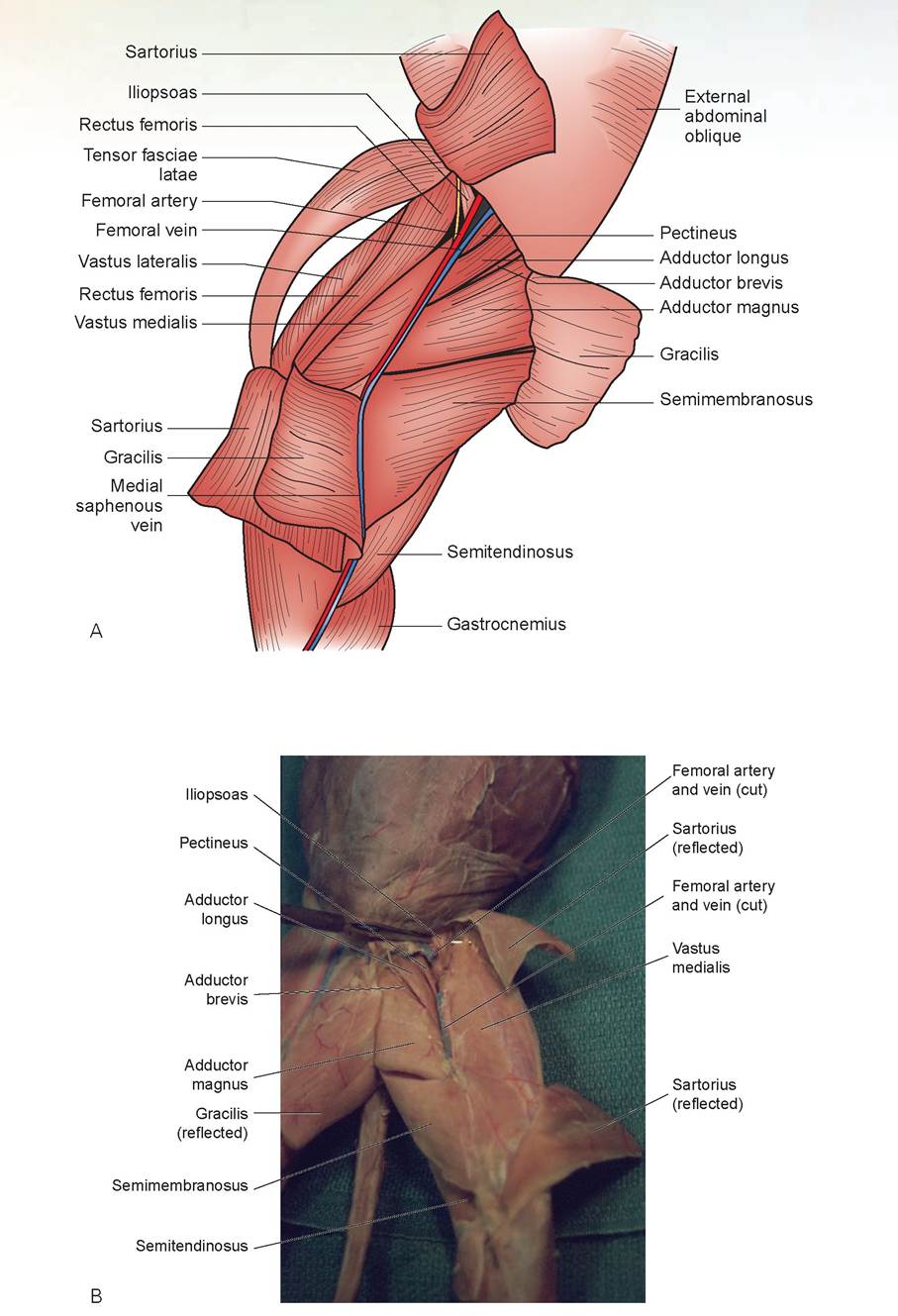
FIGURE 8.20: A. Medial view of the deep muscles of the upper hind leg. B. Medial view of the deep muscles of the upper hind leg in the cat.
FIGURE 8.21: The quadriceps femoris group of muscles in a cat.
compound muscle originating from the lumbar vertebrae and ilium and inserting on the femur. The iliopsoas muscle consists of the iliacus and psoas major muscles. Its action is to rotate and flex the thigh. Only a small, terminal portion of the iliopsoas is visible. It can be seen cranial to the femoral artery and veins. Its fibers run at nearly right angles to the blood vessels.
