The Skeletal System
Thomas Colville
OUTLINE
INTRODUCTION, 172
BONE, 173
Bone Terminology, 173
Bone Characteristics, 173
Functions of Bones, 173
Bone Structure, 173
Bone Cells, 176
Blood Supply to Bone, 176
Bone Formation, 176
Bone Shapes, 177
Bone Marrow, 178
Common Bone Features, 178
AXIAL SKELETON, 180
Skull, 180
Hyoid Bone, 188
Spinal Column, 188
Ribs, 192
Sternum, 193
APPENDICULAR SKELETON, 193
Thoracic Limb, 193
Pelvic Limb, 199
VISCERAL SKELETON, 204
JOINTS, 204
Joint Terminology, 204
Types of Joint, 204
Ball-and-Socket Joints, 209
LEARNING OBJECTIVES
When you have completed this chapter you will be able to:
1.
List the cell types that comprise bone and describe the function of each cell type.2. List the functions of bone.
3. Differentiate between cancellous and compact bone.
4. Describe the process of endochondral bone formation and growth.
5. Describe the process of intramembranous bone formation.
6. List and describe the four bone shapes.
7. Differentiate between yellow and red bone marrow.
8. List and define the terms used to describe shape and surface features of bone.
9. List the components of the axial and appendicular skeletons.
10. Name the internal and external bones of the face and cranium.
11. List the divisions of the spinal column.
12. Describe the structure of the ribs and sternum.
13. Name the bones of the thoracic and pelvic limbs.
14. List and describe the three classifications of joints.
VOCABULARY FUNDAMENTALS
Abduction ahb-duhck-shuhn
Acetabulum ahs-eh-tahb-yuh-luhm
Adduction ahd-duhck-shun
Amphiarthrosis ahm-fih-ahrth-ro-sihs
Anconeal process ahn-ko-ne-ahl proh-sehs Antebrachium ahn-te-bra-ke-uhm
Appendicular skeleton ahp-ehn-dihck-u-lar skehl-ih-tuhn
Arthrodial joint ahrth-ro-de-ahl joynt
Articular cartilage ahr-tihck-yuh-lor kahr-tih-lihj Articular process ahr-tihck-yuh-lor proh-sehs Articular surface ahr-tihck-yuh-lor suhr-fihs
Asternal rib a-stuhrn-ahl rihb
Atlas aht-lehs
Axial skeleton ahck-se-ahl skehl-ih-tuhn
Axis ahck-sihs
Ball-and-socket joint bahl and sohck-eht joynt
Body condition scoring (BCS) boh-de kohn-dihsh-shuhn skohr-ihng
Bone cortex bon kohr-tehx
Bone marrow bon mear-o
Bone of the cranium bon of the kra-ne-uhm
Bone of the ear bon of the er
Bone of the face bon of the fas
Brachium bra-ke-uhm
Brachycephalic brahck-e-seh-fahl-ihck
Calcaneal tuberosity kahl-kan-e-ahl too-buh-rohs-ih-te
Calciotropic kahl-se-ah-trδp-ihck
Calcitanin kahl-sih-tδ-nihn
Canaliculi kahn-ahl-ihck-yoo-lι
Cancellous bone kahn-sehl-uhs bon
Cannon bone kahn-nuhn bon
Carpal bone kahr-puhl bon
Carpus kahr-puhs
Cartilaginous kahr-tih-lahj -ehn-uhs
Cervical vertebrae sihr-vihck-ahl vart-eh-bra
Circumduction sihr-kuhm-duhck-shuhn
Coccygeal vertebrae kohck-sihj-e-ahl vart-eh-bra
Coccyx kohck-sihcks
Collateral ko-laht-or-ahl
Compact bone kohm-pahckt bon
Condyle kohn-dιl
Costal cartilage kohst-ahl kahr-tih-lihj
Costochondral junction kohst-o-kohn-drahl juhngk-shuhn
Cranium kra-ne-uhm
Cribriform plate krihb-reh-fohrm plat
Dens dehnz
Dewclaw doo-klaw
Diaphysis dι-ah-fih-sihs
Diarthrosis dι-ahrth-rδ-sihs
Digit dihj-iht
Distal sesamoid bone dihs-tahl sehs-ah-moyd bon
Dolichocephalic do-lih-ko-seh-fahl-ihck
Endochondral bone formation ehn-do-kohn-drahl bon fohr-ma-shuhn
Endosteum ehnd-ohs-te-uhm
Epiphyseal fracture ehp-ih-fihz-e-ahl frahck-chor
Epiphyseal plate ehp-ih-fihz-e-ahl plat
Epiphysis e-pihf-eh-sihs
Ethmoid bone ehth-moyd bon
Ethmoidal sinus ehth-moyd-ahl sι-nuhs
Extension ehck-stehn-shuhn
External acoustic meatus ehcks-tar-nahl ah-koo-stihck me-a-tuhs
Fabella fah-behl-lah
Facet fah-seht
Femur fe-mor
Fetlock joint feht-lohck joynt
Fibrous joint fi-bruhs joynt
Fibula fihb-u-lah
Flat bone flaht bon
Flexion flehck-shuhn
Floating rib flδ-fihng rihb
Foramen fohr-a-mehn
Foramen magnum fohr-a-mehn mahg-nuhm
Fossa fohs-ah
Frontal bone fruhn-tahl bon
Fursontal sin fruhn-tahl si-nuhs
Ginglymus joint gihng-gluh-muhs joint
Glenoid cavity gle-noyd kahv-ih-te
Gliding joint glι-dihng joynt
Grewth plate groth plat
FIard palate hahrd pahl-iht
Haversian canal hah-var-zhehn kuh-nahl
Haversian system hah-var-zhehn sihs-tehm
Head hehd
Hematopoiesis he-mah-to-poy-e-sihs
Hematopoietic tissue he-mah-to-poy-eh-tihck tihsh-yoo oHiinntge j yhnihtnj jo
Hip dysplasia hihp dihs-pla-zhuh
Hock hohck
Humerus hu-mor-uhs
Hyoid apparatus hι-oyd ahp-uh-raht-uhs
Hyoid bone hι-oyd bon
Ilium ihl-e-uhm
Incisive bone ihn-sι-sihv bon
Incus ihng-kuhs
Interparietal bone ihn-tor-pah-rι-eh-tahl bon
Intervertebral disc ihn-tor-var-teh-brahl dihsk
Intramembranous bone formation ihn-trah-mehm-bruh- nuhs boonhfr- ma-shuhn
Irregular bone ihr-rehg-u-lor bon
Ischium ihs-ke-uhm
Joint joynt
Joent capsule joynt kahp-sehl
Jvoitiynt ca joynt kahv-ih-te
Jaocient sp joynt spas
Lacrimal bone lah-kreh-mahl bon
Ligament lihg-ah-mehnt
Long bone lohng bon
Lumbar vertebrae luhm-bahr vart-eh-bra
Malleus mahl-e-uhs
Mandible mahn-dih-buhl
Mandibular symphysis mahn-dihb-u-lahr
sihm-fih-sihs
Manubrium mah-noo-bre-uhm
Maxillary bone mahck-seh-leor-e bon
Maxillary sinus mahck-seh-leor-e sι-nehs
Meniscus meh-nihs-kuhs
Metacarpal bone meht-ah kahr-pahl bon
Metatarsal bone meht-ah tahr-sahl bon
Nasal bone naz-ahl bon
Nasaa conchae naz-ahl kohng-ke
Nasal ^um naz-ahl sehp-tuhm
Navicular bone nuh-vihck-u-lor bon
Neck nehck
Nutrient foramen noo-tre-ehnt fohr-a-mehn
Obturator Jormen ohb-tor-a-tor fohr-a-mehn
Occipital bone ohck-sihp-eh-tahl bon
Occipital condyle ohck-sihp-eh-tahl kohn-dιl
Olecranon process o-lehck-reh-nohn proh-sehs
Os csrdis ohz kohr-dihs
Os penis ohz pe-nihs
Os rostri ohz rohs-trι
Ossicle ohs-eh-kuhl
Ossification ohs-eh-fih-ka-shuhn
Osteoblast ohs-te-o-blahst
Osteoclast ohs-te-o-klahst
Osteocyte ohs-te-o-sιt
Palatine bone pahl-ah-tιn bon
Palpation pahl-pa-shuhn
Paranasal sinus pahr-ah-na-sahl sι-nehs
Parathyroid hormone pahr-ah-thι-royd hohr-mon
Parietal bone pah-rι-eh-tahl bon
Patella pah-tehl-ah
Patellar ligament pah-tehl-ahr lihg-ah-mehnt
Pelvic limb pehl-vihck lihm
Pel-vic symphysis pehl-vihck sihm-fih-sihs
Pelvis pehl-vihs
Periosteum peor-e-ohst-e-uhm
Phalanges fah-lahn-jez
Phalanx fah-lahngks
Pituitary fossa pih-too-ih-teor-e fohs-ah
Pivot joint pihv-eht joynt
Priniary growth center prι-mahr-e groth sehn-tor
Process proh-sehs
Proximal sesamoid bone prohck-sih-mahl sehs-ah-moyd bon
Pterygoid bone tear-ih-goyd bon
Pubis pyoo-bihs
Radius rad-e-uhs
Ramus of the mandible ra-muhs of the mahn-dih-buhl
Red bone marrow rehd bon mear-o
Rib rihb
Rotation ro-ta-shuhn
Sacral vertebrae sa-krahl vart-eh-bra
Sacroiliac joint sa-kro-ihl-e-ahck joynt
Sacrum sa-kruhm
Scapula skahp-u-luh
Secondary growth center sehk-uhn-dahr-e groth sehn-tor
Sesamoid bone sehs-ah-moyd bon
Shaft of the mandible shahft of the mahn-dih-buhl
Short bone shohrt bon
Skull skuhl
Sphenoid bone sfe-noyd bon
Sphenoidal sinus sfe-noyd-ahl sι-nuhs
Spheroidal joint sfeer-oyd-ahl joynt
Spinal canal spι-nahl kuh-nahl
Spinal column spι-nahl kohl-uhm
Spinous process spι-nuhs proh-sehs
Splint bone splihnt bon
Stapes sta-pes
iSbternal r stari-hnbahl r
Sternebrae star-neh-bra
Sternum star-nuhm
Stifle joint stι-fuhl joynt
Suture soo-chor
Synarthrosis sihn-ahrth-ro-sihs
Synovial fluid sihn-o-ve-ahl floo-ihd
Synovial joint sihn-o-ve-ahl joint
Synovial membrane sihn-o-ve-ahl mehm-bran
Tarsal bone tahr-sahl bon
Tarsus tahr-suhs
Temporal bone tehm-pohr-ahl bon
Temporomandibular joint tehm-pohr-o-mahn-dihb-u- lyanhtr jo
Thoracic limb thohr-ah-sihck lihm
Thoracic vertebrae thohr-ah-sihck vart-eh-bra
Tibia tih-be-ah
Tibial crest tih-be-ahl krehst
Transverse process trahnz-vars proh-sehs oTirnotchoid j tro-yknotyd jo
Turbinate tuhr-buh-nat
Tympanic membrane tihm-pahn-ihck
mehm-bran
Ulna uhl-nah
Ungual process uhng-gwuhl proh-sehs
Vertebra vart-eh-brah
Vertebral vor-teh-brahl kohl-uhm
Visceral skeleton vih-sor-ahl skehl-ih-tuhn
Volkmann’s canal vawhlk-mahnz kuh-nahl
Vomer bone vo-mor bon
Xiphoid zι-foyd
Yellow bone marrow yehl-lo bon mear-o
Zygomatic arch zι-go-maht-ihck ahrch
Zygomatic bone zι-go-maht-ihck bon
INTRODUCTION
Try to imagine what an animal's body would be like without a skeleton.
Picture a furry sac of semisoft, gelatinlike material lying on the ground twitching. That is about what it would look like. The other connective tissues would hold the cells together, and the muscles would still contract and attempt to move the body; however, without bones to support it and give the muscles leverage, the body would lie on the ground, unable to accomplish anything useful.The skeleton is the framework of bones that supports and protects the soft tissues of the body. Besides making up the skeleton, the bones also serve a variety of other important functions. Before discussing the parts of the skeleton, let us take a look at bone—what it is, what it does, and some of its common characteristics.
BONE
BONE TERMINOLOGY
The terms os and osteo- generally refer to bone. For example, the os penis is a bone in the penis of dogs and osteocytes are bone cells.
BONE CHARACTERISTICS
Bone is one of the most fascinating body tissues. It is the second hardest natural substance in the body—only the enamel of the teeth is harder. Despite its dead, rocklike appearance, bone is a vital, living tissue with an excellent capacity to repair itself after injury. All that is usually necessary for broken bones to heal is for the broken ends to be brought together in some reasonable sort of alignment and then kept from moving for a few weeks or months. (See the Clinical Application on fracture repair for more information.)
Bone is composed of a sparse population of cells embedded in a hard intercellular substance called the matrix. The cells that produce bone are called osteoblasts: the suffix blast indicates a cell that produces something. Osteoblasts secrete the matrix, which is initially soft and composed of collagen fibers embedded in a gelatin-like ground substance made of protein and complex carbohydrates called polysaccharides.
The osteoblasts then harden the matrix through a process called ossification. When ossification takes place, the matrix is infiltrated with calcium and phosphate in the form of hydroxyapatite crystals.
These hydroxyapatite crystals give bone its characteristic hardness. As they create areas of bone, the osteoblasts become trapped in spaces in the ossified matrix called lacunae. Once they are surrounded by bone, the former osteoblasts get a new identity (kind of like people in the Witness Protection Program). They are now called osteocytes or bone cells.Osteocytes live out their days in their little cell-like lacunae. Their only contact with each other or with their blood supply is through threadlike, cellular processes in tiny channels through the bone called canaliculi. The canaliculi are like slots in the jail cell doors through which the osteo- cytes get food and communicate with each other.
Functions of bones
support
The most basic function of bone is to support the animal body. The cells and tissues that make up the rest of the body are fairly soft and do not have much inherent strength, so the bones serve as a sort of scaffolding to support them. The rest of the body either hangs from the bones or is attached directly to them.
PROTECTION
Bones also have an important protective function. Their firm strength protects many delicate, vital organs and tissues by surrounding them partially or completely. For example, the bones of the skull protect the brain and the delicate structures of the eyes and ears.
LEVERAGE
Bones act as levers for the skeletal muscles to move the body. Attachment of skeletal muscles to bones via the tendons allows the muscles to move the joints. This lets the animal move around in its environment.
STORAGE
Bones act as storage sites for minerals, particularly calcium. They act as reservoirs or “banks” for this important mineral. They enable the body to deposit and withdraw calcium as needed to control its level in the bloodstream precisely.
Calcium is involved in many important body functions, including muscle contraction, blood clotting, milk secretion, and skeleton formation and maintenance. Its level in the blood must be kept within a narrow range for these functions to proceed without difficulty.
Two hormones, calcitonin from the thyroid gland and parathyroid hormone from the parathyroid glands, act as “cashiers” at the calcium bank. Calcitonin helps prevent hypercalcemia, which is too high a level of calcium in the blood. Parathyroid hormone does the opposite: it helps prevent hypocalcemia.CLINICAL APPLICATION
The Role of Bones in Calcium Homeostasis
Calcium homeostasis is regulated by two calciotropic hormones, each of which has effects on bones. (Calcitropic means they are involved in the regulation of calcium levels in the body.)
When the level of calcium in the blood begins to rise too high, the hormone calcitonin is secreted by the thyroid glands. This encourages calcium to be deposited in the bones by osteoblasts, inhibits bone reabsorption by osteoclasts, and increases the amount of calcium excreted by the kidneys into the urine. All of these actions help decrease the amount of calcium in the blood.
When the level of calcium in the blood drops too low, parathyroid hormone is released from the parathyroid glands. This hormone inhibits calcium deposition in bones by osteoblasts, encourages osteoclasts to withdraw calcium from bones, and causes calcium to be retained by the kidneys by decreasing the amount excreted in the urine. These actions all serve to increase the amount of calcium in the blood.
This depositing and withdrawal of calcium from the bones goes on constantly as the body’s needs and the contents of its food supply change. (Chapter 11 explains this process more fully.)
BLOOD CELL FORMATION
Some of the bones serve as sites for blood cell formation— which is called hematopoiesis—in the bone marrow that fills their interiors. This will be covered in more depth later.
BONE STRUCTURE
The two main types of bone are light, spongy, cancellous bone and heavy, dense, compact bone.
CANCELLOUS BONE
Cancellous bone is sometimes called spongy bone because it looks like a sponge (Figures 7-1 and 7-2). It consists of tiny spicules of bone that appear randomly arranged with lots of spaces between them, like a bunch of pick-up-sticks that have been tossed into a pile.
The spaces between the spicules are occupied by bone marrow. To the naked eye, the many spicules and spaces give cancellous bone its spongy appearance. It is light but amazingly strong and helps reduce the weight of the bones of the skeleton without significantly reducing their strength. The organization of the spicules of cancellous bone appears random, but they are actually arranged to stand up to the forces the bone is subjected to. Muscles, gravity, and other bones all push and pull on bones constantly. The makeup of cancellous bone helps keep the bones light while also preventing them from being damaged by all the forces acting on them.COMPACT BONE
Compact bone is very heavy, dense, and strong. It makes up the shafts of long bones and the outside layer of all bones. It is composed of tiny, tightly compacted cylinders of bone called Haversian systems (see Figure 7-2). Each Haversian system runs lengthwise to the bone and consists of a
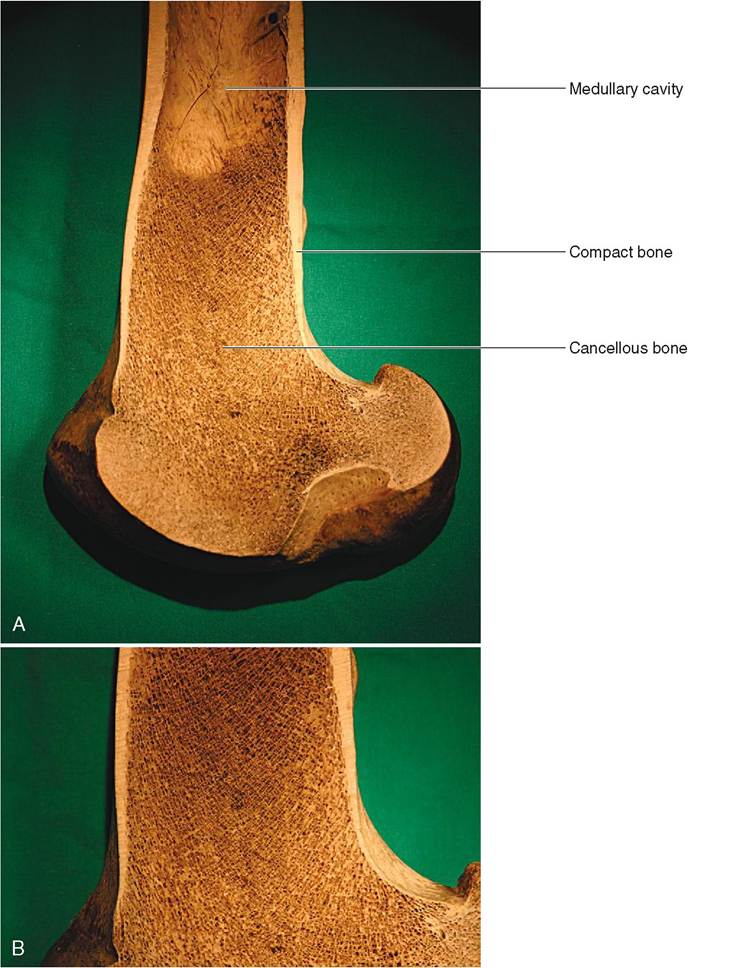
FIGURE 7-1 Bone structure. A, Cut surface of distal end of horse femur. B, Close-up view showing detail of cancellous bone structure.
