The Respiratory System
Thomas Colville
OUTLINE
INTRODUCTION, 362
STRUCTURE, 363
Upper Respiratory Tract, 363
Nose, 363
Pharynx, 365
Larynx, 365
Trachea, 367
Lower Respiratory Tract, 368
Bronchial Tree, 368
Alveoli, 369
Lungs, 369
Thorax, 371
FUNCTION, 372
Negative Intrathoracic Pressure, 372
Inspiration, 373
Expiration, 374
Respiratory Volumes, 374
Exchange of Gases in Alveoli, 374
Partial Pressures of Gases, 375
Control of Breathing, 375
Mechanical Control, 376
Chemical Control, 376
LEARNING OBJECTIVES
When you have completed this chapter you will be able to:
• Differentiate between internal and external respiration.
• List the secondary functions of the respiratory system.
• List the components of the upper respiratory tract and describe their structure and functions.
• List the components of the lower respiratory tract and describe their structure and functions.
Describe the events that occur during inspiration and expiration.
List the muscles involved in inspiration and expiration. Define the terms tidal volume, minute volume, and residual volume.
Describe the processes of oxygen and carbon dioxide exchange between the alveoli and the blood.
VOCABULARY FUNDAMENTALS
Alveolar duct ahl-ve-o-lahr duhckt
Alveolar sac ahl-ve-o-lahr sahck
Alveolus ahl-ve-o-luhs
Arytenoid cartilage eor-eh-tih-noyd kahr-tih-lihj
Bifurcation of the trachea bι-for-ka-shuhn of the tra-ke-ah
Breathing bre-thihng
Bronchial tree brohn-ke-ahl tre
Bronchiole brohn-ke-ol
Bronchitis brohn-kιt-ihs
Bronchoconstriction brohn-ko-kuhn-strihck-shuhn
Bronchus brohn-kuhs
Chemical control system kehm-ih-kuhl kohn-trol sihs-tehm
Congenital kohn-jehn-ih-tahl
Cough kawf
Cricoid cartilage krι-koyd kahr-tih-lihj
Diaphragm dι-ah-frahm
Endotracheal intubation ehn-do-tra-ke-ahl
ihn -too-ba-shuhn
Endotracheal (ET) tube ehn-do-tra-ke-ahl toob
Epiglottis ehp-ih-gloht-ihs
Expiration ehcks-puh-ra-shuhn
External respiration ehcks-tar-nahl rehs-puh-ra-shuhn
False vocal cord fahls vo-kahl kohrd
Glottis gloh-tihs
Hiccup hihck-uhp
Hilus hι-luhs
Inspiration ihn-spuh-ra-shuhn
Intercostal space ihn-tor-kohst-ahl spas
Internal respiration ihn-tar-nahl rehs-puh-ra-shuhn Laryngeal hemiplegia lahr-ehn-je-ahl hehm-ih-ple-je-ah Laryngoscope lah-rihn-jeh-skop
Laryngospasm lah-rihn-go-spahzm
Larynx lear-ihngks
Lateral ventricle laht-or-ahl vehn-trihck-ehl
Lobe lob
Lower respiratory tract lδ-or rehs-por-uh-tohr-e trahkt
Mechanical control system meh-kahn-ih-kahl kohn-trδl sihs-tehm
Mediastinum me-de-ah-stin-uhm
Minute volume mihn-iht vohl-um
Nares near-res
Nasal meatus naz-ahl me-at-uhs
Nasal passage naz-ahl pahs-ihj
Nasal septum naz-ahl sehp-tuhm
Olfactory sense ohl-fahck-tuh-re sehnz
Paranasal sinus peor-ah-na-sahl si-nuhs
Partial pressure pahr-shahl prehsh-or
pH pe-H
Pharynx fear-ihnks
Phonation fo-na-shuhn
Pleura ploor-ah
Pneumonia nu-mδn-yah
Pneumothorax nu-mo-thδr-ahx
Pulmonary puhl-muh-near-e
Residual volume rih-zihj-yoo-ahl vohl-um
Respiration rehs-puh-ra-shuhn
Respiratory center rehs-por-uh-tohr-e sehn-tor
Roaring rohr-ihng
Sigh si
Sinus si-nuhs
Sinusitis si-nuhs-i-tihs
Sneeze snez
Surfactant sor-fahck-tahnt
Thoracic cavity thohr-ah-sihck kahv-ih-te
Thorax thohr-ahx
Thyroid cartilage thi-royd kahr-tih-lihj
Tidal volume ti-dahl vohl-um
Trachea tra-ke-uh
Turbinate tar-buh-nat
Upper respiratory tract uhp-or rehs-por-uh-
tohr-e trahkt
Ventilation vehn-tih-la-shuhn
Vestibular fold vehs-tihb-yoo-lahr fold
Vocal cord vδ-kahl kohrd
Vocal fold vδ-kahl fold
Yawn yahn
INTRODUCTION
What do you think of when you read the term respiration? Do you imagine the process of breathing — drawing air into the lungs and blowing it back out? That is certainly an important part of respiration, but it is only one part of the whole, complex process.
In simplest terms respiration is the process of bringing oxygen (O2) from the outside air in to all of the body's cells, and carrying carbon dioxide (CO2) out in the opposite direction. The body's cells need a constant supply of oxygen to burn nutrients to produce energy. Carbon dioxide is a waste product of these energy-producing reactions and must be eliminated. In a simple, single-celled animal, these gases are exchanged between the interior of the cell and the outside environment directly through the cell membrane by simple diffusion (movement of molecules from an area of high concentration to an area of lower concentration). In a complex animal such as a horse or dog, most of the body's cells are located too far from the outside world for that simple system to work. Regardless, oxygen somehow has to reach all of the body's cells, and carbon dioxide has to be transported away from them. These vital processes are carried out by the respiratory system working together with the cardiovascular system.Two steps are needed for respiration to take place in an animal's body—external respiration and internal respiration. External respiration occurs in the lungs. It is the exchange of oxygen and carbon dioxide between the air inhaled into the lungs and the blood flowing through the pulmonary (lung) capillaries. Internal respiration, on the other hand, occurs all over the body. It is the exchange of oxygen and carbon dioxide between the blood in the capillaries all over the body (the systemic capillaries), and all of the cells and tissues of the body.
Internal respiration is the real “business end” of respiration. It is the means by which the body's cells receive the oxygen they need and get rid of the waste carbon dioxide they produce. Without external respiration, however, there would be no oxygen in the blood for the cells to absorb, and no way for the cells to get rid of their carbon dioxide.
In this chapter, we concentrate on the organs and structures that contribute to external respiration.
These are parts of what we call the respiratory system—the lungs and the complex system of tubes that connect them with the outside world. Box 15-1 lists the main components of the respiratory system in order, from outside in.In addition to its primary function of swapping oxygen for carbon dioxide, the respiratory system has some
BOX 15-1
Main Structures of the Respiratory System
In order, from outside in, the main structures of the respiratory system are as follows:
Upper Respiratory Tract
• Nostrils
• Nasal passages
• Pharynx
• Larynx
• Trachea
Lower Respiratory Tract
• Bronchi
• Bronchioles
• Alveolar ducts
• Alveoli secondary functions that are also important to an animal's well-being. These include voice production, body temperature regulation, acid-base balance regulation, and the sense of smell.
Voice production is also called phonation. The process usually begins in the larynx, or voice box, as it is commonly called. Two fibrous connective tissue bands called the vocal cords (also known as the vocal folds) stretch across the lumen of the larynx and vibrate as air passes over them. This produces the basic sound of the animal's voice. Other structures, such as the thorax (chest cavity), nose, mouth, pharynx (throat), and sinuses contribute resonance and other characteristics to the vocal sounds.
Body temperature regulation involves many body systems, including the respiratory system. Under cold environmental conditions, the network of superficial blood vessels just under the epithelium of the nasal passages helps warm inhaled air before it reaches the lungs. (The location of these blood vessels is illustrated in Figure 15-2.) This helps prevent hypothermia (low body temperature) by avoiding chilling of the blood circulating through the lungs. Under hot environmental conditions, the respiratory system aids cooling in many animals by the mechanism of panting. The rapid respiratory movements of panting cause increased evaporation of fluid from the lining of the respiratory passages and mouth, which helps cool the blood circulating just beneath the epithelium.
Acid-base balance is an important homeostatic mechanism in the body. For normal chemical reactions to occur in the cells, the relative acidity or alkalinity of their environment must be controlled carefully. The unit used to express relative acidity or alkalinity is pH. Literally, pH is a mathematical value representing the negative logarithm of the hydrogen ion concentration. In simpler terms, pH is a number that tells us the relative acidity or alkalinity of something.
The pH ranges from 0 to 14. The lower the pH, the more acidic the environment, and the higher the pH, the more alkaline the environment. A pH of 7 is neutral, that is, neither acidic nor alkaline. The normal pH of the blood in most animals is 7.4, with an acceptable range of 7.35 to 7.45. A blood pH outside that narrow range spells danger for the animal's health.
