Antiretroviral drugs
The clinical effectiveness of antiretroviral therapy has improved markedly over the last few years. Since 1996 in the developed world there have been dramatic falls in the incidence of new AIDS cases and AIDS-associated deaths.
Published data in the late 1990s estimated the mortality rate in patients with CD4 counts of less than 100 ? 106∕l had fallen by nearly two-thirds to patients, substantially reducing the risk of clinical disease progression and death. Reservoirs of HIV in latently infected resting T-lymphocytes and other long-lived cell populations makes it unlikely that HIV can be eradicated by antiretroviral therapy alone. Strategies to sustain suppression of viral replication in the long-term will be necessary.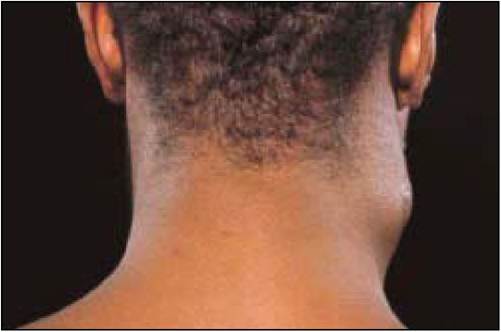
Figure 9.9 Immune reconstitution of disease: MAC lymphadenitis in a patient recently starting HAART
| Table 9.5 Targets for antiretroviral therapy | |
| Target | Treatment |
| Virus receptor and entry | Fusion inhibitors, chemokine receptor blockers |
| Reverse transcriptase | Inhibitor∕DNA chain terminators |
| RNAase | Inhibitors |
| Integration | Viral integrase inhibitors |
| Viral gene expression | Inhibitors of HIV regulatory genes and their products |
| Viral proteins synthesis | Enzyme inhibitors, for example, protease inhibitors |
| Viral budding | Interferons (also act at other sites of replication cycle) antibodies and ligands |
Box 9.5 Antiretroviral regimens
1.
2.
| 2 NRTIs: | eg. Zidovudine or Stavudine + Lamivudine or Didanosine |
| plus either | |
| 1 NRTI: | Nevirapine or Efavirenz |
| or | |
| 1 PI: | Nelfinavir, Saquinavir soft gel or a low dose Ritonavir boosted PI |
| or | |
| 2 PIs: | eg. Saquinavir + Ritonavir |
| 3 NRTIs: | Zidovudine, Lamivudine + Abacavir |
Antiretroviral regimens for the initial treatment of chronic infection in adults (2001). Choice would depend upon efficacy, tolerability, adherence and resistance profile of the regimen. Treatment guidelines are constantly reviewed and updated.
There are several potential targets for antiretroviral drugs in the viral replication cycle. Three classes of antiretroviral drugs are currently used in combination for the treatment of HIV infection, which target the activity of two viral enzymes. New therapeutic agents are constantly being evaluated.
Reverse transcriptase inhibitors
The first drugs made available for clinical use were inhibitors of the HIV reverse transcriptase enzyme. Before the virus can be integrated into the host cell genome DNA, a copy of the viral RNA has to be formed (pro-viral DNA). This is regulated by the specific HIV DNA polymerase: reverse transcriptase (RT). If a DNA copy is not formed, the viral RNA genome becomes susceptable to destruction by cellular enzymes.
The nucleoside reverse transcriptase inhibitors (NRTIs) are both competitive inhibitors of RT and DNA chain terminators. The normal 21 deoxynucleosides which are substrates for DNA synthesis link to form a chain by phosphodiester linkages bridging the 5l and 3l positions on the five carbon sugar molecule.
