Tissues: Living Communities
Joanna M. Bassert
OUTLINE
INTRODUCTION, 105
GROSS AND MICROSCOPIC ANATOMY, 105 EPITHELIAL TISSUE, 105
General Characteristics of Epithelia, 106
Classifications of Epithelia, 108
Types of Epithelia, 109
Glands, 113
CONNECTIVE TISSUE, 119
General Characteristics, 119
Components of Connective Tissue, 120
Types of Connective Tissue, 122
Membranes, 129
MUSCLE TISSUE, 140
Skeletal Muscle, 140
Smooth Muscle, 140
Cardiac Muscle, 142
NERVOUS TISSUE, 142
TISSUE HEALING AND REPAIR, 142
Inflammation: The First Stage, 144
Organization: The Formation of Granulation
Tissue, 145
Regeneration or Fibrosis, 145
Classifications, 145
LEARNING OBJECTIVES
When you have completed this chapter you will be able to:
1.
List the four major tissue types.2. Describe the functions of epithelial tissues.
3. Differentiate among the three major types of cellular junction found between epithelial cells.
4. Describe the structure of the basement membrane.
5. List and describe the characteristics used to classify different epithelial tissues.
6. List and describe the characteristics used to classify different glands.
7. List and describe the components of connective tissues.
8. Differentiate between areolar, adipose, and reticular connective tissues.
9. Differentiate between dense regular, dense irregular, and elastic connective tissues.
10. Differentiate between hyaline cartilage, elastic cartilage, and fibrocartilage.
11. List and describe the components of bone.
12. Describe each of the three types of muscle.
13. List the components of the neuron.
14. List and describe each of the phases of healing.
VOCABULARY FUNDAMENTALS
Absorptive cell ahb-sohrp-tihv sehl Acinar gland ah-sihn-ahr glahnd Adipose ahd-ih-pos
Adipose cell ahd-ih-pos sehl
Alveolar gland ahl-ve-o-lahr glahnd Amorphous ah-mohr-fuhs
Apical surface a-pihck-ahl suhr-fihs Apocrine gland ahp-o-krihn glahnd
Areolar connective tissue ah-re-o-lahr kuh-nehck-tihv tihsh-yoo
Articular cartilage ahr-tihck-yuh-lor kahr-tih-lihj
Ascites ah-sι-tez
Avascular a-vahsk-yoo-lahr
Axon ahck-sohn
Basal surface bas-sahl suhr-fihs
Basement membrane bas-mehnt mehm-bran
Blast blahst
Blood bluhd
Bone bon
Broad ligament brawd lihg-ah-mehnt
Brown adipose tissue brann ahd-ih-pos
tihsh-yoo
Brush border bruhsh bohr-Uor
Calcified kahl-sih-fiU
Canaliculi kahn-ahl-ihck-u-li
Cardiac muscle kahr-Ue-ahck muhs-uhl
Cartilage kahr-tih-lihj
Chondroblast kohn-Uro-blahst
Chondrocyte kohn-Uro-sit
Chondroitin sulfate kol-n-droy-tihn suhl-fat
Chondronectin -oI-u- dro -nehck-tihn
Cilia sihl-e-ah
Collagenous fiber kohl-lahj-ehn-uhs fi-bor
Compound gland kohm-pohwnU glahnd
Connective tissue kuh-nehck-tihv tihsh-yoo
Connective tissue proper kuh-nehck-tihv tihsh-yoo praw-por
Connexon keh-nehck-sohn
Cuboidal cell kyoo-hbl oy-Uahl se
Cuboidal epithelium kyoo-boy-Uahl ehp-ih-the-le-uhm
Cutaneous membrane kyoo-ta-ne-uhs mehm-brao
Cyte sit
Dendrite dehn-Urit
Dense fibrous connective tissue Uohnz fi-bruhs kuh-nehck-tihv tihsh-yoo
Dense irregular connective tissue dohnz ihr-rehg-u-lor kuh-nehck-tihv tihsh-yoo
Dense regular connective tissue dohnz rehg-u-lor kuh-nehck-tihv tihsh-yoo
Dermis dar-mihs
Desmosome dehz-mo-som
Diapedesis Ui-ah-peh-de-sihs
DuctuUhckt
Edema -h-de-mah
Effusion e-fu-shuhn
Elastic cartilage -Ii -lahs-tihck kahr-tih-lihj
Elastic connective tissue -Ii-lahs-tihck kuh-nehck-tihv tihsh-yoo
Elastic fiber eh-lahs-tihck fi-bor
Endocrine gland ehn-Uo-krihn glahnd
Endocrine system ehn-Uo-krihn sihs-tehm
Endothelium ohn-do-the-le-uhm
Epidermis el-p-ili-dar-milis
Epithelial tissuehep-ih- the-le-ahl tihsh-yoo
Epithelialization el-p-Hi-the-le-ahl-ih-ha-shuhn Erythrocyte e-rihth-ro-sit
Excretionheck- skre-shuhn
Excretory duct ehck-skreh-tohr-euUhckt
Exocrine gland ehcks-o-krihn glahnd
Extracellular fiber c^hs-trah-sehl-u-lahr
fi-bor
Extracellular matrix ehsks-ah-Ii-sehl-u-lahr ma-trihks
Exudate ehcks-u-Uat
Fascia fahsh-e-ah
Fibrin fi-brihn
Fibrinogen fi-brihn-o-jehn
Fibroblast fi-bro-blahst
Fibrocartilage fi-bro-kahr-tih-lihj
Fibrous adhesion fi-bruhs ahU-he-shuhn
First-intention healing HIi-S t ihn-tehn-shuhn
he-lihng
Fixed cell fihkst sehl
Gap junction gahp juhngk-shuhn
Glandular epithelium glahnd-u-lahr ehp-ih-the-le-uhm
Glycosaminoglycanl g i-kos-ah-me-no-gli-kahn
Goblet cell gohb-hlleht se
Granulation tissueraghn- u-la-shuhn tihsh-yoo
Gristle grihs-ehl
Ground substancerogunU suhb-stuhnh
Haversian canal hah-var-hhehn kuh-nahl
Hemidesmosome Iielim-e-dehs-mo-som
Hemorrhaging hehm-ohr-rihUj-ihng
Hemothorax hem-o-thorh-ahx
Heparin hehp-ahr-ihn
Hibernate hi-bor-nat
Hibernating gland hi-bor-nat-ihng glahnd
Histamine hihs-tah-men
Histiocyte hihs-te-o-sit
Histology hihs-tohl-o-je
Holocrine gland hol-alehhn-Ukrihn g
Homogeneous ho-mo-je-ne-uhs
Hormone hohr-mon
Hyaline cartilage hi-ahl-ihn kahr-tih-lihj
Hyaluronic acid hi-ah-lu-rohn-ihck
ah-sihU
Hyaluronidase hi-ah-lu-rohn-ih-Uah
Immunoglobulin ihm-u-no-gloh-bu-lihn
Infection ihn-fehck-shuhn
Inflammatory process ihn-flahm-ah-tohr-e proh-sehs
Innervated ihn-nar-vat-ehU
Integument ihn-tehg-gu-mehnt
Intermediate filament ihn-tor-me-Ue-eht fihl-ah-mehnt
Junctional complex juhnck-shuhn-ahl kohm-plehkx Keratin kear-ah-tehn
Keratinized stratified squamous epithelium kear-ah-teh-nihU straht-eh-fiU skwey-muhs ehp-ih-the-le-uhm
Kupffer cell koopf-for sehl
Lacunae lah-kyoo-ne
Lamina propria lahm-ihn-ah pro-pre-ah
Leukocyte loo-ko-sit
Loose connective tissueolso kuh-nehck-tihv
tihsh-yoo
Lumen loo-mehn
Macrophage mah-kro-faj
Mast cell mahst sehl
Merocrine gland mar-o-krihn glahnd
Mesoderm me-so-Uorm
Mesothelium me-so-the-le-uhm
Microanatomy mi-kro-ah-naht-ah-me
Microbe mi-krob
Microglial cell mι-kro-gle-ahl sehl
Microvilli mi-kro-vihl-li
Mixed exocrine gland mihckst ehcks-o-krihn glahnd
Mucin myoo-sihn
Mucosae myoo -ko-se
Mucous membrane myoo-kuhs mehm-bran
Mucous secretion myoo-kuhs seh-kre-shuhn
Muscle tissue muhs-uhl tihsh-yoo
Myoepithelial cell mι-o-ehp-ih-the-le-ahl sehl
Nephrosis nehf-ro-sihs
Nervous tissue ∏ar-vuhs tihsh-yoo
Neuroglial cell nar-ohg-le-ahl sehl
Neuron ∏ar-ohn
Nonstriated involuntary muscle nohn-stri-a-tehd ihn-vohl-uhn-tear-e muhs-uhl
Omentum o-meh∏-tuhm
Osteoblast ohs-te-o-blahst
Osteoclast ohs-te-o-klahst
Oviduct o-vih-duhckt
Paralyzed pear-ahl-izd
Paramecium pear-ah-me-ce-uhm
Paretic pah-reht-ihck
Parietal layer pah-ri-eh-tahl la-ar
Pathogen pahth-o-jehn
Pericardial fluid pear-ih-kahr-de-ahl floo-ihd
Perichondrium pear-ih-koh∏-dre-uhm
Perikaryon pear-ih-kear-e-ohn
Peristalsis pear-eh-stahl-sihs
Peritoneal fluid pear-ih-to-∏e-ahl floo-ihd
Peritonitis pear-ih-tehn-i-tihs
Phagocytize fahg-o-sih-tiz
Pitting edema piht-tihng eh-de-mah
Plaque plahck
Plasma plahz-mah
Platelet plat-leht
Pleural fluid ploor-ahl floo-ihd
Polar po-lahr
Proteoglycan pro-te-o-gli-kahn
Proud flesh proud flehsh
Pseudostratified columnar epithelium soo-do-straht-eh-fid koh-luhm-hnpa-hihr-e the-le-uhm
Reproductive system re-pro-duhck-tihv sihs-tehm
Reticular cell heh-tihck-u-lahr sehl
Reticular connective tissue re Ii-tihck-u-lahr -∏ehck-tihv
tihsh-yoo
Reticular fiber reh -tihck-u-lahr fi-bar
Sebaceous gland seh-ba-shuhs glahnd
Second-intention healing sehk-uhnd ihn-teh∏-shuhn he-lihng
Secretionhs-e kre-shuhn
Secretory unit se-kreh-tohr-e u-niht
Serosaehs-e ro-se
Serous membrane seer-uhs mehm-bran
Serous secretion seer-uhs seh-kre-shuhn
Simple ciliated columnar epithelium sihmp-ehl sihl-e-a-tehd koh-luhm-nahr ehp-ih-the-le- uhm
Simple columnar epithelium sihmp-oehh-l k luhm-nahr
ehp-ih-the -le -uhm
Simple cuboidal epithelium sihmp-ehl kyoo-boyd-ahl ehp-ih-the -le -uhm
Simple epithelium sihmp-heph-lihe- the-le-uhm
Simple gland sihmpl-aehnl dg
Simple squamous epithelia sihmp-ehl skwey-muhs ehp-ih-the-le-ah
Skeletal muscle skehl-ih-tahl muhs-uhl
Smooth muscleosthmo muhs-uhl
Specialized connective tissue spehsh-uh-lιzd kuh-∏ehck-tihv tihsh-yoo
Squamous cell skwey-hml uhs se
Stratified cuboidal epithelium straht-eh-fid kyoo-boyd-ahl ehp-ih-the -le -uhm
Stratified epithelium straht-eh-fιd ehp-ih-the-le-uhm
Stratified squamous epithelium straht-eh-fid skwey-muhs ehp-ih-the -le -uhm
Striated muscle stri-at-ehd muhs-uhl
Stroma stro-mah
Submucosa ml-b-myoo-ko-sah
Synovial membrane sih-∏o-ve-ahl mehm-bran
Thrombocyte throhm-bo-sit
Thyroxine thi-rohck-zihn
Tight junction tit juh∏gk-shuhn
Tissue tihsh-yoo
Tonofilament to^ιo-fihl-ah-mehnt
Transitional epitheliumrathn- sihsh-ihn-ahl ehp-ih-the-le-uhm
Transudaterathn-soo- dat
Tubular gland too-bul-ahr glahnd
Tubuloacinar too-bul-o-ah-sihn-ahr
Tubuloalveolar too-bul-o-ahl-ve-o-lahr
Unicellular exocrine gland u-nih-sehl-u-lar ehcks-o-krihn glahnd
Vascularized vahs-kyoo-lahr-izd
Visceral layer vih-sar-ahl la-ar
Voluntary muscle vohl-uhn-tear-e muhs-uhl
White adipose tissue whit ahd-ih-pos tihsh-yoo
INTRODUCTION
A unicellular organism, such as a paramecium, can live as an individual.
It can feed itself, respire, grow, and produce or find all of the biochemical substances that it needs without the assistance of other cells. The cells that compose multicellular organisms, however, cannot survive independently. These cells have differentiated to form a wide range of cell types, each with its own characteristic structural features and distinct function. In the course of their differentiation, they have lost the ability to perform all of the metabolic functions required to sustain life as an isolated entity. Consequently, the cells that compose animals and all multicellular organisms exist within cooperative living communities.Many different types of community are found in any individual animal. These communities differ from one another based on the types of cells that compose them and on the role that they play in the organism as a whole. In this way, cells of similar type and function are clustered into layers, sheets, or groups called tissues. Tissues are classified into the following four primary types:
• Epithelial tissue
• Connective tissue
• Muscle tissue
• Nervous tissue
Although each classification is divided further into subgroups, each with its own special purpose, we can summarize the main functions of each tissue classification. In general, epithelial tissue covers and lines, connective tissue provides support, muscle tissue enables movement, and nervous tissue controls work. Because each type completes a specific purpose, the tissues must work collaboratively to meet the vital needs of the animal as a whole. Thus tissues are clustered to form organs, such as the liver, spleen, or kidney. All four tissue types can be found in most organs. The heart, for example, is a powerful muscle that moves blood throughout the body. Blood vessels, such as the coronary arteries, provide pathways for blood to reach the heart muscle. The vessels are composed of connective and epithelial tissues. Nerves and nervous tissue are threaded throughout the muscle of the heart to govern coordinated contractions of the ventricular and atrial chambers.
These chambers are covered and lined with layers of epithelia. In this chapter, epithelial and connective tissues are the primary focus. Muscle and nervous tissues are discussed in greater detail in subsequent chapters.GROSS AND MICROSCOPIC ANATOMY
Gross anatomy is the study of anatomic structures that can be s^en with the naked eye, and includes learning the names and locations of bones, muscles, arteries, veins, and nerves. Therefore anatomists must have excellent memories, because hundreds if not thousands of isolated structures can be examined. The study of the microscopic structures of tissues and organs is called histology or microanatomy. This chapter represents an introduction to ftuhdey st o microanatomy, a discipline that beautifully complements the study of gross anatomy and gives a struc- tourral basis f understanding the physiology of each anatomic system.
EPITHELIAL TISSUE
Epithelial tissue is composed of sheets of cells that cover and iine other tissues. For example, it lines the bladder, mouth, ebslsoeolsd, v thorax, and all of the body cavities and ducts in the body. Although well grounded to underlying struc- tpuitrhese,liea have an exposed surface that affords access to tuhrerosunding environment or to the inner openings of chambers and ducts. Epithelial tissue acts as an interface layer that separates and defines the beginning and ending of different types of tissues. It is protective of underlying tissues and frequently acts as a filter of biochemical substances. In addition, epi the 1i a may be absorptive; for example, the epithelia that line the gastrointestinal tract absorb nutrient mol- eocmules fr the gut, which are then placed into circulation. Epithelia can detect changes in the environment and play an iomleportant r in the reception of sensory input. Epithelial cnells o the tongue, for example, are sensitive to touch, temperature, and taste. The eyes, ears, and nasal passages also are assisted by the presence of specialized epithelia that provide tnhseatsieons of sight, sound, and smell.
The sensory infor- omllaetciotend c by these cells is conveyed to the nervous system.oAmnomthoenr c function of epithelial tissue is the
rsecretion o excretion of biochemical substances. Epithelia that engage in the manufacture and release of substances are called glandular epitheliau Glandular epithelial cells may occur as individuals, such as the goblet cells fonnd in the irntestine, o they may occur as organized glands, such as those found in the pancreas. Some of the substances produced by gland ular epithelia lubricate parts of the body, such auscuths e m secreted in the colon, whereas others play a vital role in producing biochemical substances that influence physiologic events. Hormones, enzymes, milk, sweat, and lemusk ar al examples of substances produced by glandular epithelia. Substances that ultimately leave the body, such as sweat, u⅛e, and feces, are called excretions, and substances that remain within the body, such as regulatory molecules auncudsm, are termed secretions.
Epithelia perform vital functions in the bodies of animals. The functions of epithelial tissue are summarized as follows:
• Protects, covers, and lines
• Filters biochemical substances
• Absorbs nutrients
• Provides sensory input
• Manufactures secretions
• Manufactures excretions
GENERAL CHARACTERISTICS OF EPITHELIA
Epithelial cells are organized into tightly packed groups that form sheets of tissue. These sheets may be composed of either a single layer or multiple layers of cells, depending on where they are located in the body. Although the size and shape of the cells vary, epithelia share certain common characteristics.
1. Epithelial cells are polar, that is, they have a sense of direction relative to surrounding structures. Each epithelial cell has an apical surface and a basal surface, which are quite different from one another. The apical surface is the side of the cell that faces the lumen or body cavity, and the basal surface is the side of the cell that faces the underlying connective tissue.
2. Epithelial cells have lateral surfaces that are connected to neighboring cells by junctional complexes. These junctions bring the cells into close apposition to one another, leaving little room for extracellular matrix. The matrix that surrounds epithelia therefore exists in very small quantities, if at all.
3. All epithelial cells lack blood vessels or capillaries. They are avascular and rely on underlying connective tissue to provide oxygen and nutrients.
4. Although some epithelia lack nerves, such as those in the stomach, intestines, and cervix, most epithelial cells are innervated and provide valuable sensory input.
CELLULAR ATTACHMENTS
Epithelial cells are held together in many ways. Their lateral surfaces, for example, are wavy and fit together like pieces of a jigsaw puzzle. Between the plasma membranes of adjacent cells are matrix-filled channels, which transport nutrients from underlying connective tissue. These passages act as distribution routes for biologic supplies and as elimination routes for waste. The plasma membranes of epithelial cells are joined to form specialized attachments, called junctional complexes, that give epithelial tissue surprising strength, even though the attachments only involve a small portion of the cell membrane. Three major types of cellular junction found between epithelial cells are tight junctions, desmo- somes, and gap junctions (Figure 5-1).
A tight junction is formed by the fusion of the outermost layers of the plasma membranes of adjoining cells. The matrix- filled space between cells is lost at the site of a tight junction. For centrally placed cells, the fusion occurs as a strip that wraps around the entire circumference of the cell, like a belt. In this way, an impenetrable barrier is formed that prevents the passage of substances from the luminal end to the basal end of the cell and vice versa. Only by passing through the body of the cell can substances pass through the epithelial layer. Tight junctions are found in tissues in which there can be no leaks, such as in the urinary bladder, where urine is held, or in the digestive tract, where they play a critical role in preventing the leakage of digestive enzymes into the bloodstream.
A desmosome is a strong, welded plaque or thickening, which connects the plasma membranes of adjacent cells. The bond is a mechanical coupling formed by filaments that interlock with one another, just as plastic fibers do in Velcro. In addition to these linkages intermediate filaments called tonofilaments extend from the plaque into the cytoplasm of each cell like anchors, forming stabilizing bases for the membrane junction. Since desmosomes form tough bonds between cells they are found most commonly in tissues that undergo repeated episodes of tension and stretching, such as the skin, heart, and uterus. Junctions that look like half of a desmosome are called hemidesmosomes, and these link epithelial cells to the basement membrane.
Cells that are connected by gap junctions are linked by tubular channel proteins called connexons (ko-NEK-sonz), which extend from the cytoplasm of one cell to the cytoplasm of the other. These transmembrane proteins allow the exchange and passage of ions and nutrients, such as nucleotides, sugars, and amino acids, from one cell to the other. Gap junctions are most commonly found in intestinal epithelial cells, the heart, and smooth muscle tissue. Although the exact function of gap junctions in epithelial cells is not yet fully understood, their role in cardiac and smooth muscle cells centers around their ability to transport electrical signals quickly from one cell to another. In this way, they coordinate the contraction of cardiac and smooth muscle.
BASEMENT MEMBRANE
The basement membrane is the foundation of the epithelial cell. It is a nonliving meshwork of fibers that cements the epithelial cell to the underlying connective tissue. Its strength and elasticity help prevent the cell from being torn off by intraluminal pressures, such as stretching or erosion caused by the rubbing of luminal material. The basement membrane (also called basal lamina) is manufactured and laid down by epithelial cells in varying degrees of thickness. The basement membrane in skin, for example, is thin, but in the trachea it is much thicker. Oxygen and nutrient molecules are supplied to the epithelial cells by diffusing through the basement membrane from capillaries in the underlying connective tissue. Similarly, nutrient substances that are absorbed and waste that is excreted by the epithelium diffuse across the basement membrane into the blood supply of the connective tissue. In this way, the basement membrane acts as a partial barrier between the epithelial cell and the underlying connective tissue. Cancerous epithelia do not respect this boundary and aggressively invade the connective tissue layer underneath.