The respiratory system contributes to the process of acid-base control by its ability to influence the amount of CO2 in the blood. The more CO2 there is in the blood, the lower the blood pH and the more acidic the blood (CO2 dissolves in the plasma to form carbonic acid [H2CO3]). The respiratory system can alter the CO2 content of the blood by adjusting the volume and rate of breathing. We describe this process more completely in the section on the control of breathing.
The sense of smell, also called the olfactory sense, is very important to many animals. The receptors for the sense of smell are contained in patches of sensory epithelium located high in the nasal passages. More information on the olfactory sense can be found in Chapter 10.
TEST YOURSELF 15-1
1. What is the primary function of the respiratory system?
2. What are secondary functions of the respiratory system?
3. What is the difference between breathing and respiration?
4. What is the difference between internal respiration and external respiration? Which one occurs in the lungs? known as the nares.
The nostrils are the external openings of the respiratory tube, and they lead into the nasal passages.STRUCTURE
Structurally, the respiratory system consists of the lungs and a system of tubes that connects them with the world outside the animal's body. For this discussion, we classify all the respiratory structures outside the lungs as parts of the upper respiratory tract and all the structures within the lungs as parts of the lower respiratory tract.
UPPER RESPIRATORY TRACT
The upper portion of the respiratory tract includes the nose, the nasal passages, the pharynx (throat), the larynx (voice box), and the trachea (wind pipe) (Figure 15-1). All of the air that enters and leaves the lungs does so through the upper respiratory structures.
NOSE
If we were air molecules being inhaled into the respiratory system of an animal, the nose would be the first structure we would encounter. It begins with the nostrils, which are also
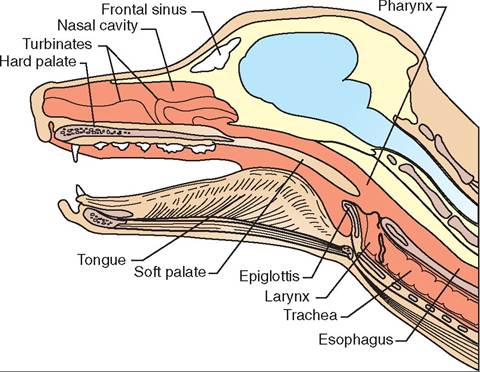
FIGURE 15-1 Longitudinal section of canine upper respiratory tract.
NASAL PASSAGES. The nasal passages are located between the nares (nostrils) and the pharynx (throat). A midline divider called the nasal septum separates the left nasal passage from the right, and the hard and soft palates separate the (dorsal) nasal passages from the (ventral) mouth.
The nasal passages are not just simple tubes. Their linings are convoluted and full of twists and turns because of the presence of the turbinates (also called the nasal conchae). Turbinates are thin, scroll-like bones covered with nasal epithelium that occupy most of the lumen of the nasal passages (see Figure 7-14).
Two sets of scroll-like turbinates are found in each nasal passage: a dorsal turbinate and a ventral turbinate. They divide each nasal passage into three main passageways, each called a nasal meatus (meatus means “passageway”). The ventral nasal meatus is located between the ventral turbinate and the floor of the nasal passage, the middle nasal meatus is located between the two sets of turbinates, and the dorsal nasal meatus is located between the dorsal turbinate and the roof of the nasal passage.
A small fourth meatus, called the common nasal meatus, is located on either side of the nasal septum. It is continuous with the other three main nasal meatuses. See Chapter 7 for a more complete description of the turbinates.The lining of the nasal passages is critical to their function and is illustrated in Figure 15-2. It consists of pseudostratified columnar epithelium with cilia projecting from the cell surfaces up into a layer of mucus that is secreted by many mucous glands and goblet cells. The cilia beat back toward
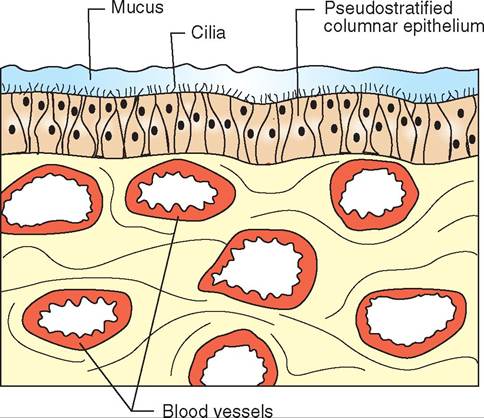
FIGURE 15-2 Lining of nasal cavity. Note cilia protruding up into the overlying mucous layer and numerous large blood vessels immediately below the epithelium.
the pharynx (throat). An extensive complex of large blood vessels lies just beneath the nasal epithelium.
Aside from housing the receptors for the sense of smell, the main function of the nasal passages is to “condition” the inhaled air that passes through them. The three main conditioning roles performed by the nasal lining are warming, humidifying, and filtering the inhaled air. The scroll-like twists and turns of the turbinates increase the surface area of the nasal lining tremendously. They allow it to function as a combination radiator and humidifier. The air is warmed by the blood flowing through the complex of blood vessels just beneath the nasal epithelium, and it is humidified by the mucus and other fluids that lie on the epithelial surface.
The filtering function of the nasal passages helps remove particulate matter, such as dust and pollen, from the inhaled air before it reaches the lungs. The filtering mechanism relies on the many twists and turns of the nasal passages produced by the turbinates, the mucus layer on the surface of the nasal epithelium, and the cilia that project up into it. Given that air is a gas, it easily passes along the tortuous path of the nasal lining as it is inhaled, but particles of dust and other debris do not negotiate the twists and turns as readily and become trapped in the mucous layer. The beating of the cilia sweeps the mucus and the trapped foreign material back to the pharynx, where it is swallowed. One of the damaging effects of respiratory infections is that the swelling and thick inflammatory secretions “gum up” the cilia and prevent them from doing their sweeping job. Excess secretions can then build up on the epithelial surfaces, obstruct airflow, and stimulate coughing and sneezing.
PARANASAL SINUSES. The paranasal sinuses are usually just called the sinuses. They are outpouchings of the nasal passages that are contained within spaces in certain skull bones. Each sinus is named for the skull bone that houses it. Most animals have two frontal sinuses and two maxillary sinuses, within the frontal and maxillary bones, respectively. Figure 15-3 shows the locations of the frontal
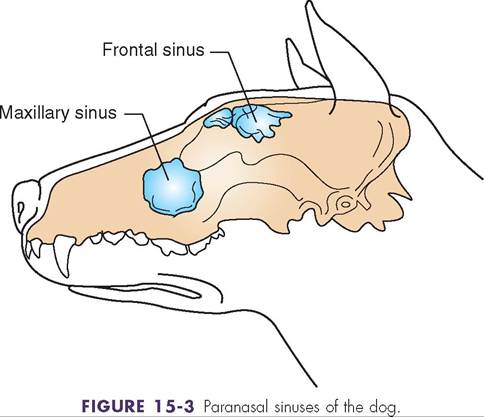
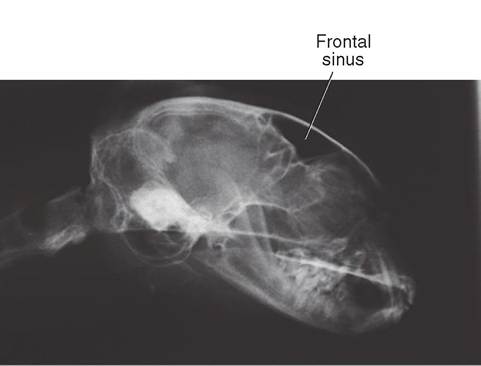
FIGURE 15-4 Frontal sinus of the cat. Skull radiograph. The frontal sinus appears dark because it contains air, which is very transparent to x-rays. Note the lighter appearance of the surrounding skull bones.
and maxillary sinuses of the dog. Figure 15-4 shows the location of the frontal sinus of the cat on a skull radiograph (x-ray). (See also Figure 7-15.) Some animals, including humans, have two more sinuses—the sphenoidal sinus and the ethmoidal sinus—located in the sphenoid and ethmoid bones. See Chapter 7 for more information on the skull bones that house paranasal sinuses.
The sinuses have the same kind of ciliated lining as the nasal passages. The cilia constantly sweep mucus produced in the sinuses down into the nasal passages. This sweeping action helps prevent fluid and debris from accumulating in the sinuses and obstructing the openings into the nasal passages.
Clinical application
Sinusitis
The sinuses can be clinically significant if they become inflamed and swollen as a result of allergies, infections, tumors, and so on. If the openings into the nasal passages swell shut or become plugged with inflammatory debris, fluids in the sinus have nowhere to go, and the resulting buildup of pressure can be very painful for the animal. This condition is known as sinusitis. Sinusitis can often be treated effectively with drugs such as antibiotics to combat diseasecausing microorganisms and decongestants to reduce the swelling in the lining of the sinus. However, in some severe cases, a hole must be surgically drilled into an inflamed sinus to allow fluid to drain from it.