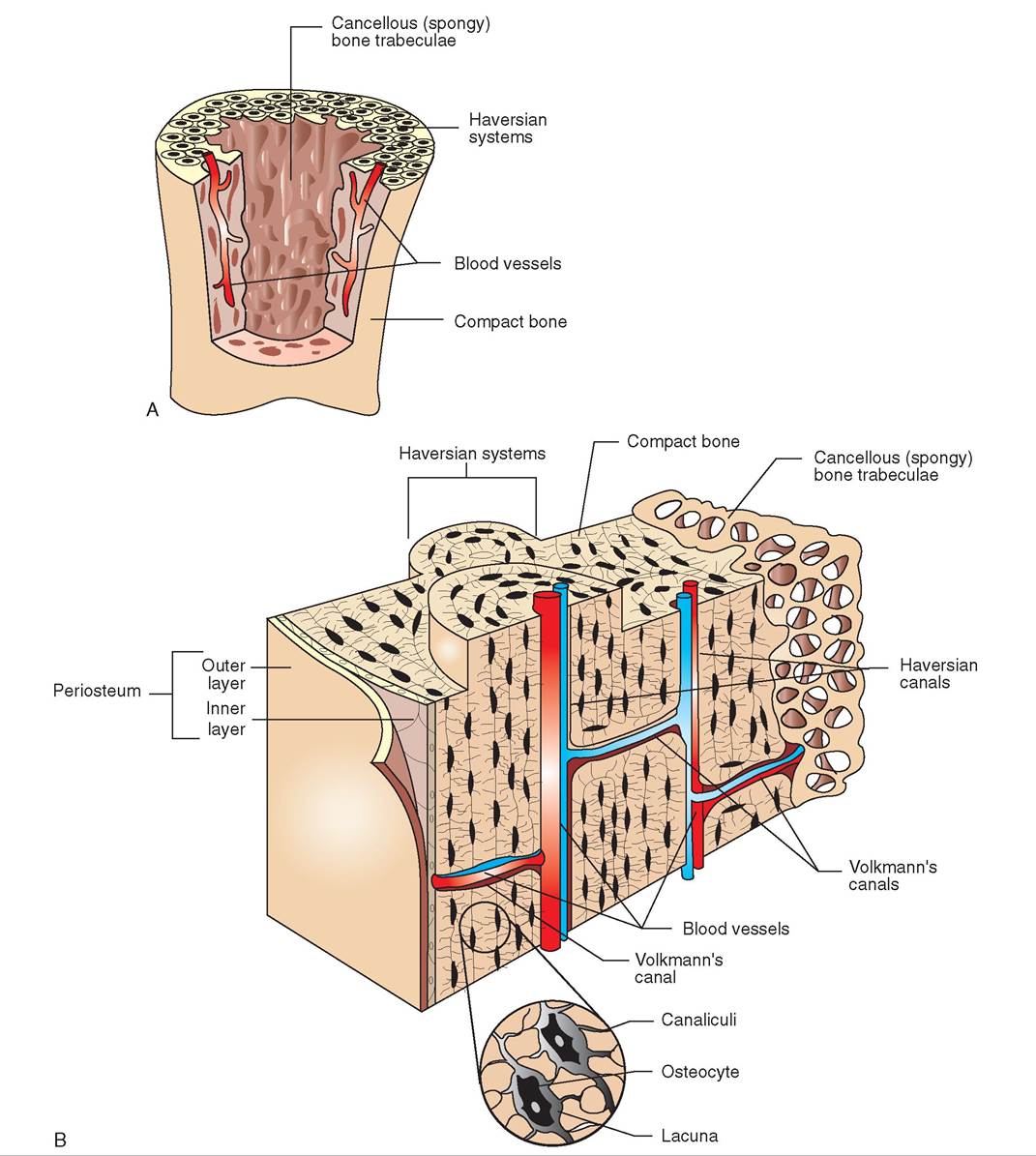
FIGURE 7-2 Structure of compact and cancellous bone. A, Section through the long bone showing outer compact and inner cancellous bone. B, Enlarged view showing components of each type of bone.
multilayered or laminated cylinder composed of concentric layers of ossified bone matrix arranged around a central Haversian canal. The Haversian canal contains blood vessels, lymph vessels, and nerves that supply the osteocytes. The osteocytes are located at the junctions between the layers of bone that make up each Haversian system. In cross section, these layers of bone look like the growth rings of a tree. Tiny channels through the bone, called canaliculi, allow osteocytes to contact each other and exchange nutrients and wastes.
Except for their articular or joint surfaces, the outer surfaces of bones are covered by a membrane called the periosteum. The outer layer of the periosteum is composed of fibrous tissue, and its inner layer contains bone-forming cells (osteoblasts). This inner, bone-forming layer enables bones to increase in diameter. It is also involved in the healing of bone fractures. Another membrane, the endosteum, lines the hollow interior surfaces of bones. The endosteum also contains osteoblasts.
BONE CELLS
Three types of cell that make up bone are osteoblasts, osteocytes, and osteoclasts. Osteoblasts are the cells that form bone. They secrete the matrix of bone and then supply the minerals necessary to harden it. Once the osteoblasts become trapped in the ossified matrix they have created, they are called osteocytes. Talk about painting yourself into a corner! Osteocytes are always ready to revert to their former lives as osteoblasts and form new bone if an injury makes that necessary.
Osteoclasts are like the “evil twins” of osteoblasts; instead of forming bone, they eat it away. Actually, they are not evil at all. Bones are dynamic structures that must be remodeled constantly. Osteoclasts are necessary for remodeling to take place by removing bone from where it is not needed, and osteoblasts form new bone in areas where it is needed. Osteoclasts also allow the body to withdraw calcium from the bones when it is needed to raise the calcium level in the blood.
TEST YOURSELF 7-1
1. Besides supporting the other tissues of the body, what else do bones do?
2. What happens to bones when the level of calcium in the blood falls too low? What happens when it rises too high?
3. What are the three kinds of bone cell? What role does each play in the life of a bone?
4. What is the matrix of bone made of? What makes it so hard?
5. What are the main differences between the structures of cancellous bone and compact bone? Why does the body need these two different types of bone?
BLOOD SUPPLY TO BONE
Most of the blood supply to bones comes from countless tiny blood vessels that penetrate in from the periosteum. The vessels pass through tiny channels in the bone matrix called Volkmann’s canals. Volkmann's canals come in at right angles to the long axis of the bone and at right angles to the Haversian canals. The blood vessels in Volkmann's canals join with the blood vessels in the Haversian canals to bring nutrition to the osteocytes in the Haversian systems.
Large blood vessels, along with lymph vessels and nerves, also enter many large bones—especially long bones— through large channels called nutrient foramina. These large vessels primarily carry blood into and out of the bone marrow. The locations of the larger nutrient foramina on long bones are fairly predictable. Seen from the side on a radiograph (x-ray picture), a nutrient foramen can resemble a crack-type fracture of the bone cortex. This is a good example of why a thorough knowledge of anatomy is necessary to interpret radiographs properly.
BONE FORMATION
Bone is formed in the body by one of two mechanisms: it either grows into and replaces a cartilage model, called endochondral or cartilage bone formation; or it develops from fibrous tissue membranes, called intramembranous or membrane bone formation.
Most bones in the body develop by endochondral bone formation. When bones form by this method, the body first creates a cartilage “template” that is subsequently replaced by bone. Most bones start out as rods of cartilage in the developing fetus. These cartilage rods are prototypes of the bones that will eventually replace them. In long bones, such as the femur or thigh bone, bone begins developing in the shaft or diaphysis of the cartilage rod in what is called the primary growth center. Cartilage is removed gradually as bone is created and the growth center expands. Additional growth centers called secondary growth centers develop in the ends or epiphyses of the bone. By the time an animal is born, most of the cartilage prototypes have been replaced by bone.
Just two areas of a long bone remain as cartilage when an animal is born: these are two plates of cartilage, located between the shaft, or diaphysis, of the bone and the ends, or epiphyses, of the bone. They are called epiphyseal plates or growth plates (Figures 7-3 and 7-4). They are the sites where the creation of new bone allows the long bones to lengthen as the animal grows. In each growth plate, cartilage cells create new cartilage on the outside or epiphyseal surface of the plate, and osteoblasts replace the cartilage on the inside or diaphyseal surface of the plate with bone. By this mechanism, the bone gradually gets longer as the animal grows. When the bone has reached its full size, the epiphyseal plates completely ossify; that is, all of the cartilage is replaced by bone. This stops the growth of the bone. Remodeling continues to take pultace, b the bone is as long as it is going to get.
Intramembranous bone formation occurs only in certain skull bones. Bone forms in the fibrous tissue membranes that cover the brain in the developing fetus. This process creates the flat bones of the cranium, which surround the brain.
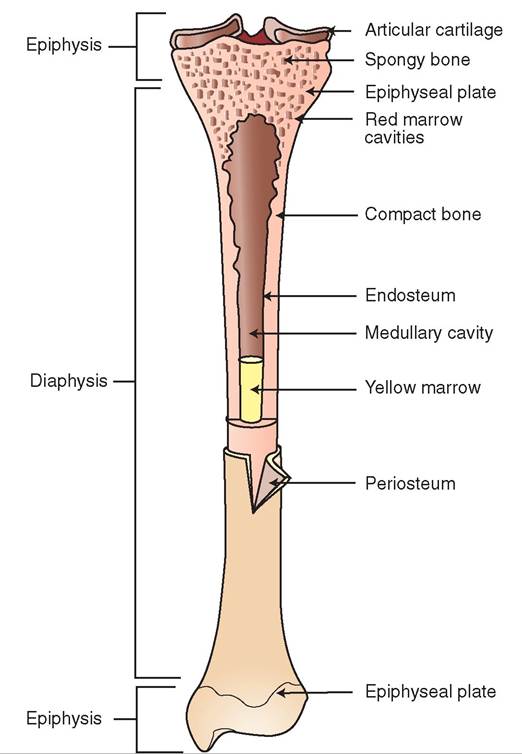
FIGURE 7-3 Long bone. Structure of long bone (tibia).
BONE SHAPES
Bones come in four basic shapes: long, short, flat, and irregular.
LONG BONES
As their name implies, long bones (Figure 7-5, A) are longer than they are wide. Most bones of the limbs are long bones. The basic parts of a long bone are illustrated in Figure 7-3. Each long bone has a proximal epiphysis and a distal epiphysis, which consist primarily of light, cancellous bone covered by a thin layer of compact bone. The main part of a long bone is the diaphysis, which is composed of strong, compact bone. In a young animal, the epiphyseal plates of cartilage found between the epiphyses and the diaphysis are commonly called the growth plates because they are the sites of bone growth that allow long bones to get longer as the animal grows. They are also weak areas of the bone. Fractures through epiphyseal plates, called epiphyseal fractures, are common in young animals. When an animal reaches its full adult size, the epiphyseal plates ossify to become solid bone.
SHORT BONES
Short bones are shaped like small cubes or marshmallows. They consist of a core of spongy bone covered by a thin layer of compact bone. Examples include the carpal (Figure 7-5, B) and tarsal bones.
CLINICAL APPLICATION
Fracture Repair
Bones are among the best healing tissues in the body. When bones are broken, three things are necessary for optimal healing to occur: alignment, immobilization, and time. The fractured ends must be brought close together in reasonable alignment and must be kept from moving apart until healing processes have had adequate time to effect new bone growth. Alignment of the fractured fragments is called setting or reducing the fracture; immobilization is called fixation of the fracture.
External fixation devices such as splints and casts may be used, as can internal devices such as pins, wires, screws, or plates, which must be surgically implanted. The length of time that the fixation device must be kept in place varies with the type and location of the fracture and must take into consideration the physical characteristics of the animal. Factors such as species, age, physical condition, and size of the animal affect the speed of healing. In a small, young animal, the whole process might only take a couple of weeks; in an older or larger animal, it might take several months or more.
Regardless of the type and location of the fracture, the basic healing processes are the same. The large blood supply of bones results in considerable bleeding (hemorrhage) at the fracture site. After the blood begins to clot, forming what is called the fracture hematoma, the bone is gradually infiltrated by healing cells and tissues over the next few weeks and months. Osteoblasts from the area form the healing tissue, called the callus, that gradually bridges the fracture gap. The callus can be felt as a lump at the fracture site, and the size of the callus is an indicator of how much movement has been occurring between the fracture fragments. The less movement, the smaller the callus. Fractures with small calluses generally heal faster, which is usually our treatment goal. Once the callus is fully formed and mineralized, the basic healing of the fracture is complete; however, what occurs after that is very important. Over the next few months, the body slowly remodels the bone at the fracture site according to the mechanical stresses that are placed on it. Ideally, this gradual remodeling will return the bone to its original size, shape, and strength.
FLAT BONES
Flat bones, as their name implies, are relatively thin and flat. Their structure is like a cancellous bone sandwich that consists of two thin plates of compact bone separated by a layer of cancellous bone. Many of the skull bones are flat bones, as are the scapulae, or shoulder blades (Figure 7-5, C), and the pelvic bones.
IRREGULAR BONES
The term irregular bone is the anatomist's version of a miscellaneous category. Irregular bones do not fit into the long, short, or flat categories. They either have characteristics of more than one of the other categories, or they have a truly

FIGURE 7-4 Epiphyseal (growth) plates. Radiograph of pelvis and femurs of a young cat. The epiphyseal plates appear dark because they are made up largely of cartilage, which is relatively transparent to x-rays. Note that the bones appear paler, because they absorb most of the x-rays.
irregular shape. The vertebrae, which are the bones of the spine (Figure 7-5, D), are irregular bones; so are some of the strangely shaped skull bones. Sesamoid bones are also included in this category. Sesamoid bones got their name because early anatomists thought their shapes resembled sesame seeds. (You have to give the early anatomists credit for their creative imaginations.) Sesamoid bones are present in some tendons where they change direction markedly over the surfaces of joints. The kneecap or patella is the largest sesamoid bone in the animal body, but several others are also found. We will discuss some of the clinically important sesamoid bones in the section on the appendicular skeleton.
BONE MARROW
Bone marrow fills the spaces within bones. This includes the spaces between the spicules of cancellous bone and the large spaces within the diaphyses of long bones. Bone marrow comes in two basic types: red bone marrow and yellow bone marrow.
RED BONE MARROW
Red bone marrow is hematopoietic tissue. Hemato refers to blood, and poiesis means to form something. Red bone marrow forms blood cells. It makes up the majority of the bone marrow of young animals but represents only a small portion of the marrow of older animals. In older animals it is confined to a few specific locations, such as the ends of some long bones and the interiors of the pelvic bones and sternum. (See Chapter 12 for more information on blood cell formation.)
YELLOW BONE MARROW
Yellow bone marrow consists primarily of adipose connective tissue, which is better known as fat. It is the most common type of marrow in adult animals. Yellow bone marrow does not produce blood cells, but it can revert to red bone marrow if the body needs to produce larger than normal numbers of blood cells. This might be necessary if, for example, an animal were suffering from chronic, low-level blood loss due to numerous bloodsucking parasites.
COMMON BONE FEATURES
The roles that particular bones play often become clear when their lumps, bumps, grooves, and holes are examined. These

FIGURE 7-5 Bone shap es. A, Long bone. Feline femur. B, Short bones. Equine carpus. C, Flat bone. Canine scapula. D, Irregular bone. Bovine cervical vertebra.
/ TEST YOURSELF 7-2
1. What is the difference between a Haversian canal and a Volkmann's canal?
2. By which mechanism of bone formation do most bones in the animal body develop before birth, and how does the process take place?
3. What is the difference between the primary growth center of a bone and a secondary growth center?
4. Where would you find an epiphyseal plate, and what would you find it doing?
5. What is bone marrow, and what is the difference between the red kind and the yellow kind?
features show us where bones form joints with each other, where muscles attach to move them, where tendons press on their surfaces, and where they are pierced by blood vessels and nerves. We can learn a lot about a bone just by looking at its shape and surface features.
ARTICULAR SURFACES
Articular surfaces are joint surfaces: smooth areas of compact bone where bones come in contact with each other to form joints. Each articular surface is covered by a smooth, thin layer of hyaline cartilage called articular cartilage. The smooth articular surface and its smooth, slightly softer articular cartilage covering help reduce friction and wear in joints.
CONDYLE. A condyle is usually a large, round articular surface. Condyles have, in the creative imagery of anatomists, a somewhat cylindrical shape. The major condyles of the body are located on the distal end of the humerus (see Figure 7-25) and femur (see Figure 7-34, A and B) and on the occipital bone of the skull (see Figure 7-12, C), where the skull joins the spinal column to attach the head to the neck.
HEAD. A head is a somewhat spherical articular surface on the proximal end of a long bone. Heads are found on the proximal end of the humerus, femur, and ribs. The heads of the humerus (see Figure 7-25) and femur (see Figure 7-34, A and B) form the ball portion of the ball-and-socket shoulder and hip joints. The head of a bone is united with the main shaft portion of the bone by an often narrowed region called the neck.
FACET. A facet is a flat articular surface. The joint movement between two facets is a kind of rocking motion. Facets are found on many bones, such as carpal and tarsal bones, vertebrae, and long bones such as the radius and ulna.
Processes
The term process includes all the lumps, bumps, and other projections on a bone. Some processes, such as heads and condyles, have joint-forming functions; they have very smooth surfaces. Other processes are not parts of joints; they have rough, irregular surfaces. These are usually sites where muscles—or more accurately, tendons—attach. In general, the larger the process, the more powerful the muscular pull on that area of the bone. This can help us figure out how and in what directions the bone usually moves and how powerful the movement usually is. This principle is often used by paleontologists to explain the functions that fossilized dinosaur bones probably had when the animals were alive.
Unfortunately, processes are given a variety of names depending on their location. Sometimes they are simply called processes, such as the spinous process of a vertebra (see Figure 7-16). On other bones they have a variety of names, such as trochanter on the femur (see Figure 7-34, A and B), tubercle on the humerus (see Figure 7-25), tuberosity on the ischium (see Figure 7-33, A), spine on the scapula (see Figure 7-24), crest on the tibia (see Figure 7-35), and wing on the atlas (see Figure 7-17). Such is the complex language of anatomy.
HOLES AND DEPRESSED AREAS
FORAMEN. A hole in a bone is called a foramen (plural, foramina). Usually something important, such as a nerve or blood vessel, passes through a foramen in a bone, but there are exceptions. For example, no major structures pass through the two large obturator foramina of the pelvis (see Figure 7-33); they merely exist to lighten the pelvis.