7. To see the quadriceps femoris muscle (M. quadriceps femoris), the sartorius and fascia lata must be bisected (this should already be done). Reflect the sartorius and the tensor fasciae latae muscle. The large muscle now exposed on the craniolateral surface of the thigh is the vastus lateralis (Figure 8.21). Craniomedial to the vastus lateralis is a narrow muscle, the rectus femoris, that originates on the ilium and inserts as part of the quadriceps femoris on the patella. Remove approximately 1 cm from the center of this muscle to view the deeper muscle. The vastus medialis muscle is located on the medial surface of the thigh, just caudomedial to the rectus femoris.
The deep muscle beneath the rectus femoris is the vastus intermedius muscle. Using blunt dissection, separate the internal margins of the vastus lateralis and vastus medialis from the vastus intermedius. The three vastus muscles originate from the upper femur and converge to encompass and insert on the patella (a sesamoid bone). The quadriceps muscle’s action is to extend the stifle joint by means of the patellar ligament attached to the tibial tuberosity.
Part 9: Posterior Leg Muscles
1. The gastrocnemius muscle (M. gastrocnemius) is the large calf muscle (Figure 8.22) visible on the caudal aspect of the tibia, distal to the stifle joint. There are two bellies in this muscle, one medial and the other lateral. The gastrocnemius originates primarily on the distal femur and inserts as the tendon of Achilles (Achilles tendon) on the calcaneal tuber (tuber calcanei) of the fibular tarsal bone (calcaneus). This muscle’s action is to extend the hock joint and flex the digits of the foot.
2. Ventral to the gastrocnemius, on the lateral aspect of the calf, is the soleus muscle (M. soleus), the third component of the triceps surae. Originating from the fibula, it joins the lateral head of the gastrocnemius and contracts simultaneously with this muscle. Deep to the gastrocnemius, and originating from the distal femur, the superficial digital flexor muscle becomes superficial surrounding the tendon of the triceps surae. It inserts temporarily on the calcaneal tuber, then continues distally dividing its tendon for each digit, and then inserts on the second phalanges of all the digits. It acts as one of the flexors of the digits. Its tendon, together with the tendons of triceps surae muscle and the calcaneal tendons of some muscles of the thigh, are known as the tendon of Achilles (Achilles tendon). It will not be dissected.
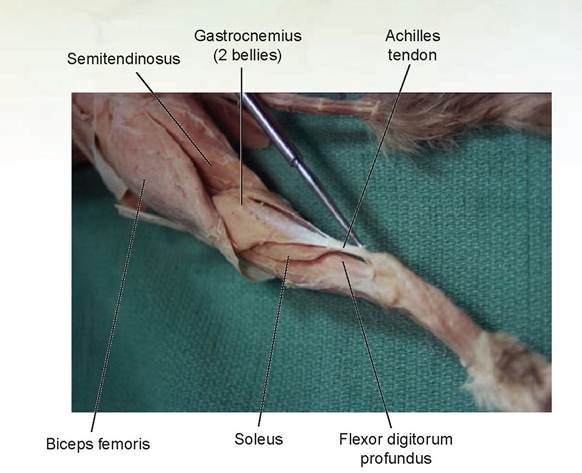
FIGURE 8.22: Caudal view of the superficial muscles of the lower hind leg of a cat.
Part 10: Deep Muscles of the Hind Leg
This is an optional dissection.
1. On the lateral side of the hind leg, locate the following muscles, starting with the most cranial muscle and proceeding caudally: Tibialis cranialis muscle (M. tibialis cranialis), extensor digitorum longus (M. extensor digitorum longus), fibularis (peroneus) longus (M. fibularis [peroneus] longus), extensor digitorum lateralis (M. extensor digitorum lateralis), and fibularis (peroneus) brevis (M. fibularis [peroneus] brevis). Consult Figure 8.23 for help.
2. On the medial side of the lower hind leg, deep to the superficial digital flexor, is the flexor digitorum profundus (M. flexor digitorum profundus) (see Figure 8.22).