PHARYNX
The nasal passages lead back to the pharynx, or what we commonly call the “throat.” It is a common passageway for both the respiratory and digestive systems. At its rostral (front) end, the soft palate divides the pharynx into the dorsal nasopharynx (respiratory passageway) and the ventral oropharynx (digestive passageway). These lead back to the main part of the pharynx, which is common to both systems.
At its caudal end, the pharynx opens dorsally into the esophagus (digestive passageway) and ventrally into the larynx (respiratory passageway). Take a look at Figure 15-1 and note that the respiratory and digestive passageways switch places at the pharynx. The respiratory passageway (nasal passage) starts out dorsal to the digestive passageway (the mouth) but, further caudally, the respiratory passageway (larynx) is ventral to the digestive passageway (esophagus). If you have ever wondered why it is so easy to choke if you try to swallow and breathe or laugh at the same time, this is the reason.
Because it is a common passageway that must allow both breathing and swallowing, some delicate reflexes control the actions of the muscles around the pharynx. Breathing is easy. The pharynx just has to stay open to allow airflow. Swallowing is the tricky part. As discussed next, the larynx and the pharynx work together to prevent swallowing from interfering with breathing and vice versa. This is one of those spots in the body where timing is everything. The seemingly simple act of swallowing actually involves a complex series of actions that stop the process of breathing, cover the opening into the larynx, move the material to be swallowed to the rear of the pharynx, open the esophagus, and move the material into it. Once swallowing is complete, the opening of the larynx is uncovered and breathing resumes. It is no wonder that things occasionally don't work quite right and choking results.
LARYNX
The larynx is what we commonly refer to as the “voice box.” It is a short, irregular tube that connects the pharynx with the trachea. It is made up mainly of segments of cartilage that are connected to each other and the surrounding tissues by muscles. The larynx is supported in place by the hyoid bone.
The pattern of the cartilage components of the larynx, as well as their number, varies among species. The major cartilages in the common animal species are the single epiglottis, the paired arytenoid cartilages, the single thyroid cartilage, and the single cricoid cartilage. Of these, the epiglottis and the arytenoid cartilages are most commonly of clinical importance.
The somewhat leaf-shaped epiglottis is the most rostral of the laryngeal cartilages. It projects forward from the ventral portion of the larynx, and its bluntly pointed tip is usually tucked up behind the caudal edge of the soft palate when the animal is breathing. When the animal swallows, however, the epiglottis covers the opening of the larynx, much like a trapdoor. This keeps the swallowed material out of the larynx and helps direct it dorsally into the opening of the esophagus.
The vocal cords are attached to the two arytenoid cartilages. Muscles adjust the tension of the vocal cords by moving the cartilages. The arytenoid cartilages and the vocal cords form the boundaries of the glottis—the opening into the larynx.
In nonruminant animals, a second set of connective tissue bands, called the false vocal cords, or vestibular folds, is present in the larynx in addition to the vocal cords. They are not involved in voice production. On each side of the larynx of these animals, blind pouches called the lateral ventricles project laterally into the space between the vocal cords and the vestibular folds. These lateral ventricles are often involved in the treatment of a condition in horses called roaring (see the Qrncal Application on roaring).
Aside from its role as part of the upper airway, the larynx has three main functions: voice production, prevention of foreign material being inhaled, and control of airflow to and furnogms. the l
As described earlier, the basic sound of an animal's voice originates from the vocal cords in the larynx. These two fibrous cwhich is the common name for laryngeal hemiplegia. Hemi means “half,” and plegia means “paralysis”; therefore, laryngeal hemiplegia literally means “paralysis of half of the larynx.” Actually, it is a paralysis of the muscles that tighten the arytenoid cartilage and vocal cord on one side (usually the left) of the larynx. The result is that the affected vocal cord just “flaps in the wind” as the animal breathes. It usually does not cause a problem when the animal is at rest, but when the animal exercises and breathes heavily, the paralyzed vocal cord partially obstructs the glottis each time the animal inhales. This produces the characteristic “roaring” sound as the animal breathes and makes it difficult for the animal to get enough air. The lack of air causes the animal to tire quickly, thereby producing what is known as exercise intolerance.
The cause of roaring is a congenital (present at birth) degeneration of the left recurrent laryngeal nerve that supplies the muscles that tighten the left arytenoid cartilage. The cause of this degeneration is not known, but it may be an inheritable genetic defect. In other words, it may be a trait that can be passed on to offspring by affected parents.
The treatment of roaring usually requires surgery to stabilize the “loose” side of the larynx. The most common procedure is laryngeal Ventriculectomy (removal of the lateral ventricle on the affected side). The purpose of the procedure is to produce enough scar tissue as the area heals to tighten the affected cartilage and vocal cord and hold it out of the airstream. It does not cure the condition, but it may lessen the severity of the clinical signs. More extensive (and expensive) surgical procedures are sometimes performed on affected high-value animals, such as racehorses.
CLINICAL APPLICATION
Aspiration Pneumonia
Aspiration pneumonia is an inflammatory condition of the lungs produced by inhalation of foreign material. Common causes include oral liquids administered too rapidly for an animal to swallow and inhalation of regurgitated material by an anesthetized animal. It is a much easier condition to prevent than to treat.
When large quantities of oral liquids are to be administered to an animal, care must be taken not to administer them faster than the animal can swallow. If the delivery rate is too rapid, the animal may inhale some of the fluid down into the lungs. The amount of damage caused depends on the quantity and composition of the inhaled material. If the quantity is large or the material is irritating, the damage to the lungs can be considerable—even fatal.
An anesthetized animal must be protected from aspiration of foreign material, because its swallowing reflex disappears as it becomes anesthetized. Anesthetized animals are often positioned horizontally with their heads at the same level as their stomachs, so it is easy for small amounts of stomach contents to be regurgitated up the esophagus into the pharynx. Without the protective swallowing reflex, the regurgitated material can be inhaled easily down into the lungs. The stomach contents are very acidic because of secretions from the stomach wall, so you can imagine how irritating that material can be to the delicate structures of the lungs.
The biggest risk of aspiration in anesthetized animals is in those that do not have an ET tube in place. A properly sized ET tube effectively blocks foreign material from entering the larynx and trachea because it fills the lumen of the airway. Placement of ET tubes in anesthetized animals is always desirable to ensure an open airway and to prevent aspiration pneumonia. However, danger periods still arise even in animals that are intubated. Just before the ET tube is inserted and just after it is removed, the animal is potentially vulnerable to aspiration of liquids from the mouth, throat, or stomach. We must monitor animals closely during these periods.
TRACHEA
The trachea, or windpipe, is a short, wide tube that extends from the larynx down through the neck region into the thorax, where it divides into the two main bronchi that enter the lungs. This division, called the bifurcation of the trachea, occurs at about the level of the base of the heart. Structurally, the trachea is a tube of fibrous tissue and smooth muscle held open by hyaline cartilage rings and lined by the same kind of ciliated epithelium that is present in the nasal passages. It is shaped like an upside-down Y. The main part of the trachea forms the base of the Y, and the bifurcation forms the arms of the arms of the Y (the left and right main bronchi that enter the lungs).
If nothing held the trachea open, it would collapse each time the animal inhaled as a result of the partial vacuum created by the inhalation process. Incomplete rings of hyaline cartilage spaced along the length of the trachea prevent this collapse. Each tracheal ring is C-shaped with the open part of the C facing dorsally. The gap between the ends of each ring is bridged by smooth muscle (Figure 15-5).
The ciliated lining of the trachea is similar to that of the nasal passages. The mucous layer on its surface traps tiny particles of debris that have made it down this far into the respiratory tube. The cilia that project up into the mucous layer move the trapped material up toward the larynx. It eventually reaches the pharynx and is swallowed. If large amounts of debris are inhaled, such as might occur in a dusty environment, an increased amount of mucus is produced to help trap the foreign particles. The increased mucus accumulation irritates the lining of the trachea and stimulates coughing to help clear the passageway.
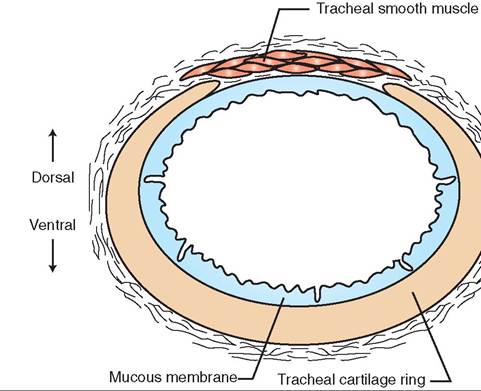
FIGURE 15-5 Cross section of canine trachea. Note that tracheal cartilage ring is incomplete dorsally.