FOSSA. A fossa is a depressed or sunken area on the surface of a bone (see Figure 7-24). Fossae are usually occupied by muscles or tendons. Paleontologists use the fossae of dinosaur bones to infer the sizes and actions of some of the animals' tendons and muscles.
AXIAL SKELETON
The bones of the skeleton can be conveniently divided into two main groups: the bones of the head and trunk and the bones of the limbs. Because the bones of the head and trunk are located along the central axis of the body, they are referred to as the axial skeleton. The limbs are appendages of the trunk and their bones are collectively called the appendicular skeleton. Some animals may have a third category of bones called the visceral skeleton. These are bones formed in the viscera or soft organs, which are discussed in more detail later. Figure 7-6 is a generic, “word” skeleton that shows the locations of the main bones of the axial and appendicular portions of the skeleton. Figures 7-7 and 7-8 show the bones that make up the skeletons of the horse and dog.
The components of the axial skeleton are the skull, the hyoid bone, the spinal column, the ribs, and the sternum. All the bones of the axial skeleton lie on or near the median plane of the body.
SKULL
The skull is the most complex part of the skeleton. At first glance it looks like one big bone—two if you count the mandible—but in most domestic animals it consists of 37 or 38 separate bones. Most of the skull bones are united by jagged, immovable, fibrous joints called sutures. Only the mandible or lower jaw is connected to the rest of the skull by a freely movable synovial joint. Figures 7-9 through 7-12 show the externally visible skull bones of horses, cattle, cats, and dogs.
Author’s suggestion: If you have access to a skull and a live animal of the same species, locate each of the external skull bones on the skull and find the comparable regions on the head of the live animal. Anatomy is a lot more fun and useful if we find the structures we are discussing on live animals.
Because of the skull's complexity, we group the skull bones into regions: the bones of the cranium, the bones of the ear, and the bones of the face. Table 7-1 lists the skull bones in each region.
TABLE 7-1 Skull Bones
EXTERNAL BONES (LANDMARKS) INTERNAL BONES (HIDDEN)
Bones of the Cranium
Frontal bones (2) Ethmoid bone (1)
Interparietal bones (2) Sphenoid bone (1)
Occipital bone (1)
Parietal bones (2)
Temporal bones (2)
Bones of the Ear
None Incus (2)
Malleus (2)
Stapes (2)
Bones of the Face
Incisive bones (2) Palatine bones (2)
Lacrimal bones (2) Pterygoid bones (2)
Mandible (1 or 2) Turbinates (4)
Maxillary bones (2) Vomer bone (1)
Nasal bones (2)
Zygomatic bones (2)
*Bones are listed in alphabetical order.
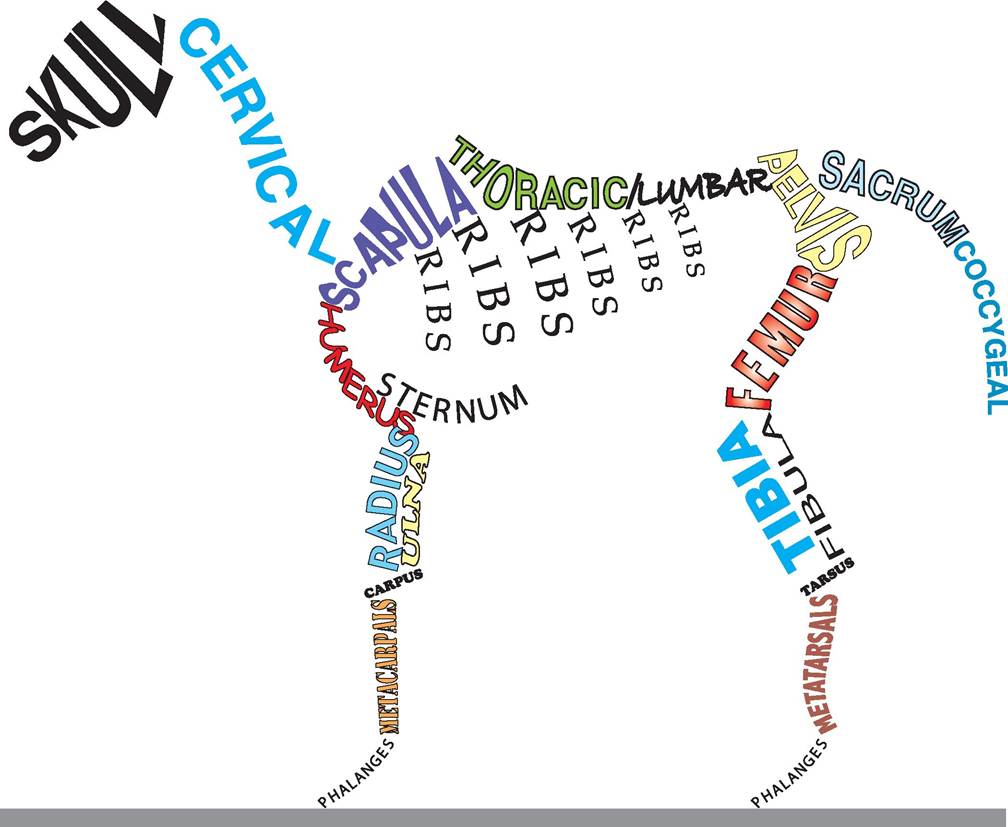
FIGURE 7-6 Word skeleton. The main bones of axial and appendicular portions of the skeleton.
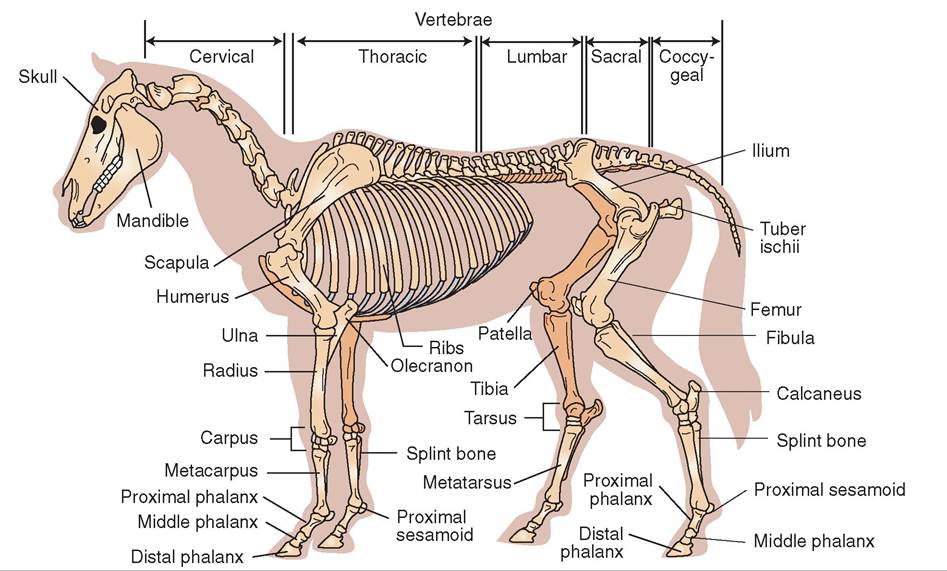
FIGURE 7-7 Equine skeleton. (Modified From McBride DF: Learning veterinary terminology, ed 2, St Louis, 2002, Mosby.)
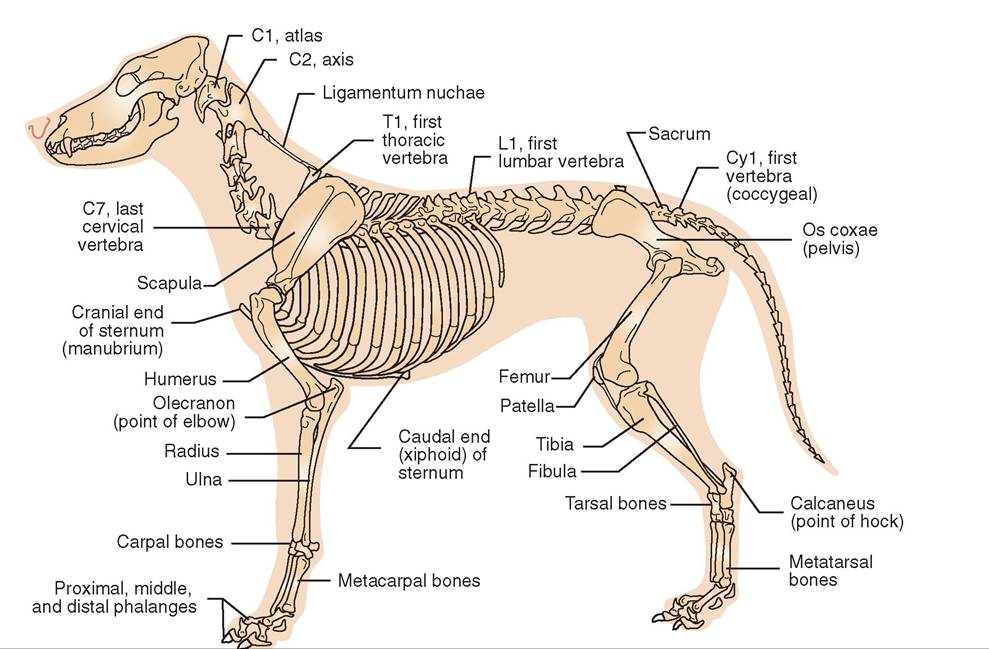
FIGURE 7-8 Canine skeleton.
EXTERNAL BONES OF THE CRANIUM
The cranium is the portion of the skull that surrounds the brain. hi most domestic animal species, 11 bones form the cranium. To make things a little easier, we can divide the bones of the cranium into external and internal bones. Enternal bones are at least partially visible on the surface of an intact skull. We can use them as landmarks to describe tchaetiolnos of features on the heads of living animals. Internal bones are hidden and cannot be seen without disassembling the skull.
Starting at the rear or caudal end of the skull and working our way forward or rostral, the external bones of the cranium are the occipital bone, the interparietal bones, the parietal bones, the temporal bones, and the frontal bones.
OCCIPITAL BONE. The occipital bone is a singe bone that forms the Caudoventral p>oi!ion or base of the skull. It is the most caudal skull bone and is very important because (1) it is where the spinal cord exits the skull and (2) it is the skull bone that articulates (forms a joint) with the first cervical (neck) vertebra. A large hole, the foramen magnum, is in the center of the occipital bone: this is where the spinal cord exits the skull. On either side of the foramen magnum are the occipital condyles: artieular surfaces that join with the first cervical vertebra, called the atlas, to form the atlan- tooccipital joint, which is the joint that connects the head cwki.th the ne As you might imagine, injuries to the occipital rebionues ar se because of its location and the vital structures it encloses. Fortunately, it is well protected by muscles, tendons, and ligaments, so injuries to the occipital bone are rare.
INTERPARIETAL BONES. The interparietal bones are ltownoessmal b located on the dorsal midline between the oncceipital b and the parietal bones. They are usually clearly voiusnibgle in y animals. In older animals, they may fuse toogether int one bone, or they may fuse to the parietal bones and W>me indistinguishable.
PARIETAL BONES. oThe tw parietal bonesofrm the dorsolateral walls of the cranium. They are large and well developed in dogs, cats, and humans but are relatively small irnsehs o and cattle.
TEMPORAL BONES. The tw temporal bonese ar leolocwated b or ventral toitehtael par bones. The temporal ebones ar important for several reasons: they form the lateral fwalls o the cranium, they contain the middle and inner ear structures, and they are the skull bones that form the temporomandibular joints (TMJs) with the mandible (fower jhaew). T ear structures are contained within the temporal bone, and most are not visible from the outside. The only ear structure that is visible from the outside is the external acoustic meatus—the Wiy canal that leads into the middle
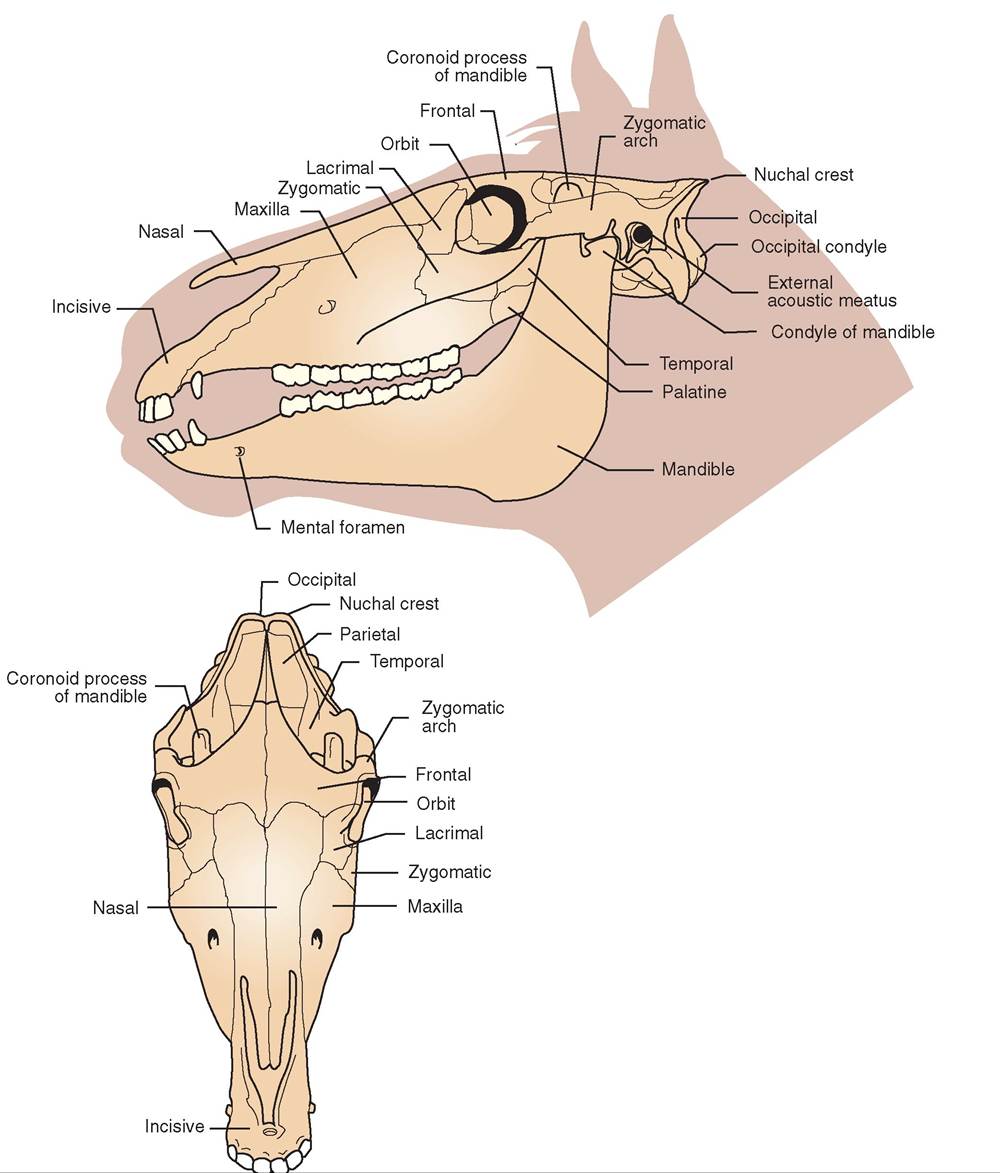
FIGURE 7-9 Skull of the horse.
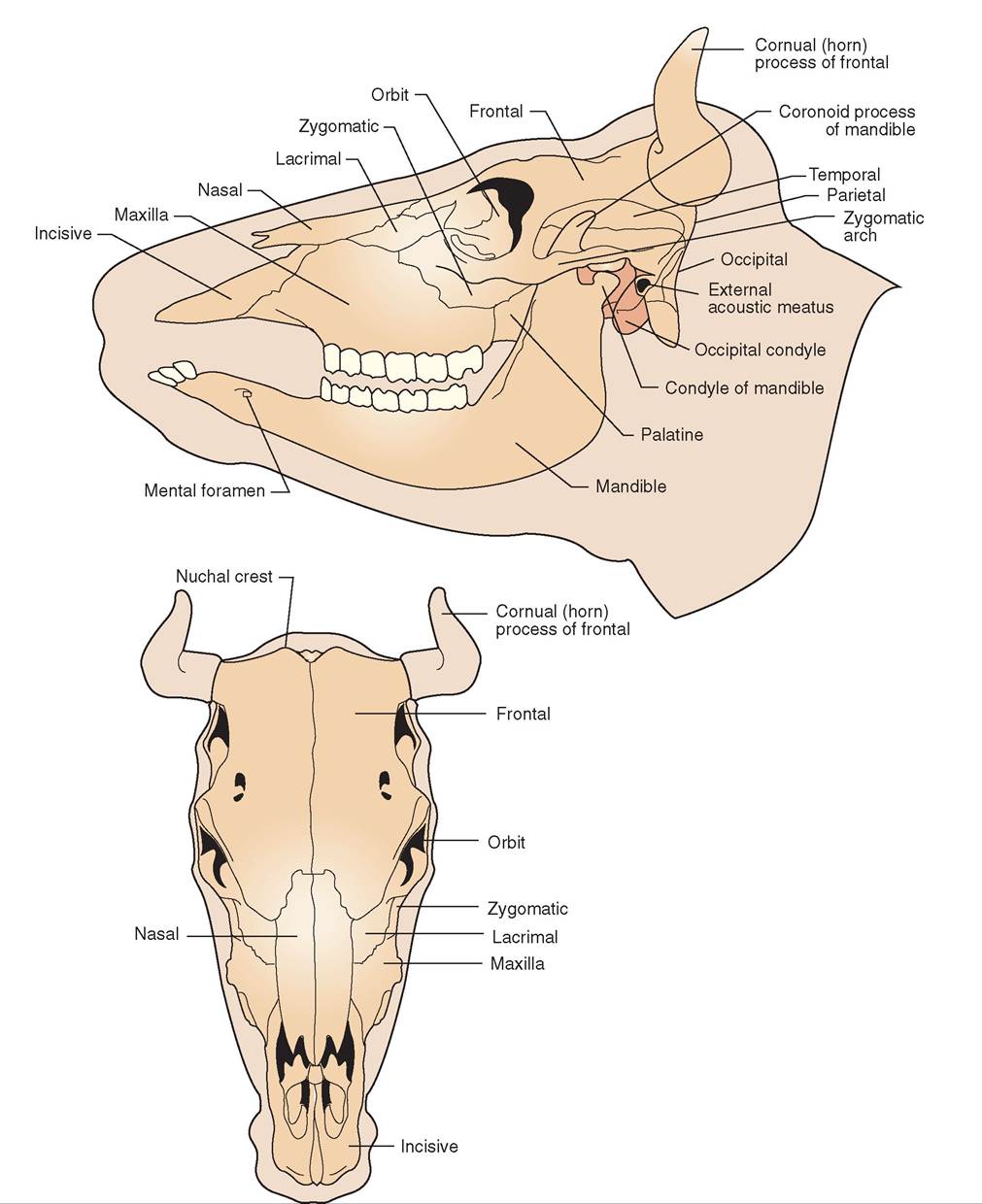
FIGURE 7-10 Skull of the cow.