SURFACE SPECIALIZATION
The surfaces of epithelial cells vary depending on where the epithelium is located in the body and, more importantly,
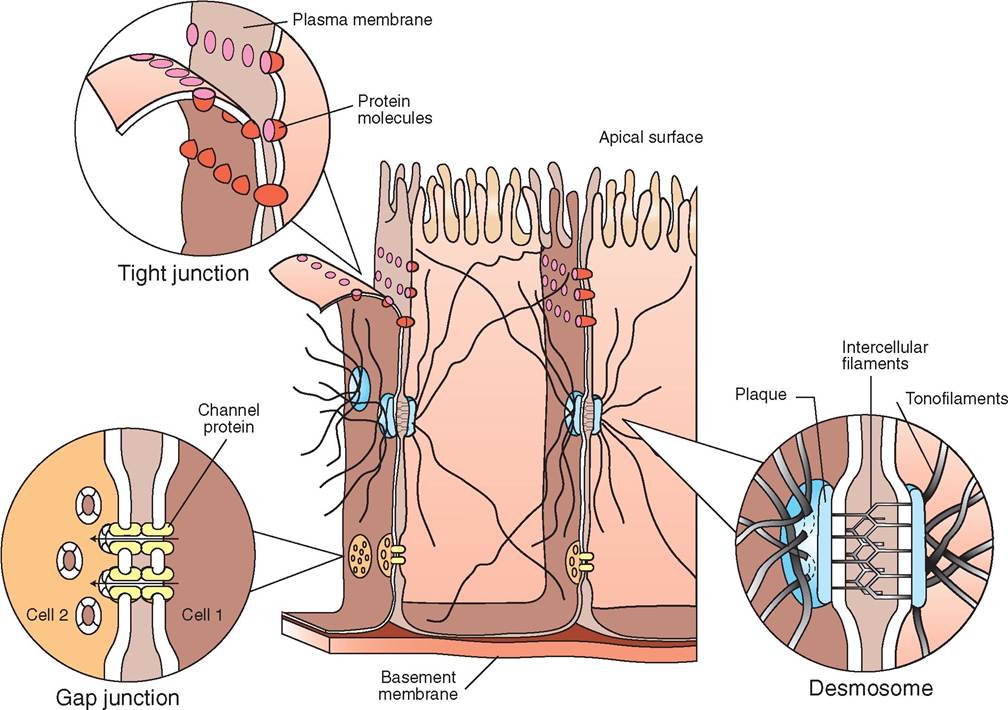
FIGURE 5-1 Intercellular junctions. An interesting feature of epithelial cells is the varied way in which they bond together. These intercellular junctions are both functionally and structurally different from one another. Three main types of intercellular connection are tight junctions, gap junctions, and spot desmosomes. A simplified form of these junctions is depicted here.
what role it plays in the function of the tissue. The epithelia that line blood vessels, for example, have smooth surfaces to allow the easy passage of blood cells. However other epithelia have irregular surfaces and may be covered with many fingerlike projections, called microvilli, or thousands of tiny hairs, called cilia (Figure 5-2).
The surface of a cell covered with microvilli is called the brush border. The brush border greatly increases the surface area of the cell, thereby increasing the absorptive ability of the cell. For this reason, microvilli usually occur on cells that are involved in absorption or secretion, such as the epithelia in the intestinal and urinary tracts. Remarkably, a cell with microvilli has about 20 times the surface area of a cell without them.
Cilia are also found on the free surface of cells, usually in the respiratory and urogenital tracts. In the trachea, for example, the cilia help to propel mucus and debris up and away from the lungs toward the mouth. In the opening of the oviduct, called the infundibulum, cilia encourage newly expelled ova into the oviduct. Ciliary movement occurs in coordinated “beats,” which enable the efficient transport of material. This coordinated action is brought about by an electrical potential that moves through junctional complexes connecting adjacent cells. The movement crosses the entire epithelial surface as a perfectly synchronized wave.
Epithelial cells of the skin become filled with a protective, waterproof substance called keratin. The accumulation of keratin occurs as the cell matures and moves from the basal layer to the superficial layer of the integument. These cells are called keratinized epithelium and are discussed in greater detail in Chapter 6.
TEST YOURSELF 5-1
1. What are the four primary types of tissue?
2. What is histology?
3. List seven functions performed by epithelial cells.
4. What four attributes characterize epithelial tissue in general?
5. List four types of cellular junction. Can you describe them?
6. How does the basement membrane act as a partial barrier between the epithelial cell and the underlying connective tissue?
7. Why do some epithelial cells have cilia and microvilli? What role do they play? Where are the cells with these specialized surfaces found in the body?
∕ j CLINICAL APPLICATION
Parvovirus: Killer of Intestinal Epithelia
Feline panleukopenia and canine parvoviral enteritis are life-threatening diseases that affect cats and dogs respectively. Parvoviruses, which cause both diseases, are highly contagious and are carried on clothing, shoes, and toys. They are shed in the feces and other excretions of affected animals and can be easily tracked into your house or veterinary office on the soles of your shoes. Fortunately, most cats and dogs are immunized against parvovirus and therefore never contract the disease. However, because of the highly contagious nature of these viruses, veterinary practices should isolate suspected carriers.
For animals that do contract parvovirus, mortality is high if untreated, particularly in young animals. The virus attacks and kills cells that are actively engaged in mitosis. Thus tissues that are continually renewing themselves, such as epithelial tissue, may be devastated by parvovirus. The small intestine, for example, is lined with epithelial tissue that helps to absorb nutrient molecules from the lumen of the gut. During parvovirus infections, the epithelial cells die and slough in sheets and animals develop diarrhea, vomit, and can become severely dehydrated in a short time. The sudden loss of epithelial tissue causes bleeding into the intestine, which creates a distinctively noxious, foul-smelling, hemorrhagic diarrhea. A simple laboratory test on the stool may indicate the presence of the virus and offer a definitive diagnosis.
Treatment centers on combating dehydration and includes intravenous fluid therapy with electrolyte supplements, antibiotics, and anti-vomiting medications. Animals that remain
alive after 3 to 4 days of illness generally survive but continue to shed the virus for several months. Because of the highly contagious nature of parvoviral diseases, some veterinary personnel who own young animals change their clothes and shoes before entering their homes.
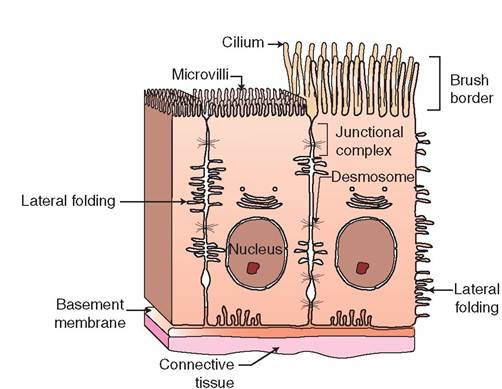
FIGURE 5-2 Epithelial cell specializations. In addition to forming unique intercellular connections, epithelial cells vary in their cell surfaces. Some cells are smooth and flat, whereas others have elaborate brush borders of microvilli designed to expand surface area to maximize the absorption or secretion of substances. In addition, epithelial cells may be covered with long, hairlike structures called cilia that beat in a rhythmic fashion to propel mucus and other materials across the cell's apical border. Elaborate folds of plasma membrane are also evident along the lateral sides of the cell, as well as on the surface. These are important in providing space for those materials that pass within cells from the apical to basal ends and vice versa.
CLASSIFICATIONS OF EPITHELIA
Epithelial tissue is classified according to the following three characteristics (Figure 5-3):
1. Number of layers of cells. If there is only a single layer of epithelial cells, the tissue is classified as simple. If there is more than one layer of cells, the tissue is called stratified. Simple epithelia provide little protection to the underlying connective tissue and therefore are found in protected areas of the body, such as internal compartments, ducts, vessels, and passageways. Stratified epithelia, on the other hand, are thicker and stronger and are found in areas of the body that are subjected to mechanical and chemical stress.
2. Shape of the cells. In cross section, epithelial cells may take on many shapes, such as squamous, cuboidal, and columnar. In stratified epithelium, many different cell shapes are visible within the same tissue, but the classification is based on the shape of the cell that resides on the exposed or luminal surface of the tissue. In stratified squamous epithelium, for example, cuboidal cells are visible near the basement membrane, but squamous cells are found at the luminal surface; therefore, the tissue is called stratified squamous, not stratified cuboidal.

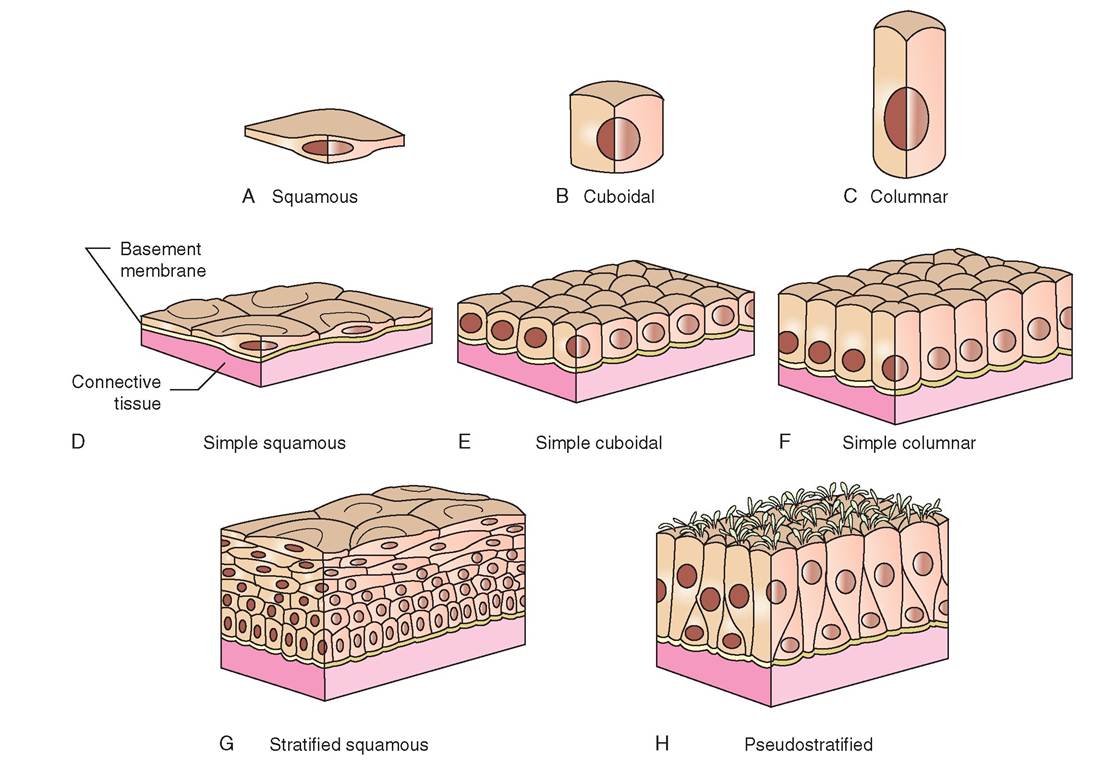
FIGURE 5-3 Classification of epithelia. Epithelial tissues are classified according to the shape of the cell and the way in which the cells are arranged. Stratified epithelial tissues are composed of many layers of cells, and each layer of cells may have a different shape. In these cases, tissue is classified according to the shape of the cells on the surface, in the outermost layer. (From Patton KT, Thibodeau GA: Anatomy & physiology, ed 8, St Louis, 2013, Mosby.)
3. Presence of surface specializations. Terms for surface specializations, such as “cilia” and “keratinized,” may be added to the classifications of epithelia to indicate an increased level of specialization. Stratified squamous epithelium, for example, may be classified as keratinized stratified squamous epithelium (found in the skin) or nonkeratinized stratified squamous epithelium (found in the lining of the mouth).
TYPES OF EPITHELIA
SIMPLE SQUAMOUS EPITHELIUM
Simple squamous epithelia are delicate and thin. They are often found lining surfaces involved in the passage of either gas or liquid, for example in the inner lining of the lung, where oxygen is absorbed and carbon dioxide released, and in the filtration membranes of kidneys, where water and other small molecules are excreted as urine (Figure 5-4). The fragile nature of simple squamous epithelium requires that it occur only in protected regions of the body, such as in the lining of the chest and abdominal cavities. Because simple squamous epithelia are flat and smooth, they are important in reducing friction and are found in the lining of blood and lymphatic vessels. Simple squamous epithelia have been given special names depending on where they are located in the body. For example, the epithelium that lines the pleural (chest), pericardial (around the heart), and peritoneal (abdominal) cavities is called mesothelium. The epithelium that lines blood and lymphatic vessels is called endothelium.
SIMPLE CUBOIDAL EPITHELIUM
Simple cuboidal epithelium is composed of a single layer of cubic cells (Figure 5-5). On microscopic examination, their round, dark-staining nuclei are seen to be aligned in a single row that resembles a string of pearls. Like simple squamous epithelium, simple cuboidal epithelium provides little protection from abrasion. Therefore it occurs in sheltered regions of the body, where secretion and absorption take place. It is found on the surface of ovaries, in the secretory portions of glands, such as the thyroid, and in the lining of
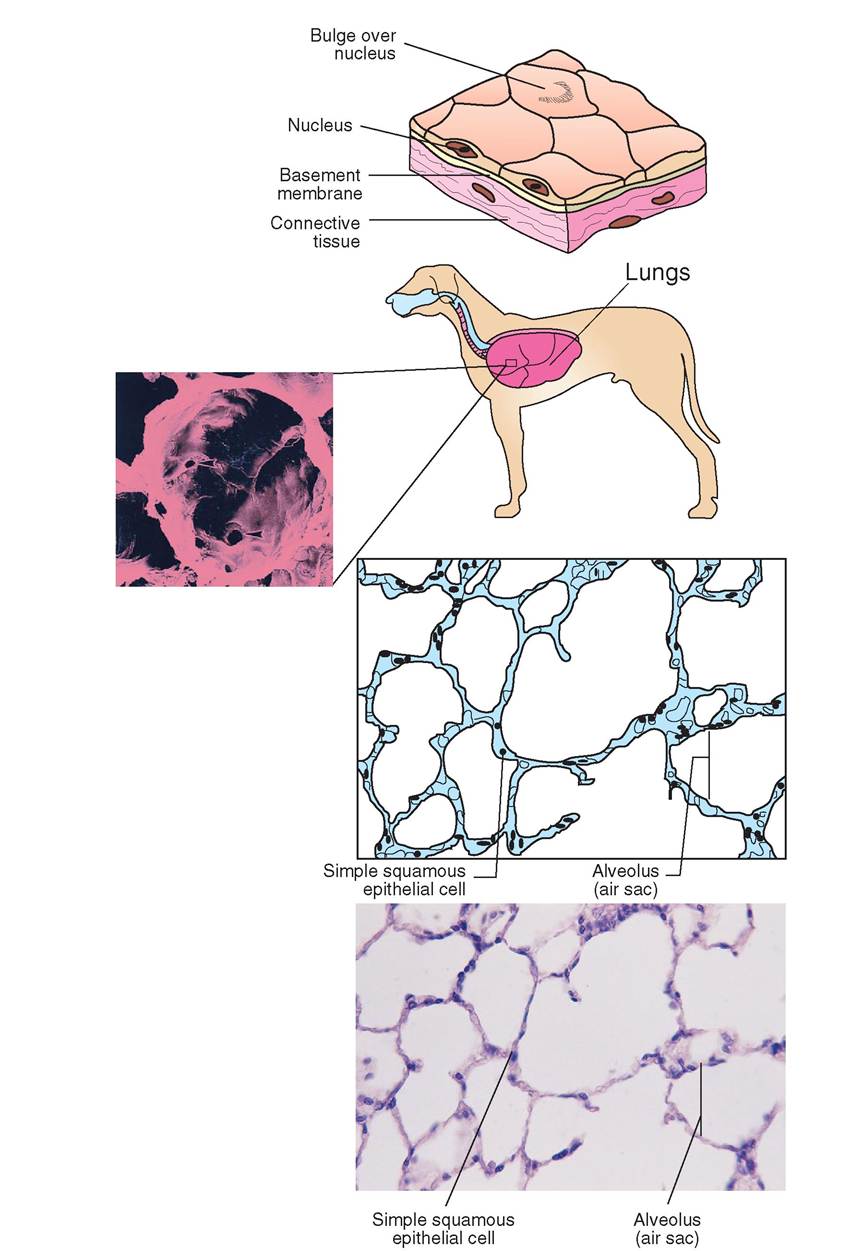
FIGURE 5-4 Simple squamous epithelium. Description: A single layer of flattened, hexagon-shaped cells. The nuclei are disc shaped and centrally located. They often appear as raised bumps in the center of the flattened cell, giving cells a 'fried-egg' appearance. Location: Alveoli of lungs, lining in blood and lymphatic vessels, lining in heart and major body cavities, filtration units (glomeruli) in kidney. Function: In regions of the body where protection is not important, simple squamous epithelium allows diffusion, filtration, secretion, and absorption. Microanatomy: Photomicrograph and sketch of simple squamous cells that compose the walls of air sacs in the lung. The scanning electron micrograph depicts the threedimensional nature of living lung tissue. (Courtesy Barbara Cousins and Ed Reschke.)
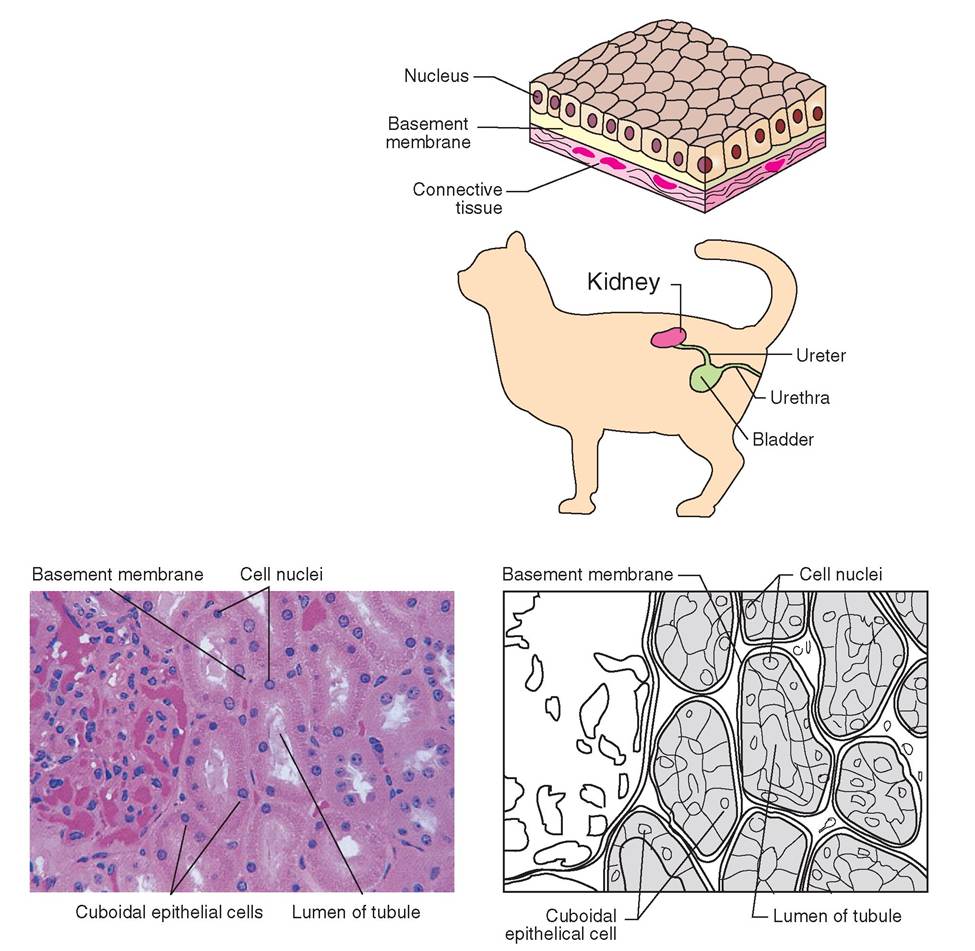
FIGURE 5-5 Simple cuboidal epithelium. Description: A single row of tightly packed, cubelike cells, each of which contains a round, centrally located nucleus. Location: Tubules of kidney; terminal bronchioles in lungs; choroid plexus of brain, glands, and their ducts; surface of ovaries. Function: Cells in kidney are engaged in absorption and secretion; cells in bronchioles are ciliated and assist with movement of particles away from lungs. Cells in choroid plexus and in glands secrete substances. Microanatomy: Photomicrograph and sketch of micrograph show a layer of simple cuboidal epithelium lining the lumen of tubules in the kidneys. (Courtesy Robert Calentine.)
the ducts of the liver, pancreas, kidney, and salivary glands. Some simple cuboidal epithelia in kidney tubules are covered with microvilli, attesting to their absorptive function. Others are smooth surfaced and associated with secretory glands.
Simple cuboidal epithelium plays an important role in both endocrine and exocrine tissues. Exocrine ducts lined with simple cuboidal epithelium, for example, carry saliva from the salivary gland to the oral cavity, and enzymes secreted by the pancreas are transported to the duodenum. In addition the thyroid gland, an endocrine structure, contains chambers lined by a single row of cuboidal cells and secretes the hormone thyroxine, which is carried throughout the body via the bloodstream.
SIMPLE COLUMNAR EPITHELIUM
Simple columnar epithelia are elongated and closely packed together, making the epithelia relatively thick and more protective than the simple squamous and cuboidal epithelia (Figure 5-6). The nuclei are not centrally located, as they are in cuboidal cells, but rather are aligned in a row at the base of the cell near the basement membrane. Simple columnar epithelia line the length of the gastrointestinal tract from the
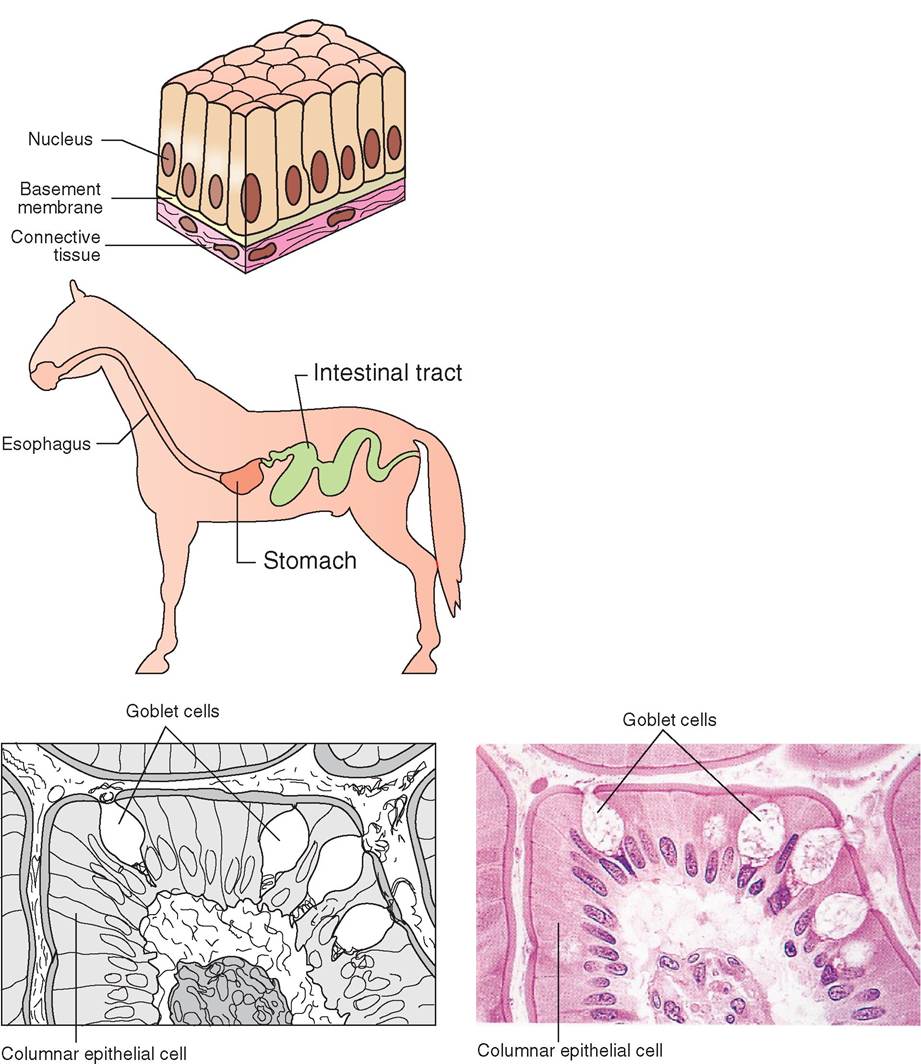
FIGURE 5-6 Simple columnar epithelium. Description: A single row of tall, slender cells with oval nuclei. The surface may or may not be ciliated. Goblet cells can be seen interspersed among the cells. Location: The nonciliated variety lines the digestive tract from stomach to rectum, including the gallbladder and the excretory ducts of some glands; ciliated cells are found in uterine tubes, uterus, and small bronchi of the lungs. Function: Absorption in intestine and secretion in stomach, glands, and intestines. Ciliated cells assist with movement of particles out of the lungs and with movement of the oocyte through uterine tubes. Microanatomy: Photomicrograph and sketch of micrograph show simple columnar epithelium lining the stomach. Notice the goblet cells, which produce mucus. (Courtesy Ed Reschke.)
stomach to the rectum. Like simple cuboidal, they are associated with absorption and secretion and are found in many excretory ducts, as well as in the digestive tract.