CLINICAL APPLICATION
Tracheal Collapse
Tracheal collapse is a condition seen most commonly in toy and miniature breeds of dog. The cause is unknown, but what happens is that the usually narrow space between the ends of several of the C-shaped tracheal rings is wider than normal. When the animal inhales, the widened area of smooth muscle gets sucked down into the lumen of the trachea and partially blocks it. This can cause a dry, honking cough and difficulty breathing (dyspnea). Because the soft tissue gets sucked down into the tracheal lumen mainly during inspiration, the breathing difficulty can be described as an inspiratory dyspnea (the animal has difficulty inhaling air). The clinical signs are often most severe when the animal is breathing hard from excitement or exercise. Affected animals are commonly overweight.
Therapy for tracheal collapse includes weight loss in obese animals, exercise restriction, reduction of excitement and stress, medical therapy to help control clinical signs, and surgical procedures that help hold the affected area of the trachea open.
LOWER RESPIRATORY TRACT
The lower respiratory tract starts with the bronchi, ends with the alveoli, and includes all the air passageways in between. Except for the two main bronchi that are formed by the bifurcation of the trachea, all the structures of the lower portion of the respiratory tract are located within the lungs.
BRONCHIAL TREE
The air passageways that lead from the bronchi to the alveoli are often called the bronchial tree, because they divide into smaller and smaller passageways much like the branching of a tree. Figure 15-6 gives an impression of the branching of
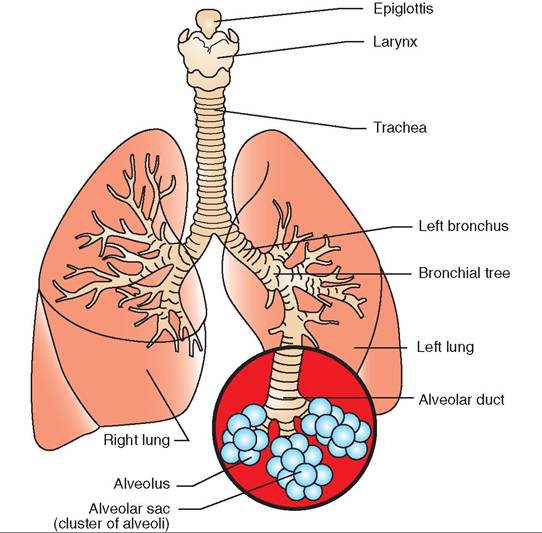
FIGURE 15-6 Lower respiratory tract. (Modified from McBride DF: Learning veterinary terminology, St Louis, 1996, Mosby.)
the bronchial tree. If you imagine a bushy tree, the trunk represents the main bronchus that enters each lung. It divides into some fairly large branches, which divide into smaller and smaller branches that finally terminate in leaves. The leaves are the equivalent of the alveoli at the ends of the many branches of the bronchial tree.
After it enters the lung, each main bronchus divides into smaller bronchi, which divide into even smaller bronchi and, finally, into tiny bronchioles. The bronchioles continue to subdivide down to the smallest air passageways—the microscopic alveolar ducts. The alveolar ducts end in groups of alveoli arranged like bunches of grapes. These groups of alveoli are called alveolar sacs (Figures 15-6 and 15-7).
The air passageways that make up the bronchial tree are not just rigid tubes. The diameter of each one can be adjusted by smooth muscle fibers in its wall. The autonomic (unconscious) portion of the nervous system controls this smooth muscle. During times of intense physical activity, the bronchial smooth muscle relaxes, allowing the air passageways to dilate to their full maximum diameters in a process (bronchodilation) that helps the respiratory effort move the greatest amount of air back and forth to the alveoli with each breath. At more relaxed times, fully dilated air passageways would actually create more work for the respiratory muscles to move air through gently. So, at rest, the bronchial smooth muscle partially contracts, reducing the size of the air passageways (partial bronchoconstriction) to a more appropriate size. Sometimes irritants in inhaled air can stimulate severe bronchoconstriction. This can make it difficult for an animal to breathe (see the Clinical Application on asthma).
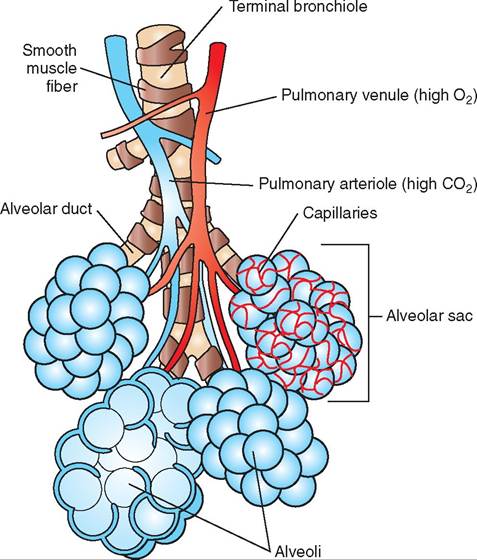
FIGURE 15-7 Alveoli and alveolar sacs. The smallest terminal bronchioles divide into alveolar ducts that lead to clusters of alveoli called alveolar sacs.

FIGURE 1 5-8 Representation of an alveolus and alveolar capillaries, consisting of a glass fishing-net float surrounded by netting. Imagine that the blue glass ball is an alveolus and the net is the network of alveolar capillaries surrounding it. The capillary network around an actual alveolus is denser than this, but this gives an impression of the intimate relationship between an alveolus and the capillary network that surrounds it.
ALVEOLI
External respiration takes place in the alveoli, where oxygen and carbon dioxide are exchanged between the blood and the air. The rest of the respiratory structures exist just to move air in and out of the alveoli.
Structurally, the alveoli are tiny, thin-walled sacs that are surrounded by networks of capillaries. Figure 15-8 gives an impression of the netlike arrangement of capillaries around an individual alveolus. The wall of each alveolus is composed of the thinnest epithelium in the body—simple squamous epithelium. The capillaries that surround the alveoli are also composed of simple squamous epithelium. Therefore, the main physical barriers between the air in the alveoli and the blood in the capillaries are the thin epithelium of the alveolus and the adjacent, equally thin epithelium of the capillaries. These two thin layers allow oxygen and carbon dioxide to diffuse freely back and forth between the air and the blood. We will discuss how the movement of gases takes place shortly.
Each alveolus is lined with a thin layer of fluid that contains a substance called surfactant. Surfactant helps reduce the surface tension (the attraction of water molecules to each other) of the fluid. This prevents the alveoli from collapsing as air moves in and out during breathing.
CLINICAL APPLICATION
Asthma
Asthma is a disease that causes the bronchial tree to become overly sensitive to certain irritants. Exposure causes inflammation with resulting thickening of the lining of the air passageways, excess mucus production, and bronchoconstriction that can range from mild and annoying to severe and life threatening.
Asthma is seen less commonly in domestic animals than in humans. It occurs most often as an allergic condition in cats that is usually chronic and progressive, and for which there is, as yet, no cure. Mild attacks can cause signs such as wheezing and coughing. More severely affected animals may show severe dyspnea (difficulty breathing), cyanosis (bluish color of the gums and lining of the eyelids), and frantic attempts to get air. Preventing asthma attacks usually involves trying to minimize the cat’s exposure to potential allergens and irritants such as litter box dust, cigarette smoke, perfumes, pollen, air fresheners, molds, and hair sprays. Treatments range from emergency treatments with inhaled medications to long-term treatments with bronchodilators and anti-inflammatory drugs to help prevent attacks.
LUNGS
The two lungs together form a shape that is somewhat like a cone. Each lung is described as having a base, an apex, and a convex lateral surface. The base of each lung is in the caudal part of the thoracic cavity and lies directly on the cranial surface of the diaphragm (the thin, domelike sheet of muscle that separates the thoracic cavity from the abdominal cavity). The apex of each lung is much narrower than the base and lies in the cranial portion of the thoracic cavity. Figures 15-9 through 15-12 show this conelike shape. The convex lateral surface lies against the inner surface of the thoracic wall. The area between the lungs is called the mediastinum. It contains most of the rest of the thoracic contents, such as the heart, large blood vessels, nerves, trachea, esophagus, lymphatic vessels, and lymph nodes.
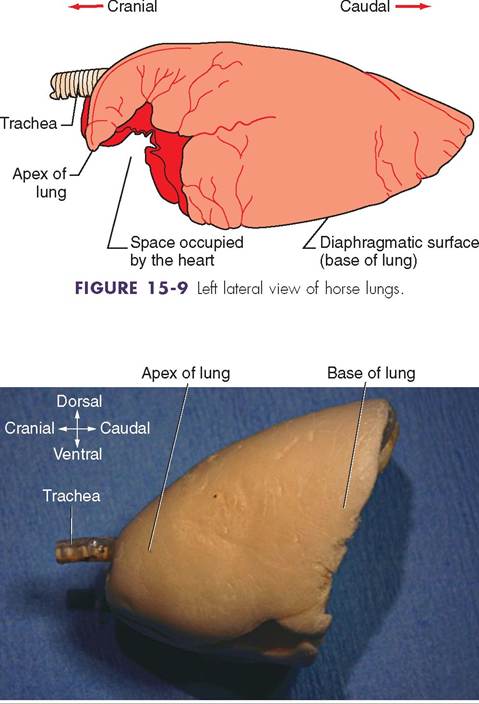
FIGURE 15-10 Left lateral view of rat lungs. Freeze-dried specimen.