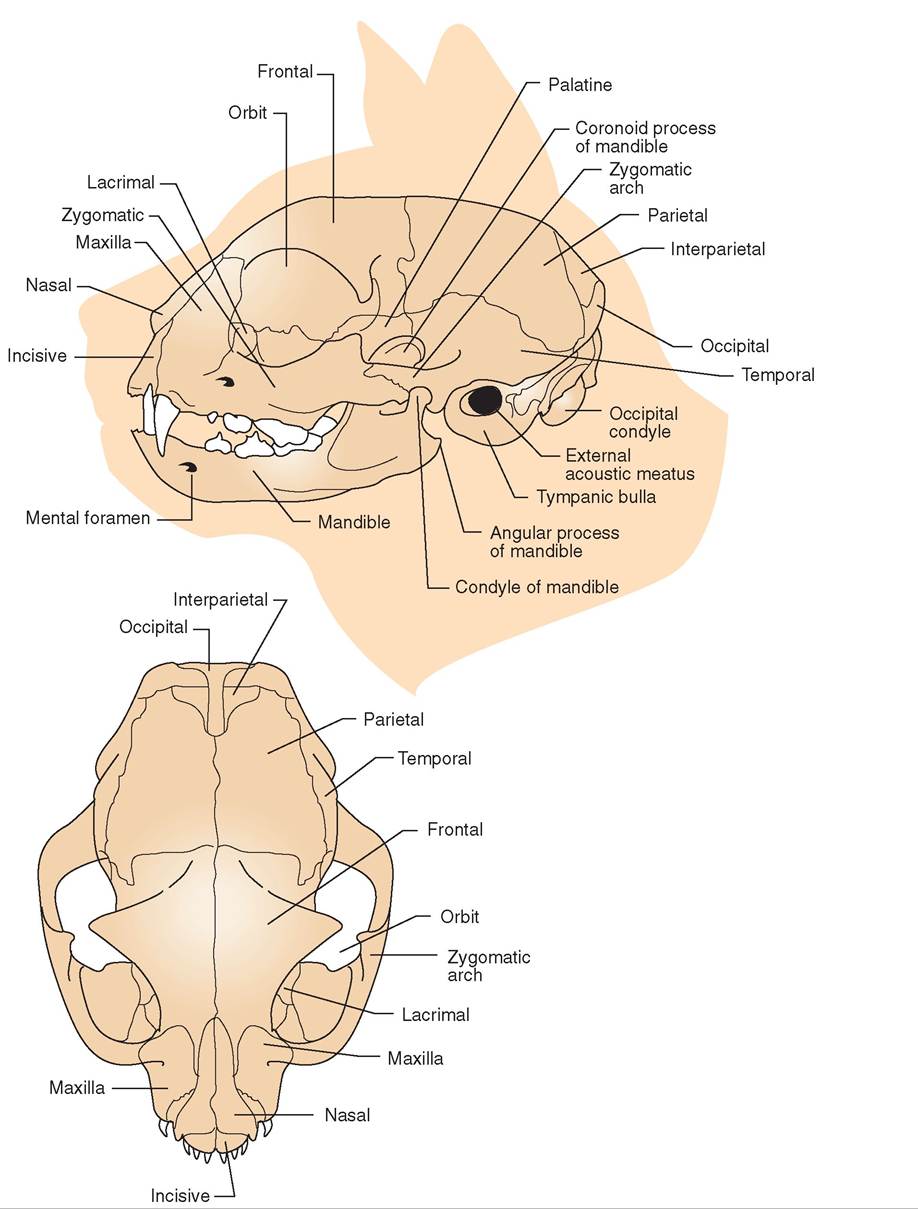
FIGURE 7-11 Skull of the cat.
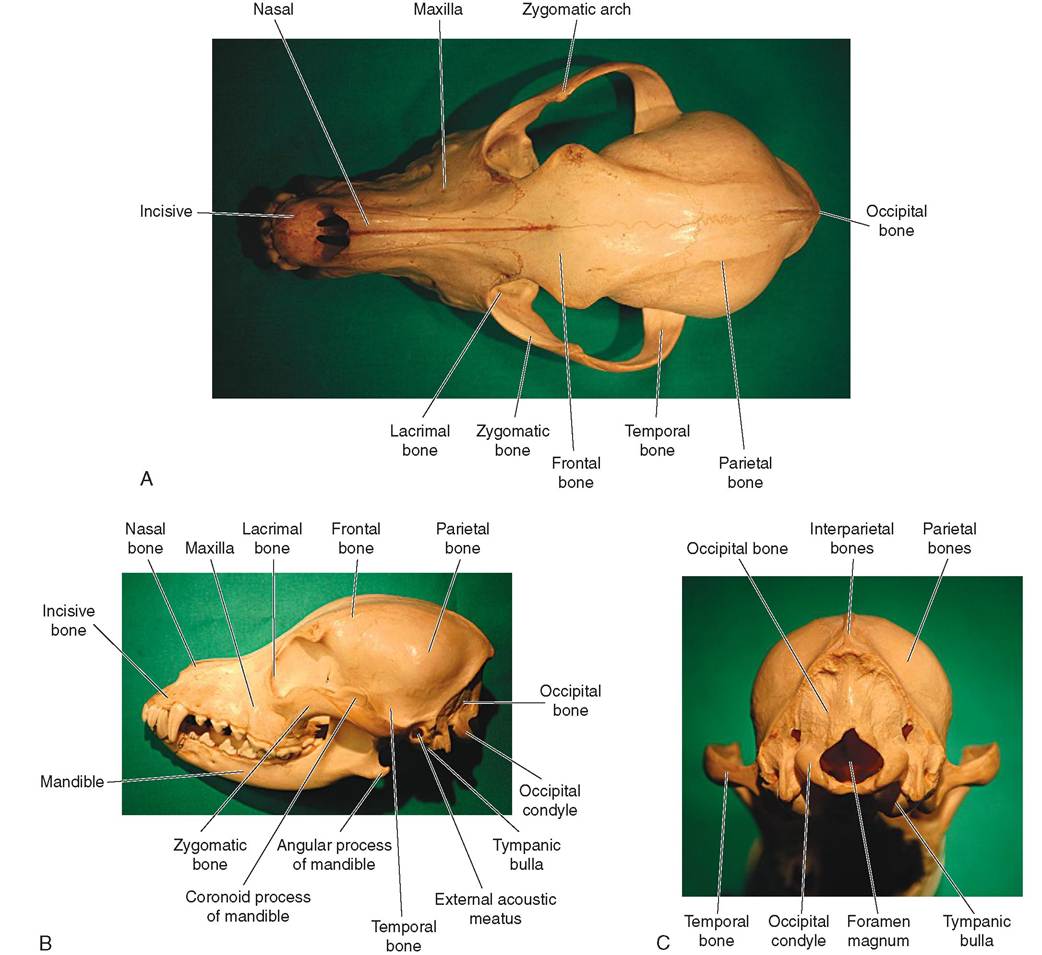
FIGURE 7-12 Skull of the dog. A, Dorsal view. B, Lateral view. C, Caudal view.
and inner ear cavities. In the living animal it contains the external ear canal. By looking into the external acoustic meatus, we can see the middle ear cavity. Ventral to (below) the external acoustic meatus on each side is the concave articular (j^mt) surface that receives the condyle of the mandible to fem the TMJ. These articular surfaces are located on the ventral (bottom) surface of each of the temporal bones.
FRONTAL BONES. The frontal bones form the feehead region of the skull. They are located just rostral to (in front of) the parietal bones, and they form the rostrolateral portion of the crnum and a portion of the orbit, which is the concave socket that holds the eye. A large paranasal sinus, the frontal sinus, is contained within the frontal bone. In horned breeds of cattle, the cornual process of the frontal bone is the horn coournedar which the horn develops. This process is hollow and communicates with the frontal sinus. When adult cattle are dnhd^^d, the cornual processes are sawed off and we can ilogowhontk r d into the frontal sinus. This is a really good reason to dehorn cattle when they are young, before the horn vbeuds ha united with the frontal bones.
INTERNAL BONES OF THE CRANIUM
The tw hidden bones of the cranium are the sphenoid bone and the more rostral ethmoid bone.
SPHENOID BONE. A singe sphenoid bone fems the ventral part (bottom) of the cranium and contains a depression—the pituitary fossa—that houses the pituitary gland, which is an important endocrine (hormone-producing) gland. The sphenoid bone is located just rostral to (in front of) the occipital bone. If removed from the skull and examined, the sphenoid bone looks like a bat with its wings and legs extended. The sphenoid bone of most animals contains a paranasal sinus called the sphenoidal sinus.
ETHMOID BONE. The ethmoid bone is a single bone located just rostral to (in front of) the sphenoid bone. It contains the sievelike cribriform plate, through which the many branches of the olfactory (sense of smell) nerve pass from the upper portion of the nasal cavity to the olfactory bulbs of the brain. Horses and humans have a small paranasal sinus, the ethmoidal sinus, in the ethmoid bone.
BONES OF THE EAR
The three tiny but very important pairs of ear bones are hidden away in the middle ear. Known as the ossicles, these bones are—starting from the outside—the malleus or hammer, the incus or anvil, and the stapes or stirrup. Their function is to transmit vibrations from the tympanic membrane (eardrum) across the middle ear cavity to an inner ear structure called the cochlea. In the cochlea, receptor cells for hearing convert the vibrations to nerve impulses that are interpreted by the brain as sound. The characteristics and functions of the ossicles are covered more completely in Chapter 10.
EXTERNAL BONES OF THE FACE
The bones of the face make up the rest of the skull. We can also divide them into external, landmark bones and internal, hidden bones.
Starting at the rostral (front) end of the skull and working caudally (toward the rear), the external bones of the face are the incisive bones, the nasal bones, the maxillary bones, the lacrimal bones, the zygomatic bones, and the mandible.
INCISIVE BONES. The two incisive bones, sometimes called the premaxillary bones, are the most rostral (forward) skull bones. In all common domestic animals except ruminants such as cattle, sheep, and goats, the incisive bones house the upper incisor teeth. Our ruminant friends do not have upper incisor teeth; they have a hard dental pad instead.
NASAL BONES. The two nasal bones form the bridge of the nose, which is the dorsal or upper part of the nasal cavity. Considerable variety is seen in the relative size and shape of the nasal bones, depending on the species and breed of animal. The length of the animal's face is the main influence on the nasal bones. In animals with long faces, such as horses, and dolichocephalic or long-faced dog breeds, such as collies, the nasal bones are long and thin. In animals with short faces, such as cats and brachycephalic or short-faced breeds of dogs, such as Pekingese, the nasal bones are short and more triangular.
MAXILLARY BONES. The two maxillary bones make up most of the upper jaw. (The incisive bones make up the rest.) The maxillary bones house the upper canine teeth, all of the upper cheek teeth (premolars and molars), and the maxillary sinuses. Along with the palatine bones, the maxillary bones form the hard palate, which is the bony separation between the mouth and the nasal cavity that we call the roof of the mouth. The maxillary bones form the rostral (forward) portion of the hard palate, and the palatine bones form the caudal (rear) part.
LACRIMAL BONES. The lacrimal bones are two small bones that form part of the medial portion of the orbit of the eye. A space within each lacrimal bone houses the lacrimal sac, which is part of the tear drainage system of the eye.
ZYGOMATIC BONES. The two zygomatic bones are also known as the malar bones. They form a portion of the orbit of the eye and join with a process from the temporal bones to form the zygomatic arches on either side of the skull. The caudal-facing (rear-facing) temporal process of the zygomatic bone joins with the rostral-facing (forwardfacing) zygomatic process of the temporal bone (do you sense a pattern here?) to form the zygomatic arch on each side. The zygomatic arches are easily palpable, bony landmarks below and behind the eyes that form the widest part of the skull in dogs and cats.
MANDIBLE. The mandible is the lower j aw (Figure 7-13). It houses all the lower teeth and is the only movable skull bone. It forms the TMJ with the temporal bone on each side. In some species, such as dogs, cats, and cattle, the two sides of the mandible are separate bones united by a cartilaginous joint, the mandibular symphysis, at their rostral (front) ends. Because the symphysis is the weakest part of the mandible, separation of the bones can occur at that site from blunt-force trauma to the face. This is called a mandibular symphyseal fracture. It is the most common type of
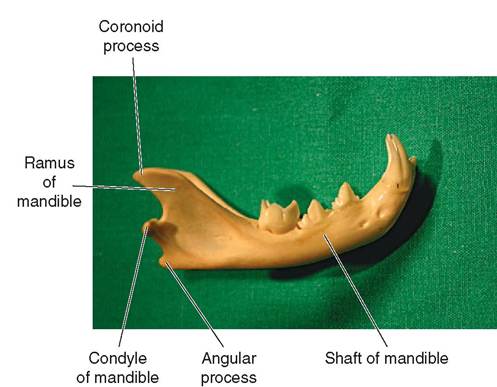
FIGURE 7-13 Cat mandible. Right lateral view.
mandibular fracture in dogs and cats. Fortunately, it usually is easy to repair. In adult horses and swine, the two halves of the mandible fuse together into one solid bone.
The two main regions of the mandible are the shaft and the ramus. The shaft of the mandible is the horizontal portion that houses all the teeth. At its caudal end is the vertical portion of the mandible, called the ramus of the mandible. This is where the powerful j aw muscles attach and where the articular condyles that form the TMJs with the temporal bones are located.
INTERNAL BONES OF THE FACE
The internal bones of the face are the palatine bones, the pterygoid bones, the vomer bone, and the turbinates.
PALATINE BONES. The two palatine bones make up the caudal portion of the hard palate (the bony part of the roof of the mouth), which separates the mouth from the nasal cavity. The rest of the hard palate (the rostral portion) is made up of part of the maxillary bones.
PTERYGOID BONES. The two small pterygoid bones support part of the lateral walls of the pharynx (throat).
VOMER BONE. The single vomer bone is located on the midline of the skull and forms part of the nasal septum, which is the central “wall” between the left and right nasal passages.
TURBINATES. The turbinates are also called the nasal conchae (Figure 7-14). They are four thin, scroll-like bones that fill most of the space in the nasal cavity. Each side has a dorsal and a ventral turbinate. The turbinates are covered by the moist, very vascular soft tissue lining of the nasal passages. The scroll-like shape of the turbinates forces air inhaled through the nose around many twists and turns as it passes through the nasal cavity. This helps warm and humidify the air and also helps trap any tiny particles of

Rostral portion of turbinate removed to show interior detail
FIGURE 7-14 Turbinates. Rostral view of deer skull.
inhaled foreign material in the moist surface of the nasal epithelium. This process helps condition the inhaled air before it reaches the delicate lungs. (I’ll bet you didn't know you had air conditioners in your nose.)
TEST YOURSELF 7-3
1. Name the skull bones that make up each of these groups:
External bones of the cranium
Internal bones of the cranium
Bones of the ear
External bones of the face
Internal bones of the face
2. In which skull bones are each of the following structures found?
Cribriform plate
External acoustic meatus
Foramen magnum Frontal sinus
Lacrimal sac
Lower teeth
Pituitary fossa
Upper incisor teeth Upper cheek teeth
3. Which would likely be a greater threat to an animal's well-being: a fracture of the mandible or a fracture of the occipital bone? Why?
HYOID BONE
The hyoid bone, also called the hyoid apparatus (Figure 7-15), looks somewhat like the letter H with its two legs bent back to form a U-shaped structure. It is located high in the neck, just above the larynx, between the caudal ends of the mandible. It supports the base of the tongue, the pharynx, and the larynx and helps the animal swallow. It is usually referred to as a single bone, but it is composed of several individual portions united by cartilage. It is attached to the temporal bone by two small rods of cartilage. Some authors include the hyoid bone as a skull bone for convenience, but its location and attachments seem to indicate that it is a separate bone of the axial skeleton.
SPINAL COLUMN
The spinal column, also called the vertebral column, is made up of a series of individual irregular bones called vertebrae (singular, vertebra) that extend from the skull to the tip of the tail. The spinal column is divided into five regions: cervical (neck), thoracic (chest), lumbar (abdomen), sacral (pelvis), and coccygeal (tail). Most vertebrae do not have individual names. Instead, they are numbered within each region from cranial to caudal. A shorthand way of referring to particular vertebrae uses the abbreviation for the region— C for cervical, T for thoracic, L for lumbar, S for sacral, and Cy for coccygeal—followed by the number of the vertebra within that region, starting at the cranial end. For example, C5 is the fifth cervical vertebra, and L2 is the second lumbar vertebra. The usual numbers of vertebrae within each region,
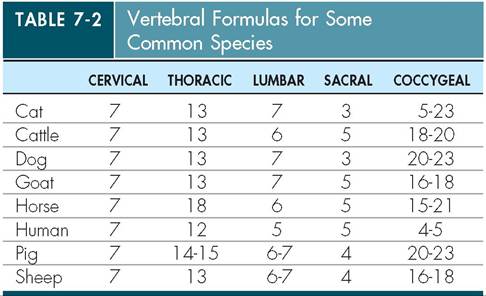
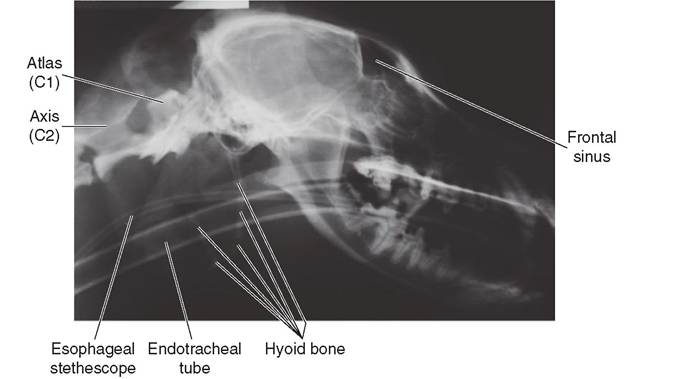
FIGURE 7-15 Hyoid bone. Radiograph of dog skull.
called vertebral formulas, are listed in Table 7-2 for some common species.
VERTEBRAL CHARACTERISTICS
A typical vertebra consists of a body, an arch—sometimes called the neural arch—and a group of processes (Fignre 7-16). The body of a vertebra is the main, ventral portion of the bone. It is the strongest, most massive portion. The bodies of adjacent vertebrae are separated by the intervertebral discs, made of fibrocartilage, which act as little shock-absorbers.
Dorsal to the body of a vertebra is the hollow arch. When the arches of all the vertebrae are lined up, they form a long, flexible tunnel called the spinal canal, which houses and protects the spinal cord.
Vertebrae usually have some combination of three kinds of processes. The single, dorsally projecting spinous process and the two laterally projecting transverse processes vary in size among vertebrae. These act as sites for muscle attachment and provide leverage to move the spine and trunk. The articular processes are located on the cranial and caudal ends of the vertebral arches and help form the joints between adjacent vertebrae. Each intervertebral joint allows only very limited movement but, taken as a whole, the entire spinal column has considerable flexibility. Cats demonstrate this flexibility by the strange positions they can get their bodies
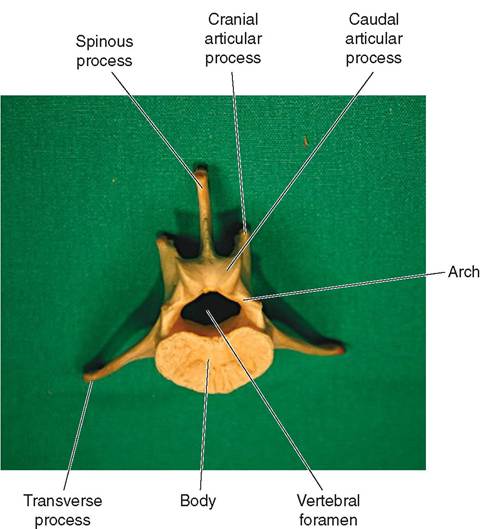
FIGURE 7-16 Basic anatomy of a vertebra. Caudal view of dog L4 vertebra.
into, especially while lying in a sunbeam. Author’s note: As I was writing this section, one of our cats, Bogie, was doing a spinal flexibility demonstration beside my computer by lying on his back with his front end facing one direction and his back end facing the other.
