Impact of Antiretroviral Treatments on Coronary Heart Disease
Although it is now clearly established that cART is linked to metabolic disorders, the long-term impact of these disorders is still being discussed. The first questions concerning an increase in the risk of CHD and the possible responsibility of PIs were raised in May 1998.
Henry et al. [15] described two cases of coronary artery disease in HIV-infected patients treated with PIs. One of the subjects had lipodystrophy and hypercholesterolemia with no other known risk factors, while the second patient had traditional risk factors such as smoking and cocaine use. Similar series of cases were reported in the medical literature in subsequent months [16-19, 21-23]. Gallet et al. [17] reported the cases of three patients with ischemic cardiopathy, including two with MI. All were being treated with PIs, and two had high lipid levels that were not present before antiretroviral treatment. Similarly1Vittecoq et al. [24] described four young patients with ischemic coronary events (MI in three cases). Three subjects were being treated with PIs, and three had major lipid disorders, associated with smoking and familial factors in two cases. Pas- salaris et al. [25] described six subjects with coronary artery disease who were receiving PI-containing combinations of antiretroviral drugs; four of these patients had acute MI. Coronary angiography revealed thrombotic lesions in two subjects, atheromatous lesions in two subjects, and both types of lesions in one subject. Friedl et al. [20] later described 14 coronary events in 11 subjects treated with PIs or NNRTIs. However, none of these studies proved a link between CHD and antiretroviral treatment.Some studies [26-32], but not others [33-36, 37], have shown a link between the risk of CHD and exposure to PIs (Table 1). Some suffered from methodological problems such as small sample size, median PI treatment periods of less than 12 months (two studies), and likely underreporting relative to the general population.
Some studies used different endpoints. In addition, the incidence of MI in people under 50 years of age is very low, meaning that lengthy follow-up of large populations (person-years) is necessary to observe a small difference between the HIV-infected population and the general population, or between two HIV-infected populations treated/not treated with cART.Far from increasing the incidence of cardiovascular events, a study from a database on administrative data [36] showed that cART tended to reduce the short-term risk in a population of more than 36,000 HIV- infected U.S. army veterans. Between 1995 and 2001, the rate of hospital admission for cardiovascular or cerebrovascular disease fell from 1.7 to 0.9 per 100 person-years (PY), while the overall mortality rate fell from 21.3 to 5.0 per 100 PY during the same period.
A study based on the French Hospital Database on HIV (FHDH) using DMI2 software (property of the French Ministry of Health) included 34,976 men with a total follow-up of 88,029 PY between 1996 and 1999 [31]. There were 49 cases of MI during 39,023 PI-exposed PY. The incidence rate of MI among subjects exposed to PIs between 1996 and 1999 was estimated according to the duration of PI therapy, based on three periods: infarction
157 912 PY
RR=1.49 (1.14-1.95)
recent use didanosine vs no recent use
PY, person-years; med, median
The expected incidence of MI in the general male population with the same age distribution was 10.8 cases per 10,000 PY. The estimated incidence of MI was 8.2 per 10,000 PY (95% CI=4.7-11.7) in group 1, 15.9 (95% CI=7.9-23.9) in group 2, and 33.8 (95% CI=15.4-52.1) in group 3 (Fig. 1). No significant difference was observed between the general male population of the same age and the patients treated with PIs for less than 18 months.