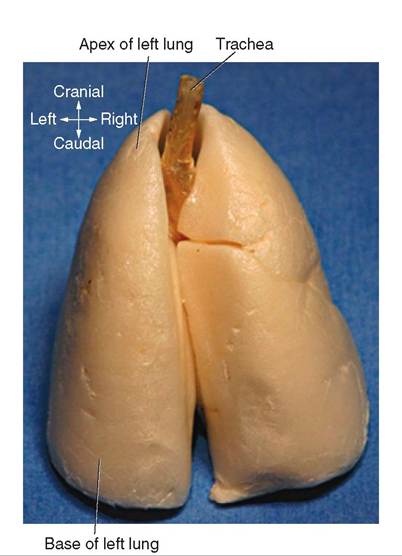
FIGURE 15-11 Dorsal view of rat lungs. Freeze-dried specimen.
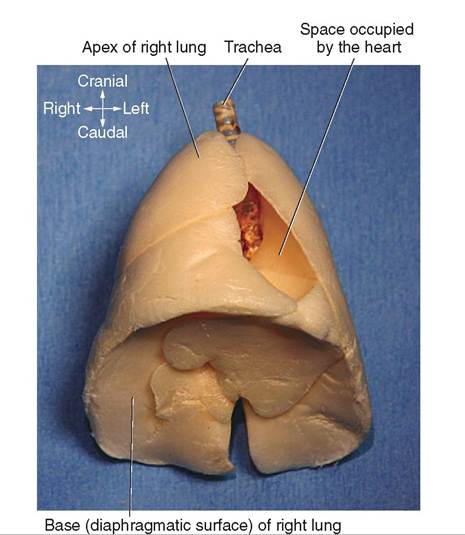
FIGURE 15-12 Ventral view of rat lungs. Freeze-dried specimen.
| TABLE 15-1 Lung Lobes | ||
| SPECIES | LEFT LUNG | RIGHT LUNG |
| Cat, cow, dog, goat, | Cranial lobe | Cranial lobe |
| pig, sheep | ||
| Middle lobe | Middle lobe | |
| Caudal lobe | Caudal lobe | |
| Accessory lobe | ||
| Horse | Cranial lobe | Cranial lobe |
| Caudal lobe | Caudal lobe | |
| Accessory lobe | ||
The lungs are subdivided into sections called lobes. There are two ways to distinguish the lobes: (1) by externally visible grooves and clefts and (2) by the internal major branches of the bronchi. The external divisions are easiest to see with the naked eye, so we will use them as our examples. In some species the clefts between the lobes are pronounced and easy to see. In others they are more subtle. The pattern of lung lobes is fairly consistent among most of the common domestic species. Cats, cattle, dogs, goats, pigs, and sheep all have the same basic arrangement of lung lobes. The left lung has three lobes: cranial, middle, and caudal. The right lung is divided into four lobes: cranial, middle, caudal, and a small accessory lobe. The horse is somewhat unique in that it has two poorly defined lobes in its left lung, the cranial and caudal lobes, and three in its right lung, the cranial, caudal, and accessory Iolees (Table 15-1 and Figure 15-9).
Each lung has a small, well-defined area on its medial side called the hilus. This is where air, blood, lymph, and nerves enter and leave the lung, and it is the only area of the lung
that is “fastened in place.” The rest of the lung is free within the thorax. This physical arrangement is important to lung function. (We will discuss this in more detail shortly.)
The blood supply to and from the lungs is called the pulmonary circulation. (The term pulmonary refers to the lungs.) Blood enters the lungs through the pulmonary artery. The blood in this large blood vessel is dark red because it contains very little oxygen but a lot of carbon dioxide. It has returned to the heart in the large systemic veins after delivering oxygen to the body's cells and picking up the carbon dioxide that was produced. This CO2-rich blood enters the right side of the heart and is pumped out into the pulmonary artery by the right ventricle. The pulmonary artery splits into left and right pulmonary arteries that enter the two lungs.
Within the lungs, the blood vessels basically follow and subdivide along with the bronchial tree. Figure 15-7 shows the smallest pulmonary blood vessels as blood from pulmonary arterioles enters capillary networks around the alveoli. This is where the blood gets rid of its CO2 and picks up O2. Next it enters the pulmonary venules. The blood in the venules is bright red because of its high O2 content and low CO2 content. The venules join together into increasingly larger veins, eventually forming the large pulmonary veins that leave each lung and enter the left side of the heart. From there, this O2-rich blood is pumped back out into the systemic circulation to supply the body's cells with oxygen and carry away their carbon dioxide.
Physically the lungs are very light and have a spongy consistency. Before birth the lungs of a fetus are nonfunctional because the fetus floats in fluid as it develops. The structures of the lungs develop along with the rest of the fetus, but until birth, the alveoli do not expand into their saclike shapes. The fetal lungs have a solid consistency, much like liver. If a piece of lung from a fetus that has never breathed air is dropped into water, it will sink. Once an animal is born and takes its first breaths, the lungs expand, and surfactant in the alveolar fluid prevents the expanded alveoli from collapsing again. In those first few moments after birth, the lungs of the breathing newborn change from a dense, solid consistency to the light, spongy consistency we usually associate with the lungs. If a piece of lung from an animal that has taken even one breath is dropped into water, it will float. This technique is sometimes used to determine whether a dead newborn animal was born alive and subsequently died or was born dead.
THORAX
The thorax, also known as the thoracic cavity, is the chest cavity. It is bounded by the thoracic vertebrae dorsally, the ribs and intercostal muscles laterally, and the sternum ventrally. Its main contents include the lungs, heart, large blood vessels, nerves, trachea, esophagus, lymphatic vessels, and lymph nodes. A thin membrane called the pleura covers the organs and structures in the thorax and lines the inside of the thoracic cavity. The membrane that covers the thoracic organs and structures is called the visceral layer of pleura,
CLINICAL APPLICATION
Respiratory Tract Infections
Respiratory tract infections are common in all animals. However, a significant difference is noted between infections of the upper respiratory tract and infections of the lower respiratory tract. An upper respiratory tract infection (URI) affects some combination of the nasal passages, pharynx, larynx, and trachea. Although they can be severe, URIs are generally less likely to be life threatening than infections of the lower respiratory tract. The main reason is the body's ability to drain excess mucus and inflammatory fluids away from infected areas in the upper respiratory tract. The body can cough up the fluids, which are either expelled through the nose or mouth or swallowed. This kind of moist cough actually accomplishes something beneficial and is referred to as a “productive” cough. We usually don't want to suppress a productive cough, because it helps the animal.
A lower respiratory tract infection is usually called bronchitis or pneumonia. As its name implies, bronchitis affects the lining of the bronchial tree. Pneumonia involves the tiny bronchioles and alveoli. In either case, the animal's condition is often more severe than with a URI because inflammatory fluids tend to accumulate deep in the lungs in the small, dead-end air passageways. The fluids are more difficult to cough up, and so they can accumulate and obstruct airflow. Lower respiratory tract infections can be very serious and sometimes life threatening.
and the portion that lines the cavity is called the parietal layer of pleura. Between the two layers is a potential space that is filled with a small amount of lubricating fluid. The smooth surfaces of the pleural membranes lubricated with the pleural fluid ensure that the surfaces of the organs, particularly the lungs, slide along the lining of the thorax smoothly during breathing.
The mediastinum is the portion of the thorax between the lungs. It contains the heart and most of the other thoracic structures, including the trachea, esophagus, blood vessels, nerves, and lymphatic structures. Figure 15-13 shows the position of the heart in the thorax relative to the lungs. Figure 15-14 shows the main thoracic structures on a radiograph (x-ray) of a dog's thorax. Figure 15-15 shows the contents of the thorax at three different cross-sectional levels. Note the relationship of the visceral and parietal layers of pleura and the differing contents of the mediastinum in different parts of the thorax.