CERVICAL VERTEBRAE
The cervical vertebrae are in the neck region. A quick look at Table 7-2 will show that seven cervical vertebrae are found in all common domestic animals and in humans. Actually, nearly all mammals have seven cervical vertebrae. Even the long-necked giraffe has only seven v-e-r-y l-o-n-g cervical vertebrae. This is the only group of vertebrae that has a constant number across most species.
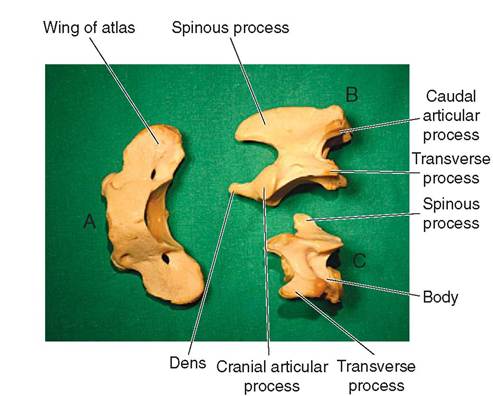
FIGURE 7-17 Cervical vertebrae of the dog. A, Atlas (C1), dorsal view. B, Axis (C2), lateral view. C, Fourth cervical vertebra (C4), lateral view.
The first two cervical vertebrae are somewhat unusual in shape and have specific names (Figure 7-17). The first, C1, is called the atlas because, like the mythical figure Atlas who holds up the world, this vertebra “holds up” the head. The atlas has two large, winglike transverse processes called the wings of the atlas that can be palpated (felt) just behind the skulls of most animals. The next time you are around a dog or cat, feel the wings of the atlas right behind the skull. The atlas is unique in that it has no vertebral body: it consists only of a bony ring that the spinal cord passes through with the two wings sticking out laterally. Just caudal to the atlas is the second cervical vertebra, C2, which is called the axis. Its most prominent features are its large, bladelike spinous process that projects up dorsally and the pegike dens that fits into the caudal end of the atlas to help form the atlantoaxial joint. The rest of the cervical vertebrae are fairly normal looking and are numbered like the rest of the vertebrae.
CLINICAL APPLICATION
Fun Facts About Human Intervertebral Discs
Because we walk upright, gravity compresses our intervertebral discs slightly when we are up and moving around during the day. At night when we lie down and sleep, the compression stops and the discs expand back to their original size. The compression and expansion of each individual disc are very slight but, when combined, the variation in the total length of the spine is measurable. As a result, we are tallest in the morning—by as much as an inch! We proceed to get shorter throughout the day. For astronauts living in the microgravity environment of space, the result is even more impressive: after just a few days in space, their spines can expand up to 2 inches or more. Some astronauts report back pain during the first few days in space because this spinal expansion stretches the muscles around the spinal column. This dramatic increase in height is temporary, and astronauts quickly return to their normal, terrestrial height when they return to earth.
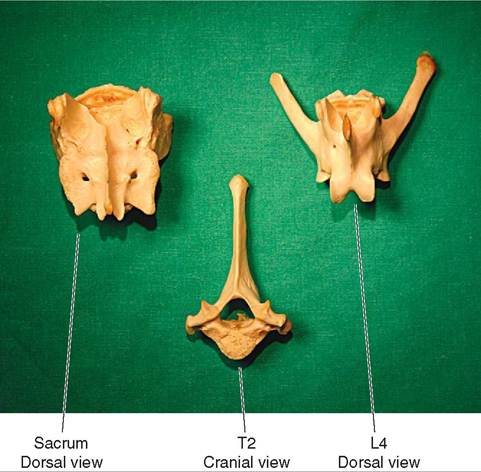
FIGURE 7-1 8 Thoracic, lumbar, and sacral vertebrae of the dog.
THORACIC VERTEBRAE
The thoracic vertebrae are located dorsal to the thorax. Their number varies among species and can even vary within a species. Usually, however, the number of thoracic vertebrae is the same as the number of pairs of ribs the animal has. The most characteristic features of thoracic vertebrae are their tall, spinous processes and their lateral articular facets, which form joints with the heads of the ribs (Figure 7-18).
CLINICAL APPLICATION
Intervertebral Disc Disease
Normal intervertebral discs have a soft, cushioning center of gelatinous material called the nucleus pulposus, which is surrounded by tough fibrocartilage. On their sides and bottoms, intervertebral discs are surrounded by tough ligaments and dense muscles that support the spinal column and join the vertebrae together. The only thing dorsal to these discs is the spinal cord, which is tightly encased in the bony spinal canal.
Intervertebral disc disease results when one or more discs degenerate. When a disc becomes diseased, normal mechanical forces on the spine often result in degenerated disc material being squeezed out. The ligaments and muscles on the sides and bottom of the disc prevent the material from moving in any of those directions, so the only direction it can protrude is dorsally, up into the spinal canal, where it presses on the spinal cord. Because the spinal cord is surrounded by bone, it has no way to escape the pressure when the protruded disc material compresses it, which causes the common clinical signs of intervertebral disc disease: pain, numbness, weakness, and paralysis.
Intervertebral disc disease can occur in any species of animal but is seen most often in dogs, particularly long- backed breeds such as Dachshunds. It usually occurs in one
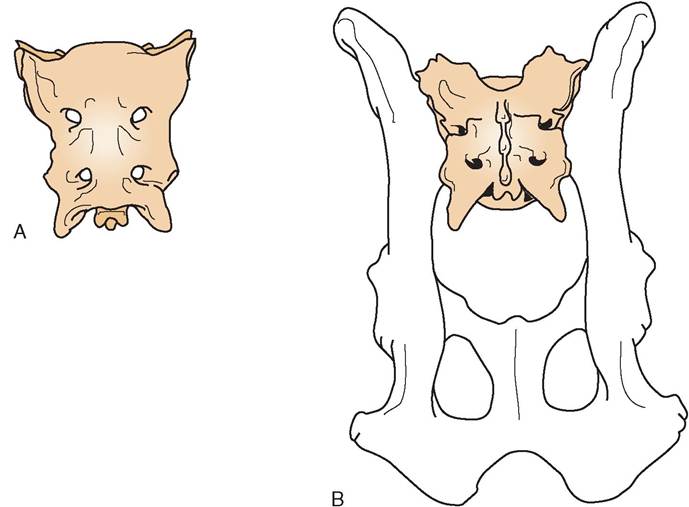
FIGURE 7-19 Can ine sacrum. A, Ventral view. B, Dorsal view.
CLINICAL APPLICATION—cont'd
of two sites: the cervical region or the thoracolumbar region. Cervical disc disease usually causes severe pain. The neck muscles go into spasm, and the animal holds its head and body very rigidly and does not like being touched. Disc disease in the mid back usually causes weakness, sometimes called paresis, and numbness of the hind legs that can progress to complete paralysis. Treatment options include exercise restriction or cage rest, medical treatment with drug therapy to reduce pressure on the spinal cord, and surgery to decompress the spinal cord directly. The prognosis depends on the location, extent, and duration of the damage to the spinal cord.
Author’s note: I once had a Dachshund patient with thoracolumbar disc disease whose rear legs remained paralyzed despite weeks of intensive treatment. The dog’s owners reluctantly decided to euthanize him and have him buried in a nearby pet cemetery. The afternoon before the scheduled euthanasia, a representative from the pet cemetery came to our hospital to measure the dog for a coffin. This apparently got his attention, because the next morning, when the time came to do the regrettable deed, we noticed some slight rearleg movement. We canceled the euthanasia and the dog went on to make a full recovery. Apparently, he had only needed the proper motivation.
LUMBAR VERTEBRAE
The lumbar vertebrae are dorsal to the abdominal region. Like the thoracic vertebrae, their number varies among species and even within a species. The lumbar vertebrae are the most massive-looking bones of the spinal column. Their
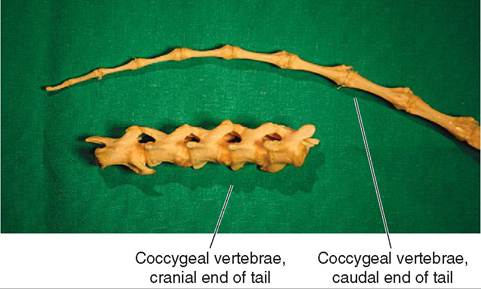
FIGURE 7-20 Coccygeal vertebrae of the dog.
bodies are large and bulky, because they have to support all the weight of the abdominal organs and structures without the aid of the ribs, which help support the thoracic contents (see Figure 7-18).
SACRAL VERTEBRAE
The sacral vertebrae are unique in that they fuse to form a single, solid structure called the sacrum (Figures 7-18 and 7-19). The number of vertebrae fused in the sacrum varies among species (see Table 7-2). The sacrum is located dorsal to the pelvic region and forms a joint with the pelvis on each side in what is called the sacroiliac joint.
COCCYGEAL VERTEBRAE
The coccygeal vertebrae are the bones of the tail (Figure 7-20). Their number varies greatly not just between species but even within a species. Their appearance also varies quite
a bit, even within an individual animal. The first few coccygeal vertebrae have the usual characteristics of vertebrae, such as bodies, arches, and processes, but nearer the tip of the tail they are reduced to simple little rods of bone. In humans the coccygeal vertebrae are fused into a single bone called the coccyx or, more commonly, the tailbone.
CLINICAL APPLICATION
Wobbler Syndrome
Wobbler syndrome occurs most commonly in certain breeds of dog—Basset Hounds, Borzois, Doberman Pinschers, and Great Danes—and horses, particularly Thoroughbreds. It results from a narrowing of the spinal canal in the cervical region that compresses the spinal cord. This narrowing can result from physical abnormalities (malformations) of cervical vertebrae or improper joints (malarticulations) between them. The precise cause is not known, but inherited factors and nutritional factors seem to be involved. Clinical signs typically develop slowly and gradually, starting with weakness and incoordination, called ataxia. The name wobbler syndrome comes from the wobbly, uncoordinated gait seen in affected animals, and the disease can progress to complete paralysis. Medical treatments may be attempted to decrease the compression of the spinal cord, but surgery is often necessary. The prognosis for recovery is usually guarded at best.
CLINICAL APPLICATION
Bony rib
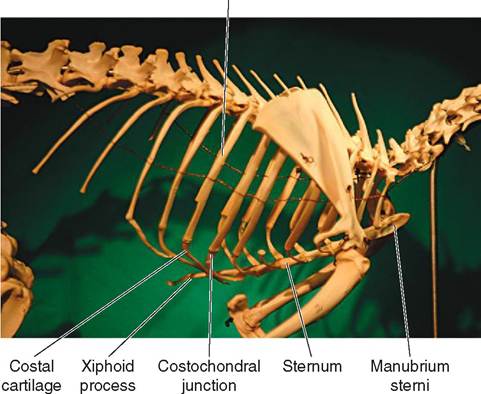
FIGURE 7-21 Rabbit ribs and sternum.
The Anticlinal Vertebra
In most veterinary practices, dogs are the animal species in which intervertebral disc disease is most commonly seen. As a result, veterinary personnel take a lot of spinal radiographs of dogs. The bones of the spine can be confusing to look at. When trying to identify the precise location of a lesion, the anticlinal vertebra is a convenient landmark. The eleventh thoracic vertebra, T11, is called anticlinal because its spinous process, unlike those of the surrounding vertebrae, projects straight up. The spinous processes of the first 10 thoracic vertebrae all recline caudally, and the last two, T12 and T13, incline cranially, so T11 looks out of place and is easily identified. The anticlinal vertebra in cats is also T11, but in horses it is T16; in cattle and sheep it is T13, and it is T10 in swine.
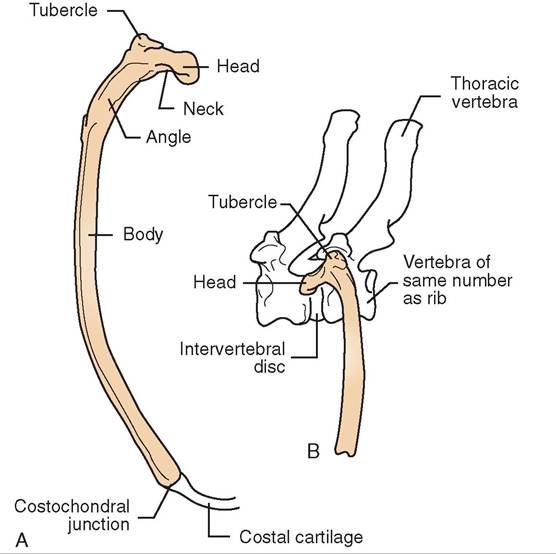
FIGURE 7-22 Canine rib. A, Caudal view of rib. B, Lateral view of rib articulating with vertebrae.
RIBS
The ribs are flat bones that form the lateral walls of the thorax (Figures 7-21 to 7-23). The number of pairs of ribs usually equals the number of thoracic vertebrae the animal has. At their dorsal ends, the heads of the ribs form joints with the thoracic vertebrae. These freely movable joints help the process of ventilation, which is the movement of air in and out of the lungs. By swivelling the ribs at their dorsal ends, the ventilatory muscles can enlarge or diminish the size of the thorax, depending on the direction of the muscle contraction.
The ventral ends of the ribs are a lot more variable. Each rib actually has two parts: a dorsal part, made of bone, and a ventral part, made of cartilage. The term for rib is costal, so the cartilaginous part is called the costal cartilage, and its junction with the bony part is called the costochondral junction. The costal cartilages either join the sternum directly or join the costal cartilage ahead of them (see Figure 7-23). The ribs whose cartilages join the sternum are called sternal ribs and make up the cranial part of the thorax. The
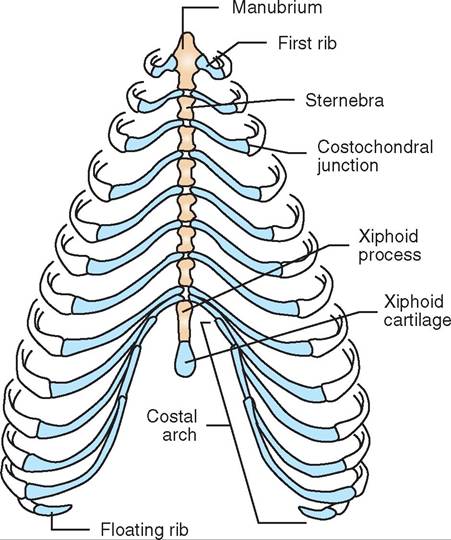
FIGURE 7-23 Can ine costal cartilages and sternum. Ventral view.
ones that join the adjacent costal cartilage are called asternal ribs and make up the caudal part of the thorax. The cartilages of the last ribs, the two on each side, may not join anything at all; they may just end in the muscles of the thoracic wall. These unattached ribs are called floating ribs.
STERNUM
The sternum, also called the breastbone, forms the floor of the thorax. It is made up of a series of rodlike bones called sternebrae (see Figures 7-21 and 7-23). Only the first and last sternebrae are named and used as landmarks. The others are numbered from cranial to caudal. The first, most cranial
TEST YOURSELF 7-4
1. Which groups of vertebrae make up the spinal column dorsal to the following regions?
Abdomen
Neck
Pelvis
Tail
Thorax
2. What are the three kinds of processes found on vertebrae and what are their characteristics?
3.Where in a vertebra is the spinal cord located?
4. What are the names of the first two cervical vertebrae and what are their distinguishing characteristics?
5. What is the difference between a sternal rib, an asternal rib, and a floating rib?
6.What is the manubrium?
7.What is the xiphoid?
| TABLE 7-3 Bones of the Limbs (Proximal to Distal) | |
| THORACIC LIMB | PELVIC LIMB |
| Scapula | Pelvis |
| Ilium | |
| Ischium | |
| Pubis | |
| Humerus | Femur |
| Radius | Tibia |
| Ulna | Fibula |
| Carpal bones (carpus) | Tarsal bones (tarsus) |
| Metacarpal bones | Metatarsal bones |
| Phalanges | Phalanges |
sternebra is called the manubrium or manubrium sterni. The last, most caudal sternebra is called the xiphoid or xiphoid process. A piece of cartilage, known as the xiphoid cartilage, extends caudally from the xiphoid process and is easily felt in most animals at the caudal end of the sternum.
APPENDICULAR SKELETON
The appendicular skeleton is made up of the bones of the main appendages of the animal body, that is, the limbs. In anatomical terms, the front leg is the thoracic limb, and the hind leg is the pelvic limb IMbIe 7-3).
Author’s suggestion: Find the bones discussed in the following section on skeletons, and identify the bones in living animals. Sometimes they are not where we think they are.
THORACIC LIMB
In common domestic animals, the thoracic limb has no direct, bony connection with the axial skeleton. This is in contrast with primates, such as humans, that have a collarbone or clavicle that joins the scapula with the sternum. Instead, the forelegs support the weight of the body by a slinglike arrangement of muscles and tendons. Some animals, such as dogs and cats, may have a small remnant of the clavicle embedded in a tendon in the shoulder region, but it does not articulate with the axial skeleton and is of little or no clinical significance.
SCAPULA
The scapula (Figure 7-24) is the most proximal bone of the thoracic limb. It is a flat, somewhat triangular bone with a prominent, longitudinal ridge on its lateral surface, which is referred to as the spine of the scapula. At its distal end, it forms the socket portion of the ball-and-socket shoulder joint. This fairly shallow, concave articular surface is called the glenoid cavity. It is connected with the main body of the scapula by a narrowed area known as the neck.
HUMERUS
The humerus (Figure 7-25) is the long bone of the upper arm or brachium. On its proximal end is the ball portion of
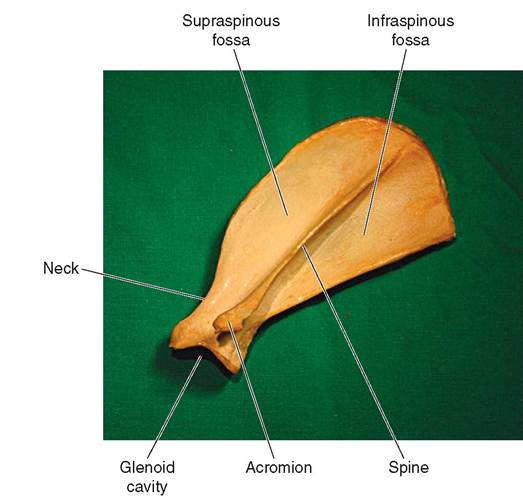
FIGURE 7-24 Canine left scapula. Lateral view.