Although not significantly so, the risk of MI increased among patients treated with PIs for 18-29 months. In contrast, the risk of MI among patients exposed to PIs for 30 months or more was three times that of the general population (standardized morbidity ratio, SMR=2.9, 95% CI=1.5-5.0). Compared to patients exposed to PIs for less than 18 months, those treated for 18 months or more were at an increased risk of MI (SMR=1.9, 95% CI=1.0-3.1 for group 2 and SMR=3.6, 95% CI=1.8-6.2 for group 3). These results show that the risk of MI in HIV-infected men increases with the duration of PI treatment, while other antiretroviral classes are not associated with an increased risk of MI.How can this discordance between the results of Bozzette et al. [36] and Mary- Krause et al. [31] be explained? A direct comparison of the results of the two studies is impossible because they did not examine the same types of event. Mary-Krause et al. [31] examined admissions for and deaths from MI, whereas Bozzette et al. [36] only looked at admissions for cardiovascular disease, without taking deaths into account (especially deaths occurring outside hospital), probably leading to an underestimation of the number of cases. Also, this latter study grouped together deaths and admissions for cardiovascular and cerebrovascular disease. Holmberg et al. [28], who found an effect of PIs regarding the risk of MI, did not observe an increased risk of cerebrovascular disease. Results from the published DAD study (Data Collection on Adverse Events of Anti-HIV Drugs) indicated that there is an increasing risk of first cardio- and cerebrovascular events with longer exposure to combination antiretroviral treatment [38]. The ninth version of the international classification of diseases [46], used by Bozzette et al. [36], includes codes 410 (acute MI), 411 (other acute and subacute forms of ischemic heart disease), 413 (angina pectoris), and 414 (other forms of chronic ischemic heart disease), whereas Mary-Krause et al. [31] used only code 410.
It would be interesting to study the impact of PIs on each pathology separately. It should be noted that, although not significant, Bozzette et al. observed a higher risk of admission for cardiovascular diseases [36] among subjects exposed to PIs for 24 months as compared with 0 months (RR=1.23). It is surprising that the incidence of admissions for cardiovascular disease-more than 10 cases per 1,000 PY-observed in the study by Bozette et al. [36] was much higher than the incidence rates of CHD observed among seropositive American subjects exposed to PIs in other studies (5.9-6.6 events per 1,000 PY) [30, 35]. It is also surprising that Bozzette et al. found that the rate of CHD fell with time despite the increasing age of HIV-infected subjects.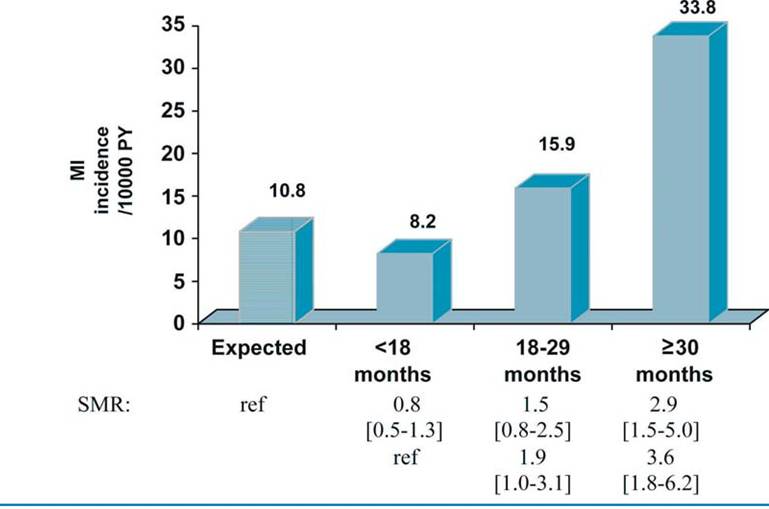
Fig. 1 Incidence of myocardial infarction (MI) per 10,000 person-years (PY) among HIV-infected men according to the duration of PI exposure (in months) compared to the incidence of MI among the general male population of the same age. The standardized morbidity ratios (SMR) with their 95% confidence intervals in brackets were used to test the differences between incidence rates. (From [31], with permission)
A recent update of the study of Bozette et al [37] continues to find hazards for serious cardiovascular events near 1.0 for exposure to cART. Nevertheless, the HR of cART that includes an NNRTI or a PI, even non significant, is equal to 1.22 (95% CI=0.77- 1.92) and the HR of cART that includes a PI only is equal to 1.28 (95% CI=0.71-2.30).