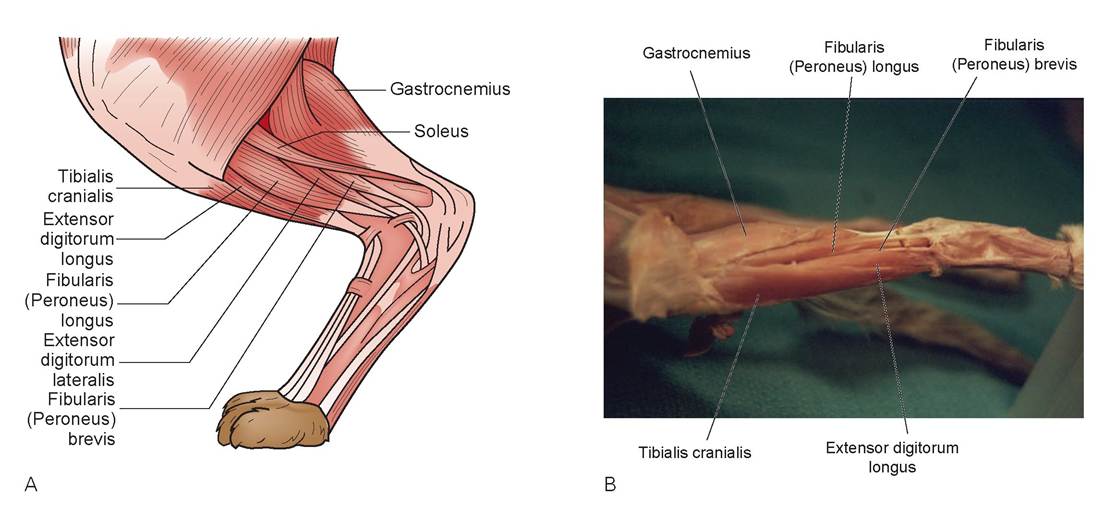
FIGURE 8.23: A. Craniolateral view of the muscles of the lower hind leg. B. Craniolateral view of the muscles of the lower hind leg of a cat.
Part 11: Deep Back Muscles
1. To view the intercostal muscles (the muscles between the ribs), reflect the caudal border of the origin of the serratus ventralis muscle and expose the ribs.
2. The fibers of the external intercostals (Figure 8.24) course in a craniodorsal to caudoventral direction between the ribs. The action of the external intercostals is to lift the ribs in inspiration, thereby expanding the thoracic cavity.
3. Remove approximately 1 cm of the external intercostal muscle between two ribs to expose the internal intercostals, the fibers of which run at right angles to the external intercostals. These muscles act to depress the ribs during active expiration.
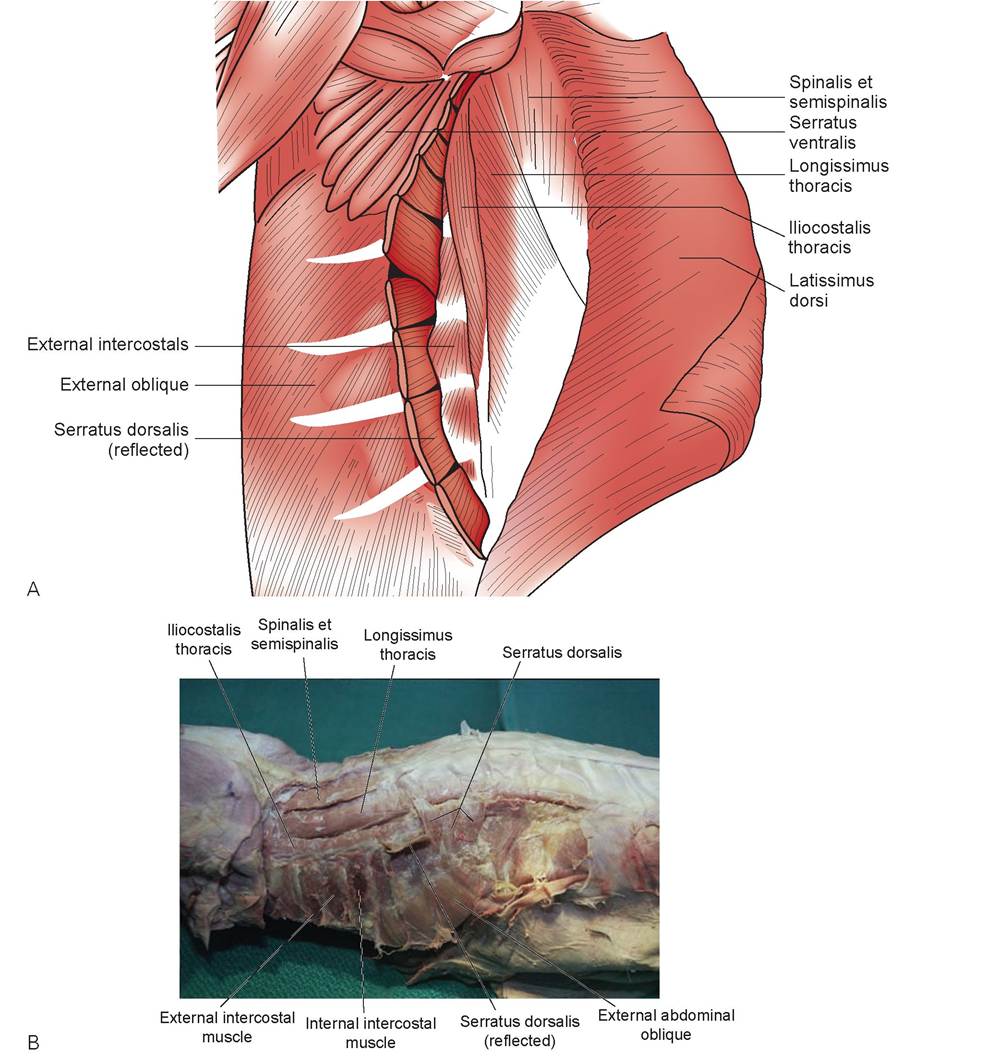
FIGURE 8.24: A. Deep muscles of the back and ribs. B. Deep muscles of the back and ribs in a cat.