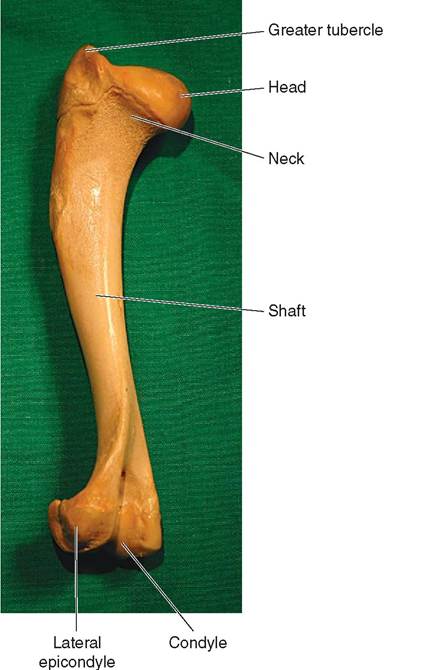
FIGURE 7-25 Canine left humerus. Lateral view.
the ball-and-socket shoulder joint: the head of the humerus, which is joined to the shaft by a neck. Opposite the head on the proximal end are some large processes called tubercles, where the powerful shoulder muscles attach. The largest one is called the greater tubercle. The shaft of the humerus extends down to the distal end that forms the elbow joint with the radius and ulna. The distal articular surfaces of the humerus are referred to collectively as the condyle. To be more precise, the medial articular surface is the trochlea, which articulates with the ulna, and the lateral one is the capitulum, which articulates with the radius. Just above the condyle on the back surface of the humerus is a deep indentation called the olecranon fossa, which will be discussed later with the ulna. The nonarticular “knobs” on the medial and lateral surfaces of the condyle are called the medial and lateral epicondyles. These are easily palpated and can be used as landmarks on living animals.
Author’s note: Note the spelling of humerus. It looks a lot like the word humorous, which might lead you to believe that it is the “funny bone.” It is not. Actually, the “funny bone” is not a bone at all, but the ulnar nerve, which is located fairly superficially as it passes through the elbow joint region. When we bump it, we experience that distinctive, funny-bone tingle.
ULNA
Two bones form the forearm or antebrachium: the ulna and the radius. The ulna (Figure 7-26) forms a major portion of the elbow joint with the distal end of the humerus. Several interesting structures can be found on its proximal end. The large olecranon process forms the point of the elbow, where the tendon of the powerful triceps brachii muscle attaches. The trochlear notch is a half-moon shaped, concave articular surface that wraps around part of the humeral condyle to help make the elbow joint a tight, secure joint. At the proximal end of the trochlear notch is a beak-shaped process known as the anconeal process. When the elbow is extended into a straightened position, the anconeal process tucks into the olecranon fossa on the distal end of the humerus. At the distal end of the trochlear notch are the medial and lateral coronoid processes. They are located on the medial and lateral ends of the horizontal, concave facet on the proximal end of the ulna that articulates with the radius. The shaft of the ulna extends down to the carpus in all common species except for the horse. Its shape parallels the straight or curved shape of the radius. In the horse the ulna consists only of the proximal portion, which joins with the radius about midshaft. In other species, the distal end of the ulna consists of a pointed process, called the styloid process,t itchualtataers with the carpus.
RADIUS
The radius (Figure 7-27) is the main weight-bearing bone of the antebrachium. On its proximal end, the radius has facets that articulate with the proximal end of the ulna and a large, concave articular surface, where it joins with the distal end of the humerus. The shaft of the radius varies from fairly straight in cats and cattle to somewhat bowed in dogs, horses, and swine. At its distal end, the radius has several
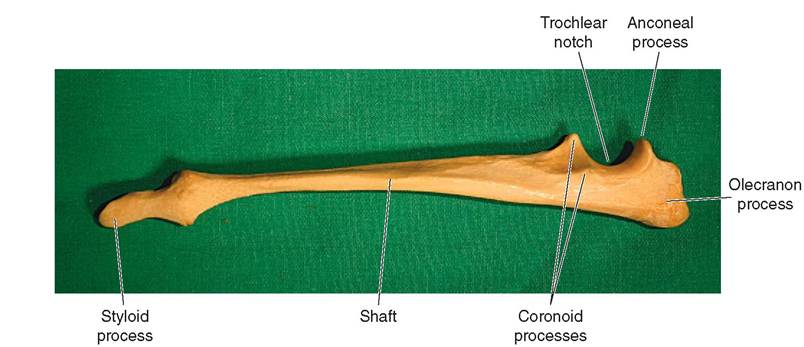
FIGURE 7-26 Canine left ulna. Lateral view.

CLINICAL APPLICATION
Ununited Anconeal Process in the Dog
The anconeal process of the ulna develops from a secondary growth center that is separate from the primary growth center in the ulnar shaft. In dogs it normally fuses to the rest of the ulna by about 6 months of age. Sometimes, particularly in large and giant dog breeds, mechanical forces in the elbow break down the fusing tissues and prevent the anconeal process from uniting with the rest of the bone. This results in elbow joint instability that damages the joint surfaces and leads to secondary osteoarthritis, and the affected animal gradually becomes lame. The diagnosis can be confirmed by taking a lateral radiograph of the elbow in the flexed position, which will show the unattached process. Treatment usually involves surgical removal of the ununited anconeal process.
facets and a pointed process called the styloid process that articulate with the carpus.
CARPAL BONES
The carpus (Figure 7-28) consists of two rows of carpal bones. The two rows of bones are arranged parallel to each other in a proximal row and a distal row. In humans the carpus is our wrist, but in horses it is referred to as the knee. Considerable variety is seen among the species in the precise makeup of the carpus, but a basic naming convention holds true across species lines. The bones of the proximal row are given individual names. All common species have a radial carpal bone, an ulnar carpal bone, and, protruding backward on the lateral side of the carpus, an accessory carpal bone. Some species also have an intermediate carpal bone. The bones of the distal row of the carpus are given numbers instead of names, starting at the medial side and working laterally. Figure 7-29 shows the distal bones of the horse leg from the carpus down, and Figure 7-30 shows comparable bones of the dog.
METACARPAL BONES
The metacarpal bones extend distally from the distal row of carpal bones to the proximal phalanges of the digits. In humans, metacarpal bones are the bones of our hands. They extend from our wrists down to our first knuckles and are numbered from medial to lateral. The metacarpal of our thumb is metacarpal I, and that of our little finger is metacarpal V. The flexibility of the joint between the metacarpal bone of our thumb and our wrist makes our thumb apposable with the rest of our hand, which gives us a great grasping advantage over many other animal species. In other animals the appearance of the metacarpal bones is determined largely by what kind of foot the animal has.
Horses have a simple foot consisting of only one digit or toe. Therefore they have only one large metacarpal bone

FIGURE 7-28 Equine left carpus. Cranial view.
supporting their weight in each leg (see Figure 7-29). This large metacarpal bone is commonly referred to as the cannon bone. Actually, a horse has three metacarpal bones in each leg: one large metacarpal and two smaller vestigial metacarpal bones known as the splint bones. According to fossil evidence, ancestors of the modern horse had multiple toes. Over many millennia, those animals became increasingly specialized for speed and eventually developed into the modern horse that walks on only one toe. Figure 7-31 shows a modern horse digit alongside the fossilized distal leg bones of Parahippus leonensis, a small, three-toed horse considered to be an ancestor of the modern horse. The large metacarpal bone of the horse is assumed to be what is left of metacarpal III, and the smaller splint bones on either side of it are designated as metacarpals II and IV. There is no remnant of the first or fifth digits.
The splint bones do not support any weight and only extend one-half to two-thirds of the way down the shaft of the large metacarpal. They do, however, sometimes cause problems for horses, because they can suffer various kinds of injury including fractures. Most commonly, though, the ligaments joining them to the large metacarpal bone become inflamed. This condition is referred to as splints, and it can be quite painful for the horse. Treatment ranges from rest to surgery.
The feet of cattle are like horse feet split in two (Figure 7-32). Cattle walk on two toes. Accordingly, they have two metacarpal bones, bones III and IV, but these are
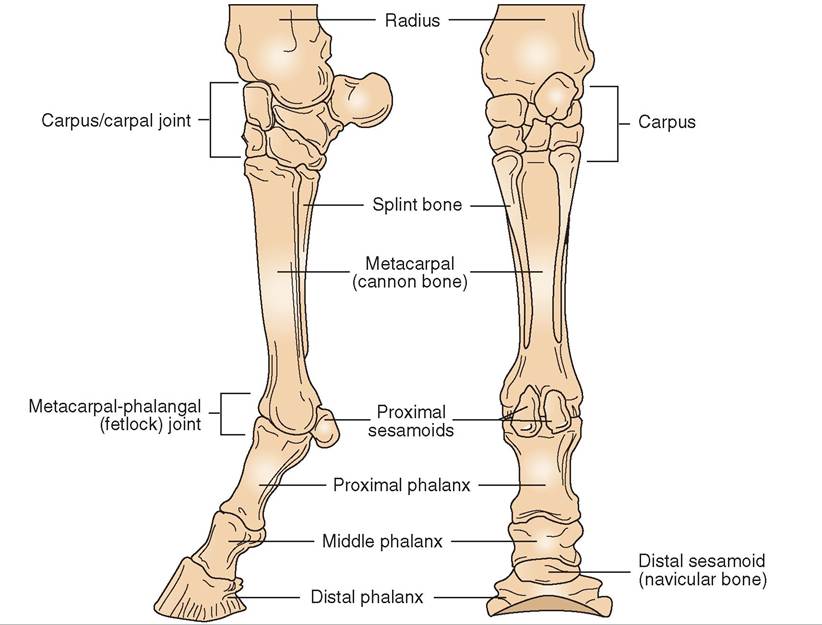
FIGURE 7-29 Distal limb bones of equine right front leg. (Modified from McBride DF: Learning veterinary terminology, ed 2, St Louis, 2002, Mosby.)
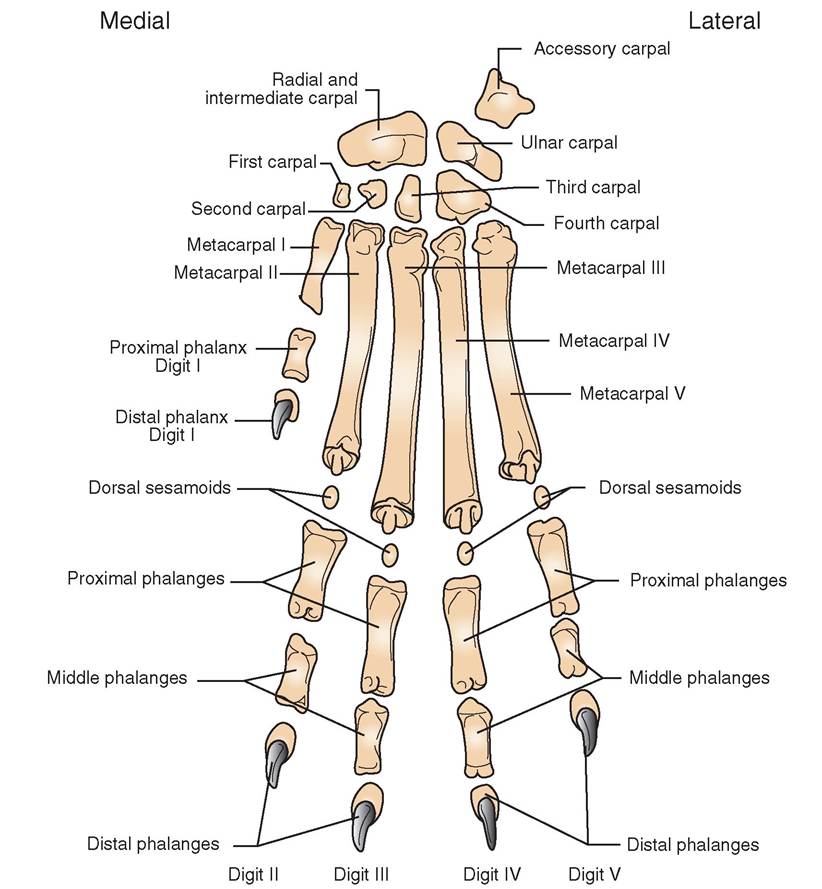
FIGURE 7-30 Distal limb bones of canine left front leg.
fused into a single bone. A longitudinal groove running down the metacarpal bone clearly shows its two-bone origin, however.
Dogs and cats have paws that are structurally similar to our hands. They typically have five digits or toes making up their front paws. Figure 7-30 shows the bones of the canine forepaw. The bones of the cat are quite similar. Note that, like us, dogs have five metacarpal bones that are numbered from medial to lateral. Metacarpal I is part of what is usually termed the dewclaw, and the others are numbered II, III, IV, and V Metacarpal V is the lateral- most metacarpal.
Phalanges
We need to clarify and differentiate a couple of terms used to describe animal feet. The anatomical term digit means the same as the common term toe (and, in our case, finger). Each digit is made up of two or three bones called phalanges (singular, phalanx). So the phalanges are the individual bones that make up the digits.
Horses have one digit on each limb. It is composed of three phalanges and three sesamoid bones. The phalanges are named according to their position: they are the proximal phalanx, commonly called the long pastern bone; the middle phalanx, commonly called the short pastern bone; and the distal phalanx, commonly known as the coffin bone. In some older anatomy texts, the phalanges are numbered from proximal to distal instead of being named. This method works okay for horses, since they have only one digit, but it becomes confusing in animals with multiple digits that are already numbered. For clarity, we ignore that particular identification scheme.
The digit of the horse also contains two proximal sesamoid bones and one distal sesamoid bone. You will recall
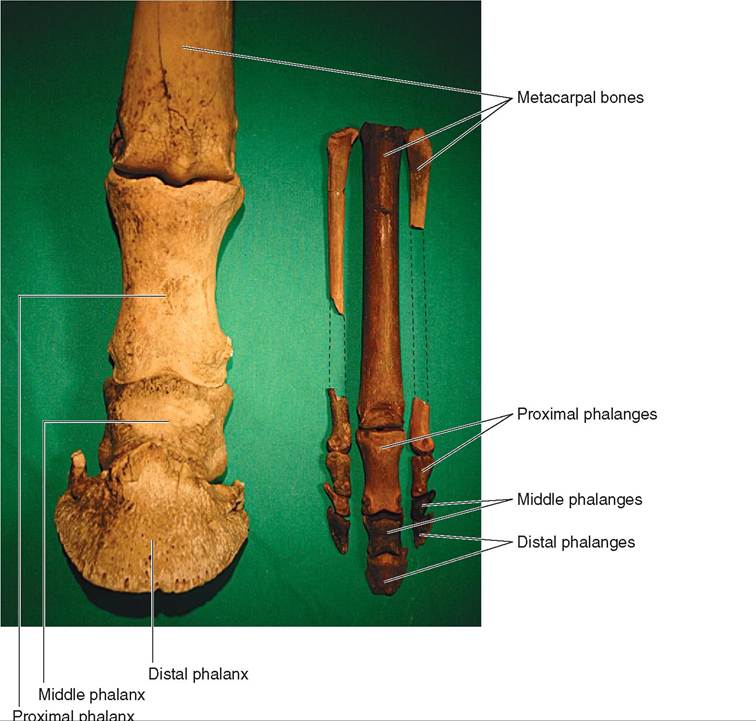
FIGURE 7-31 Digit of horse (left) compared with fossilized distal leg of Parahippus Ieonensis (right). Parahippus was a primitive, three-toed horse that lived over 13 million years ago. Considered to be an ancestor of the modern horse, it was about the size of a large dog. It had a large, central hoof that bore most of its weight and two “side hooves.” All that is left of those extra toes in the modern horse are the splint bones. (Parahippus fossils from the author's collection.)
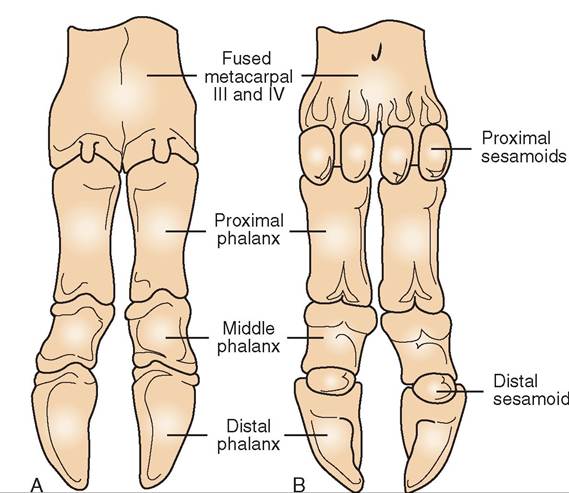
FIGURE 7-32 Digit of the cow. A, Dorsal (front/top) view. B, Palmar/plantar (rear/bottom) view.
that sesamoid bones are irregular bones found in some tendons where they change direction suddenly over the surfaces of joints. They act as bearings over the joint surfaces to allow muscles to exert powerful forces on the bones without the tendons wearing out from the constant, back- and-forth movement over the joint. The sesamoid bones of the horse digit are important in allowing the spindly little horse foot to support and propel the large horse body around. The two proximal sesamoid bones are located behind the joint between the large metacarpal bone and the proximal phalanx in the large digital flexor tendons. This joint is commonly referred to as the fetlock joint. The distal sesamoid bone is located deep in the hoof behind the joint between the middle and distal phalanges, where the digital flexor tendon attaches to the distal phalanx. Some imaginative early anatomist thought this distal sesamoid bone resembled a tiny boat, which led to its common name: the navicular bone. Proximal and distal sesamoid bones are found in both the front and hind digits of the horse.
Cattle have four digits on each limb: the third and fourth support the body weight, and the second and fifth are vestiges. The two vestigial digits are called the dewclaws, and each contains one or two small bones that do not articulate with the rest of the bones of the foot. Figure 7-32 shows the structure of the weight-bearing bones of the bovine foot. As you can see, each digit has a proximal, middle, and distal phalanx, as well as two proximal sesamoid bones and one distal sesamoid bone.
Dog and cat forepaws contain bones that are very similar to our fingers. Figure 7-30 clearly shows that digit I—the dewclaw—contains only two bones: a proximal phalanx and a distal phalanx. This is similar to our thumb, which contains only two phalanges. Digits II to V each contain three bones: a proximal phalanx, a middle phalanx, and a distal phalanx. Each distal phalanx contains a pointed ungual process that is surrounded by the claw. The digits of dogs and cats also contain tiny sesamoid bones, but they are rarely of clinical significance except in performance dogs, such as racing Greyhounds, and heavy large-breed dogs, such as St. Bernards. These heavy breeds can fracture sesamoid bones by jumping.
TEST YOURSELF 7-5
1. Name the bones of the thoracic limb from proximal to distal.
2. What is the anatomical name for the shoulder blade?
3. What are the brachium and the antebrachium, and which bones form them?
4. On which bone is the olecranon process found? What is its purpose?
5. What are the anatomical names for the cannon bone and the splint bones in a horse?
6. Which digit is the dewclaw on the front leg of a dog?
7. What is the common name for the distal sesamoid bone in the horse?
CLINICAL APPLICATION
Navicular Disease in the Horse
Because of its location deep in the hoof, where powerful forces are placed on it with each step, the navicular or distal sesamoid bone is subject to chronic wear and injury. This is particularly true in the front feet because of their more upright position. When the bone starts to undergo chronic, painful degeneration, the condition is called navicular disease.