The DAD study [29], a prospective observational study of 23,468 patients enrolled in 11 cohorts on 3 continents from December 1999 to July 2002, showed a similar relationship between exposure to combination antiretroviral therapy (including PIs or NNRTIs) and the risk of MI to that found by Mary- Krause et al. [31], the risk increasing with the duration of cART. In the same way, Moore et al.
[30] reported a study of 2,671 subjects followed up after 1 January 1996, in which the risk of cardiovascular events was higher among subjects exposed to PIs. Of 3,083,209 individuals analyzed among them, 28,513 were HIV-infected. Currier et al. [44] found a higher incidence of CHD among young men and women with HIV infection than that among non-HIV-infected individuals. Their results also suggest that any exposure to potent combination antiretroviral therapy may contribute to the incidence of CHD among younger individuals when controlling for certain comorbidities.An update of the DAD study [32] on 23,437 subjects corresponding to 94,469 person-years (PY) of follow-up among them 345 MI showed an incidence of 3.7/1,000 PY with a decrease between 1999 and 2005. The incidence increased with increasing length of exposure to PI with an incidence increased from 1.5 per 1,000 PY among those not exposed to PI to 6.0 per 1,000 PY among those exposed to PI. In addition, the relative rate per year of exposure to PI was 1.16 (95% CI=1.10-1.23), result found as well by Klein et al. [47], which corresponds to a doubling of the risk over a 5-year period of exposure, whereas for non-nucleo- side reverse transcriptase inhibitors it was 1.05 (95% CI=0.98-1.13).
Recent results reported by the D:A:D group at the 2008 CROI meeting [39], and published in The Lancet [40], showing that recent use of abacavir and didanosine (current use or interruption less than 6 months previously) was associated with an increased risk of myocardial infarction (MI) need to be confirmed or not by other studies.
The Strategies for Management of Antiretroviral Therapy (SMART) study [48] recently showed an increased risk of cardiovascular disease in patients whose antiretroviral therapy was interrupted when their CD4+ cell count reached a certain level as opposed to patients who received continuous treatment. This international randomized trial, conducted in 318 sites in 33 countries, had enrolled 5,472 patients when it was stopped.
The HIV-infected persons who had a CD4+ cell count of more than 350/mm3 were randomly assigned to the continuous use of antiretroviral therapy (the viral suppression group) or the episodic use of antiretroviral therapy (the drug conservative group) until the CD4+ count decreased to less than 250/mm3. This trial was stopped because episodic antiretroviral therapy increased the risk of opportunistic disease or death from any cause, as compared with continuous antiretroviral therapy (HR=2.6, 95% CI=1.9-3.7). The risk for major cardiovascular, renal or hepatic disease was also higher in the episodic group (HR=1.7, 95% CI=1.1-2.5). So, these drug conservative strategy guided by the CD4 is not recommended. One of the most discussed hypotheses is that treatment may contribute to atherosclerotic plaque formation and that inflammation, due to viral load replication rebond following interruption of treatment, should support the destabilization of these atherosclerotic plaques.The increased risk of MI observed just after the advent of PI could be in part explained by a population who lived longer, and so the aging of the population which is at higher risk of cardiovascular diseases; by the chronic inflammatory state of HIV-infection, by the impact of known risk factors or CHD as smoking, and by the metabolic effects of antiretroviral treatment. Nevertheless, although today it is admitted that incidence of CHD was higher in HIV-infected patients than in the general population, links between viral infection, antiretroviral treatment, especially the impact of new antiretroviral drugs which have potentially less metabolic disturbances than PI, and the increase of MI incidence need to be precise even if we are not able to study each drug separately.
More on the topic Impact of Antiretroviral Treatments on Coronary Heart Disease:
- Ischemic Heart Disease
- Barbaro Giuseppe, Boccara Franc (eds.). Cardiovascular Disease in AIDS. 2nd edition. — Springer,2009. — 169 p., 2009
- Myocarditis or Acute Coronary Syndrome?
- Antiretroviral Therapy Today
- Common HIV Therapies and the Heart
- Interstitial Lung Disease