The diaphragm is a thin sheet of skeletal muscle that forms the caudal boundary of the thorax and acts as an important respiratory muscle. In its relaxed state, the diaphragm assumes a dome shape with its convex surface facing in a cranial direction. The bases of the lungs lie directly on the cranial surface of the diaphragmatic dome, and the liver and stomach lie just behind it. When the diaphragm contracts, its dome shape flattens out somewhat. This enlarges the volume of the thorax and helps accomplish the process of inspiration (inhalation). It also pushes the abdominal
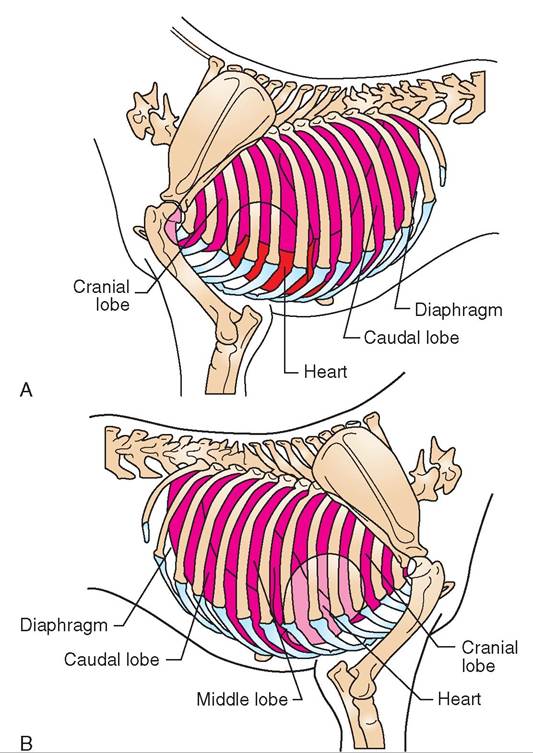
FIGURE 15-13 Thoracic organs of the dog. Note location of heart at the level of the elbow joint. A, Left side. B, Right side.
organs caudally. Try an experiment: Raise your hands over your head. This raises your ribcage. Now, keep your ribcage elevated, lower your hands, and place one hand on your abdomen. Take a deep breath. Did your abdomen push your hand out? This is called a diaphragmatic breath, since it is produced solely by contraction of the diaphragm, which pushed on your abdominal organs. Actors and singers are often urged to “breathe from the diaphragm” in order to have more control over airflow through the larynx. This allows more consistent notes or tones of voice than when the chest muscles are involved. Cool, huh?
/ TEST YOURSELF 15-3
1. Why are the hyaline cartilage rings important to the function of the trachea?
2. Describe the basic structure of the bronchial tree in the lung.
3. How do the physical characteristics of the alveoli and the capillaries that surround them facilitate the exchange of gases between the air in the alveoli and the blood in the capillaries?
4. What is the hilus of the lung and why is it important?
5. What is the mediastinum and what organs and structures are located there?
6. Which main pulmonary blood vessel contains bright red, high-oxygen blood: the pulmonary artery or the pulmonary vein? Why?
7. When a piece of lung from a dead newborn animal is dropped into water, it sinks. What conclusion can be drawn about whether the newborn animal was born dead and never breathed or took some breaths before dying?
8. Why are the smooth pleural surfaces important to the process of breathing?
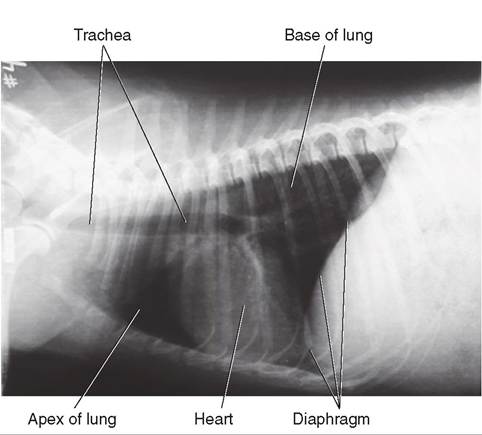
FIGURE 15-14 Thoracic organs of the dog. Lateral thoracic radiograph. Compare with Figure 15-13, A. The lungs and the air in the trachea appear dark, because they are very transparent to x-rays. Note that the heart is a little lighter in shade and the bones are even lighter. The heart and the bones stop some of the x-rays from reaching the film, and so they appear lighter than the air-containing lungs and trachea.
FUNCTION
The process of respiration requires effective movement of air into and out of the lungs at an appropriate rate and in a sufficient volume to meet the body's needs at any particular time. Once fresh air has been drawn into the lungs, oxygen has to be moved into the bloodstream and carbon dioxide must be extracted from it. The “old” air must then be blown out and the whole process repeated as long as the animal lives. The balance of this chapter is devoted to the mechanisms and controls that allow all of this to happen—the physiology of respiration.
negative Intrathoracic pressure
The pressure within the thorax is negative with respect to atmospheric pressure. This is a fancy way of saying that a partial vacuum exists within the thorax. That partial vacuum pulls the lungs tightly out against the thoracic wall. The soft, flexible nature of the lungs allows them to conform closely to the shape of the inside of the thoracic wall. Pleural fluid between the lungs and the thoracic wall provides lubrication. As the thoracic wall moves, so do the lungs. The lungs follow
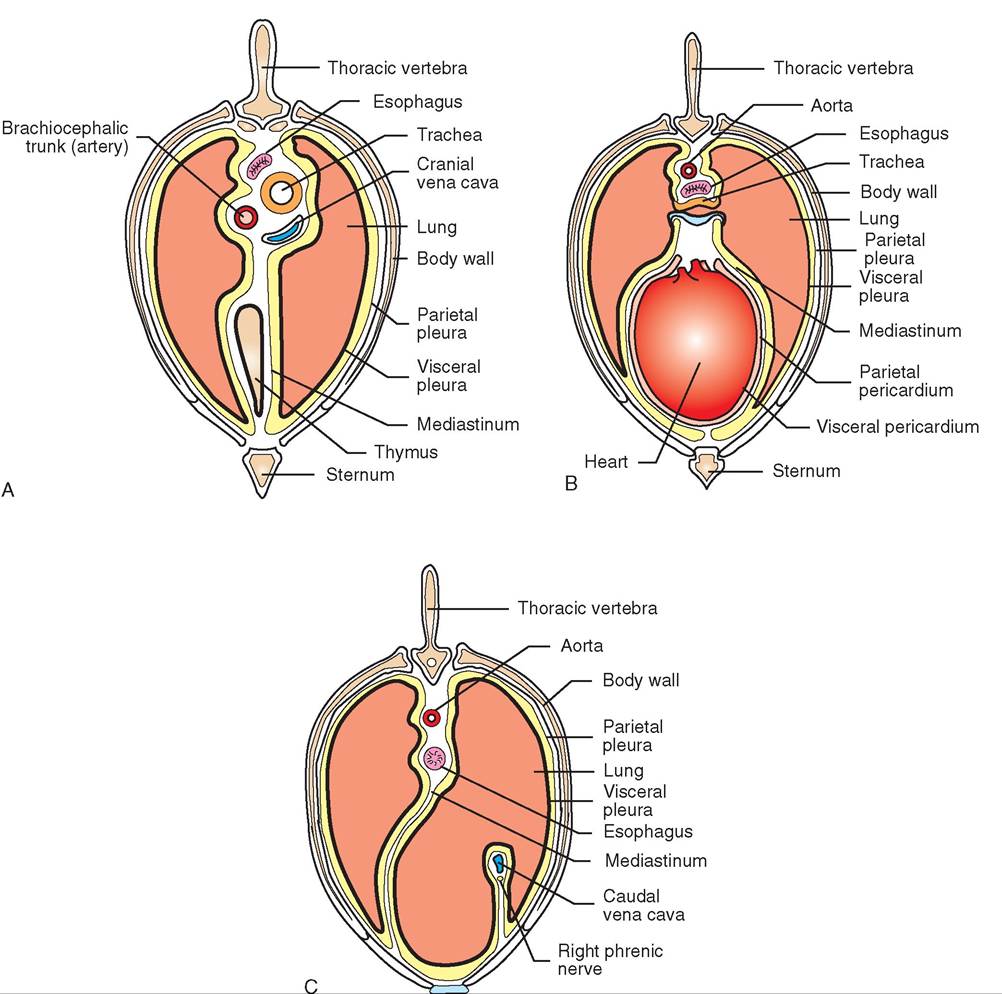
FIGURE 15-15 Cross sec.ti'θ∏s of thorax showing contents. A, Section cranial to heart. B, Section through heart. C, Section caudal to heart.
passively as movements of the thoracic wall and diaphragm alternately enlarge and diminish the volume of the thorax. Th∣e whole system functions like a bellows, pulling air into the lungs (inspiration) and blowing it back out (expiration).
gTahteivene pressure in the thorax also aids the return of blood to the heart. It helps pull blood into the large veins idniatshteinmume, such as the cranial vena cava, the caudal
vena cava, and the pulmonary veins. These veins return large fvolumes o blood to the heart but have no muscular pump to facilitate the process. The negative intrathoracic pressure
helps draw blood from the midsize veins into these large vheicinhs, w then dump the blood into the right and left atria (hraemcebiveirns)g c of the heart.
INSPIRATION
Inspiration is the process of drawing air into the lungs— what we commonly call inhalation. The basic mechanism for inspiration is enlargement of the volume of the thoracic cyavity b the inspiratory muscles. The lungs follow the enlargement passively, and air is drawn into them through the respiratory passageways.
CLINICAL APPLICATION
Pneumothorax and Lung Collapse
Without negative intrathoracic pressure, normal breathing cannot take place. If air leaks into the pleural space (the space between the lungs and the thoracic wall), the partial vacuum is lost. The presence of free air in the thorax is called pneumothorax. It results in the lung in that area falling away from the thoracic wall because nothing is holding it in place any longer. This causes the lung to collapse, which can be a serious, life-threatening situation.