4. Dissection of the deep back muscles requires that you reflect the latissimus dorsi toward its origin. Bisect this muscle now if you have not already done so. The serratus dorsalis muscle (M. serratus dorsalis) (see Figure 8.24), which is a series of muscle bundles that appear serrated, originates from a middorsal aponeurosis and inserts ventrally on the ribs. Reflect this muscle ventrally by cutting through the aponeurosis and exposing the iliocostalis part of the erector spinae muscle system.
5. The epaxial spinal musculature (dorsal trunk muscles) (see Figure 8.24) is a system of muscles divided into three parts: the m. iliocostalis system, m. longissimus system, and the m. transversospinalis system. We will dissect the most visible representative muscle from each system. It may be necessary to remove the dorsal fascia to visualize these muscles. The most ventral, the iliocostalis thoracis muscle (M. iliocostalis thoracis), lies beneath the serratus dorsalis and inserts on the ribs. The middle muscle is the longissimus thoracis muscle (M. longissimus thoracis). It occupies the space between the spinous and transverse processes of the caudal thoracic and lumbar vertebrae, and thus runs the length of the back. The dorsal muscle of the transversospinalis system we will dissect is called the spinalis et semispinalis muscle (M. spinalis et semispinalis). It is found next to the spinous processes of the thoracic vertebrae. The action of this group of muscles is to extend the spine and neck. Each system has more muscles cranial and/or caudal to the three dissected muscles, such as the iliocostalis lumborum and longissimus lumborum.
- Clinical Significance
The clinical significance of this chapter is illustrated in the following exercise.
EXERCISE 8.3 MUSCLE PHYSIOLOGY AND PATHOLOGY
The classic experiment to illustrate muscle physiology is to sacrifice a frog, remove its gastrocnemius muscle, attach it to a myograph, and stimulate it electrically to show summation and tetany. Please read about these experiments in your textbook; we will not do them.
Instead, we will demonstrate the importance of an enzyme found within muscle. Creatinine kinase (CK) catalyzes one of the most important reactions in body chemistry. The concentration of adenosine triphosphate (ATP) in skeletal muscle is relatively low; it supplies only the energy needed to maintain contraction for a brief period of time. Muscles continue to contract after the initial supply of ATP has been used, leaving adenosine diphosphate (ADP). The ADP is phosphorylated again from another source, creatinine phosphate (CP). About five time more CP than ATP is stored in the sarcoplasm. When ATP is used to supply energy for muscular contraction, the ADP produced is transphosphorylated by the following equation:
This reaction replenishes the ATP almost as fast as it is being used. Therefore, the ATP level changes little until the concentration of CP gets low.
Horses are susceptible to a condition known as exertional rhabdomyolysis. Rhabdomyo- refers to skeletal muscle, and lysis means to rupture. In this condition, muscle damage occurs because of the breakdown of skeletal muscle cells. This is actually one of a group of disease conditions that share common symptoms and causes; these are tying-up syndrome, azoturia, Monday morning disease, and exertion-associated myositis. These conditions most often occur in heavily muscled horses that are working or in training and/or have been rested for one or more days, but were kept on full feed during that period. When returned to exercise, these horses may develop a myopathy.
The resulting pathology is myonecrosis, and the severity of the disease is directly related to the extent of the necrosis. When a muscle cell breaks down, it liberates myoglobin and CK, among other chemicals, into the bloodstream. When a sufficient amount of myoglobin has been released, urine will appear coffee-colored because of its presence.
Procedure
1. Three samples of horse serum will be provided: Horse A, normal horse, minimal activity; Horse B, normal horse, exercised vigorously or given an intramuscular injection; Horse C, horse showing much pain, sweating, reluctance to move.