Two types of cell make up the gut lining. The most numerous is the absorptive cell, wfee apical surface is Tlanketed by dense microvilli that maximize absorption by increasing surface contact with the nutrient-filled lumen. The other cell is called a goblet cell bacaiise of its wineglass shape. Goblet cells manufacture and store lubricating mucus that is secreted onto the luminal surfaces of the epithelia.
Some less common epithelia are covered with cilia on their apical surfaces. These cells are called simple ciliated columnar epithelia, and they line the uterine tubes and respiratory tracts.
STRATIFIED SQUAMOUS EPITHELIUM
Stratified squamous epithelium consists of various cell layers (Figure 5-7). It occurs in regions of the body that are subject to mechanical and chemical stresses, such as the linings of the mouth, esophagus, vagina, and rectum. The epithelial cells that make up the outer surface are continually being worn away or sheared off, but they are replaced at an equal rate by cells from deeper layers. Cuboidal cells form the base of stratified squamous epithelium. They are attached to the basement membrane and are continually dividing to keep up with the cell losses from the luminal surface. As the young cuboidal cells mature, they are progressively pushed to the surface, away from the nutrient sources provided by the underlying connective tissue. During this movement, the cells lose their cytoplasm and nuclei, take on a squamous shape, and eventually become paperlike sheets that slough.
STRATIFIED CUBOIDAL EPITHELIUM
Stratified cuboidal epithelium generally occurs as two layers of cuboidal cells and is found primarily along large excretory ducts, such as those of sweat glands, mammary glands, and salivary glands (Figure 5-8). This type of epithelium is important in protecting the delicate tissues in deeper layers.
STRATIFIED COLUMNAR EPITHELIUM
Stratified columnar epithelium is rare and is found only in select parts of the respiratory, digestive, and reproductive systems and along some excretory ducts (Figure 5-9).
PSEUDOSTRATIFIED COLUMNAR EPITHELIUM
Pseudo- means “false,” therefore pseudostratified columnar epithelium is an epithelial layer that is not truly stratified. The epithelial cells appear to be stratified because the nuclei are found at different levels across the length of the tissue layer. However, not all of the cells reach the luminal surface, so cells appear to be at different levels as though stratified. In reality, each cell forms a distinct attachment, however subtle, with the basement membrane. In this way, pseudostratified columnar epithelium forms a single layer and therefore is considered a simple epithelium (Figure 5-10).
Most pseudostratified columnar epithelium is ciliated and is found in the respiratory tract and in portions of the male reproductive tract. In the trachea, for example, the epithelium is coated with a layer of mucus that is propelled by cilia across the luminal surface toward the mouth. This assists in preventing debris from entering the lungs. The mucus is also fortified with protective immunoglobulins, which are disease-fighting molecules that help to protect animals from pathogens (bacteria and viruses) that have been inhaled.
TRANSITIONAL EPITHELIUM
Transitional epithelium has the remarkable ability to stretch. It is found in regions of the body that are required to expand and contract as part of their normal function. Thus transitional epithelium is found in portions of the urinary tract where great changes in volume occur, such as the urinary bladder, ureters, urethra, and calyxes of the kidney. The histologic appearance of transitional epithelia varies, depending on how much it is stretched. For example, in an empty bladder the epithelium is thick, multilayered, and has rounded, domelike cells on the luminal surface. When the bladder is filled, greater pressure is applied to the epithelial layer, making it stretch and thin out. The extent to which the membrane stretches depends on how full the bladder is and how much force is applied to the epithelium. As epithelia stretch, they may thin out from six to three cell layers, and the apical cells become flattened and squamous. The ability of transitional cells to change shape in the urineholding tissues allows greater volumes of urine to be transported, stored, and excreted (Figure 5-11).
In addition to its ability to stretch, transitional epithelium forms a leak-proof membrane that prevents the diffusion of potentially scalding urine into the delicate environment of the abdominal cavity.
TEST YOURSELF 5-2
1. Epithelial tissue is characterized as simple, stratified, or pseudostratified. What does this mean?
2. What are the three basic shapes of epithelial cell?
3. Draw a picture of each of the following types of epithelia and give an example of where each of them can be found in the body.
• Simple squamous
• Simple cuboidal
• Simple columnar
• Stratified squamous
• Pseudostratified columnar
• Transitional
GLANDS
A gland is a cell or group of cells that have the ability to manufacture and discharge a secretion. Secretions are specialized protein molecules that are produced in the rough endoplasmic reticulum, packaged into granules by the Golgi apparatus, and discharged from the cell. Thus typical glandular epithelial cells are recognized by their prominent endoplasmic reticulum, Golgi apparatus, and secretory granules. Some of the secretions produced by glandular epithelia are used locally, whereas others are needed in distant regions of the body.
During embryonic development, multicellular glands form from an infolding layer of epithelial cells. Initially, these invaginations form ducts and tubules that maintain contact with the surface epithelium. In the course of development, some of the glands lose the ducts and become separated from
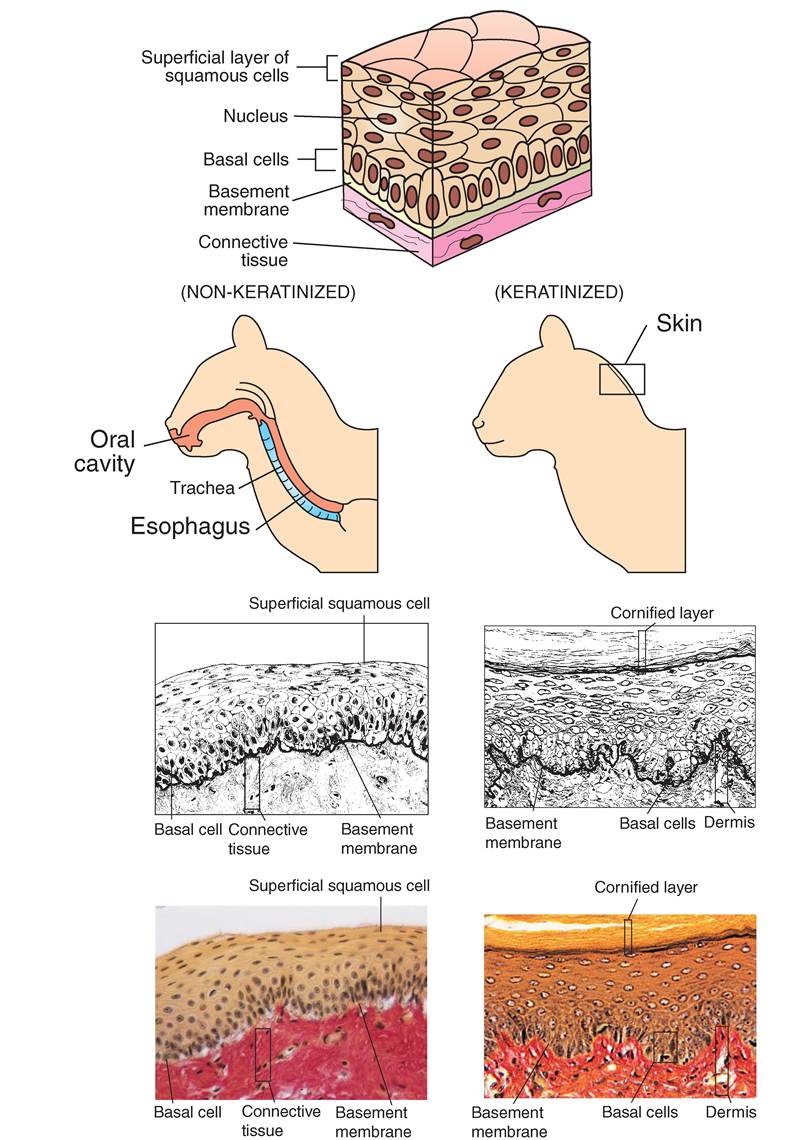
FIGURE 5-7 Stratified squamous (keratinized and nonkeratinized) epithelium. Description: A multilayered tissue in which cells along the basement membrane are metabolically active and dividing. These basal cells are cuboidal or columnar, and as they mature they are pushed to the surface, lose their organelles, and flatten into thin flakes. In skin, maturing cells fill with keratin. Location: Nonkeratinized epithelium is found lining the mouth, esophagus, and vagina. Keratinized cells are found in epidermis, the superficial layer of the skin. Function: In areas that are prone to abrasion, stratified squamous epithelium protects underlying tissues. Microanatomy: Photomicrograph and sketch of micrograph show nonkeratinized squamous epithelium lining the mouth and esophagus in a cat. Photomicrograph and sketch of micrograph show keratinized stratified squamous epithelium in the epidermis of skin. (Courtesy Ed Reschke.)
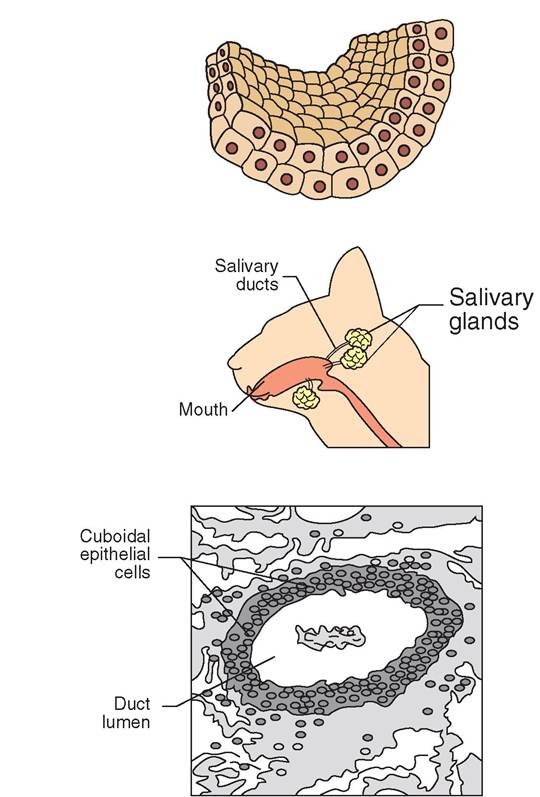
FIGURE 5-8 Stratified cuboidal epithelium. Description: Generally, two layers of cuboidal cells. Location: Ducts of mammary glands, sweat glands, and salivary glands. Function: Secretion, absorption, and protection. Microanatomy: The sketch shows stratified cuboidal epithelia in a salivary gland.
the parent epithelial sheet (Figure 5-12). In this way, glands are derived from epithelium.
Glands can be classified in many ways. For example, we can organize them based on the following factors:
1. Presence or absence of ducts (endocrine or exocrine).
2. Number of cells that compose them (unicellular or multicellular).
3. Shape of the secreting ducts (simple or compound).
4. Complexity of the glandular structure (tubular, acinar, or tubuloacinar).
5. Type of secretion they produce (mucoid or serous).
6. Manner in which the secretion is stored and discharged (merocrine, apocrine, or holocrine).
Each of these classifications is discussed.
ENDOCRINE GLANDS
Glands that do not have ducts or tubules and whose secretions are distributed throughout the body are called
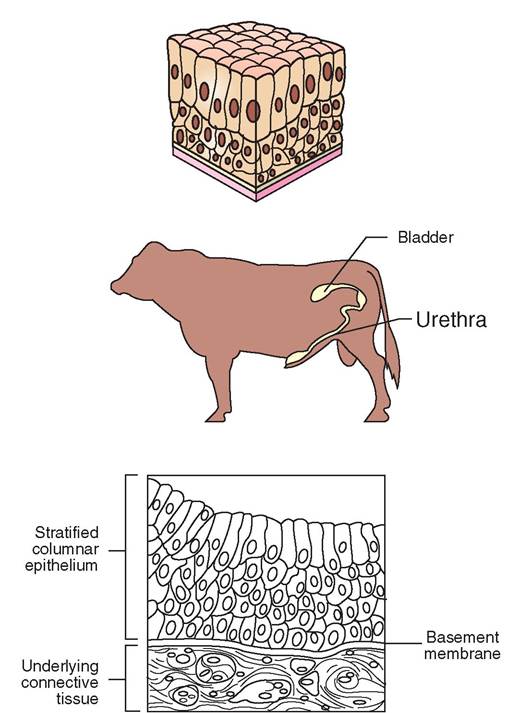
FIGURE 5-9 Stratified columnar epithelium. Description: Several layers of cells in which basal cells are cuboidal and superficial cells are columnar. Location: Large ducts of mammary glands and small portion of the urethra of some male animals. This type of epithelium is rare. Function: Secretion and protection. Microanatomy: Stratified columnar epithelium in the urethra.
endocrine glands. They produce and secrete regulatory chemicals, known as hormones, into the bloodstream or the lymphatic system, where they are carried to many regions of the body. Endocrine glands are part of a complex, biochemical network known as the endocrine system. The pituitary gland in the brain and the adrenal gland near the kidney are examples of endocrine glands. The endocrine system and the glands it includes are discussed in detail in Chapter 11.
EXOCRINE GLANDS
With the exception of the goblet cell, exocrine glands possess ducts. They are more common than endocrine glands and act by discharging secretions via their ducts directly into nearby areas where they may, for example, cover cell surfaces or empty into body cavities. Unlike those of endocrine glands, the secretions of exocrine glands act locally and do not normally enter the circulation. A wide variety of exocrine glands are found in animals, including hepatoid, musk, sweat, and salivary glands. Other examples can be found in the liver and pancreas, where exocrine glands secrete bile
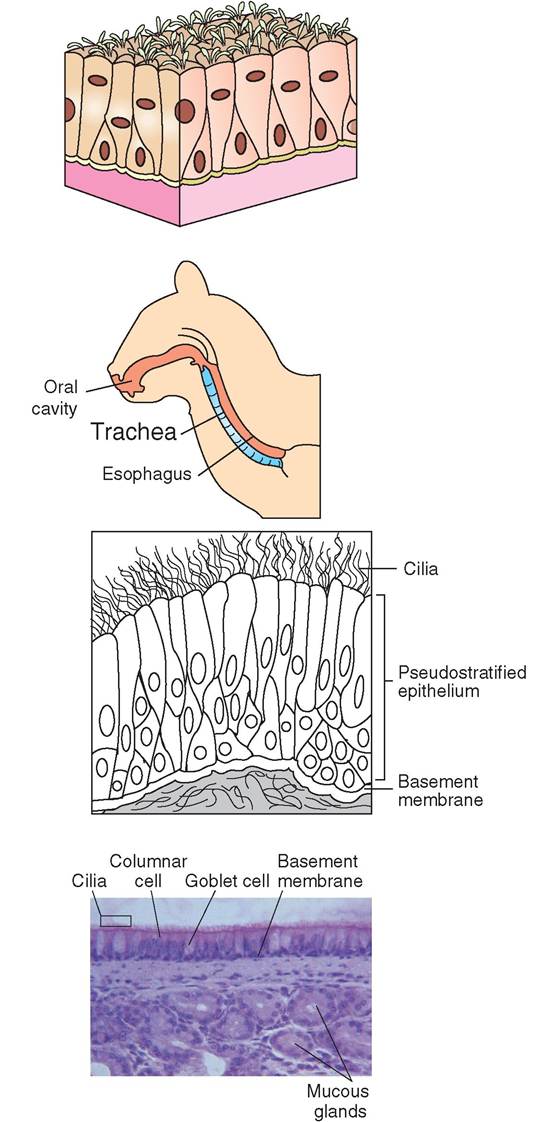
FIGURE 5-10 Pseudostratified epithelium. Description: Pseudostratified epithelia appear stratified but are not. Each cell is attached to basement membrane, but not all of them reach the luminal surface. Cells vary in shape and height. Their nuclei occur at different distances from the basement membrane. Cells are generally ciliated and are often associated with goblet cells. Location: Respiratory tract, including nasal cavity, larynx, pharynx, trachea, and bronchi. Function: Surface layer of mucus traps particles, which are moved away from the lungs by beating cilia. Microanatomy: Photomicrograph and sketch of micrograph show ciliated pseudostratified epithelium lining the trachea. Note the goblet cells that secret protective mucus. (Courtesy Robert Calentine.)
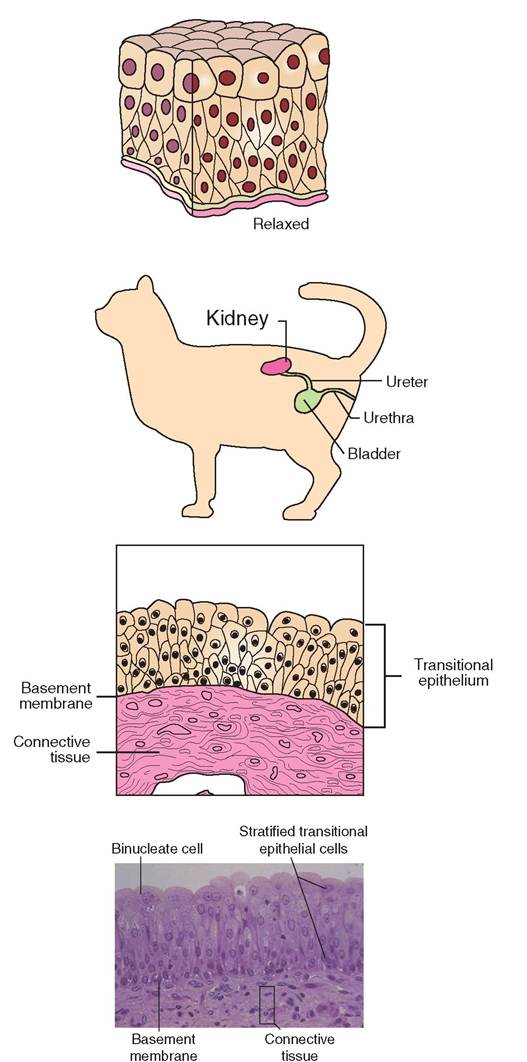
FIGURE 5-1 1 Transitional epithelium. Description: Stratified epithelium in which the basal layer is composed of cuboidal or columnar cells. The superficial layer is composed of cuboidal or squamous cells, depending on level of distension of the tissue. Location: Urinary bladder, ureters, and urethra. Function: Transitional epithelium is flexible to accommodate fluctuations in amount of urine in bladder, ureters, and urethra. It forms a permeable barrier that holds liquid and protects underlying tissues from caustic effects of urine. Microanatomy: Photomicrograph and sketch of micrograph show transitional epithelium in the bladder of a cat. Notice that the shape of the cells is highly variable and that the superficial layers do not touch the basement membrane, making this a type of stratified epithelium. The epithelium changes (transitions) and is compressed as the bladder fills. (Courtesy Ed Reschke; from Thibodeau GA, Patton KT: Anatomy & physiology, ed 6, St Louis, 2007, Mosby.)
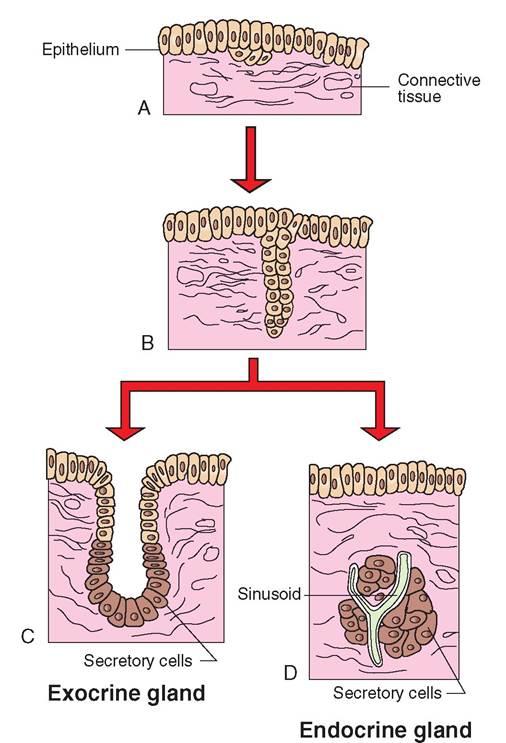
FIGURE 5-12 Development of glands. A and B, Exocrine and endocrine glands develop from epithelium during the maturation of a fetus. Surface epithelial cells grow down into the underlying connective tissue. Exocrine glands develop when the connections between deep and superficial layers of cells form a duct. C, The deepest cells become secretory. Endocrine glands form when connecting cells die. D, Secretions of the gland are transferred to sinusoids and then into the circulatory system, rather than through a duct.
and digestive enzymes, respectively. The pancreas possesses endocrine and exocrine properties because it is responsible for producing many hormones and for secreting digestive enzymes.
UNICELLULAR EXOCRINE GLANDS. The only example of a unicellular exocrine gland is the ductless goblet cell, so named because of its resemblance to a drinking goblet (Figure 5-13). The goblet cell is a modified columnar epithelial cell and is found interspersed among the columnar cells of the respiratory and digestive tracts and in the conjunctiva of the eye. Goblet cells secrete mucin: a thick, sticky mixture of glycoproteins and proteoglycans that when mixed with water becomes mucus. The mucus functions in two ways: it helps protect the apical surface of the epithelial layer, and it assists with the entrapment of microorganisms and foreign particles.