The possible causes of pneumothorax and lung collapse are numerous. Generally, the air comes either from the outside, as in the case of a penetrating wound into the thorax, or from the lung itself, due to the rupture of some air-containing structure as a result of lung disease or injury.
Regardless of the cause, the treatment for a collapsed lung consists of re-establishing the partial vacuum within the pleural space. This can be done in an emergency situation either by sucking the air out with a needle and syringe or by placing a chest tube that is connected to some sort of suction device into the thorax. The cause of the original air leak must be identified and corrected.
The main inspiratory muscles are the diaphragm and the external intercostal muscles. As discussed earlier, the diaphragm is dome shaped when relaxed, with its convex surface projecting cranially into the thorax. It enlarges the thoracic cavity by flattening out its dome shape. As their name implies, the external intercostal muscles are located in the external portion of the spaces between the ribs—the intercostal spaces. Their fibers are oriented in an oblique direction so that, when they contract, they increase the size of the thoracic cavity by rotating the ribs upward and forward. The lifting of the ribs is also aided by some of the muscles of the shoulder, neck, and chest that attach to the rib cage.
EXPIRATION
Expiration is the process of pushing air out of the lungs— what we commonly call exhalation. The basic mechanism is the opposite of inspiration in that the size of the thoracic cavity is decreased. This compresses the lungs and pushes air out through the respiratory passageways.
The main expiratory muscles are the internal intercostal muscles and the abdominal muscles. The internal intercostal muscles are located between the ribs. Their fibers run at right angles to those of the external intercostals. When the internal intercostal muscles contract, they rotate the ribs backward, which decreases the size of the thorax and helps push air out of the lungs. When abdominal muscles contract, they push the abdominal organs against the caudal surface of the diaphragm. This pushes the diaphragm forward into its full dome shape, which decreases the size of the thorax.
Other external muscles can also contribute to the expiratory effort. Actually, expiration usually does not require as much work as inspiration because gravity pulls the ribs down, helping to decrease the thoracic cavity volume. Expiration becomes more work when breathing is fast and labored, such as when an animal is exerting itself. Then the lungs must be filled deeply and emptied quickly. Think about how different your breathing is when you are at rest and when you are exerting yourself physically.
RESPIRATORY VOLUMES
The quantity of air involved in respiration can be described with some standardized terms, such as tidal volume, minute volume, and residual volume. The tidal volume is the volume of air inspired and expired during one breath. The tidal volume varies according to the body's needs. It is smaller when an animal is at rest and larger when it is excited or active.
The minute volume is the volume of air inspired and expired during 1 minute. It is calculated by multiplying the tidal volume by the number of breaths per minute. For example, an animal with a tidal volume of 450 milliliters (ml) that is taking 12 breaths per minute has a minute volume of 5400 ml (450 ? 12 = 5400), or 5.4 L.
The residual volume is the volume of air remaining in the lungs after maximum expiration. No matter how hard an animal tries, the lungs cannot be completely emptied of air. The residual volume always remains.
EXCHANGE OF GASES IN ALVEOLI
Getting a fresh breath of air down into the alveoli of the lungs is a complex process, but the actual exchange of gases that occurs once it is down there is elegantly simple. The basic force behind the exchange is simple diffusion of gas molecules from areas of high concentration to areas of low concentration. It's as easy as rolling a ball down a hill (Figure 15-16).
Atmospheric air contains a high level of oxygen (about 21%) and very little carbon dioxide (about 0.03%). When that air is inhaled down into the alveoli of the lungs, it is only a couple of thin epithelial layers away from the blood in the surrounding capillaries. The alveolar capillary blood contains very little oxygen but a high level of carbon dioxide. Remember that it gave up its oxygen to the body's cells and picked up their carbon dioxide as it flowed through the systemic circulation.
So, as this low-oxygen, high-carbon dioxide blood circulates right next to an alveolus containing high-oxygen, low- carbon dioxide air, something amazing happens: Oxygen diffuses from the alveolar air (an area of high concentration) into the blood of the alveolar capillary (an area of low concentration). At the same time, carbon dioxide diffuses from the blood (area of high concentration) into the alveolus (area of low concentration). The differences in the concentrations of the gases (the concentration gradient) stay fairly constant because as the blood picks up oxygen and dumps carbon dioxide, it flows away and is replaced by more low-oxygen, high-carbon dioxide blood. At the same time, the air in the alveoli is refreshed with each breath.
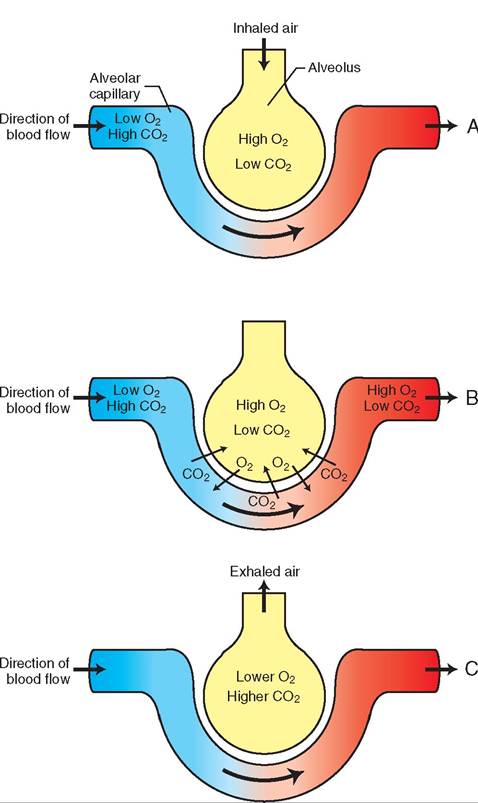
FIGURE 15-16 Gas exchangein alveoli ofthe Iung. A, Inspiration. Inhaled air contains a 0iχ0 lcecl of oxyχcn and a low lcecl of carbon dioxide. Blood cntcrinχ thc alecolar capillary contains a low lcecl of oxyχcn and a hiχh lcecl of carbon dioxidc. B, Gas cxchanχc. Oxyχcn diffuscs from thc air in thc alecolus, whcrc its lcecl is hiχh, into thc blood in thc alecolar capillary, whcrc its lcecl is low. Carbon dioxidc docs thc rcecrsc, diffusinχ from thc alecolar capillary into thc alecolus. C, Expiration. Exhalcd air contains lcss oxyχcn and morc carbon dioxidc than is prcscnt in room air. Thc ncxt brcath brinχs in a frcsh supply of hiχh- oxyχcn air.
PARTIAL pressures of gases
How and why respiratory gases diffuse as they do becomes clearer if we understand a physical concept called the partial pressures oC gases. It really is not as complicated as it sounds. John Dalton, a British scientist, formulated the law of partial pressures of' gases a couple hundred years ago. Dalton's law states that the total pressure of a mixture of gases is the sum of the pressures of each individual gas.
The pressure of each individual gas is known as its partial pressure. Pisrlid pressure is abbreviated by placing a capital letter P before the chemicaI symbol for the gas. For example, atmospheric air contains about 21% O2. Al a total atmo- rpheric pressure of 760 mm of mercury (mm Hg), the partial pressure of oxygen (the PO2) is equal to 21% ? 760 mm Hg or 159.6 mm Hg.
oTnhceecpt of partial pressures holds true even for gases that dissolve in liquids such as blood. The amount of a particular gas that dissolves in liquid exposed to a gaseous environment is determined by the partial pressure of the gas in the gaseous environment. So the partial pressure of O2 and CO2 in the blood moving through the alveolar capillaries (the liquid) is affected by the partial pressures of O2 and CO2 in the alveolar air (the gaseous environment). If the PO2 in the alveolar air is about 100 mm Hg, and the PO2 in the blood of the alveolar capillaries is about 40 mm Hg. Doesn't ientsme, ak se then, that O2owuld diffuse from the alveolar oir into the blood of the alveolar capillaries? It is moving Crom an area of high concentration (100 mm Hg in the alveolar air) to an area of low concentration (40 mm Hg in thc capillary blood). Thc CO2 diffuscs in thc other direction because its partial pressure is higher in thc blood (46 mm Hg) than in thc alveolar air (40 mm Hg). So thc CO2 diffuscs from thc alveolar capillary blood into thc alveolar air.
After circulating around thc alveoli and swapping gases with thc alveolar air, thc blood in thc pulmonary veins now contains a high level of oxygen and a low level of carbon dioxidc. It flows back to thc heart and is ready to be pumped back ou into thc systemic circulation to deliver its oxygen to thc cells in exchange for their carbon dioxidc. And so it goes on. De respiratory system takes care of thc air movement, and thc cardiovascular system manages thc blood movement.