Navicular disease is not one specific disease with one specific cause; it is a complex syndrome that involves many factors, including damage to the bone itself, damage to the bone’s blood supply, and damage to surrounding structures, such as bursas, tendons, and ligaments. The net result is a lameness that begins intermittently and progressively gets worse. The animal tries to shift weight off the heel area of the affected foot where the damaged navicular bone is located. This changes the animal’s gait and can lead to secondary problems.
The signs of navicular disease can sometimes be managed, but the condition is usually not curable. Some pain relief sometimes can be provided with corrective hoof trimming and shoeing and with drug therapy.
PELVIC LIMB
Unlike the thoracic limb, the pelvic limb is directly connected to the axial skeleton through the sacroiliac joint that unites the ilium of the pelvis with the sacrum of the spinal column. This eliminates the need for large, slinglike muscles in the rear quarters to support the weight of the caudal part of the body and allows room for all the reproductive, urinary, and digestive system structures that lie between and behind the rear legs.
PELVIS
The pelvis is sometimes referred to anatomically as the os coxae. It starts developing as three separate bones on each side that eventually fuse into a solid structure. The two halves of the pelvis are joined ventrally by a cartilaginous joint called the pelvic symphysis. The pelvis joins the axial skeleton dorsally at the left and right sacroiliac joints.
Even though the bones that make up the pelvis fuse together, the names of the individual bones are still used to designate the main regions of the pelvis: the ilium, the ischium, and the pubis (Figure 7-33).
ILIUM. The ilium is the cranial-most bone of the pelvis. When we put our hands on our hips, the ilium on each side is the bone each hand rests on. It projects up in a dorsocra- nial direction and is the bone that forms the sacroiliac joints with the sacrum. In dogs and cats, the smooth “wing” of the ilium projects forward and is easily felt as a landmark in living animals. In cattle and horses, the cranial end of the ilium on each side has large medial and lateral processes. The tuber sacrale projects medially and joins with the sacrum to
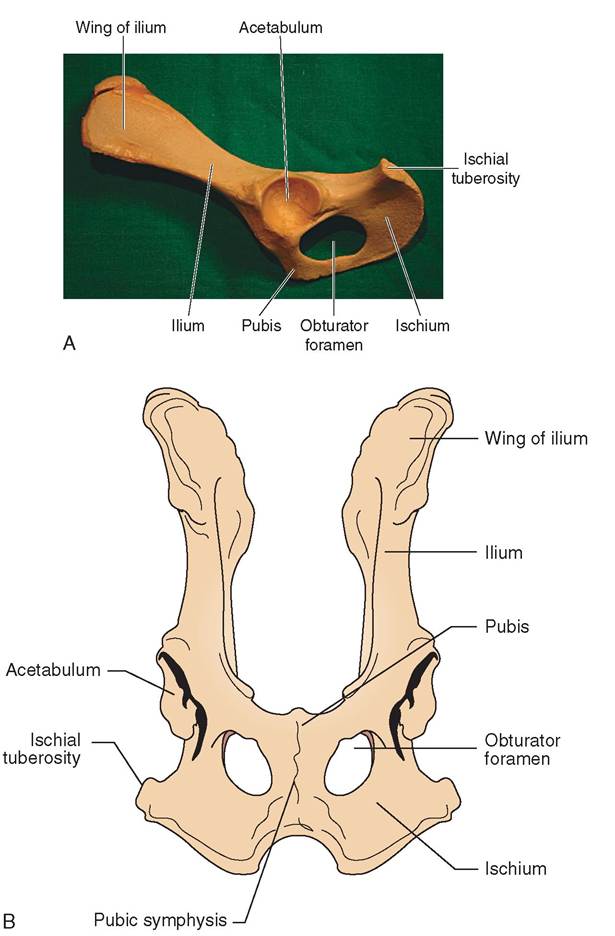
FIGURE 7-33 Can ine pelvis. A, Lateral view. B, Ventral view.
form the sacroiliac joint. The tuber coxae projects laterally and is called the point of the hip.
ISCHIUM. The ischium is the caudal-most pelvic bone. If you are sitting down as you are reading this, you are sitting on your ischia. The main, rear-projecting process of the ischium is the ischial tuberosity.
PUBIS. The pubis is the smallest of the three pelvic bones. It is located medially and forms the cranial portion of the pelvic floor, while the ischium forms the caudal part.
The three bones that make up each side of the pelvis come together at the socket portion of the ball-and-socket hip joint in a concave area called the acetabulum. The acetabulum is a deep socket that tightly encloses the head of the femur to form the relatively stable hip joint.
Located on either side of the pelvic symphysis are two large holes known as the obturator foramina. Usually a big hole in a bone would allow something large and important to pass through it; however, that is not the case here. Nothing but a few small blood vessels and nerves pass through the obturator foramina. Their primary function is to lighten the pelvis. Drag racers use this same principle when they drill numerous holes in many of the chassis components of their race cars to lighten them.
FEMUR
The femur (Figure 7-34) is the long bone of the thigh. On its proximal end is the ball portion of the ball-and-socket hip joint, called the head of the femur, which is attached to the shaft by a neck. In contrast to the large, round head of the humerus, the head of the femur is smaller and more
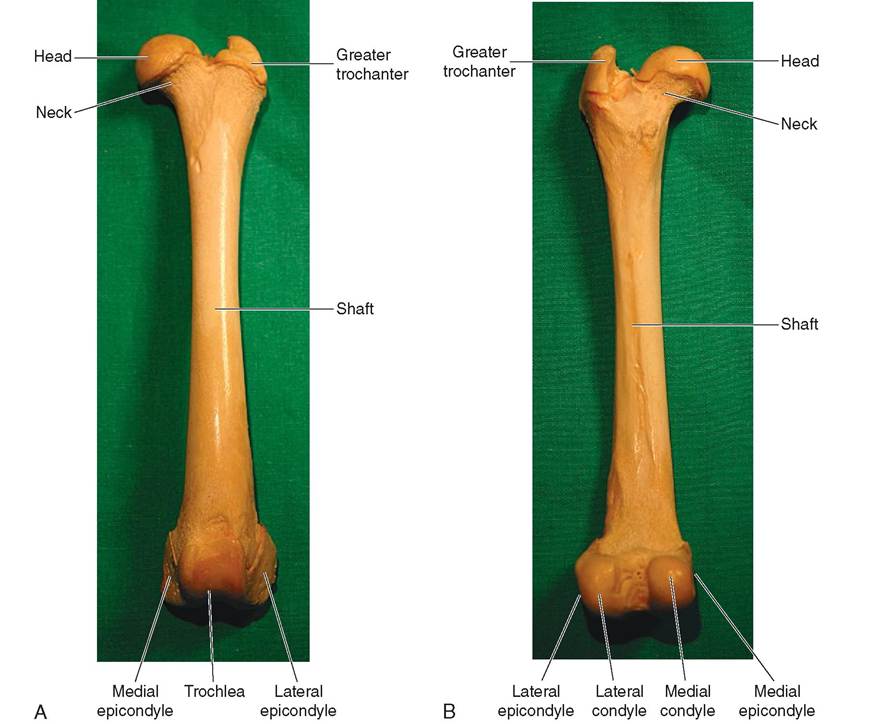
FIGURE 7-34 Can ine left femur. A, Cranial view. B, Caudal view.
spherical. It normally fits very deeply and securely into the acetabulum of the pelvis.
Opposite the head on the proximal end are some large processes, the trochanters, where strong hip and thigh muscles attach. The largest one is called the greater trochanter. The shaft of the femur is fairly straight and extends down to the distal end to form the stifle joint, which is equivalent to our knee, with the patella and tibia. The three articular surfaces on the distal end of the femur are the two condyles caudally and the trochlea cranially. The medial and lateral condyles articulate with the condyles on the proximal end of the tibia. The trochlea is a smooth articular groove in which the patella rides. Like the humerus, the femur has nonarticu- lar “knobs” medial and lateral to the condyles; these are called the medial and lateral epicondyles, and they are easily palpated and can be used as landmarks on living animals.
PATELLA
The patella or kneecap is the largest sesamoid bone in the body. It is formed in the distal tendon of the large quadriceps femoris muscle on the cranial aspect of the stifle joint. It helps protect the tendon as it passes down over the trochlea of the femur to insert on the tibial crest.
FABELLAE
The medial and lateral fabellae are two small sesamoid bones located in the proximal gastrocnemius or calf muscle tendons just above and behind the femoral condyles of dogs and cats. They are not present in cattle or horses.
TIBIA
The tibia (Figure 7-35) is the main weight-bearing bone of the lower leg. It forms the stifle joint with the femur above it and the hock with the tarsus below it. When viewed from above, the proximal end of the tibia appears triangular with the apex of the triangle facing forward. The tibial condyles on top of the proximal end articulate with the condyles of the femur. The forward-facing point of the triangle is the tibial tuberosity, which continues distally as a ridge called the tibial crest. The patellar ligament attaches to the tibial tuberosity. The shaft of the tibia is triangular at the proximal end and fairly round further distally. At its distal end, the articular surface of the tibia consists of grooves that articulate with the tibial tarsal bone. Medial to the distal articular surface of the tibia is a palpable process called the medial malleolus, which is the “knob” on the medial side of our ankle at the distal end of our tibia. If you start at the tibial crest just below
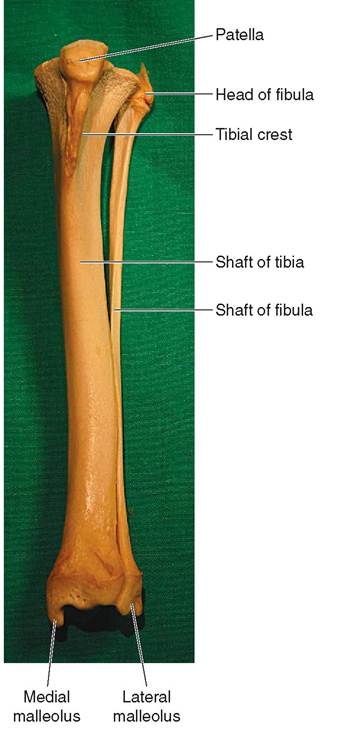
FIGURE 7-35 Can ine left tibia, fibula, and patella. Cranial view.
the front of your knee, you can trace down the tibia or shinbone to your medial malleolus.
FIBULA
The fibula (see Figure 7-35) is a thin but complete bone in dogs and cats that parallels the tibia and consists of a proximal extremity, a shaft, and a distal extremity. It does not support any significant weight but mainly serves as a muscle attachment site. In horses and cattle, only the proximal and distal ends of the fibula are present—the shaft is not. At its distal end, the fibula forms a palpable process called the lateral malleolus. The lateral knob of our ankle is our lateral malleolus.
TARSAL BONES
The tarsus (Figure 7-36) is what we call our ankle. In a fourlegged animal, it is commonly called the hock. It consists of two rows of short bones known as the tarsal bones. Like the carpus, the proximal row of bones is named, and the distal row is numbered. The two largest proximal tarsal bones are the tibial tarsal bone and the fibular tarsal bone. A smaller, central tarsal bone is tucked behind the two larger bones. The tibial tarsal bone has a large trochlea that articulates with the distal end of the tibia to form the most movable part of the hock joint. The calcaneal tuberosity of the fibular tarsal bone projects upward and backward to form the point of the hock. It acts as the point of attachment for the tendon of the large gastrocnemius muscle and corresponds to our heel. The distal row of tarsal bones is numbered from medial to lateral, much like the distal row of carpal bones.
CLINICAL APPLICATION
CLINICAL APPLICATION
Canine Hip Dysplasia
Canine hip dysplasia is an abnormal looseness or laxity of the hip joints of some dogs that leads to joint instability and degenerative bony changes. Many factors contribute to its development, including overnutrition that leads to too rapid growth, exercise, and genetic factors. Puppies of dysplastic parents are more likely to develop hip dysplasia than are puppies of normal parents, and larger breeds are affected more often than smaller breeds.
In a dysplastic animal, the normally tight-fitting hip joint is much looser, allowing the femoral head to “rattle around” in the acetabulum. This damages the joint surfaces and leads to degenerative changes and osteoarthritis. Movement of the diseased hips is painful, especially after exercise. Definitive diagnosis of canine hip dysplasia usually requires pelvic radiographs, and treatment can range from weight reduction and exercise restriction, to medical treatments with antiinflammatory drugs, to a variety of surgical procedures. The best treatment for canine hip dysplasia is to attempt to prevent its development by only breeding hip dysplasia-free parents.
Patellar Luxation in Dogs
Normally the patella rides securely in the deep groove of the trochlea on the distal end of the femur. The pull of the quadriceps tendon is normally directly in line with the trochlea. Sometimes physical abnormalities cause the pull of the tendon to be off-line, or one rim of the trochlear groove may not be high enough to hold the patella securely in place. When that occurs, the patella can luxate or pop out of the trochlea, usually toward the medial side. The most common type of patellar luxation occurs in small and miniature dog breeds and results in the patella popping out of the medial side of the trochlear groove when the foot is planted. This causes pain when the animal tries to flex the stifle joint to take its next step, and so it will often carry or hold up the affected leg for a step or two until the patella pops back into place. This causes a periodic, skipping-type gait that is characteristic of this disorder. The condition is easily diagnosed by extending the stifle joint and palpating the easily displaced patella. Treatment usually consists of any of several types of surgical correction.
METATARSAL BONES
The metatarsal bones (see Figure 7-36) are almost exactly the same as the metacarpal bones. The only major differences
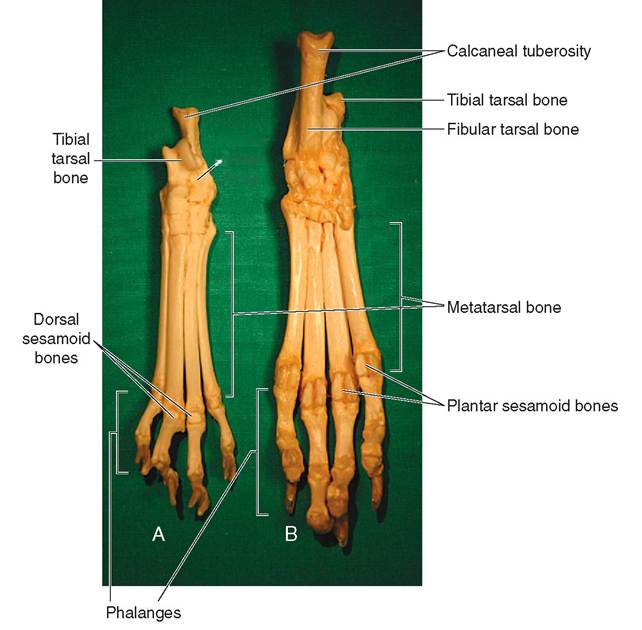
Fibulai,tarsat,bone
FIGURE 7-36 Left feline and canine tarsus, metatarsals, and phalanges A, Feline, dorsal view. B, Canine, plantar view.
are in the dog and cat. Usually only four digits make up the paw on each hind leg, so there are usually only four metatarsal bones: metatarsals II through V. Like the front leg, horses have a large metatarsal bone—the cannon bone—and two small metatarsal bones—the splint bones—on each hind leg. Our metatarsal bones are the bones of our feet.
PHALANGES
The phalanges of the pelvic limb (see Figure 7-36) are almost exactly like the phalanges of the thoracic limb. The only major difference is, again, in dogs and cats. Usually only four digits make up the paw on each hind leg: digits II through V.
CLINICAL APPLICATION
Using External Skeletal Landmarks in Body Condition Scoring
Body condition scoring (BCS) uses a numerical scale to indicate the amount of fat in an animal’s body. The details of different BCS systems vary, but most use either a 9-point or 5-point scoring system. In each case the middle of the range, 5 out of 9 (BCS = 5/9) or 3 out of 5 (BCS = 3/5), is the desired body condition status. An animal with a low BCS is too thin: a BCS of 1/5 or 1/9 means the animal is emaciated. An animal with a high BCS is overweight: one with a BCS of 5/5 or 9/9 is obese.
Regardless of the BCS system being used, the basic technique involves visually assessing the animal’s body shape, and palpating (feeling) external skeletal landmarks to determine how much fat is around them. Common skeletal landmarks used in body condition scoring include ribs, vertebrae (wings of atlas, spinous processes, transverse processes), shoulder (greater tubercle of humerus, spine of scapula), elbow (olecranon process of ulna, epicondyles of humerus), pelvis and hip (ilium, ischium, greater trochanter of femur), and stifle (patella, epicondyles of femur).
The more prominent these skeletal landmarks are, the lower the amount of fat in the animal’s body, and the lower the BCS. Conversely, the more difficult these landmarks are to feel, the greater the amount of fat in the body, and the higher the BCS.
Author’s note: Precise BCS criteria vary from species to species. (Enter “Body Condition Scoring” into your favorite internet search engine to see some examples.) But the basic concepts can be applied to virtually any animal species. At the zoo I am often asked by zookeepers to assess their animals’ body conditions. They use those values along with body weights to judge whether the animals’ diets are appropriate. On a given day I may evaluate the BCS of a chinchilla weighing less than a pound, and that of a camel weighing a ton. The same basic principles apply to each.
TEST YOURSELF 7-6
CLINICAL APPLICATION
1. Name the bones of the pelvic limb from distal to proximal.
2. What three pairs of bones make up the pelvis? What region of the pelvis does each form?
3. What is the largest sesamoid bone in the animal body?
4. Which bone is larger and supports more of an animal's weight, the tibia or the fibula?
5. On which bone of the pelvic limb is the calcaneal tuberosity found? What is its purpose?
6. Is an animal with a body condition score (BCS) of 3/9 too fat or too skinny?
VISCERAL SKELETON
The visceral skeleton consists of bones that form in soft organs or viscera. It is the strangest division of the skeleton and the most variable. Not all animals have visceral bones. As a matter of fact, they are pretty unusual. Three examples include the os cordis, os penis, and os rostri. The os cordis is a bone in the heart of cattle and sheep that helps support the valves of the heart. The os penis (Figure 7-37) is a bone in the penis of dogs, beavers, raccoons, and walruses that partially surrounds the penile portion of the urethra. The urethral groove on the ventral surface of the bone encloses the dorsal portion of the urethra. The os rostri is a bone in the nose of swine that strengthens the snout for the rooting behavior of pigs, whereby they dig into the ground with their snouts. In Europe, pigs are used to find and root out rare and expensive truffles, a type of underground fungus used in gourmet cooking.
JOINTS
Joints are the junctions between bones. Some of them are completely immovable, some are slightly movable, and some are freely movable. When we think of joints, we usually think of freely movable joints, such as the elbow or the hip; however, the immovable sutures that hold most of the skull bones together are joints also.
JOINT TERMINOLOGY
The terms arthro- and articular refer to joints. For example, the study of joints is arthrology, and the smooth bony
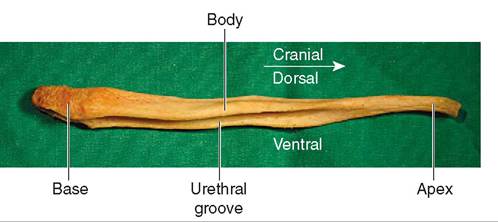
FIGURE 7-37 Can ine os penis. Lateral view.