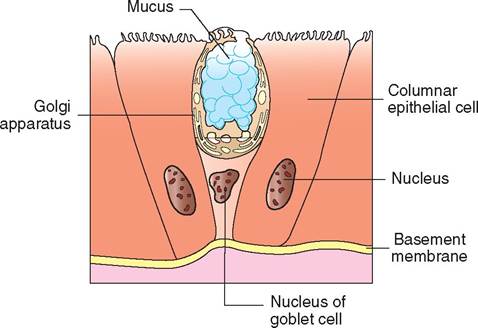
FIGURE 5-13 Goblet cell. A unicellular goblet cell occurs among simple and pseudostratified epithelia that line the respiratory and digestive tracts. Mucus is contained within the cytoplasm at the luminal end of the cell, and the nucleus is located in the basal end of the cell, near the basement membrane. A goblet cell releases its stored mucus onto the tissue surface.
MULTICELLULAR EXOCRINE GLANDS. Multicellular exocrine glands are made up of two distinct components: a secretory unit in which secretions are produced by secretory cells and a duct that carries the secretion to the deposition site. In most glands the secretory unit is surrounded by connective tissue that is rich in blood vessels and nerve fibers. It not only nourishes the secretory unit but also provides structural support and may extend into the gland to form distinct lobes. In some exocrine glands the secretory unit is surrounded by contractile cells called myoepithelial cells that assist with the discharge of secretions into the glandular duct. The rate of secretion production and discharge is controlled by hormonal and nervous influences.
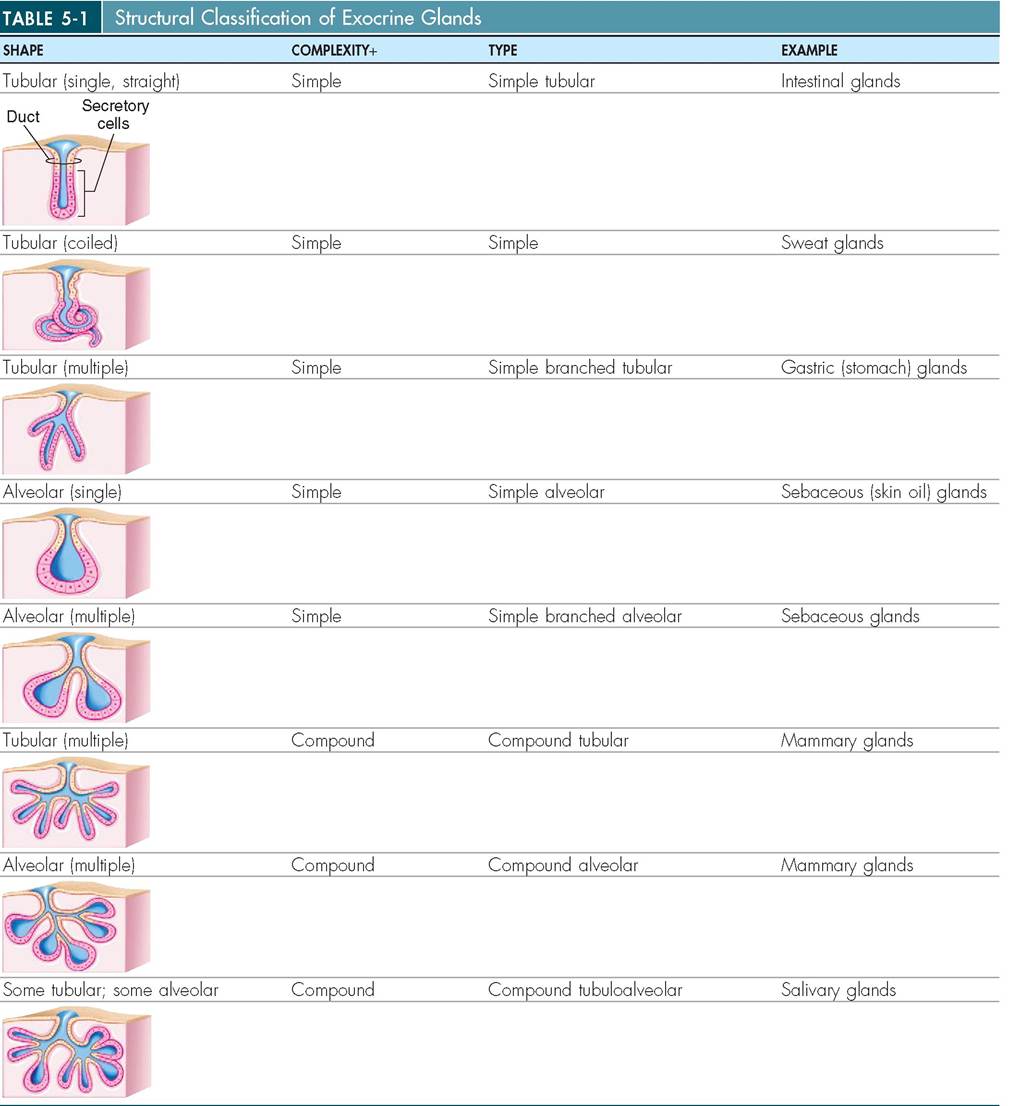
We begin the classification of exocrine glands with examination of the glandular ducts (Table 5-1). If the main duct is unbranched, the gland is considered a simple gland. If the main duct is branched, the gland is called a compound gland. Next, we examine the secretory portions of glands. If the secretory cells form a long channel of even width, the gland is called a tubular gland (Figure 5-14). If the secretory unit forms a rounded sac, the gland is called an alveolar gland or an acinar gland. Glands with secretory units that possess both tubular and alveolar qualities are called tubuloalveolar or tubuloacinar (Figure 5-14).
Glands are classified further according to the way in which they secrete their products. How much of the cell is sacrificed in the act of secretion determines whether the gland is merocrine, apocrine, or holocrine (Figure 5-15). The majority of glands package their secretions into granular units and release them via exocytosis as they are manufactured. These glands are called merocrine glands because the secretory cells remain intact during the secretory process. The pancreas, sweat glands, and salivary glands are examples of merocrine glands. Secretion in apocrine glands involves the loss of the top part of the cell, called the apex of the secretory cell. The secretory cells in apocrine glands do not
(From Patton KT, Thibodeau GA: Anatomy & physiology, ed 8, St Louis, 2013, Mosby.)
release their granules as they are manufactured. Instead, they store the granules until the apex of the cell is full. Then the cell pinches in two and releases the apex into the duct system. Later, the cell repairs the damage and repeats the process. Apocrine glands can be found in mammary tissue and are represented by some sweat glands.
Like apocrine glands, holocrine glands also store granules in the secretory cells until they are needed. However, icnrinheolo glands, the entire secretory cell is destroyed in the act of releasing its secretory product. The subsequent degeneration of the cell allows the release of the granules. nolocr'ine secretion occurs principally in sebaceous glands.
We can also categorize glands according to the type of secretion they produce. Serous secretions are watery and contain a high concentration of enzymes, whereas mucous
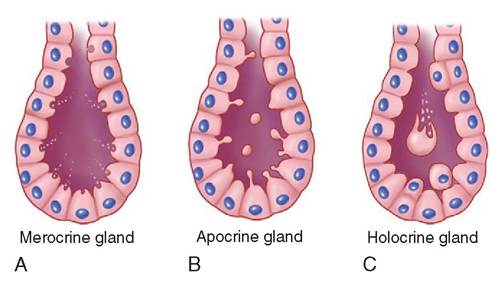
FIGURE 5-15 Secretion styl es of exocrine glands. A, Cells of merocrine glands store substances intended for excretion in vesicles in their cytoplasm. The vesicles are transported to the surface of the cell, where they release their contents. A cell can continue to produce and excrete substances throughout its life and is not in any way harmed by the secretory process. B, Cells of apocrine glands also store secretory substances within vesicles. However, secretion occurs as the luminal end of the cell is detached from the basal portion. Cytosol, inclusions, and other cytoplasmic components are discharged along with the secretory vesicles. The cell must take time to regrow lost portions of itself before it can secrete again. C, Holocrine secretion involves release of the entire contents of the cell. In this process, the cell is killed and is replaced by new cells that have moved up from deeper layers. (From Patton KT, Thibodeau GA: Anatomy & physiology, ed 8, St Louis, 2013, Mosby.)
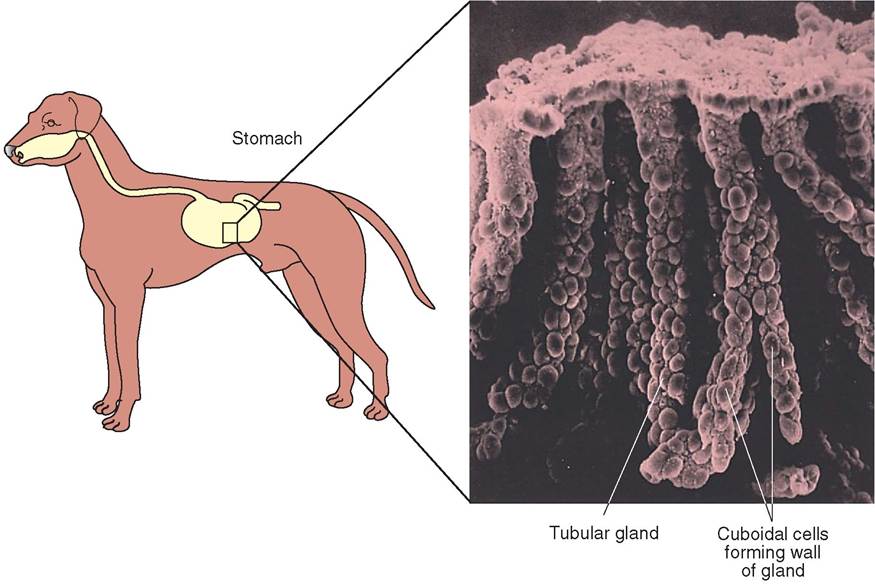
FIGURE 5-14 Tubular exocrine glands in the canine stomach. Exocrine glands are structured in many different ways and occur in diverse regions of the body. In the lining of the stomach exocrine glands occur as simple straight, simple coiled, and compound (or branched) tubular glands. These gastric glands produce a mixture of water, enzymes, acid, and mucus, which together form an important digestive 'juice.'
secretions are thi^k, viscous, and composed of glycoproteins. Secretory cells that manufacture both types of secretion are common in the digestive and respiratory tracts. Mixed exocrine glands coai^nn both mucous and serous components.
TEST YOURSELF 5-3
1. Whicit is α gland?
2. How doglands developembcyologically?
3. Vdhct idthe differegge between ecdoodno and exocrine glands? Ccn you give examples of dcchS
4. Vghere ete gobletsellsfound? W hat typoof secretion do they produce?
5. Ie general, hew are multicellnlar exogrine glands constructed?
6. Con you Oescrieemerosrine,apodrine, ondeolocrine glands? How do they differ from one onother?
7. Howarendreuu oud mcoQuo sodretionsdifferent?
CONNECTIVE TISSUE
GENERAL CHARACTERISTICS
Connective tissue is found everywhere in the body and represents the most abundant tissue type by weight. Some organ systems, such as the skeletal and integumentary systems, are composed almost exclusively of connective tissue, whereas otlhers, such as the neurologic system, contain very little. Connective tissue is derived from mesoderm and, unlife iespsiuteh,elial t is composed primarily of nonliving extracellular maGx. The matrix surrounds and separates the cells, raonvdiditeps important structural and nutritional support that enables connective tissue cells to exist farther apart than epithelial cel Is. In addition, unlike epithelial tissue, which has no direct blood supply, connective tissue is vascularized although the level of vascularity varies among different connective tissue types. Loose connective tissue and adipose connective tissue, for example, possess good blood supplies, whereas dense connective tissue is poorly vascularized.
All connective tissue is composed of three distinct components: extracellular fibers, ground substance, and cells. The mixture of fiber and ground substance is called the extracellular matrix. Variations in the ground substance, fibers, and cellular components have given rise to a wide range of connective tissue types (Figure 5-16). Blood, tendon, fat, cartilage, and even bone are all examples of connective tissue, though their textures and appearances are different. Variations in the type of ground substance and in the type of fiber enable the tissue to take on many different qualities. It can be elastic and flexible, rigid, semisolid, or liquid. Blood, for example, is a highly cellular connective tissue with a liquid matrix containing relatively little fiber. In contrast, bone is composed of a solid calcified matrix. Tendon contains a matrix that is primarily fibrous with little ground substance. These variations give connective tissue the ability to withstand a wide range of forces, such as direct pressure, abrasion, and shearing forces that would destroy other tissue types.
As with all living structures, form and function are intertwined. Thus the plethora of forms that characterize connective tissue give rise to a wide range of functions. In general, as its name implies, connective tissue forms metabolic and structural connections between other tissues; however it serves many other important roles as well. For example, connective tissue forms a protective sheath around organs and helps insulate the body. It acts as a reserve for energy, provides the frame that supports the body, and composes the medium that transports substances from one region of the body to another. In addition, connective tissue plays a vital role in the healing process and in the control of invading microorganisms.
COMPONENTS OF CONNECTIVE TISSUE
The major components of connective tissue are summarized in Box 5-1.
GROUND SUBSTANCE
The ground substance in connective tissue is an amorphous, homogeneous material that ranges in texture from a liquid or gel to a calcified solid. In soft connective tissues, it
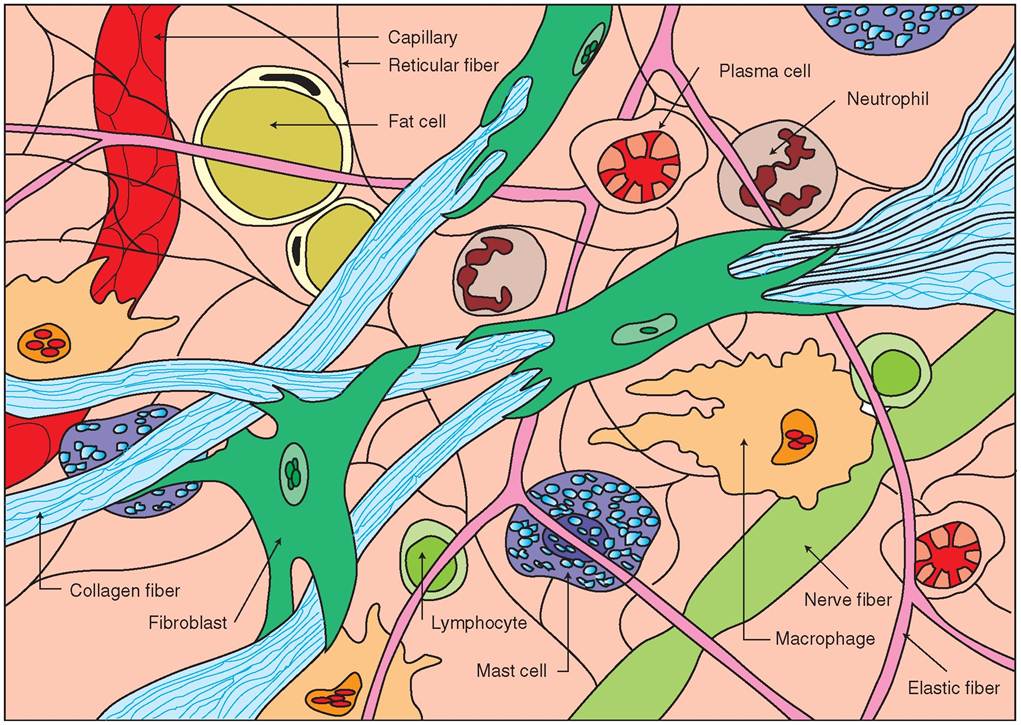
FIGURE 5-16 Loose or areolar connective tissue. Loose or areolar tissue is a model-type of connective tissue because it contains all three types of fiber (elastic, collagen, and reticular) and a wide variety of cells (lymphocytes, mast cells, neutrophils, fibroblasts, adipocytes, and plasma cells) suspended in ground substance. These three components—fibers, cells, and ground substance—are found in varying amounts in all connective tissue.
BOX 5-1 Major Components of Connective Tissue
Ground Substance
Ranges from liquid to gel to solid
Fibers
Collagenous
Reticular
Elastic
Cells
Fixed cells
Fibroblasts
Adipocytes (fat cells)
Reticular cells
Wandering cells
Mast cells
Leukocytes (white blood cells)
Macrophages (fixed and wandering)
is composed of unbranched chains of glycoproteins called glycosaminoglycans (GAGs). The most commonly found GAG in connective tissue is hyaluronic acid combined with 2% pnotein. These large molecules help to orient the formation of fibers within the tissue.
Ground substance is the medium through which cells exchange nutrients and waste with the bloodstream. It acts as a shock-absorbing cushion and helps to protect the more delicate Wls that it envelops. In addition, its thick texture serves as an effective obstacle for invading microorganisms, although some microbes have developed the ability to produce the enzyme hyaluronidase, which degrades hyaluronic Wd and enables the microbe to move Wfi greater eoausgehthr the tissue.
FIBERS OF CONNECTIVE TISSUE
Connective tissue contains three types of fiber: collagenous, reticular, and elastic, hlthc>ιιgh these fibers exist in all con- insescutei,ve t their proportions vary from one type of connective Mue to another. Collagenous fibers are by far the ommosmt ocnly found in the body.
Collagenous fibers arn strong, thick strands composed of trhuec tsutral protein collagen. Collagen fibers are organized
into discrete bundles of long, parallel fibrils, which in turn are comdosed of bundled microfibrils. Because they possess tremendous tensile strength, enabling them to resist pulling forces, collagenous fibers are found in tendons and ligaments that are continually being pulled and stretched. When not undor ⅛'on, collagenous fibers look wavy. The fiber ihtisteel,f is w and the tissue it forms when the fibers are lpoasceklyed c together is also white. Therefore it is not surprising that collagenous fibers are sometimes known as the white fibers.
The yensity and arrangement of collagen fibers can vary depending on the function of the tissue as a whole. Collag- eononuesctcive tissue can range from loose, as in the loose
connective tissue that surrounds and protects organs, to
dense arrangements seen in tendons. The tissue forms when rcotlleaingesn p are secreted into the extracellular environ
ment, where they are arranged into formation. If subjected toollahgeeant, c denatures and turns into a soft gel. This is whh meat, which is rich with collagenous fibers, softens when aooked for long periods in soups and stews. At the same toilmlaeg,ecn can be fortified with tannic acid, as is evident irn leathe that has been strengthened by tanning.
Reticular fibers, IIOc collagenous fibers, are composed of collagen, Wt they are not thick. Instead, they are thin, delicate, end branched into complicated networks. Reticular fibers Mm a kind of “mist net” (rete is Latin for net) that uprpopvoirdtes s for highly cellular organs, such as endo- lcarnindes,g lymph nodes, spleen, bone marrow, and liver. eRresticular fib are also found around blood vessels, nerves, emrsu,scle fib and capillaries.
Elastic fibers are cemposed primarily of the protein elastin. Lik reticular fibers, elastic fibers are branched and foomrmplecx networks, but they lack the tensile strength of collagenous fibers. Elastic fibers are composed of bundles of microfibrils, and because they are coiled, they can stretch aondtrcact like a rubber band. Therefore elastic fibers tend
to oκur in tissues that are commonly subjected to stretch- iuncgh, s as the vocal cords, lungs, skin, and walls of blood evceassuesles. B of their color, elastic fibers are sometimes referred to as the yellow fibers.
MAJOR CELL TYPES
oAnltnheocutigvhe c tissue contains a wide variety of cell
tyypes, the can be organized into two major categories: those that remain in the connective tissue, called fixed cells, and those that pass in and out of the connective tissue, called transient cells, dixed Wls remain in the connective tissue and auraellyus involved in the production and maintenance of trhixe. mat Transient cells, however, do not have a perma- enseindte nrce in the tissue but move in and out of it as
rnaenesdiedn.t T cells generally are involved in the repair
raontdecption of the tissue.
FIXED CELLS. The most noteworthy fixed cell is the fibroblast.ehTese ar large, irregularly shaped cells that manufacture and secrete both the fibers and the ground substance characteristic of their particular matrix. Fibroblasts ecapnrorduce and are metabolically very active. Each type ofncnective tissue is characterized by a predominant fibro- xlast. For exam pie, cartilage contains chondroblasts, bene contains osteoblasts, nnd connective tissue contains fibro- sblasts. A the cells mature and the matrix is formed, the cells adopt a less active role. When this occurs, the name of the cell adopts the suffix -cyte, for examp 1 e chondrocyte, osteocyte, Ot fibrocyte, denrending on the tissue in which they are found. If additional matrix is required later, the cells can convert back to the -blast form.
eFlalts c ar found throughout connective tissue and are known as adipose cells or adipocytes. An young cells, adi- epsoecmytbelse r fibroblasts, but as they mature, they fill
with lipid and become swollen, with their nuclei pushed to one side. When adipocytes cluster into groups, they become a tissue in their own right, known as adipose tissue. Adipose tissue is found throughout the body but is particularly evident under the skin (particularly on the ventrum between the hind legs in cats), behind the eyes, around the kidneys, and in the omentum of the abdominal cavity.
Reticular cells are flat, star-shaped cells with long, out- reaching arms that touch other cells, forming netlike connections throughout the tissue they compose. The function of reticular cells is debated, but most agree that they are involved in the immune response and in the manufacture of reticular fibers. It is not surprising therefore that reticular cells are found primarily in tissues that are part of the immune system, such as lymph nodes, spleen, and bone marrow.
WANDERING CELLS. There are many types of wandering cell that move in and out of connective tissue as needed. In this section, three common types of wandering cells are discussed: leukocytes, mast cells, and macrophages.
Commonly known as white blood cells, leukocytes are found in blood and move into connective tissue in large numbers during times of infection. Although they are relatively large and round compared to red blood cells, they can squeeze through the walls of tiny blood vessels to enter the surrounding tissue. This process is called diapedesis. Leukocytes are important members of the defensive immune system. There are five different types of leukocyte, but most protect the body by engulfing and digesting invading microbes. Other kinds, however, defend against infection by manufacturing antibodies that attach to microbes and destroy them.
Mast cells are oval cells that are easily identified by the large number of dark-staining granules stored in the cytoplasm. These granules contain histamine and heparin, potent biochemicals that initiate an inflammatory response when released into the tissue. Histamine increases blood flow to the area by making the capillaries leaky, and heparin prevents blood from clotting and ensures that the pathways for increased blood flow remain open. Mast cells tend to be found near blood vessels, where they can release their contents directly into the bloodstream and where they can most effectively guard against foreign proteins or microbes. When stimulated by the presence of these invaders, mast cells burst open, releasing hundreds of stored granules. This begins the complex events of allergic and inflammatory reactions, a process discussed in greater detail later in this chapter.
Macrophages are massive, irregularly shaped phagocytizing scavengers that may be either fixed or transient in connective tissue. They engulf microbes, dead cells, and debris that are subsequently digested in the macrophage's lysosomes. Mobile macrophages are drawn to sites of infection or inflammation, where they move aggressively through the affected area to engulf microinvaders. In this way, they are an important part of the immune system and help tissues fight infection. Macrophages are given different names depending on the tissue. For example, they are called Kupffer cells in the liver, microglial cells in the brain, and histiocytes in loose connective tissue.