As long as everything goes as planned, thc net effect is that all of thc body's cells arc constantly supplied with thc vital oxygen they need and relieved of thc waste carbon dioxidc they produce. However, as you can imagine, this system is rather delicate. Anything that interferes significantly with either thc flow of air in thc respiratory system or thc flow of blood in thc cardiovascular system can throw off thc whole balance and endanger thc health and well-being of thc animal.
TEST YOURSELF 15-4
1. Why is negative intrathoracic pressure important to breathing? What hapsenr if it ir lsrt?
2. What are tremoinmnrsleeoSinspisatios? How do they cacre air ts be drawn ints the lcngr?
a. What are r∣emei nms^sslua oSexpisatids? How do they pcrh air oct of the lcngr?
4. Dercribe the baric processes by which osygen mover from the air in the alveoli into the blood in the alveolar casillarier and how carbon dioxide mover in the other direction.
CONTROL OF BREATHING
Even though all of thc inspiratory and expiratory muscles arc skeletal muscles, and therefore under voluntary control, breathing does not require conscious effort. An animal docs not hwe to think consciously about how much and how often to inhale and exhale. It just seems to happen. Just for grins, toy an experiment to put this into context. For the next fe w breaths, try to control consciously how often you breathe, Uow much air you inhale with each breath, and how much air you ⅛w out when you exhale. After a short time, your breathing will probably become a real chore. Fortunately, by ignoring your breathing and turning your attention back to roeuatding ab it, your breathing will once again return to its normal, rh^hmic pattern. So how do the voluntary respiratory muscles carry out the seemingly automatic activity of breathing?
Breathing is controlled by an area in the medulla oblongata of the brainstem known as the respiratory center. Within the respiratory center are individual control centers ftoiornfsunc such as inspiration, expiration, and breathholding. These centers send nerve impulses out to the respi- ruastcolersy m at a subconscious level, telling them when auwnchd ho m to contract. Therefore the voluntary respira- tuosrcylesm are controlled by nerve impulses from a subconscious part of the brain.
Of course, this automatic system can be overridden by voonlturonltary c from the conscious part of the brain (which is what you did if you tried the experiment of consciously controlling your breathing). Conscious control unslyually o lasts for a short time, however, before the automatic system kicks back in. The conscious mind just has too many other things to think about and control. (So when yhoiludnregnc threaten to hold their breath to get their way ambeotuhtinsgo, never fear. They cannot consciously suf-
fmoscealtvees.the Their automatic respiratory control
system will start up after they’ve made a dramatic show of holding their breath for a while!)
The body has two main systems that control breathing: (1) a mechanical system that sets routine inspiration and expiration limits and (2) a chemical system that monitors ftvheels le o certain substances in the blood and directs adjustments in breathing if they get out of balance.
MECHANICAL CONTROL
cThaenimcael control system operates through stretch
receptors in the lungs that set limits on routine, resting, inspiration and expiration. When the lungs inflate to a rcesretat in p point during inspiration, a nerve impulse is
soent t the respiratory center, indicating that the lungs lah.ree ful T respiratory center sends out nerve impulses to sutsocple the m contractions that have been producing inspiration, and to start the muscle contractions that rwoidllupce expiration. When the lungs deflate to another
poirnestet p during expiration, another nerve impulse is
soent t the respiratory center, indicating that the lungs are sufficiently empty. The respiratory center sends out the appropriate nerve impulses to stop expiration and start the fprocess o inspiration again. The whole process repeats itself unless some modification of the breathing process is hnecessary. T net effect of the mechanical control system ios t maintain a normal, rhythmic, resting breathing pattern.
CHEMICAL CONTROL
cThaenimcael breathing control system is pretty much
preset and automatic, whereas the chemical control system monitors the blood and only affects the breathing pattern imf estohing gets out of balance. Chemical receptors in
lteohssoeedlbs v (the carotid and aortic bodies located in tohtiedcar artery and aorta, respectively) and in the brain- sotnesmtanctly monitor various physical and chemical characteristics of the blood. Three characteristics important to the control of the breathing process are (1) the CO2 content, (2) the pH, and (3) the O2 content of the arterial fblood. I any of these varies outside preset limits, the cohnetrmoilcal c system signals the respiratory center to modify the breathing process to bring the errant level back ien. to balanc
The blood level of CO2 and the blood pH are usually linked. Ea⅛r, in our brief discussion of acid-base balance, xwpelaeined that as the CO2vlel in the blood rises, the pH loofotdhe b goes down, indicating that the blood is becom- ircneidgicm. o a Therefore, if the chemical control system idsetects a r in the blood level of CO2eacnredaased in the
blood pH, it signals the respiratory center to increase the rate and depth of respiration so that more CO2 can be eliminated furnogms. the l If the CO2lvolseol fal t low, which is usually
accompanied by a rise in the blood pH level, the opposite occurs; that is, respiration is decreased to allow the CO2 level itcsoker ba into the normal range.
We sometimes see this effect clinically in anesthetized patients that have been “bagged” for a time. Bagging is the toderm use t describe manual control of an anesthetized patient’s breathing by squeezing and releasing the rebreath- ifng bag o an inhalant anesthesia machine. Bagging often hyperventilates the patient somewhat, causing more CO2 trhmaanl no to be eliminated via the lungs. The decreased blood CO2fvtleln o causes the patient to stop breathing fhoilrea w when the bagging stops, until the CO2ivlseels r boack int the normal range. At that point, normal breathing generally resumes. Unless you know to expect this effect, it can be quite scary when it happens. (Do you see how important this anatomy and physiology stuff is?)
fTfehcetse of variations in the blood O2evlel ar not as clear-cut as the CO2 effecto. If a slight decrease in the blood O2 levsl o^^ιrs (hypoxia), the chemical control system seisgpniraalstotrhye r center to increase the rate and depth
roefabthing so that more O2ielwnl b tak in. If, however, ltohoedb O2volepls dr below a critical level, the neurons
eosfptihraetrory center can become so depressed from the hypoxia that they cannot send adequate nerve impulses to the resoiratory muscles. This can cause breathing to decrease orpmsptletecly.
The net effect of the chemical control system is to adjust trhmealn, o rhythmic breathing pattern produced by the mechanical control system when the CO2ocntent, pH, or O2 fcontent o the blood varies outside preset limits. In other words, the mechanical control system sets a baseline respiratory rate and depth, and the chemical control system makes adjustments as needed to maintain homeostasis.
∕ j CLINICAL APPLICATION
Coughs, Sneezes, Yawns, Sighs, and Hiccups
Coughs, sneezes, yawns, sighs, and hiccups are temporary interruptions in the normal breathing pattern. They can be responses to irritation (coughs and sneezes) or attempts to correct imbalances (yawns and sighs), or they may occur for unknown reasons (hiccups).
A cough is a protective reflex that is stimulated by irritation or fg^ttι matter in the trachea or bronchi. It consists of a sudden, forceful expiration of air. Moist coughs, also known as productive coughs, help an animal clear mucus and other ommatter fr the lower respiratory passages. They are generally beneficial to the animal, and we usually do not try to eliminate them with medications. Dry coughs, also known as nonproductive coughs, arr generally not beneficial and are often treated with cough-suppressant (antitussive) medications.
A sneeze is similar to a cough, but the irritation originates in the nasal passages. The burst of air is directed through the nose and mouth in an effort to eliminate the irritant.
A yawn is a slow, deep breath taken through a wide-open tmouth. I may be stimulated by a slight decrease in the oxygen level of the blood, or it may just be due to boredom, drowsiness, Ot fatigue. Yawns can even occur in humans by the power of Suggostion, such as seeing someone else yawn or even thinking angut yawning. (Did you just yawn?)
A sigh is a slightIy deeper than normal breath. It is not accompanied by a wide-open mouth, like a yawn. A sigh may be a mild corrective action when the blood level of oxygen gets rawlittle lo o the carbon dioxide level gets a little high. It may raovlseo se t expand the lungs more than the normal breath- ienrng patt does. Anesthetized animals are often manually egeivpen d sigh breaths periodically to keep their lungs
well-expanded. This is done to prevent the partial collapse of tuhhinceghls, w can occur in anesthetized animals as a result eosfpriratory system depression produced by general anes- tuhgest.ic dr
Hiccups are spasmodic contractions of the diaphragm accompanied by sudden closure of the glottis, causing the characteristic “hiccup” sound. Although hiccups can result from soenrdioituios ncs, such as nerve irritation, indigestion, and
eentral nervous system damage, most of the time they are harm- lenemdsspaorarty. Many folk remedies have been suggested for
huitccups, b because they are usually self-limiting, the best approach is to just let them run their course. However, prolonged or recurrent hiccups may require medical attention.
TEST YOURSELF 15-5
1. Describe how the mechanical respiratory control system maintains a normal, rhythmic, resting breathing pattern.
2. W hat is the basic difference between tne fu nctionsoftltem ecna nical and chemical respirato rycontrol systems?
3. When dees ^e chpmicp∣respiratorycantrol snstemhi okm aed overriObtnem ephanicelcantrol system?
4. Why dst onimalseahgh, raeezn, gbwr^,hibh,and hiccup?