2. Using your blood chemistry machine, measure the CK from each horse.
Horse A =_____________________________
Horse B =_____________________________
Horse C =_____________________________
Questions
1. Was CK elevated in Horse B; if so, why?
2. Given that CK levels cannot determine the extent of muscle damage (despite the fact that it is organ-specific), why were CK levels elevated in Horse C?
Discussion
CK levels can rise slighdy from minor muscular injuries because of the release of CK from the cells. Damage can be minor due to such events as receiving an intramuscular injection, persistent recumbency, bruising, a laceration, or hypothermia. In a situation in which there is considerable muscle damage, CK levels will elevate dramatically, but diagnosing exactly what amount of muscle damage has occurred is not possible based on CK levels alone. The presence of myoglobin in the urine is a better indicator of injury severity than a CK level by itself.

“—y' oc, I think Lucas has tetanus,” Ann Coles told me over the phone.
) “Why do you think that?” I asked. Dogs so rarely get tetanus that we don't k-? ' vaccinate for it.
“Well, isn't tetanus lockjaw?” she asked. “He can't open his mouth.”
I assured her it probably wasn't really tetanus, but there were some other things it could be. The first thing a veterinarian must do when an animal can't move a body part is to determine whether it is reluctance or a true inability. The former is usually due to pain, and the latter is often a neurological problem. In Lucas's case, the differential diagnosis was a broken jaw, a tooth problem, a retrobulbar abscess (behind the eye), eosinophilic myositis, and atrophic myositis. The latter two diseases are now combined into a syndrome known as masticatory muscle myositis (MMM).
Ann brought Lucas to the hospital that afternoon. She was very worried; I could tell by the look on her face and the strain in her voice.
Lucas's jaw was really painful; just attempting to open his mouth caused him to cry out loudly. This caused Ann even more distress.
“Ann, the only way I'm going to figure out what's going on is by anesthetizing and administering an analgesic to Lucas. I'll open his mouth while he's out and not feeling any pain.”
It was senseless to continue my examination of the oral cavity. There was nothing I was going to learn until I got the mouth open. We did check the rest of the dog's systems for abnormalities, but there were none. As I studied Lucas's face, it seemed as though his facial muscles were a little swollen, but this was mostly a subjective impression and was difficult to say with certainty.
After Lucas was anesthetized, I was able to open his mouth. Because there was no muscle atrophy and the jaw was not locked shut, he did not have the atrophic form of this disease. The teeth looked fine, as did both mandibles. There did not appear to be an abscess behind either eye, and that left only an inflammatory or autoimmune condition on my list of diseases to rule out. I made an incision, took a small piece of muscle tissue from the masseter muscle, and sent it to the lab. We also ran blood chemistries and found the CK level mildly elevated. Eosinophils were normal, but this wasn't an unexpected finding. The lab confirmed the diagnosis of MMM.
Because this is an immune-mediated disease, immunosuppressive doses of corticosteroids were indicated, and the dog responded nicely. In talking to Ann I soon realized that her fear of giving her dog cortisone would hamper its needed therapy. I tried to convince her that Lucas would need to stay on the cortisone for six months, even though he would appear to be doing well and be back to normal. Just to be safe, I decided to educate her into giving treatment. I found some good articles on the disease, complete with photos from my veterinary journals, copied them, and gave them to her. The photos of both the atrophic and chronic forms of the disease were very graphic. I don't think the dog missed a pill the entire six months he was on the medication.
Summary
Most of this chapter has consisted of a detailed dissection of the muscular anatomy of the cat. We started at the chest, moved to the neck, upper back, front leg, abdomen, hind leg, and then to the deep muscles of the back and ribs. We also studied the histology of the three types of muscle tissue and discussed muscle physiology. The muscles of other animals are similar to that of the cat, so it serves as a good basis for other domestic animals.
REVIEW QUESTIONS
1. Name the three types of muscles, and indicate whether they are striated
or non-striated, and voluntary or involuntary.
2. What are fascicles?
3. Describe the locations of the epimysium, perimysium, and endomysium.
4. Fill in the blank: The nuclei of the muscle cell are located in the
position.
5. What is the difference between myofibrils and myofilaments?
6. What are the two contractile proteins of muscle?
7. Define sarcomere.
8. Which of the “bands” does not change in size when a muscle cell contracts, and which “bands” shorten?
9. What is the sarcoplasmic reticulum?
10. Cells of cardiac muscle interconnect at junctions known as what?
11. True or False: Cardiac muscle cells do not branch.
12. True or False: Actin and myosin are present only in skeletal muscle.
13. Define origin, insertion, and action of muscle.
14. What is the function of creatinine kinase?
15. Under what circumstances might a veterinarian measure CK levels, and what do elevated CK levels mean?