The 2l, 3l-dideoxynucleosides analogues are formed by the replacement of the 3l-hydroxy group by an azido (zidovudine), hydrogen or other group. These nucleoside analogues as substrates will bind to the active site of the HIV RT enzyme and will be added to the growing HIV proviral DNA chain. However, once inserted, the normal 5l to 3l links will not occur resulting in HIV proviral DNA chain termination.Genotypic mutations at various codons in the RT gene result in decreased susceptability of HIV to inhibition by the NRTIs. Several NRTIs are currently licensed for the treatment of HIV infection in combination regimens and newer agents with better tolerability and resistance profiles are under evaluation.
The non-nucleoside reverse transcriptase inhibitors (NNRTIs) are a group of structually diverse agents which bind to RT at a site distant to the active site resulting in confirmational changes at the active site and inhibition of enzyme activity. These agents show high antiviral activity in vitro and have relatively low toxicity. They are also highly specific, inhibiting the reverse transcriptase of HIV-1 but not HIV-2. As monotherapy, rapid emergence of resistant strains associated with single point mutations of the RT gene, high-level phenotype resistance and loss of antiviral effect occurs. The drugs therefore need to be combined with other antiretroviral agents, usually two NRTIs, to achieve and maintain an effective long-term treatment response.
Protease inhibitors
The protease inhibitors bind competitively to the substrate site of the viral protease enzyme. This enzyme is responsible for the post-translational processing and cleavage of a large structural core protein during budding from the infected cell. Inhibition results in the production of immature virus particles. Their potent anti-HIV activity and introduction to clinical use from 1996 was one of the main reasons for the observed substantial falls in morbidity and mortality associated with HIV infection in the developed world. However, tolerability, relatively high pill burden and poor adherence were frequent problems with the initial protease inhibitor containing regimens. Specific genotypic mutations in the protease gene can result in high levels of phenotype resistance to individual protease inhibitors and cross-resistance. New protease inhibitors are under evaluation.
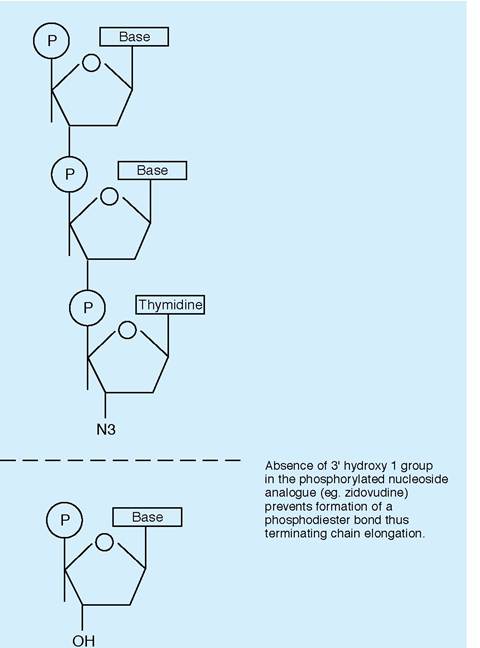
Figure 9.10 Mechanism of action of nucleoside reverse transcriptase inhibitors

Figure 9.11 MAC infection causing multiple cutaneous pustular lesions in a severely immunosuppressed patient after initiating HAART
More on the topic Antiretroviral drugs:
- Mixing Drugs
- Appendix 2 Interactions Between Antiretrovirals and Drugs Commonly Used to Treat Cardiovascular Disease
- INTRODUCTION: OVERVIEW OF COMPLICATIONS ASSOCIATED WITH HIV THERAPY
- From Now On
- INTRODUCTION
- Antiretroviral Therapy Today
- The treatment of HIV infection can be largely divided into: (i) specific antiviral agents that inhibit viral replication, (ii) measures that either treat or prevent (prophylaxis) its complications — namely opportunistic infections and tumours.
- Antiretroviral Therapy and Metabolic Disorders
- Medical problems of HIV-infected drug users
- The history of HIV is brief but dense. It is filled with aggressive debates, politics, human tragedy, a rich vein of research in medical science, and a dramatic change in drugs and tests in 1996 that translated immediately into better health and longer life.