Canine Os Penis Problems
The most common clinical problem associated with the os penis in dogs occurs when urinary calculi, called stones, lodge in the urethra where it enters the narrow urethral groove at the base of the bone. The lodged calculi can obstruct the flow of urine, and surgery may be required to remove them.
Author’s note: I once saw a fractured os penis in a Labrador-type dog. The dog was very weak and nearly comatose when it was presented by the owners. They reported lethargy, vomiting, and progressive weakness over the previous several days. Abdominal radiographs showed fluid in the dog’s abdomen and a complete fracture through the body of the os penis. When I explored the abdomen surgically, I found a sizeable tear in the wall of the urinary bladder and a large quantity of urine free in the abdominal cavity. The fractured os penis had apparently obstructed the flow of urine through the urethra, which resulted in the urinary bladder filling to the point that it burst. The dog became very ill after waste products from the urine in its abdomen were absorbed back into the bloodstream. I removed the urine, repaired the urinary bladder, and sutured a urethral catheter into place until the fracture healed. Happily, the dog went on to make a complete recovery.
surfaces that come together to form freely movable joints are called articular surfaces.
The terminology of arthrology can be confusing because the meanings of many anatomical terms used to describe types of joint are obscure and cryptic to many of us. In our discussions of joints, we use the clearer terms commonly used in clinical veterinary medicine. The more complex anatomical terms are mentioned in case you wish to consult other, more in-depth anatomical references.
TYPES OF JOINT
The three general classifications of joint in the animal body are the immovable fibrous joints, the slightly movable cartilaginous joints, and the freely movable synovial joints.
FIBROUS JOINTS
The anatomical term for fibrous joints is synarthroses. (See what I mean about that obscure terminology?) Fibrous joints are immovable in that the bones are firmly united by fibrous tissue. Some examples include the sutures that unite most of the skull bones (Figure 7-38) and the fibrous union of the splint bones of horses with the large metacarpal and metatarsal bones.
CARTILAGINOUS JOINTS
Slightly movable, cartilaginous joints are termed amphiarthroses. They are capable of only a slight rocking movement. Examples include the intervertebral joints (containing the discs) between the bodies of adjacent vertebrae in the spine and the symphyses between the two halves of the pelvis and
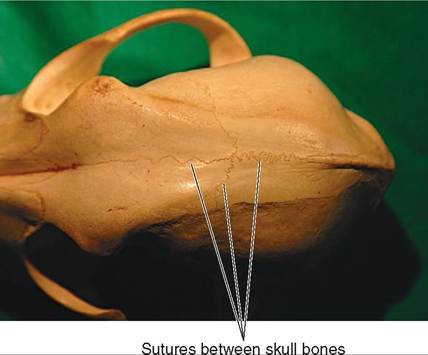
FIGURE 7-38 Fibrous joints. Dorsal view of sutures between canine skull bones.

FIGURE 7-39 Cartilaginous joint. Rostral view of feline mandibular symphysis.
between the two sides of the mandible (Figure 7-39) in some animals.
SYNOVIAL JOINTS
Synovial joints are what we usually think of when we hear the word joint. They are freely movable joints, such as the shoulder joint and the stifle joint. The anatomical term for synovial joints is diarthroses.
The rest of our discussion of joints centers on synovial joints.
SYNOVIAL JOINT CHARACTERISTICS. Synovial joints all share some common characteristics. These include articular surfaces on the bones, articular cartilage covering the articular surfaces, and a fluid-filled joint cavity enclosed by a joint capsule. Firm connective tissue bands called ligaments may help stabilize the bones and hold the j oint together.
Articular surfaces are the very smooth joint surfaces of bones, where they rub together in a joint. They consist of a smooth, thin layer of compact bone over the top of cancellous bone.
Articular cartilage is a thin, smooth layer of hyaline cartilage that lies on top of the articular surface of a bone. The articular cartilage functions like a Teflon coating on the joint surfaces to aid the smooth movement between them to reduce friction.
The joint cavity, also called the joint space clinically, is a fluid-filled potential space between the joint surfaces. A multilayered joint capsule surrounds it. The outer layer of the joint capsule is fibrous tissue, and the lining layer is called the synovial membrane. The synovial membrane produces the synovial fluid that lubricates the joint surfaces. Synovial fluid is normally transparent and has the viscosity of medium-weight motor oil. When joint disease is suspected, a joint “tap” is often done. This involves doing a presurgical skin prep, inserting a sterile needle into the joint cavity, and withdrawing synovial fluid for examination, analysis, and possible bacterial culture.
Ligaments are bands of fibrous connective tissue that are present in and around many synovial joints. They are similar to tendons but differ in that they join bones to other bones. Tendons join muscles to bones. Ligaments are not present in all synovial joints, but when they are present, they are often vital to the joint's effective operation.
The stifle joint, which is equivalent to our knee, offers an excellent model of how important ligaments can be to normal joint function. Consult Figure 7-40 as we look at the components of the stifle joint. The arrangement of the joint surfaces of the stifle joint, between the distal end of the femur and the proximal end of the tibia, makes it an inherently unstable joint. No deep sockets or closely fitting heads are present to hold it together or to allow only the desired hingelike movements between the bones. The round condyles of the femur sit on top of the flattish condyles of the tibia, supported only by two shallow, concave, half-moonshaped fibrocartilage structures, which are the medial meniscus and the lateral meniscus.
The stifle joint normally only bends and straightens like a hinge. Bend and straighten your knee and you will see the normal movement of the joint. A large tendon and a group of four ligaments provide the stability that allows the stifle joint to function properly. The large tendon is the distal tendon of the large quadriceps femoris (cranial thigh) muscle that passes over the cranial surface of the stifle joint and attaches to the proximal end of the tibia at the tibial tuberosity. The patella, or kneecap, is embedded in this tendon. The tendon is called the quadriceps femoris tendon until it reaches the patella. Distal to the patella its name changes to the patellar ligament. Same structure, different name. The patellar ligament provides support on the front of the stifle joint. On the medial and lateral sides of the joint, two straplike collateral—which means on both sides—ligaments connect the femur and the tibia, and prevent sideways movement of the bones. Inside the joint are two ligaments that cross each other like the letter X. They are called the cranial and caudal cruciate (X-shaped) ligaments. They help prevent the bones of the stifle from sliding forward and backward as the joint bends and straightens.
SYNOVIAL JOINT MOVEMENTS. The movements possible in synovial joints are illustrated in Figures 7-41 and 7-42. They are flexion, extension, adduction, abduction, rotation, and circumduction.
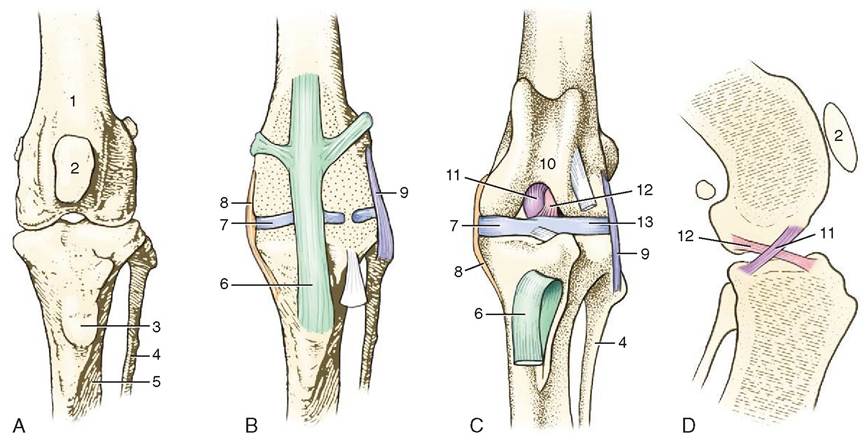
FIGURE 7-40 Left stifle joint of the dog. A-C, Cranial views. A shows just the bones. The extent of the joint capsule is shown in B. The patella has been removed in C. D shows the crossing of the cruciate ligaments in a medial view. 1, Femur; 2, patella; 3, tibial tuberosity; 4, fibula; 5, tibia; 6, patellar ligament; 7, medial meniscus; 8, medial collateral ligament; 9, lateral collateral ligament; 10, trochlea; 11, caudal cruciate ligament; 12, cranial cruciate ligament; 13, lateral meniscus. (Adapted from Dyce KM, Sack WO, Wensing CJG: Textbook of veterinary anatomy, ed 4, St Louis, 2010, WB Saunders Company.)
CLINICAL APPLICATION
Cranial Cruciate Ligament Rupture
Sometimes, particularly in dogs, a wrong step can result in a rupture or tearing of the cranial cruciate ligament (CCL), which is damaged more often than other ligaments. This injury can occur in athletic dogs if they plant a foot wrong while running and turning, or it can occur in overweight, sedentary dogs if they land wrong as they jump off the couch. The result is instability of the stifle joint. Instead of hinging on each other like they are supposed to, the femur and tibia also slide forward and backward relative to each other. This can damage other joint structures, such as the menisci, and can lead to osteoarthritis in the joint.
Rupture of the CCL is diagnosed by palpating the stifle joint and producing what is called anterior drawer movement, which is an abnormal forward and backward movement of the femur and tibia relative to each other. Therapy for CCL rupture can range from exercise restriction, weight reduction, and physical therapy to any of several surgical repair techniques.
Flexion and extension are opposite movements. Flexion decreases the angle between two bones. Picking a horse's front foot up for examination flexes the carpus joint. Extension is the opposite movement, and it increases the angle between two bones. Straightening a bent (or flexed) elbow joint extends the joint.
Adduction and abduction are also opposite movements. They involve movement of extremities relative to the median plane of the body. Adduction is the movement of an extremity toward the median plane, and abduction is a movement away from the median plane. One way to avoid confusion is to remember that to abduct something is to take it away.
Rotation is a twisting movement of a part on its own axis. If you hold your arm out with your palm down and move it so your palm is up, that movement is rotation.
Circumduction is the movement of an extremity so that the distal end moves in a circle. You can produce this movement by extending your arm and moving your hand in a circle.
TYPES OF SYNOVIAL JOINT. Synovial joints can be categorized according to the type of joint surfaces and the movements that are possible. Most of the joints of the body can be classified into one of four basic joint types: hinge joints, gliding joints, pivot joints, and ball-and-socket joints.
HINGE JOINTS. Hinge joints are also called ginglymus joints. One joint surface swivels around another. The only movements possible are flexion and extension. The elbow joint (Figure 7-43) is a good example of a hinge joint, as is the atlantooccipital joint (Figure 7-44) between the occipital bone in the skull and the first cervical vertebra. Flexion and extension of the atlantooccipital joint moves the skull up and down in a nodding, “yes” motion.
GLIDING JOINTS. The complicated name for gliding joints is arthrodial joints, but rocking joints would be more
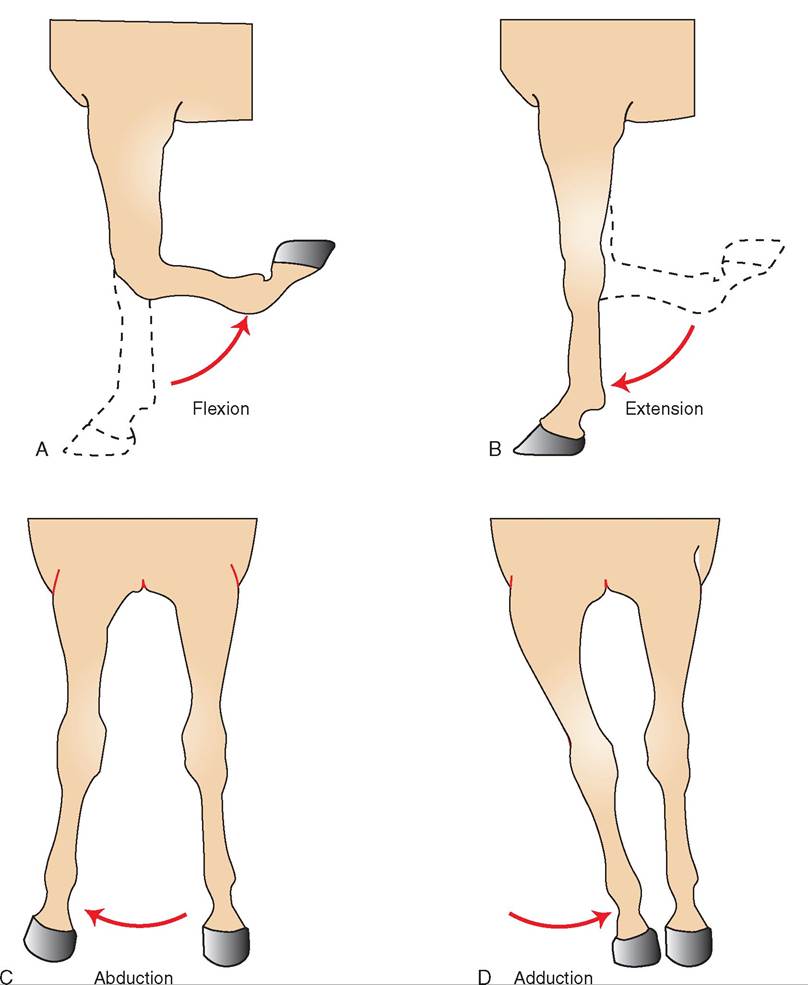
FIGURE 7-41 Movements of equine front leg. A, Flexion, lateral view. B, Extension, lateral view. C, Abduction, cranial view. D, Adduction, cranial view.
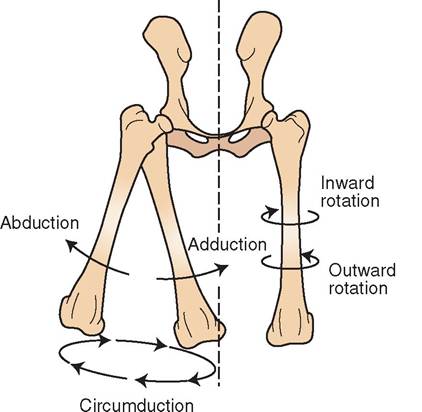
FIGURE 7-42 Movements of the canine femur. Cranial view.
FIGURE 7-43 Hinge-type synovial joint. Canine left elbow, lateral view.
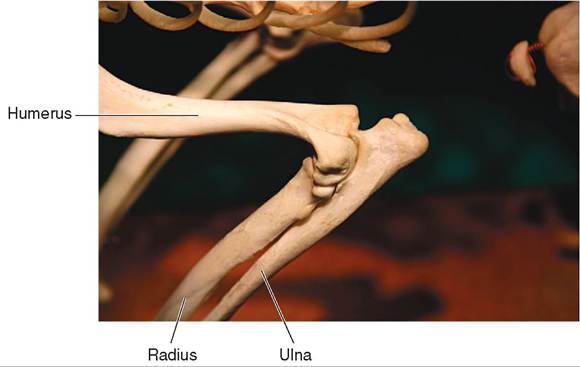
FIGURE 7-44 Hinge-type and pivot-type synovial joints. Canine atlantooccipital (hinge) joint and atlantoaxial (pivot) joint.
Canine skull and cervical vertebrae, caudal view.
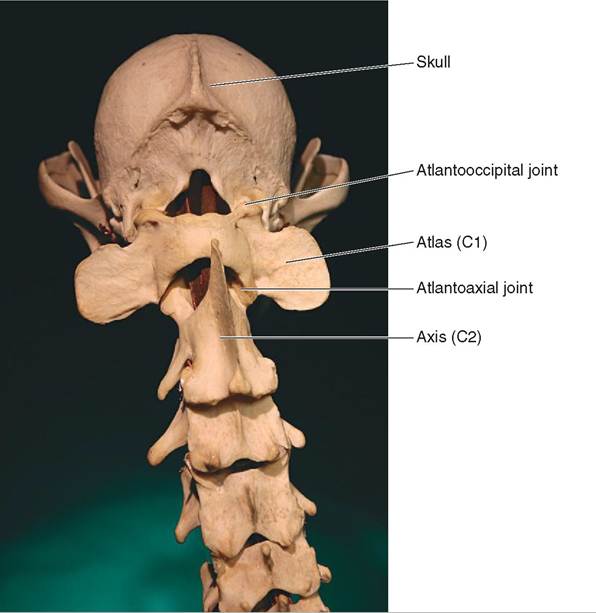
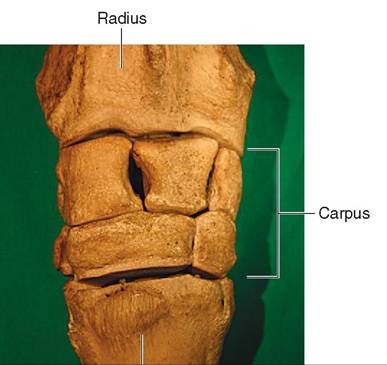
Large metacarpal bone
(cannon bone)
FIGURE 7-45 Gliding-type synovial joint. Equine carpus, cranial view.
descriptive. The joint surfaces of a gliding joint are relatively flat. The movement between them is a rocking motion of one bone on the other. The main movements possible are flexion and extension, but some abduction and adduction may also be possible. The carpus or wrist (Figure 7-45) is a good example of a gliding joint. Note that you can flex and extend your wrist, but you can also move your hand side to side (abduction and adduction). Most four-legged animals can do only the flexion and extension part.
PIVOT JOINTS. Pivot joints are also known as trochoid joints. One bone pivots or rotates on another. The only movement possible is rotation. Only one true pivot joint is found in the bodies of most animals, that being the joint between the first and second cervical vertebrae— the atlantoaxial joint (see Figure 7-44). Some anatomists with a sense of humor refer to this as the no joint, because the only movement it allows is a rotation of the head back and forth in a “no” movement. The movement is actually occurring between the vertebrae, but the head goes along with the first cervical vertebra as it pivots on the second cervical vertebra.
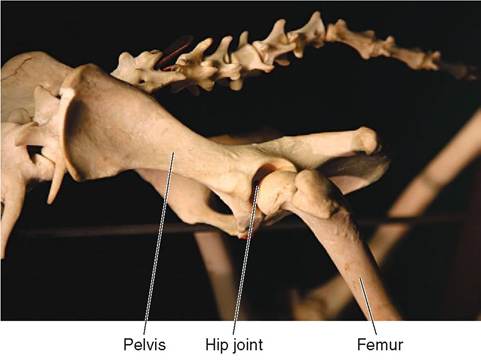
FIGURE 7-46 Ball-and-socket synovial joint. Canine left hip joint, craniolateral view.
BALL-AND-SOCKET JOINTS
Ball-and-socket joints are also called spheroidal joints. They allow the most extensive movements of all the joint types and allow all the synovial joint movements. Ball-and- socket joints permit flexion, extension, abduction, adduction, rotation, and circumduction. The shoulder and hip joints (Figure 7-46) are ball-and-socket joints.
TEST YOURSELF 7-7
1. What are the main characteristics of fibrous joints, cartilaginous joints, and synovial joints?
2. What is synovial fluid and why is it important to the functioning of a synovial joint?
3. What is the difference between a tendon and a ligament?
4. Make the following joint movements with your own body: abduction, adduction, circumduction, extension, flexion, and rotation.
5. Name some examples of each of these kinds of synovial joint:
Ball-and-socket joint
Gliding joint
Hinge joint
Pivot joint