TEST YOURSELF 5-4
1. How are connective tissue and epithelial tissue similar? How are they different?
2. What are the three basic constituents of connective tissue?
3. List seven functions of connective tissue.
4. What are GAGs and what role do they play in connective tissue? Why do you suppose animals with joint injuries are sometimes given dietary supplements of GAGs?
5. Compare and contrast collagenous, reticular, and elastic fibers.
6. What are fibroblasts and what role do they play in connective tissue?
7. Can you give three examples of cells that are transient in connective tissue? Can you describe their form and function?
TYPES OF CONNECTIVE TISSUE
As already mentioned, all connective tissue is made up of three major components:
• Ground substance
• Cells
• Fibers
Many different types of connective tissue are formed by the variety of textures of ground substance, the number and type of cells, and the number and type of fibers present in the tissue. By varying the three major constituents, a wide range of connective tissue types is generated.
In general, connective tissue is divided into two broad categories: connective tissue proper and specialized connective tissue.
CONNECTIVE TISSUE PROPER
Connective tissue proper is the largest classification and contains every subtype of connective tissue except bone, cartilage, and blood. The two subclasses of connective tissue proper are loose connective tissue and dense connective tissue. Loose connective tissue includes areolar, adipose, and reticular tissue; dense connective tissue includes dense regular, dense irregular, and elastic tissue.
LOOSE CONNECTIVE TISSUE
AREOLAR TISSUE. Areolar connective tissue is a beautiful tangle of randomly placed fibers and cells suspended in a thick, translucent ground substance (Figure 5-17). The tissue appears relaxed with a myriad of round and star-shaped cells placed among crisscrossing fibers. The predominant cell is the fibroblast, a large spindle-shaped cell that manufactures the elastic, reticular, and collagenous fibers found throughout the tissue. Areolar tissue acquires its name from the Latin areola, which means small, open space.
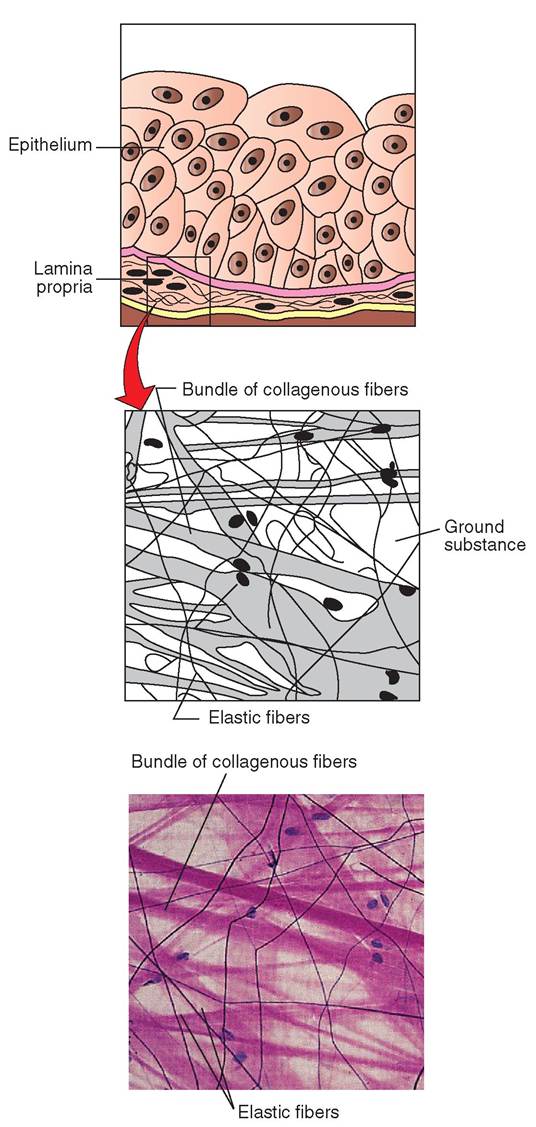
FIGURE 5-17 Loose or areolar connective tissue. Description: Loose array of fibers suspended in gel-like ground substance. Includes all three types of fiber and many cells, such as macrophages, fibroblasts, mast cells, and some white blood cells. Location: Throughout the body, under epithelial basement membranes; between glands, muscles, and nerves; surrounding capillaries and many organs. It is also found under skin and helps to attach it to underlying tissues. Function: Provides nutrients to tissues that it surrounds and supports. Important as a loose packing material. Microanatomy: Photomicrograph and sketch of loose areolar tissue, which serves as soft padding for many organs. The staining turns the collagen fibers pink and the elastin fibers purple. (Courtesy Ed Reschke.)
Areolar tissue is the most common type of connective tissue and is found everywhere in the body. It acts generally as packing material to support and cushion organs and other delicate structures of the body. It surrounds every organ; forms the subcutaneous layer that connects skin to muscle; envelops blood vessels, nerves, and lymph nodes; and is present in all mucous membranes as the lamina propria and submucosa. It is supportive to body structures but is flexible and soft to enable organs the freedom to move within their position. Thus areolar tissue is moderately elastic but tears easily compared with the other types of connective tissue.
The small, open spaces in areolar tissue are filled with a mixture of body fluids and ground substance. The ground substance is thick and is composed primarily of hyaluronic acid, which serves as a medium through which nutrients, gases, and waste can be easily transported to and from the bloodstream. In addition, the viscous texture of the ground substance is an effective barrier against most invading microorganisms, because it inhibits their movement through the tissue. Some white blood cells have developed the ability to produce hyaluronidase, an enzyme that liquefies the matrix and allows white blood cells to pass through with greater ease. This adaptation has improved the ability of white blood cells to perform their duties in loose connective tissue. Unfortunately, some microbes have also developed the ability to produce hyaluronidase, which facilitates the spread of infection throughout the tissue.
During trauma or other pathologic states, the spaces in loose connective tissue can fill with an excessive amount of body fluid. This condition is called edema, and the connective tissue is said to be edematous. You can see this condition in cats that have a swollen paw caused by an insect bite or in dogs that have fractured a bone in their leg. Sometimes, the edema will remain compressed in an area after pressing on it with your thumb. This is called pitting edema because the tissue, rather than springing back after being compressed, leaves impressions or pits in the tissue.
ADIPOSE TISSUE. Adipose tissue is commonly known as fat. It is areolar tissue in which adipocytes or fat cells predominate (Figure 5-18). Adipose tissue is found beneath the skin, in spaces between muscles, behind the eyeballs, on the surface of the heart, surrounding the joints, in bone marrow, and in the omentum of the abdomen. Its cells expand and wither depending on the amount of lipid that is being stored within them. Not surprisingly, the rate of lipid storage and use is based on the amount of calories being consumed by the animal relative to the amount of energy exerted. In addition the sympathetic nervous system, certain hormones, and genetic influences may also profoundly affect fat metabolism. Adipose tissue is highly vascularized so that the lipid droplets contained within adipocytes are accessible to the enzymes responsible for triglyceride breakdown and to a bloodstream that readily transports the glycerol and free fatty acid products to other parts of the body. Thus adipose tissue represents an important energy store for animals. It also acts as a thermal insulator under the skin, prevents heat
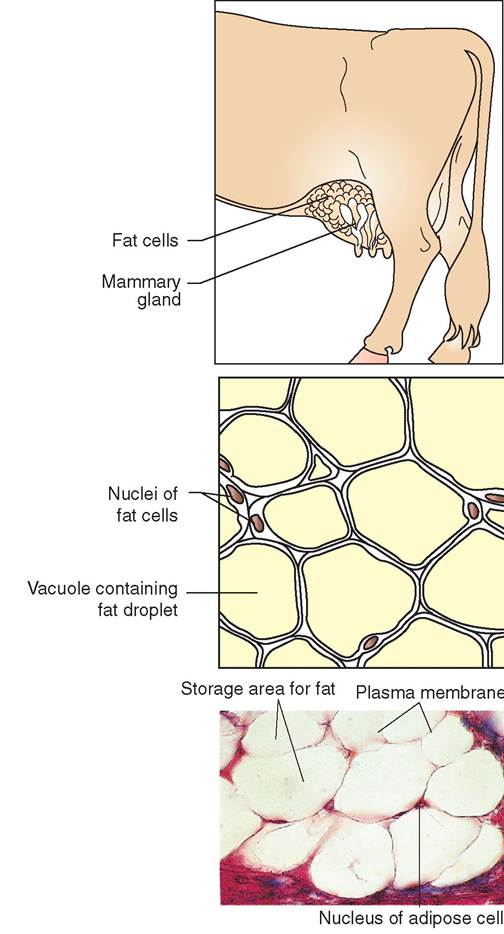
FIGURE 5-18 Adipose tissue. Description: Adipose tissue is fat. The tissue has little extracellular material and is composed primarily of closely packed adipocytes filled with lipid. The nucleus is pushed to the periphery of each cell to accommodate sizable lipid stores. Location: Throughout the body, under skin, around heart and kidneys, within mesenteries and omentum, and around the colon. Function: Thermoinsulator; protects organs and other tissues it surrounds. Microanatomy: Photomicrograph and sketch of adipose tissue, which is composed of fat cells. Notice that the nuclei of the cells are pushed to the perimeter as the cytoplasm fills with triglyceride (fat). (Photomicrograph from Dennis Strete.)
loss from the body, and acts as a mechanical shock absorber around organs, such as the kidneys.
The two main types of adipose tissue are white adipose tissue and brown adipose tissue. White adipose tissue is found throughout the body, particularly in the deep layers of the skin. Initially, white adipocytes resemble fibroblasts, but as they fill with lipid, the organelles and nuclei are pushed to one side and the cells become large spheres with eccentrically placed nuclei. As the cells swell, the cytosol is compressed into a thin, barely visible rim that surrounds the lipid droplet. Despite the compact condition of the cytoplasm, it continues to house all of the organelles normally found in cells. During tissue preparation for microscopic examination, the lipid content of the adipocyte is extracted, leaving a large unstained space in the center of the cell. This, combined with the densely cellular nature of adipose tissue, lends itself to the chicken-wire appearance that is evident microscopically.
Brown adipose tissue is found in newborn animals and in animals that hibernate during the winter. It is a highly specialized form of adipose tissue and plays an important part in temperature regulation, because it is a site of heat production. In brown fat, as in white adipose tissue, the nucleus is eccentrically placed; however the cytoplasm in brown fat is clearly visible, and lipid is stored in multiple small vesicles rather than in a single large droplet. The energy derived from the oxidation of lipids and released from electron transport is dissipated as heat in brown fat, rather than adenosine triphosphate (ATP). For this reason, brown fat contains an exceptionally high number of mitochondria (the site of electron transport), which become darkly stained in the cytoplasm. This dark coloration gives brown fat its name. Brown fat is also more vascular than white fat and this rich vascular network helps to dissipate the heat to many areas of the body. In this way, neonatal animals and hibernating animals can generate enough body heat during the vulnerable periods after birth and during the winter to survive. Histologically, brown fat looks glandular and therefore is sometimes called the hibernating gland.
RETICULAR CONNECTIVE TISSUE. Reticular connective tissue is composed of a complex, three-dimensional network of thin reticular fibers (Figure 5-19). It resembles areolar connective tissue in that it contains loosely arranged fibers and many fibroblasts suspended in a supportive ground substance. Unlike areolar connective tissue, however, reticular connective tissue contains only one type of fiber: reticular fibers. Together, the cellular and matrix components form a network called stroma, which constitutes the framework of several organs, such as the liver, spleen, lymph nodes, and bone marrow. Although reticular fibers are found throughout the body, reticular connective tissue is found in a limited number of sites.
DENSE FIBROUS CONNECTIVE TISSUE
Dense fibrous connective tissue is characterized by its densely packed arrangement of collagen fibers. Because little room is available for ground substance and cells, these are found in smaller quantities than in loose connective tissue. Nevertheless, as in loose connective tissue, fibroblasts can be found intermingled with fibers, where they play out their important role of manufacturing fibers and ground substance. The three major types of dense fibrous connective tissue are dense regular, dense irregular, and elastic.
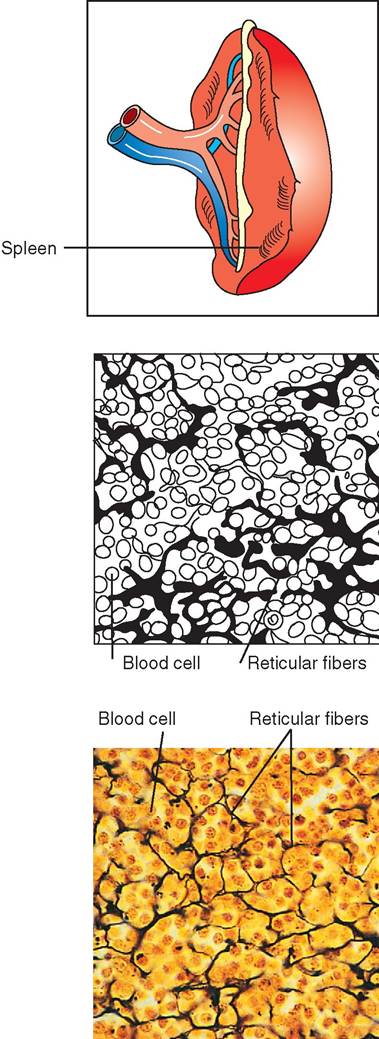
FIGURE 5-19 Reticular connective tissue. Description: Reticular cells supported by a fine network of irregularly arranged reticular fibers. Location: Spleen, lymph nodes, and bone marrow. Function: Provides internal skeleton for hematopoietic and lymphatic tissue. Microanatomy: Photomicrograph and sketch of reticular fibers, which stain darkly. They surround and support cells in the spleen. (Courtesy Ed Reschke.)
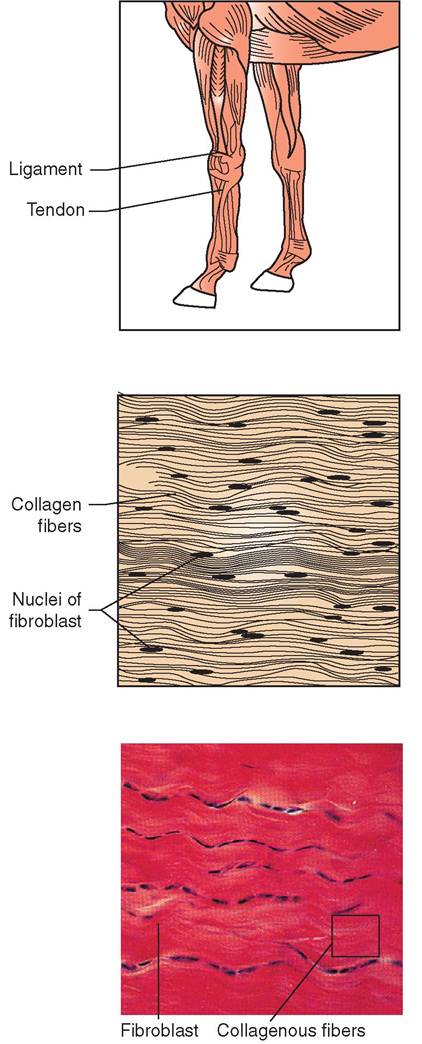
FIGURE 5-20 Dense regular connective tissue. Description: Primarily parallel collagen fibers. Occasional fibroblast interspersed among the fibers. Location: Tendons and ligaments. Tendons attach muscle to bone, and ligaments attach bones to one another. Function: Resists strong pulling forces. Has great capacity for stretch resistance in the direction of the fibers. Microanatomy: Photomicrograph and sketch of dense regular connective tissue in the tendon of a horse. Notice that the collagen fibers are arranged in parallel, tight bundles. (Courtesy Phototake.)
DENSE REGULAR CONNECTIVE TISSUE. Dense regular connective tissue is composed of tightly packed, parallel collagen fibers (Figure 5-20). The fibers lie in the direction of the force that is exerted on them, thereby giving the overall tissue tremendous tensile strength, but only in one direction. Dense regular connective tissue is silvery or white. It is relatively avascular and therefore is very slow to heal, because restorative nutrients and building molecules have difficulty reaching the damaged tissue. Fibroblasts form rows along the crowded fibers and devote most of their energy to the manufacture of fibers. Little ground substance is produced.
Dense connective tissue makes up the tendons that attach muscles to bone and the ligaments that hold bones together at joints. It also composes the broad, fibrous ribbons that sometimes cover muscles or connect them to other structures. In addition, dense connective tissue can be found in fascial sheets that cover muscles. These sheets are stacked into layers, one on top of another, but the direction of the fibers in one fascial layer may be different from the direction of the fibers in another layer. This helps to create an overall structure or fascia that can withstand forces from more than one direction.
DENSE IRREGULAR CONNECTIVE TISSUE. Dense irregular connective tissue is composed primarily of collagen fibers that are arranged in thicker bundles than those found in dense regular connective tissue (Figure 5-21). The fibers are interwoven randomly to form a single sheet that can withstand forces from many different directions. It is found in the dermis of the skin and in the fibrous coverings of organs such as the kidney, testes, liver, and spleen. It also forms the tough capsule of joints.
ELASTIC CONNECTIVE TISSUE. Ligaments can stretch more than tendons because of the larger number of elastic fibers contained within them. The massive nuchal ligament in the neck of horses, for example, has a particularly high concentration of elastic fibers and is therefore extremely flexible, enabling horses to lower their heads for long periods while grazing. Dense connective tissue that is primarily composed of elastic fibers, rather than collagen fibers, is called elastic connective tissue.
Elastic connective tissue is found in relatively few regions of the body, such as in the spaces between vertebrae in the backbone. It also occurs in regions of the body that require stretching, such as in the walls of arteries, stomach, large airways (bronchi), bladder, and regions of the heart. It lies beneath the transitional epithelium in the urinary tract and in the ligament suspending the penis. As its name implies, elastic connective tissue consists primarily of yellow elastic fibers. These fibers may be arranged in parallel or in an interwoven pattern with fibroblasts and collagenous fibers interspersed.
SPECIALIZED CONNECTIVE TISSUE
CARTILAGE. Cartilage is a tough, specialized connective tissue that is commonly called gristle. It is more rigid than dense connective tissue but is more flexible than bone (Figure 5-22). Cartilage is found in joints and helps to prevent the sensitive outer layers of bone from rubbing against one another. Because cartilage does not contain nerves, it can tolerate a great deal of compression without causing pain to the animal. (Imagine the compressive forces in the legs of an elephant!) In addition to joints, cartilage is found in the ear, nose, and vocal cords and forms a vital framework on which bone is formed in growing animals.
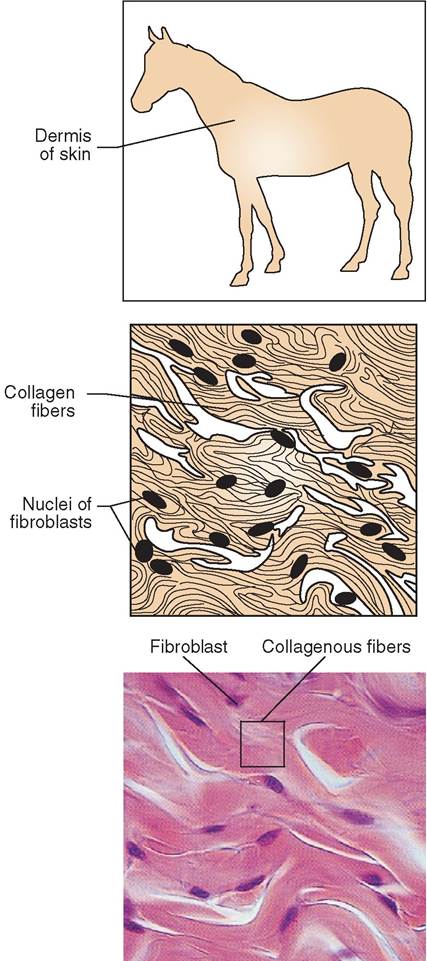
FIGURE 5-21 Dense irregular connective tissue. Description: Sheets of collagen that run in different directions or sheets of parallel fibers stacked in alternating directions. Location: Dermis of skin, organ capsules, submucosa of digestive tract. Function: Designed to withstand pulling forces in all directions. Microanatomy: Photomicrograph and sketch of dense irregular connective tissue found in the dermis of a cat. Notice that the pink collagen fibers and dark purple staining fibroblast cell nuclei are arranged in a swirling pattern. (Courtesy Ed Reschke.)
Like other forms of connective tissue, cartilage is composed of cells and matrix. The cells, called chondrocytes, live in hollowed-out pockets in the matrix, called lacunae. The ground substance of the matrix is a firm gel containing two different types of glycosaminoglycans (chondroitin sulfate and hyaluronic acid) and an adhesion protein called chon- dronectin. It also contains an unexpectedly large amount of tissue fluid. The fluid is held within the matrix and is
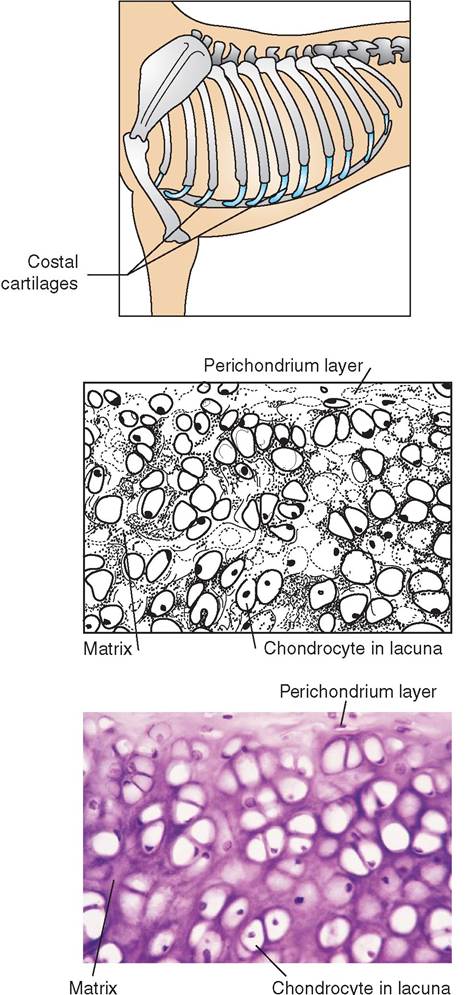
FIGURE 5-22 Hyaline cartilage. Description: Collagen fibers are evenly distributed throughout a rigid matrix. Cartilage cells or chondrocytes sit in spaces within the matrix called lacunae. Location: Articulating surfaces of bones; costal cartilages of ribs; cartilages in nose, trachea, and larynx; most of embryonic skeleton. Function: Provides both structural rigidity and flexibility simultaneously. Cushions joints against compressive forces. Microanatomy: Photomicrograph and sketch of hyaline cartilage from the chondral region of the sternum in a horse. (Courtesy Robert Calentine.)
important in transporting nutrients to the chondrocytes. It also gives cartilage its flexible resiliency and its ability to withstand compression. Collagen fibers are most commonly found in the matrix, but elastic fibers are also present in varying amounts.
Cartilage is avascular and therefore is very slow to heal. It receives its nutrition from a surrounding membrane, called the perichondrium, which is rich in tiny blood vessels. Nutrients diffuse from the perichondrium through the matrix to the chondrocytes. Therefore the chondrocytes that are farthest away from the perichondrium are potentially less well nourished than cells closer to it. For this reason, the thickness of cartilage is limited.
Three types of cartilage that vary from one another on the basis of the type of fiber found in the matrix are hyaline cartilage, elastic cartilage, and fibrocartilage.
HYALINE CARTILAGE. Hyaline cartilage is the most common type of cartilage found in the body. It is composed of closely packed collagen fibers that make it tough but more flexible than bone. Grossly, hyaline cartilage resembles bluewhite, frosted, ground glass. It is found as articular cartilage at the ends of long bones in joints and connects the ribs to the sternum. In addition, it forms supportive rings in the trachea and composes most of the embryonic skeleton. In growing animals, it is found in the growth plates of long bones, where it supports continued bone development and the extension of the length of the bone. Hyaline cartilage is the most rigid type of cartilage and is enclosed within a perichondrium.
ELASTIC CARTILAGE. Histologically, elastic cartilage is similar to hyaline cartilage but contains a plethora of elastic fibers, which form dense, branching bundles that appear black microscopically (Figure 5-23). These fibers give elastic cartilage tremendous flexibility so that it can withstand repeated bending. Elastic cartilage is found in the epiglottis of the larynx and in the pinnae (external ears) of animals.
FIBROCARTILAGE. Fibrocartilage usually is found merged with hyaline cartilage and dense connective tissue (Figure 5-24). It contains thick bundles of collagen fibers, like hyaline cartilage, but it has fewer chondrocytes and lacks a perichondrium. Fibrocartilage is particularly well designed to take compression and therefore is found in the spaces between vertebrae of the spine, between bones in the pelvic girdle, and in the knee joint.
BONE. Bone or osseous connective tissue is the hardest and most rigid type of connective tissue (Figure 5-25). Its specialized matrix is a combination of organic collagen fibers and inorganic calcium salts, such as calcium phosphate and calcium carbonate. The calcium salts alone would render bone brittle, but when combined with collagen fibers, bone becomes more flexible and has greater strength.
Despite the rigidity of its matrix, bone, unlike cartilage, is well vascularized. A central Haversian canal contains both a vascular and a nerve supply. In addition, tiny channels exist within the matrix that support the passage of blood vessels into deeper portions of the tissue. Bone cells, such as osteoblasts and osteoclasts, collaborate to remodel bone in response to the stresses placed on them. This involves a
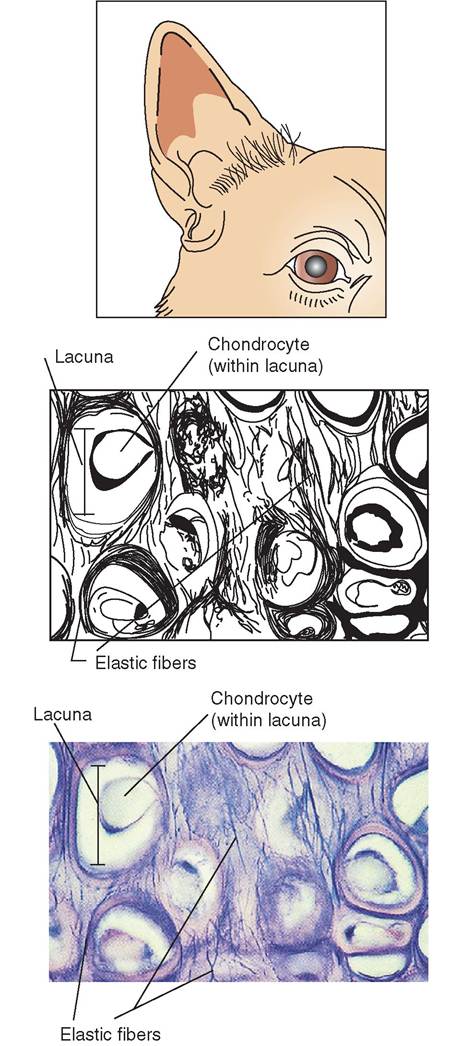
FIGURE 5-23 Elastic cartilage. Description: Elastic fibers suspended in firm matrix. Chondrocytes arranged in lacunae. Location: External ear (pinna), auditory tubes, and epiglottis. Function: Provides support and even more flexibility than hyaline cartilage. Microanatomy: Photomicrograph and sketch of elastic cartilage of the canine ear. Notice the chondrocytes situated within the lacunae and surrounded by a matrix filled with elastic fibers. (Courtesy Ed Reschke.)
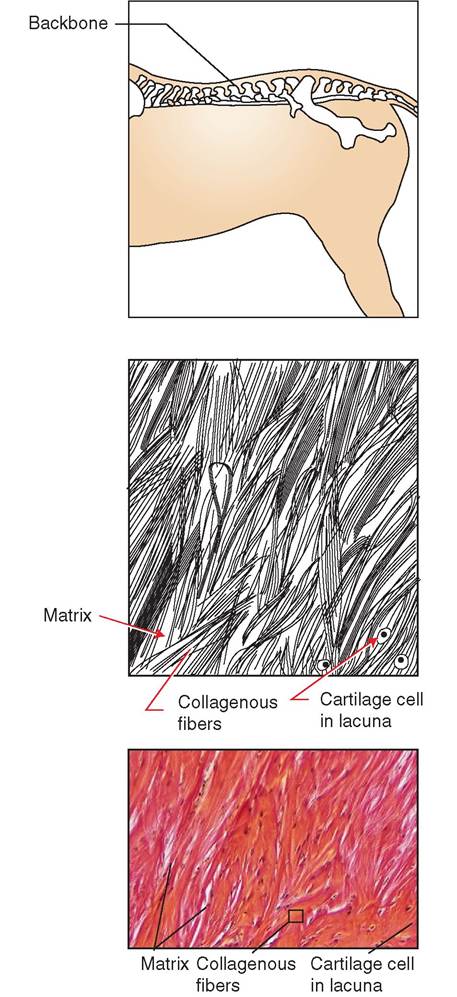
FIGURE 5-24 Fibrocartilage. Description: Similar to hyaline cartilage, but collagen fibers are more numerous and are arranged in thicker bundles. The matrix is less firm. Location: Pubic symphysis, intervertebral discs, discs in stifle and knee joints. Also found in temporomandibular joint of jaw. Function: Withstands compressive forces. Microanatomy: Photomicrograph and sketch of fibrocartilage from the spine of a horse. Notice that the strong, dense fibers are good at absorbing shock, particularly in the direction of the fibers. (Courtesy Robert Calentine.)
well-orchestrated combination of laying down new bone and taking away bone that is not needed. Osteoblasts, like other fibroblasts, manufacture the fibers that are part of the maNx. Although mature osteocytes reside individually in chembers called lacunae, they possess long, cellular extensions that pass through tiny threadlike channels called canaliculi, which radiate away from the lacunae. These chambers and canals are created as the osteoblasts surround themselves with the bony matrix they manufacture. Later they matae to become osteocytes. In this way, the cells not
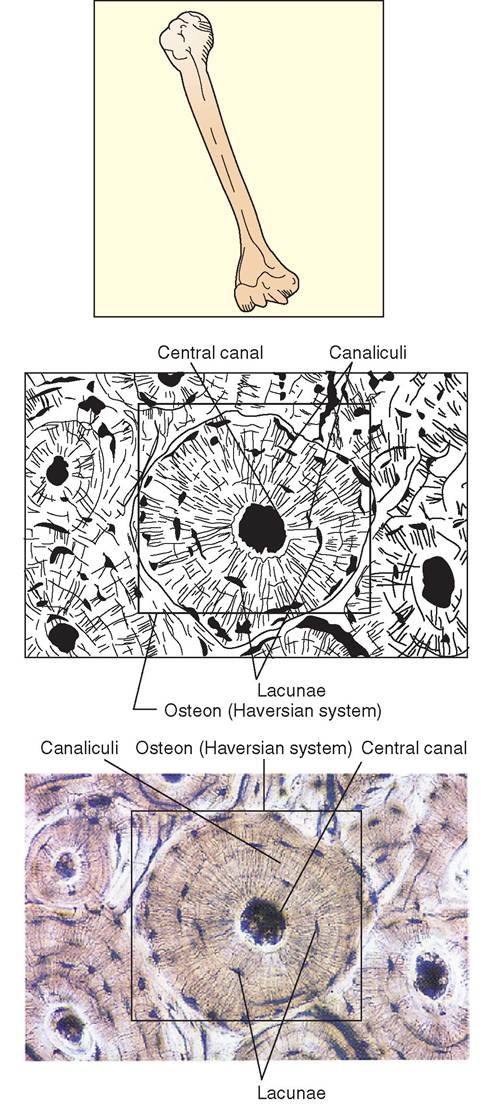
FIGURE 5-25 Compact bone. Description: Hard matrix dominates this tissue and is organized into concentric rings that surround a central canal. Chambers called lacunae and tunnels called canaliculi form spaces in hard matrix to accommodate bone cells (osteocytes) and their long cytoplasmic projections. Location: Bones of skeleton. Function: Provides support and protection; blood is produced in bone marrow; provides storage depot for calcium and other types of minerals. Microanatomy: Photomicrograph and sketch of compact bone. Notice the osteocytes located in lacunae within the Haversian canal system. (Courtesy Phototake.)
only create their own living spaces but also maintain connections with other cells.
Bone forms the skeletal frame of animals. It protects vital organs, such as the brain and heart, and acts as a calcium reserve for the body. In addition, bone marrow is the site of blood cell production and fat storage. A discussion of the development, structure, and function of bone is found in Chapter 7.
BLOOD. The red fluid that passes through vessels and that carries nutrient molecules and gases throughout the body is the most atypical connective tissue (Figure 5-26). The liquid component of blood is called plasma and constitutes the matrix. The fibrous component of the matrix is an array of protein molecules suspended in solution and visible only when blood clots. Blood is rich with a variety of cell types, such as erythrocytes (red blood cells), leukocytes (white blood cells), and thrombocytes, also known as platelets. Blood is discussed in greater detail in Chapter 12.
Table 5-2 summarizes the organization of connective tissue.
/ TEST YOURSELF 5-5
1. Connective tissue is divided into two broad categories. What are they?
2. What are the components of areolar tissue?
3. What is the common term for adipose tissue?
4. In terms of its form and function, how is brown fat different from white fat?
5. What are three subtypes of dense connective tissue?
6. Give three examples of specialized connective tissue. How are they similar to connective tissue proper? How are they different?
7. Why is cartilage limited in thickness and slow to heal?
8. Describe three types of cartilage. What are their differences and similarities?
9. Even though blood and bone appear to be grossly different, they both represent types of connective tissue. Why?
MEMBRANES
Epithelial and connective tissue may be collaboratively linked to form membranes in the body. Membranes are thin, protective layers that line body cavities, separate organs, and cover surfaces. They are composed of a multicellular epithelial sheet that is bound to an underlying layer of connective tissue proper. Commonly, the epithelium is bathed in a wet solution of liquid mucus or in the case of the bladder, in urine. Four common types of epithelial membranes are mucous, serous, cutaneous, and synovial (Figures 5-27 and 5-28, Table 5-3).
MUCOUS MEMBRANES
Mucous membranes, or mucosae, are characterized by their position in the body, because they are always found
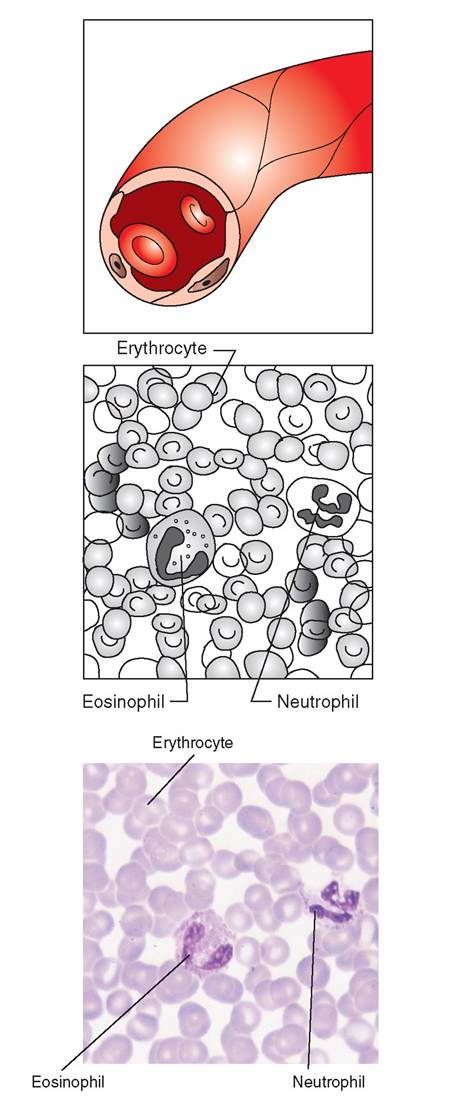
FIGURE 5-26 Blood. Description: Cells in a fluid matrix. Location: Found in blood vessels and heart. Function: Carries oxygen and nutrients to tissues; transports waste products and gases for disposal. Microanatomy: Photomicrograph and sketch of a blood smear. Notice that mature red blood cells (erythrocytes) have no nuclei and are biconcave. They appear lighter in their center where they are thinner. White blood cells (leukocytes) are larger than erythrocytes and have dark-staining nuclei. The leukocyte with the large pink granules in the cytoplasm is called an eosinophil and the other one is called a neutrophil. (From Thibodeau GA, Patton KT: Anatomy & physiology, ed 6, St Louis, 2007, Mosby.)
lining the organs that have connections to the outside environment. These organs are part of the digestive, respiratory, urinary, and reproductive tracts and include the mouth, esophagus, stomach, intestines, colon, nasal passages, trachea, bladder, and uterus, to name a few. The epithelial layer in mucous membranes is usually composed of either stratified squamous or simple columnar epithelium, and it covers a layer of loose connective tissue called the lamina propria. Another connective tissue layer, called the submucosa, usually connects the mucosa to underlying structures.
With the exception of the mucosae of the urinary tract, mucosae in general can produce large quantities of protective and lubricating mucus. Goblet cells or multicellular glands may be found throughout the tissue. These structures are responsible for the production and secretion of mucus, which consists primarily of water, electrolytes, and a protein called mucin. The mucus is slippery and therefore can decrease friction and assist with the passage of food or waste. Because of its rich supply of antibodies and viscous consistency, the mucus produced by the mucosae is also helpful in the entrapment and disposal of invading pathogens and foreign particles. This is particularly apparent in the nasal passages, where microorganisms and debris are inhaled and trapped by mucus. We may find, for example, accumulations of black debris in our noses after we have been near a sooty campfire. When we have a cold, we find that the amount of mucus produced and secreted by the mucosae increases and a runny nose develops.
Some mucosae can absorb as well as secrete. For example, the epithelial layer in the intestine is specially designed for rapid and efficient transfer of nutrient molecules from the intestinal lumen to the underlying connective tissue and its blood supply. The mucous membranes therefore play an important role in monitoring and controlling what enters the body and form an important barrier between the outside environment and the delicate inner workings of underlying tissues. Their secretory and absorptive qualities make them particularly well suited for this role.
SEROUS MEMBRANES
Serous membranes are also called serosae. They line the walls and cover the organs that fill closed body cavities, such as the chest cavity or thorax and the abdominal and pelvic cavities (see Figures 5-27 and 5-28). Serosa is characterized as a continuous sheet that is doubled over to form two layers with a narrow space in between. The portion of the membrane that lines the cavity wall is called the parietal layer, and the portion that covers the outer surfaces of the organs is called the visceral layer.
The serosa is composed of a sheet of simple squamous epithelium bound to an underlying layer of loose connective tissue. This histologic organization allows a great deal of permeability and enables interstitial fluid to pass through the membrane into the narrow spaces between the serosal layers. In this way, serosal fluid is a transudate and, unlike the mucoid thick secretion of mucous membranes,
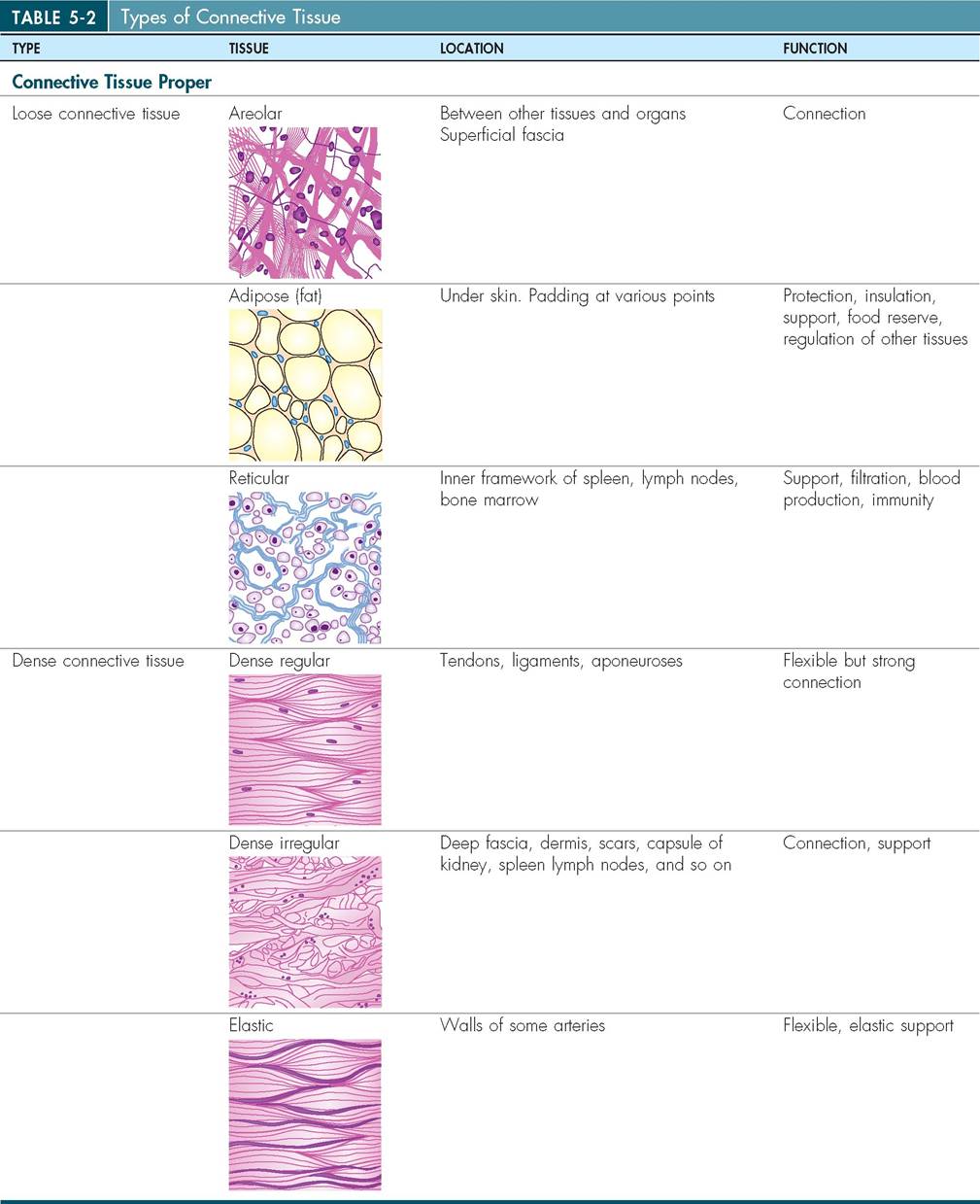
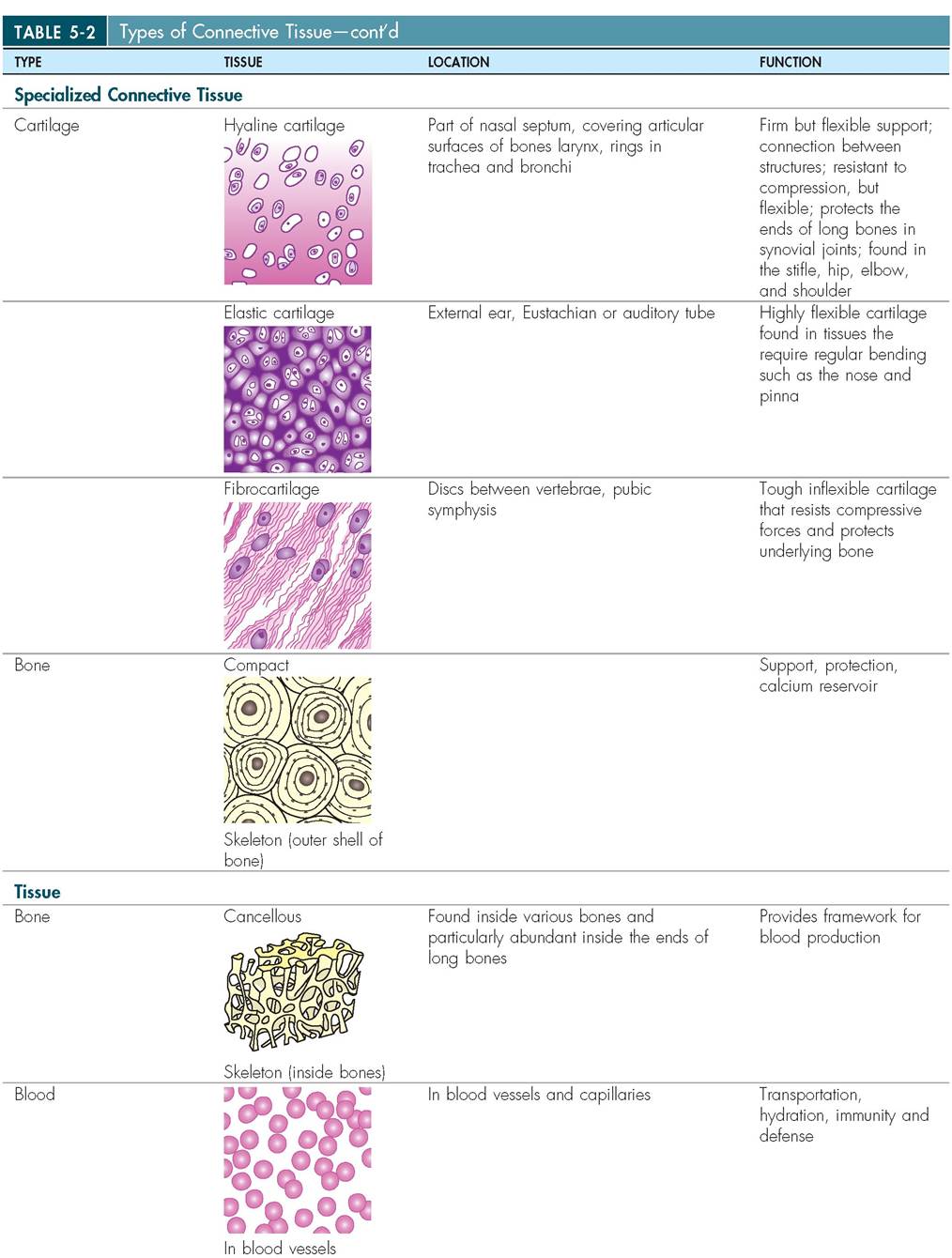
(Images from Patton KT, Thibodeau GA: Anatomy & physiology, ed 8, St Louis, 2013, Mosby.)
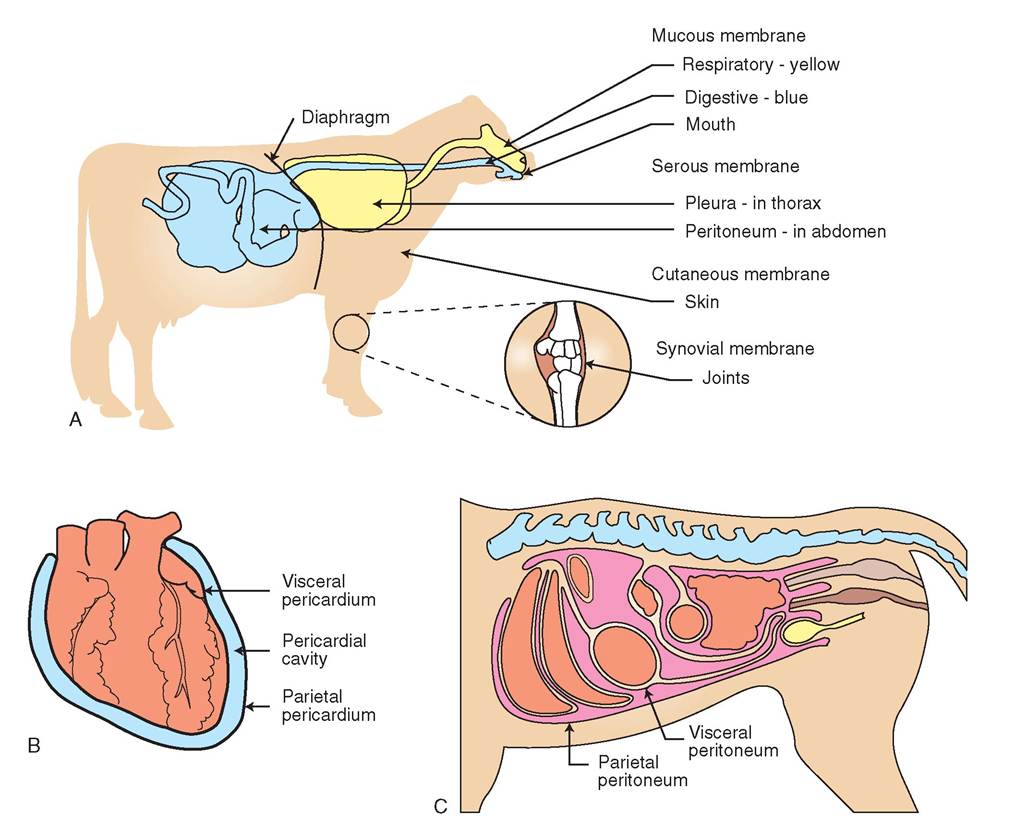
FIGURE 5-27 Types of membrane. A, Mucrous, serous, cutaneous, and synovial membranes are found throughout the body. Mucous membrases line body cavities that are exposed to the outside, such as the anus, mouth, and nares. Membranes often contain glands, which secrete mucus. Serous membranes line body cavities that have no connection with the outside. Although they do not contain glands, they secrete serous fluid, which helps lubricate and prevent adhesions within body cavities. The cutaneous membrane is the dermis, or skin, which covers the outer region of the body. Synovial membrases line cavities that surround joints. B, Tire heart is covered by a serous membrane called the pericardium. Tine pericardium folds back on itself, forming two layers with a space or cavity in between. The layer closest to the heart is called visceral pericardium, whereas the outer layer is called the parietal pericardium. C, Mu serous membrane in the abdominal cavity is called the peritoneum. Visaeral peritoneum covers organs, and parietal peritoneum lines the peritoneal, or abdominal, cavity.
is thin and watery. It contains electrolytes but no mucin. By coating the parietal and visceral layers, serosal fluid creates a moist and slippery surface, which reduces friction between adjacent oroans and between the oroans and the cavity wafl. Transudates take on different names dependino on where they are located in the body. A transudate in the thorax, for example, is called pleural fluid; in the abdomen, peritoneal fluid; and in the reoion around the heart, pericardial fluid.
oTnhseisctency of serous fluid may vary and chanoe in patholooic conditions. For example, if an animal fractures a lreoilblos,db c and fluid may leak from ruptured capillaries into the pleural space, creatino a hemothorax. When cel Is, protein, and other solid material mix with serous fluid, it ebnecseormes d than a transudate and is called an exudate.
Normally, the amount of serous fluid found in body cavities is small, but durino trauma or some patholooic condi- tuicohns, s as in hemothorax, the amount of fluid may Xecome excessive. When an abnormally laroe amount of nuid enters a body cavity, the fluid is known as an effusion. Ascites, for example, is the presence of an effusion in the peritoneal space of the abdominopelvic cavity and can be cyaused b a wide ranoe of patholooic conditions, such as conoestive heart failure, nephrosis,namntalio neoplastic
disease, and peritonitis.
rWouhsen the se membranes are damaoed, production of serous fluid may be impeded and abnormal connections called adhesions may fem between the parietal and visceral lhaeyseers. T connections may alter the normal function of trhoeanos involved and can cause excruciatino discomfort
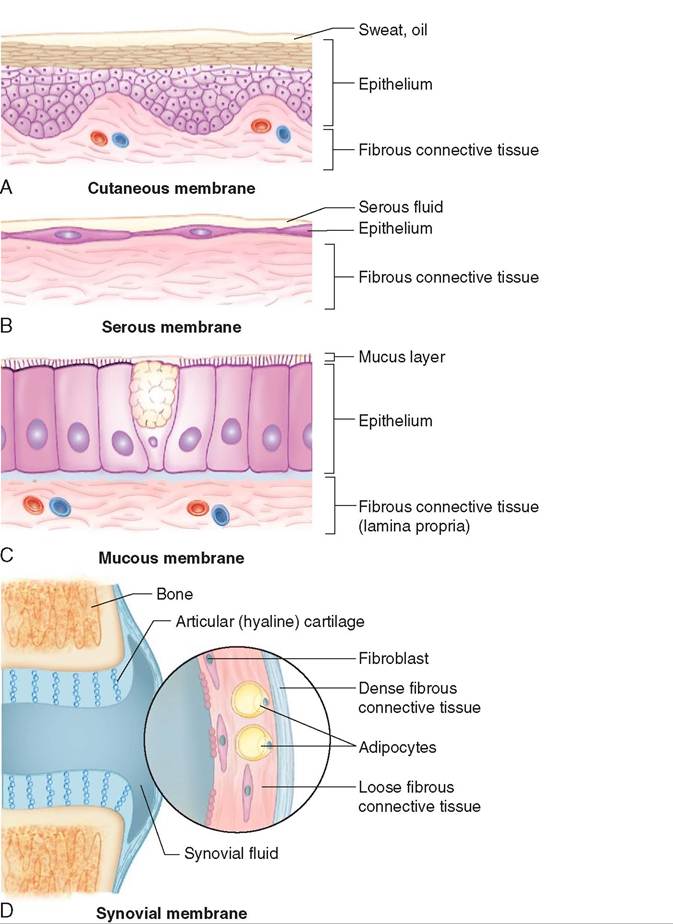
FIGURE 5-28 Structure of membranes. Epithelial membranes (contain epithelium): A, Cutaneous membrane (skin); B, serous membrane (serosa: 'pleura' in the thoracic cavity, 'peritoneum' in the abdominal cavity); and C, mucous membrane (mucosa: epithelium that lines body orifices). Connective tissue membranes (do not contain epithelium): D, synovial membrane (line mobile joints and bursae, produce synovial fluid). (From Patton KT, Thibodeau GA: Anatomy & physiology, ed 8, St Louis, 2013, Mosby.)
to the patient, particularly if the adhesions occur in the pleural space of the thoracic cavity.
In the abdominopelvic cavity, the visceral layers of serosa merge to form supportive ligaments called mesenteries. These ligaments secure organs to the body wall and form a framework for the passage of blood vessels and nerves. The stomach, for example, is connected to the abdominal wall by mesentery called the omentum, and the uterus is similarly attached via the broad ligament.
CUTANEOUS MEMBRANES
The cutaneous membrane is also called the integument, or, more simply, skin. It is an o^aιt that is perpetually eoxposed t the outside environment and therefore possesses unique features that distinguish it from the other membrane types. It is composed of an outer keratinized stratified squamous epithelium, or epidermis. Keratin is a waxy substance that fills the cells of the epidermal lyayer as the make their developmental migration from the basement membrane to the outermost layer. It is responsi- bolre f the waterproof quality of skin and aids in the prevention of desiccation. Keratinized squamous epithelium is also durable and is partly responsible for the skin's ability ittohwstand abrasive forces.
pTihdee remis is attached to an underlying layer of
rdeegnuslearir connective tissue called the dermis.heT
| TABLE 5-3 Membranes in Animals | |||||
| TYPE | SUPERFICIAL LAYER | DEEP LAYER | LOCATION | FLUID SECRETION | FUNCTION |
| Epithelial | |||||
| Cutaneous Example: Integument | bgcolor=white>Keratinized stratified squamous epithelium (epidermis) Dense irregular fibrous connective tissue (dermis) | Directly exposed to external environment | Sweat; sebum (skin oil) | Protection, sensation, thermoregulation | |
| Serous Examples: Lining of thorax (plura) and abdomen (peritoneum) | Simple squamous epithelium | Fibrous connective tissue | Lines body cavities that are not open to the external environment | Serous fluid | Lubrication |
| Mucous Examples: Gums, vulva, and anus | Various types of epithelium | Fibrous connective tissue (lamina propria) | Lines tracts that open to the external environment | Mucus | Protection, Lubrication |
| Connective | |||||
| Synovial Examples: Lining of knee, elbow, and shoulder joints | Dense fibrous connective tissue | Loose fibrous connective tissue (in movable joints) | Lines joint cavities lubricates, cushions | Synovial fluid | Helps hold joint together |
From Patton KT, Thibodeau GA: Anatomy & physiology, ed 8, St Louis, 2013, Mosby.
dermis is rich in collagenous, reticular, and elastic fibers, which enable skin to be both strong and elastic. The structural and functional properties of skin are discussed further in Chapter 6.
SYNOVIAL MEMBRANES
Synovial membranes line the cavities of joints. Unlike the other membrane types, synovial membranes have no epithelium. They are composed exclusively of connective tissue. Grossly, the synovial membrane is smooth, shiny, and white. Histologically, the membrane is composed of loose connective tissue and adipose tissue covered by a layer of collagen fibers and fibroblasts. Synovial membranes manufacture the synovial fluid that fills the joint spaces and, together with hyaline cartilage, reduces friction and abrasion at the ends of the bones.
∕ j CLINICAL APPLICATION
Mucous Membranes: Keys to a Diagnosis
When animals are sick, they show signs of illness in many ways. We know that they may become depressed and lethargic. They may stop eating and drinking, may vomit, have diarrhea or bloody urine, or stop urinating entirely. Animals may show signs of illness through changes in the appearance of their mucous membranes. The easiest mucous membranes to examine are those located on the inside of the mouth and on the gums. Here, a veterinarian or veterinary technician can gain clues about the general state of the animal. For example, dehydrated animals have dry, tacky mucous membranes. Animals with wet mouths are less likely to be dehydrated.
The color of mucous membranes is also very important. A yellow tinge, for example, may indicate elevation of bilirubin in the blood. This condition is known as icterus, and the yellow appearance of an animal is called jaundice. There are many causes of increased levels of bilirubin, such as liver failure and hemolytic anemia. For this reason, additional tests are needed to determine the cause of the jaundice. Blue mucous membranes occur in animals that cannot provide their tissues with adequate amounts of oxygen. These animals develop a condition called hypoxia (hypo meaning below [normal] and oxia meaning oxygen). Animals with tracheal obstruction, severe pneumonia, or circulatory collapse may all show signs of hypoxia. Bright red mucous membranes may be evident in animals that are hyperperfused, a condition in which blood flow to peripheral tissues is increased. Febrile and hypertensive animals and animals undergoing an allergic reaction may have hyperemia or bright red mucous membranes. In contrast, pale or white mucous membranes may indicate anemia, shock, or hypothermia.
Finally, the clinician may gain additional clues about the state of the circulatory system by examining the gums. If pressed firmly, the pink region of a animal’s gum blanches white. When released, the gum changes from white back to pink relatively quickly. The time that it takes for blood to return to the capillaries and turn the gum pink again is called the capillary refill time (CRT). Normal CRT is 1 to 2 seconds. In animals that have compromised cardiac output, low blood pressure, or severe peripheral vasoconstriction, the CRT will be prolonged. Animals with high blood pressure and those in hypercompensatory states may have shortened CRTs, lasting less than 1 second.
Thus examination of the mucous membranes in an animal is very important and may lead to a greater understanding of the animal’s condition.
∕ j CLINICAL APPLICATION—cont'd
Capillary refill time (CRT). A, If you press firmly on the pink region of a horse's gum, the gum blanches white. B, When you remove your finger, you will notice that the gum changes from white back to pink relatively quickly. The time that it takes for blood to return to the capillaries, and turn the gum pink again, is called the CRT. (From Speirs VC: Clinical examination of horses, St Louis, 1997, Saunders.)
∕y CLINICAL APPLICATION
Histopathology: An Introduction
Histopathology is the microscopic study of disease in tissues (histo- means tissue and pathology is the study of disease). He normal microanatomy of tissues is altered by pathologic disorders in many ways. For example, in mammary tissue that contains a malignant tumor, abnormally large, immature mammary cells may be evident microscopically. Tlie nuclei of these cells are abnormally large, and many of the cells may be actively dividing. Other diseases, such as viral and ebcatcitoenrisa, l inf may cause cell death and create regions
within the feιιe that are dead or necrotic. Stil 1 other diseases may cause the abnormal accumulation of fluid, leading to a condition called edema, or my∙ involve the accumulation of a waxlike glycoprotein called amyloid. TWis pathologic condi- teyions ma b evident microscopically as an increase or decrease in cell numbers, cell size, and changes in the cell’s shape and in the architecture of the tissue’s support structures.
Although the pathologic nature of diseased tissue is often evident under microscopic examination, grossly the tissue may appear normal. For this reason, a definitive diagnosis eoften can b made only through the microscopic examination iyosfs ut e b taking a biopsy. Occasionally, aspirating cells from itshseuet can lead to a diagnosis also.
A biopsy is the removal of a small piece of tissue from an organ or mass. This may involve the insertion of a special kind ieoodfplbesy ne into the tissue, or it may involve cutting out, or excising, a pi^ce W tissue with a scalpel. Some biopsy seamples ar obtained using special grasping attachments on the exμ^lr^⅛)ry end of endoscopes; others may be acquired using a coolde-cutter type of instrument called a biopsy punch. Biopsy samples are harvested from the normal-abnormal toirsdsueresb if possible. In addition, because the tissues are ydelicate, the should be cut with sharp instruments, such as scalpels, and maneuvered with tissue forceps, not dressing forceps, so that the microanatomy is not crushed.
No matter how the sample is obtained, it must be handled ewith car and specially prepared before it can be examined. Samples should be sliced so that each piece is no thicker than 1 cm, and these should be placed in a fixative solution of 10% buffered formalin. The ratio of the volume of formalin solution to the volume of tissue should be approximately 10 : 1, seocimthensp can absorb enough fixative to preserve it in
its thickest regions. For example, if a large section of heart from a Doberman Pinscher is stuffed into a small container ofrmf alin, the fixative may not be able to penetrate the tissue adequately and the heart will degenerate. Thus the architec- fture o the muscle will be lost, and a potential diagnosis of dilated cardyo^^iathy, for example, will be impossible to confirm. Encapsulated or very fibrous tissues are also difficult tooodfix. A g rule of thumb is to make sure that the tissue is freely mobile in the container of formalin. Conversely, samples texhtraetmarelye small are sometimes invisible within a sea
ofrmf alin and are seemingly lost. In these cases, reports
stating “no sample found” are returned to the clinician. There- fuotree, min specimens should be placed in small, labeled cassettes.

Preparation of tissues for histopathologic evaluation. Tissue is placed in formalin-filled, leak-proof containers. The ratio of the volume of formalin to tissue is about 10: 1. Once received by the laboratory, the tissue is examined and sectioned. Sections are placed into tissue cassettes, which are numbered with the patient's surgical accession number. Sections are then placed in an automatic tissue processor to be treated overnight. Under a vacuum system, the tissues are dehydrated with progressively higher concentrations of alcohol. Tissues are then cleared with xylene, which is a solvent capable of dissolving paraffin. Cassettes are put through a series of xylene-paraffin solutions in which the concentration of paraffin increases until the tissue becomes infiltrated, which facilitates thin slicing.
Tissue cassettes are removed from the processor.

Tissues are individually transferred to rectangular metal molds, which are filled with liquid paraffin.
The paraffin hardens into a soft white wax.
∕ j CLINICAL APPLICATION—cont'd


Before the paraffin hardens completely, the cassette cover with the correct identification is placed over the mold.
Paraffin provides support to the tissue and enables it to be sliced into very thin sections. Just before being sliced, the paraffin is chilled further with ice to make it easier to slice.
The molds are then arranged and ordered for slicing.

Extraordinarily thin slices (4 to 8 μm) are cut from the chilled paraffin blocks using a special cutting device called a microtome.

Several serial slices form a paper-thin strip, which is floated on the surface of a water bath.

Carefully, these thin sections are collected onto labeled glass microscope slides.

Slides are stood vertically to drip dry and are then transferred to a warm incubator, such as the one pictured, to speed drying and help tissue adhere to the slide.
In preparation for staining, tissue sections are de-paraffinized and rehydrated so that aqueous stains can react with them. Laboratories that process large numbers of slides daily use automated staining machines such as the one pictured. After being stained, tissues are again dehydrated with progressively higher concentrations of alcohol and then cleared with xylene.
∕ j CLINICAL APPLICATION—cont'd
Finally, a protective glass cover slip is applied to each slide with Permount (a type of glue) sandwiched in between the two glass layers. Finished slides are logged in a journal before being examined microscopically by a veterinary pathologist.
TEST YOURSELF 5-6
1. Membranes are composed of what two tissue types?
2. Where are mucous membranes found? What functions do they perform?
3. What portion of a serous membrane covers the outer surface of organs?
4. What is an effusion? What is ascites?
5. What is another name for cutaneous membrane?
6. Where are synovial membranes found? How are they different from other membrane types?
MUSCLE TISSUE
Muscle cells, or muscle fibers, are uniquely designed for contraction. The fibers are composed of specialized proteins called actin and myosin, which are arranged into microfilaments. Contraction, or shortening, of the muscle cell occurs when the microfilaments slide over one another, like the bars in an old-fashioned slide ruler. In this way, the cells change shape and can be made shorter or longer. As the muscles contract, thee move the bones, blood, and soft tissue structures that are associated with them. Thus blood is circulated, legs are made to run, and food is moved slowle through the intestine. There are three types of muscle tissue: skeletal, smooth, and cardiac (Figure 5-29).
SKELETAL MUSCLE
Skeletal muscle contains numerous large cells that may be a foot or more in length. Because of their large size and heavy metabolic requirements, the cells contain hundreds of nuclei and mitochondria needed to maintain cellular homeostasis. Skeletal muscle is responsible for an animal's ability to walk, run, kick, bite, and show facial expression. Unlike cardiac and smooth muscle, skeletal muscle is usually controlled through conscious effort and therefore is called voluntary muscle. In other words, the animal can control its movement through conscious thought. In addition, skeletal muscle cells are striated, or striped, because histologically they have alternating bands of light and dark across them. Thus skeletal muscle is referred to as voluntary, striated muscle.
The cells of skeletal muscle are essentially fibers that are clustered into bundles and held together by loose connective tissue. The collagen fibers that surround the cells merge with the collagen fibers in tendons to attach muscle firmly to bone. Muscle cells are stimulated to contract by the action of nerve fibers attached to them, located throughout the entire muscle belly. If the nerves are damaged, the ability of the muscle to contract is impaired, and the muscle is said to be paretic, or paralyzed. In this way, all of the actions that an animal can normally control, such as walking, running, eating, and moving the head and arms, depend on a healthy nervous system as well as a healthy muscular system.
SMOOTH MUSCLE
Smooth muscle is composed of small, spindle-shaped cells that lack striations or bands and therefore appear smooth. Like skeletal muscle, smooth muscle may be stimulated to contract by the action of nerves but, unlike skeletal muscles, the contractions cannot be consciously controlled. Smooth muscle is therefore called nonstriated, involuntary muscle. It is found in the walls of hollow organs, such as blood vessels, urinary bladder, uterus, intestines, and stomach and is also found in exocrine glands and along the respiratory
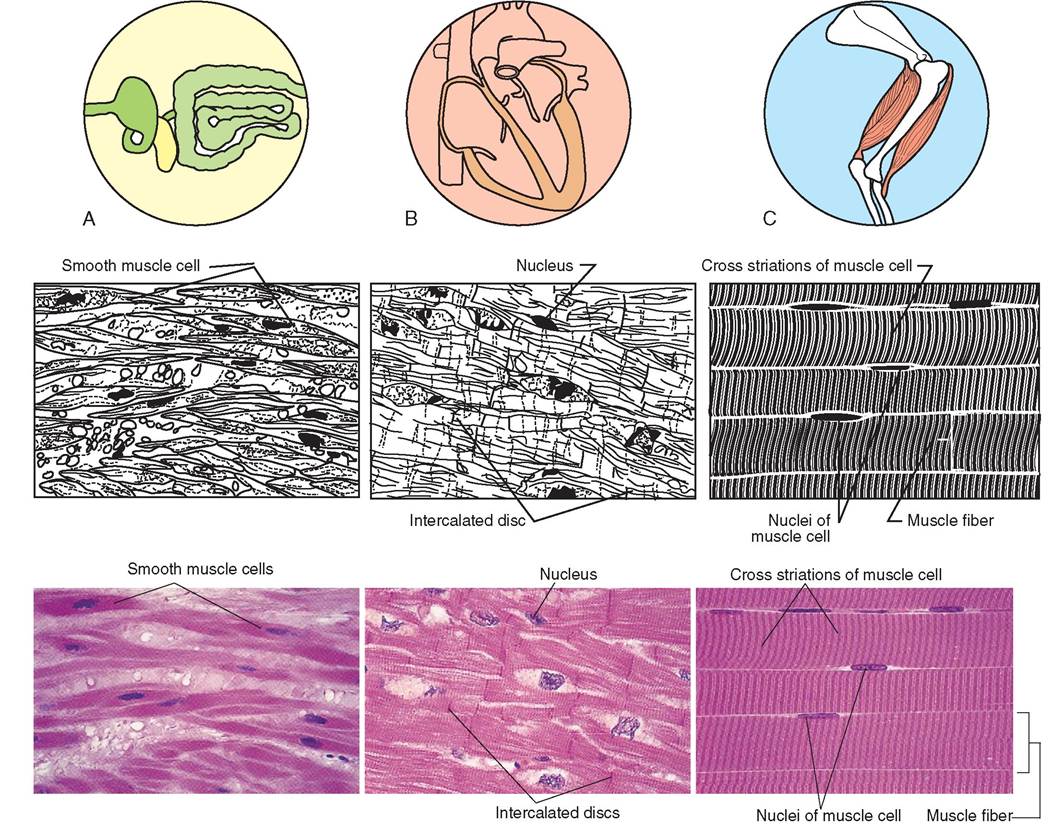
FIGURE 5-29 Types of muscle tissue. A, Smooth muscle. Description: Nonstriated, involuntary; composed of small, spindle-shaped cells that lack striations or bands and therefore appear 'smooth.' Each cell has a centrally located nucleus. Location: In the walls of hollow organs such as the esophagus, stomach, intestine, colon, blood vessels, and bladder; also in skin attached to hair and in the iris of the eye. Function: Moves food through the digestive tract, regulates the size of an organ, controls light entering the eye, moves fluid through vessels, and causes hair to stand erect. Microanatomy: Photomicrograph and sketch of smooth muscle cells. B, Cardiac muscle. Description: Striated, involuntary; cells are cylindrical and branched with a single, centrally located nucleus. Cells form an intricate network and are connected by intercalated discs in a specialized type of gap junction. Location: Found only in the heart. Function: Pumps blood through the vascular system. Microanatomy: Photomicrograph and sketch of cardiac muscle cells. Notice the intercalated discs unique to the cardiac cell. Each cell contains only one, centrally located, nucleus. C, Skeletal muscle. Description: Striated, voluntary; cells are striped, long, and cylindrical, each one with multiple, eccentrically placed nuclei. Location: Attached to bone and occasionally to skin, eyeballs, and upper part of the esophagus. Function: Voluntary movement of body, including movement of the eyes and the initial part of swallowing. Microanatomy: Photomicrograph and sketch of skeletal muscle cells. Notice that each cell contains multiple nuclei, which are found along the cell membrane. (A, Courtesy Carolina Biological Supply Company/Phototake. B and C, Courtesy Ed Reschke.)
tract. It is responsible for peristalsis in the gastrointestinal tract, for the constriction of blood vessels, and for the emptying of the bladder. Because smooth muscle cells are relatively small, they require only one centrally located nucleus.
CARDIAC MUSCLE
Cardiac muscle exists only in the heart and possesses the remarkable ability to contract even when neural input has been altered. Specialized pacemaker cells within the heart muscle supply the signal for the heart to contract at regular intervals. This input is entirely involuntary and is responsible for initiating the pumping force, which propels blood through blood vessels. Thank goodness we do not need to concentrate on keeping our hearts beating!
As in smooth muscle, the cells of cardiac muscle are relatively small and contain only one nucleus. However, unlike smooth or skeletal muscle, cardiac muscle branches to form a complex network. The cardiac muscle cells are striated and are connected to one another at each end via a specialized intercellular junction called an intercalated disc. These discs occur only in cardiac muscle. Thus cardiac muscle is classified as an involuntary, striated tissue.
NERVOUS TISSUE
Nervous or neural tissue is uniquely designed to receive and transmit electrical and chemical signals throughout the body (Figure 5-30). It is found in the brain, spinal cord, and peripheral nerves and is composed primarily of two general cell types: neurons and supporting neuroglial cells.
Neurons are the longest cells in the body and may reach up to a meter in length. They are composed of three primary parts: a cell body called a perikaryon, short cytoplasmic extensions called dendrites, and a long, single extension called an axon. The cell body contains the nucleus, which controls the metabolism of the cell. The dendrites receive impulses from other cells, whereas the axon conducts impulses away from the cell body. The neuron forms connections with many other tissues, such as muscle, viscera, glands, and other neurons. In this way, a complex network is formed that controls and regulates many body functions. The neuron is exquisitely sensitive to electrical and chemical changes in its environment and may respond by transmitting nerve impulses along its axon to other tissues. These electrical impulses, which carry information and instructions, are transmitted through conductive membranes on the neurons.
Neuroglial cells are found in greater numbers in neural tissue than are neurons. They do not transmit impulses but rather serve to support the neurons. Some specialized types of neuroglial cells function to isolate the conductive membranes, others provide a supportive framework that helps bind the components of neural tissue together, and still others phagocytize or digest debris, or they help supply nutrients to neurons by connecting them to blood vessels.
BOX 5-2 Summary of Tissues
I. Epithelial tissue
A. Simple squamous
B. Simple cuboidal
C. Simple columnar
D. Stratified squamous
E. Stratified cuboidal
F. Stratified columnar
G. Transitional
H. Pseudostratified
II.Connective tissue
A. Connective tissue proper
1. Loose connective tissue
a. Areolar tissue
b. Adipose tissue
c. Reticular tissue
2. Dense connective tissue
a. Dense regular
b. Dense irregular
c. Elastic tissue
B. Specialized connective tissue
1. Cartilage
a. Hyaline cartilage
b. Elastic cartilage
c. Fibrocartilage
2. Bone
a. Compact
b. Cancellous
3. Blood
III. Muscle tissue
A. Skeletal (striated, voluntary)
B. Cardiac (striated, involuntary)
C. Smooth (nonstriated, involuntary)
IV. Nervous tissue
The gross anatomy and physiology of nervous tissue are discussed in Chapter 9.
Box 5-2 summarizes tissues.
TISSUE HEALING AND REPAIR
Injuries occur in many ways. Animals may experience trauma from being hit by a car or from falling out a window. They may be bitten, scratched, or kicked by other animals and may experience broken bones and wounds that later become infected by pathogens. The body's initial response to these injuries is inflammation, a series of events that develop quickly to limit further damage and eliminate any harmful agents. Repair occurs more slowly and involves the organization of granulation tissue and the regeneration of lost tissue or the formation of scar tissue. Many of these processes occur simultaneously, making the injured area a busy workplace for cells. We will take a closer look at what is happening during the healing process. A summary of tissue repair is illustrated in Figure 5-31.
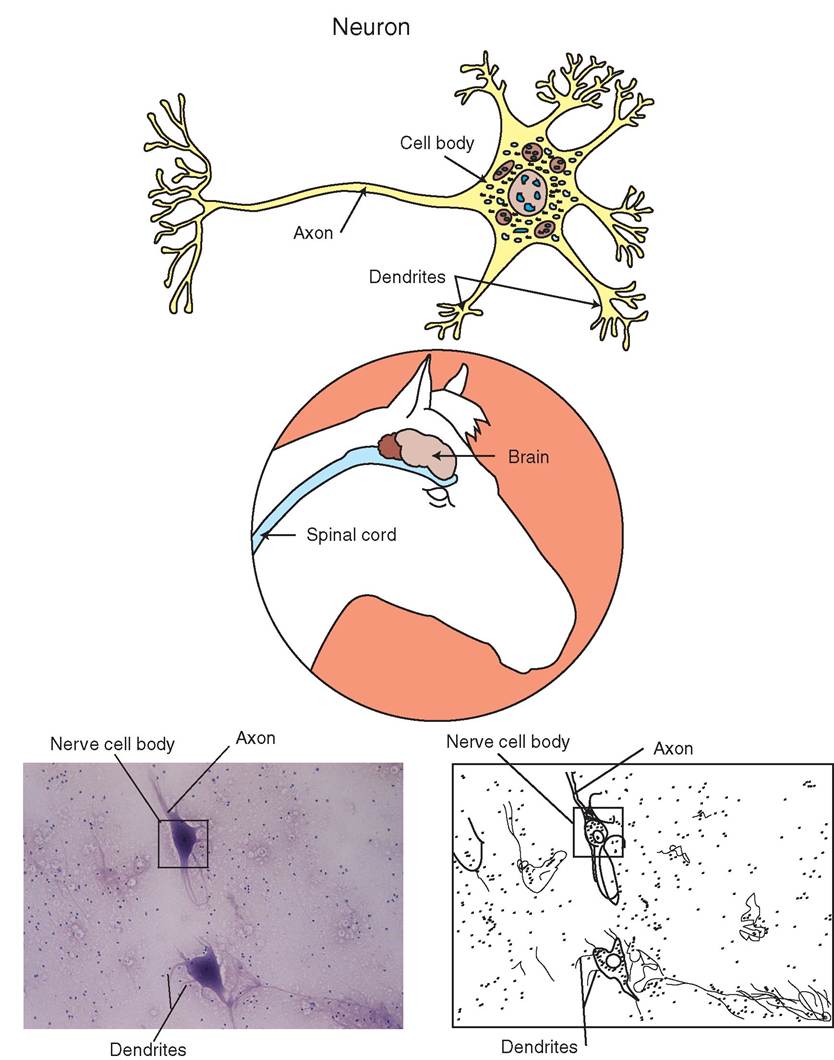
FIGURE 5-30 Nervous tissue. Description: Composed of neurons and supportive neuroglial cells. A neuron may be multipolar (as shown) or unipolar. Each multipolar neuron is composed of a cell body, which contains a nucleus; multiple short, branched dendrites; and a single long axon. A unipolar neuron is composed of a cell body and one branched axon. Location: Brain, spinal cord, and nerves. Function: To conduct electrical signals, store information, and evaluate data; to transmit sensory information to spinal cord and brain. Microanatomy: Photomicrograph and sketch of tissue from a spinal cord. Notice the cell body (soma) from which multiple dendrites and a single axon emerge. (Photomicrograph from Thibodeau GA, Patton KT: Anatomy & physiology, ed 6, St Louis, 2007, Mosby.)
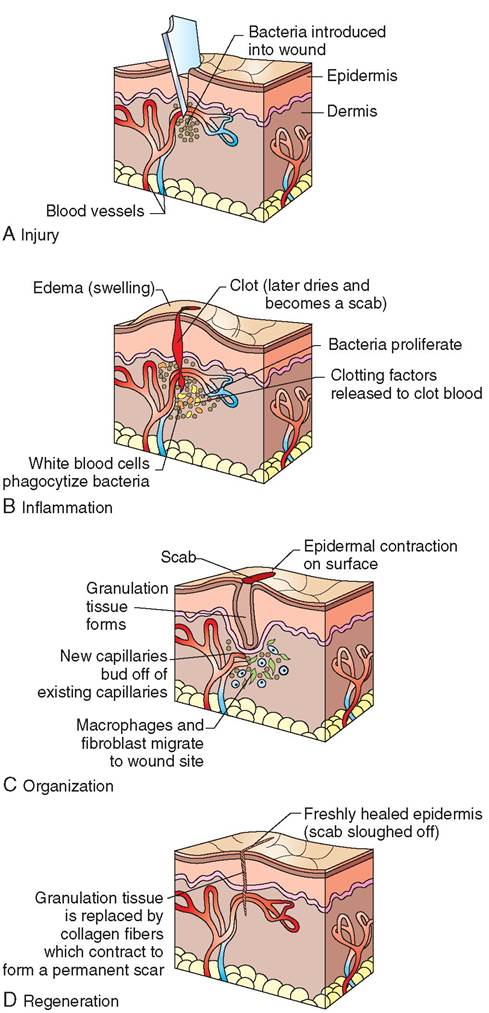
FIGURE 5-31 Tissue repair of minor skin wound. A, Injury. A piece of glass causes a cut in the skin. B, Inflammation. Blood vessels dilate and become more permeable, causing redness in the tissue around the wound. Fluid leaks into the tissue from dilated capillaries and causes swelling. A blood clot, which later becomes a scab, forms at the wound opening. Pressure of fluid on nerve endings causes pain. C, Organization. Granulation tissue forms below the scab. Fibroblasts lay down collagen fibers while macrophages engulf foreign debris and invading microorganisms. D, Regeneration or fibrosis. Epithelial cells around the wound edges proliferate and cover the granulation tissue. The scab is pushed off. Granulation tissue becomes fibrous scar tissue, which contracts and pulls the wound edges together.
Inflammation: the first stage
Whenever a tissue is injured, it causes an immediate inflammatory response. The affected area becomes red, swollen, hot, and tender. Sometimes there is decreased function of the injured body part. Inflammation is the body's attempt to isolate the area, limit the damage caused by the injury, and prevent further damage. Note that inflammation does not imply infection. Infection is inflammation caused by viruses, bacteria, and fungi. Injuries such as chemical burns, broken bones, and pulled muscles do not necessarily involve the ifnvasion o these microorganisms. Inflammation therefore is a noni^fi^^ofic reaction to injury or disease. The inflammatory process is the same regardless of the type of disease or injury. ⅞e extent of inflammation, however, depends on the type of tissue involved and on the severity of the injury or illness.
STEPS IN THE PROCESS OF INFLAMMATION
1. Inflammation begins with a 5- to 10-minute period of vasoconstriction, fcWowd by a sustained period of Vasodilationi The initial constriction occurs in the small vessels of the injured tissue and aids in the control of hemorrhagei Histamine and heparin molecules subsequently are released from mast cells, which stimulate vasodilation and increase permeability of the capillaries. Blood flow to the area is increased, which in turn causes ltihneiccal signs of heat and redness. It also increases the supplies of oxygen and nutrients to the active cells of the idsasmuea.ged t
2. Fluid from plasma, composed of enzymes, antibodies, raontdeipns, pours into the affected area, causing swell- ifng o the soft tissue structures. This swelling irritates rdveelicate ne endings and causes pain and tenderness in tehcteeadff area.
3. Clot formation begins to take place, which slows bleeding. The clot also helps to isolate the wound from the invasion goefnpsatho and helps to prevent bacteria and toxins from spreading to surrounding soft tissue structures. A olot first forms when platelets become sticky and clump together. Fibrinogen, which is found in large quantities ionllethne sw tissue, is converted to an insoluble protein called fibrin. The fiHn is woven into a netlike structure tuhrartousnds the platelets and provides support and sotability t the newly formed clot. It also forms a framework to support the movement of cells throughout the lsoittes. C that form on external surfaces, such as skin, eventually dry to become scabs.
4. Large cells such as macrophages and neutrophils, a type
lohofiotedw b cell, move through blood vessels and
soquugeheze thr dilated capillaries to assist in the removal
of debris and microinvaders. These phagocytic cells are svhedo,rt li however, and can function for only a few hours before dying. Pus, which is an accumulation of dead and degenerated neutrophils and macrophages, may therefore collect in the injured area.
5. With increased blood flow, histamine and heparin are dispersed, and their levels drop in the affected area. The decrease in these molecules causes the return of normal capillary size and permeability. When capillaries return to normal size, blood flow and fluid leakage into the affected area abate. Swelling, heat, and redness begin to subside.
ORGANIZATION: THE FORMATION OF GRANULATION TISSUE
Wound repair begins soon after the injury occurs and con- thiinleues w dead cells and debris are removed from the area. In wounds that are infected, neutrophils and macrophages play a particularly critical role in the healing process, because they are responsible for phagocytizing and disposing of invasive microorganisms. The presence of pathogens inhibits healing.
As macrophages work to clear debris, a new, bright pink tissue, called granulation tissue, forms beneath the overlying blood clot or scab. Granulation tissue is composed of a layeg of collagen fibers that have been manufactured by fibroblasts. ft is richly infiltrated with small permeable capillaries that have branched off from existing capillaries in the yderesper la of the damaged tissue. These tiny new vessels poush up int the bed of collagen fibers and provide rich supplies of nutrients and oxygen to the hard-working fibro- cbrlaospths,amgeas, and neutrophils. Grossly, the capillaries
appear to be minute granules end therefore account for the name. Gnanulation tissue produces bacterium-inhibiting substances, which make it highly resistant to infection.
In some cases, granulation tissue becomes too thick and stands ou above the epithelial layer. This is known as proud flesh and may be surgically cut down to facilitate closure of the epithelial layer. Proud flesh is commonly seen in horses tvuhesatatihnaed s skin wounds.
REGENERATION OR FIBROSIS Epithelialization and scar tissue rWgahniliezaotion is occurring, epithelial cells around the
dwgoeusnd e actively divide to lay down a new layer of epi- itshseulieal t over the granulation tissue. This process is called epithelialization. Canneations between the scab and tkheenitnhgic epithelial layer are weakened, and the scab subsequently falls off. Fibroblasts in the granulation tissue coontinue t manufacture collagen fibers and ground sub- shtiacnhce, w are used to replace lost tissue and bridge the lwoowulyn,d. S the granulation tissue is completely replaced rboyufisb scar tissue, which contracts and assists in pulling tohuendw closed. When epithelialization is complete, the underlying scar may or may not be visible, depending on the severity of' the injury and on the extent of scar formation.
Although scar tissue is strong, it is less flexible than insosurme al t and cannot perform the function of the idsasmuea.ged t With time, scar tissue shrinks, but its pres- ielnl ce can st have detrimental effects on the organ as a owrhole. F example, if scar tissue forms in the wall of the heart, it can interrupt electrical pathways, weaken contractile capability, and result in decreased cardiac function. Similarly, icfcuitrso in the wall of the intestine or esophagus, it can decrease the diameter of the lumen and lead to obstruction cocrluosion. For this reason, dogs that have undergone esophageal surgery to remove a foreign body are likely to ehpaevaeteadr episode. The site of the first incision in the esophagus often heals with a thick, fibrous scar, which narrows the esophageal lumen and increases the possibility trhat anothe foreign body, such as a piece of bone or chew itnlolcye, w o again become lodged.
Ionmtihnealabd and thoracic cavities, healing is often associated with the formation of fibrous adhesions and tags, owvheirch c organs and form connections between multiple structures. Reentry into the abdomen to repeat a surgical procedure or to correct a complication therefore can be more difficult because of the formation of adhesions. Adhe- seidouncsecan r the visibility of important structures. They ecastnricrt normal shifting of bowel loops and can bind organs to the body wall or to the omentum. In addition, adhesions can be painful to the animal if they cause tension eblelt-wineneenr vwated structures.
CLASSIFICATIONS
eWpoauirnd r may be classified as first or second intention, depending on the mechanism of healing and the proximity ofunthde w edges. Wounds that heal via first intention are
thhicohse in w the edges of the wound are held in close apposition. These wounds may be superficial scratches or wounds that have been sutured or held closed with special
CLINICAL APPLICATION
The Clinical Patient and Healing
Some tissue types heal more readily than others. Epithe- iiah tissues such as skin and mucous membranes heal rapidly but smooth muscle and dense regular connective tissue have eimited reeenerative ability. Cardiac muscle and nervous tissue in the brain and spinal cord regenerate extremely slowly if at all and are often replaced by scar tissue. In addition, some patients heal more easily than other patients. Old, immunosuppressed, debfiftated, or sick animals heal more slowly than young, healthy, well-nourished animals. In this ew,ay, the ag overall health, and nutrition of patients are important factors in the rate and extent of healing. This is lwechtyive surgery is avoided in unhealthy animals and
rwahvyenionuts nutrition may be used in critically ill
opmatieents. S diseased or otherwise stressed animals, for example, may produce too much cortisol, which can inhibit the animal's ability to heal; incision sites may take weeks rather than days to close, and wounds from even superficial injuries my become chronic nightmares. In addition, some udrcuhgs, s as prednisone, can also delay healing if blood leevels ar high. Thus the clinician must consider the overall health and medical history of an animal before carrying out any procedure that subsequently requires the healing of tissue.
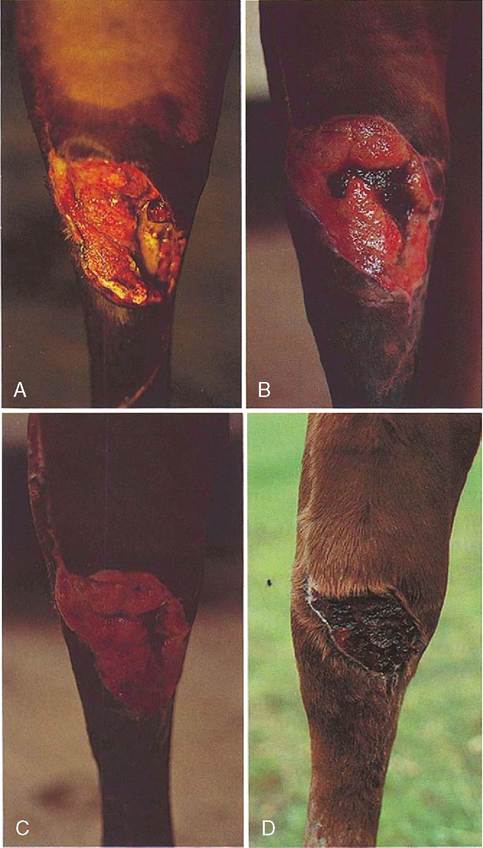
FIGURE 5-32 Second -intention wound healing in a horse. A, Wound on the anterior aspect of the hock in a gelding. Note the granulation tissue evident in B and C and the epithelial contraction that followed (D). Scarring remained after the wound healed, but this is well concealed in animals because of coverage by the hair coat. (From Melling M, Alder M: Equine practice, ed 3, Philadelphia, 1998, Saunders.)
bandages. During first-intention healing, the skin forms a primary union without the formation of granulation tissue or significant scarring. Second-intention healing occurs in wounds in which the edges are separated from one another, in which granulation tissue forms to close the gap, and in which scarring results (Figure 5-32).
TEST YOURSELF 5-7
1. In what ways are muscle fibers uniquely adapted for contraction?
2. List three types of muscle. How do they differ from one another?
3. What are the two basic cell types that make up neural tissue?
4. What is the most important function of neural tissue?
5. Describe the process of inflammation. What causes the clinical signs of heat, swelling, redness, and tenderness?
6. When does the healing process begin?
7. What is granulation tissue? Why is it important in the healing process?
8. Describe first- and second-intention wound repair.