Opportunistic Infections
GENERAL PRINCIPLES
• Potent ART has decreased the incidence, changed the manifestations, and improved the outcome of OIs. However, OIs are still a common presentation of unrecognized HIV infection.
• A clinical syndrome associated with the immune enhancement induced by potent ART, IRIS, generally presents as local inflammatory reactions. Unmasking IRIS is when a patient develops symptoms of an OI while on ART treatment with no previous symptoms or indications of the patient having that OI previous to immune reconstitution. Paradoxical IRIS is when a patient is known to have a particular OI and worsens while on ART with immune reconstitution. Examples include recurrent symptoms of cryptococcal meningitis, paradoxical reactions with TB reactivation, localized Mycobacterium avium complex (MAC) adenitis, aggravation of hepatitis viral infection, and CMV vitreitis soon after the initiation of potent ART.
• In the case of IRIS, ART is usually continued, and the addition of low-dose steroids might decrease the degree of inflammation. TB and cryptococcal meningitis are the only OIs for which delay of starting ART is recommended to prevent IRIS.
• Additional details with updates may be found in the Guidelines for the Prevention and Treatment of Opportunistic Infections in HIV-Infected Adults and Adolescents.18
TREATMENT
• Prophylaxis for OIs can be divided into primary and secondary prophylaxis.
• Primary prophylaxis is established before an episode of OI occurs. Institution of primary prophylaxis depends on the level of immunosuppression as judged by the patient's CD4 cell count and percentage (Table 16-2).
TABLE 16-2
OPPORTUNISTIC INFECTION PROPHYLAXIS
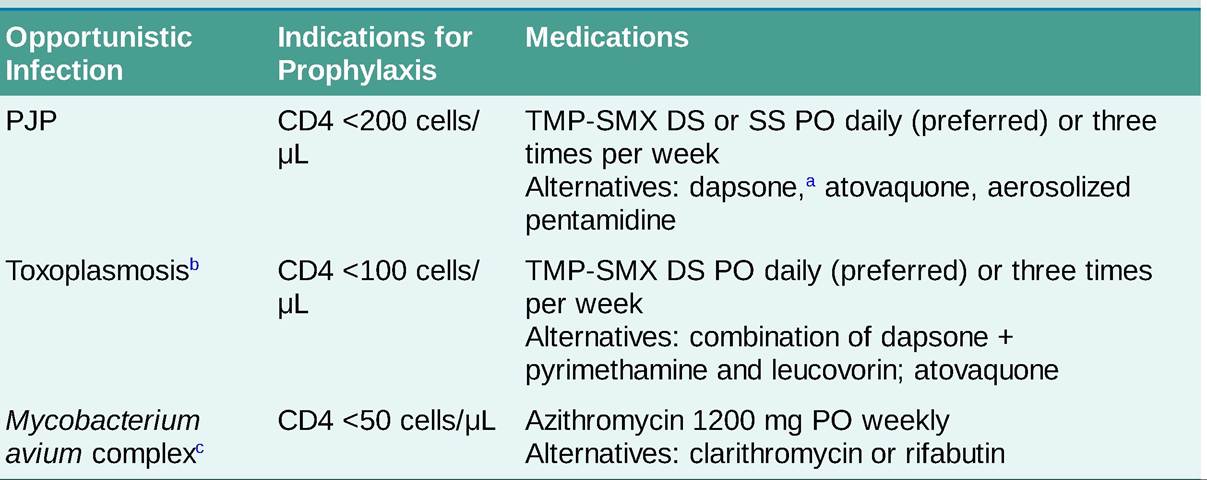
DS, double strength; PJP, Pneumocystis jirovecii pneumonia; TMP-SMX, trimethoprim-sulfamethoxazole. aGlucose-6-phosphate dehydrogenase (G6PD) testing should be done for dapsone.
bIf toxoplasmosis IgG is positive.
cNot recommended if patient is on effective ART.
• Secondary prophylaxis is instituted after an episode of infection has been adequately treated. Most OIs will require extended therapy.
• Withdrawal of prophylaxis: Recommendations suggest withdrawing primary and secondary prophylaxis for most OIs if sustained immunologic recovery has occurred (CD4 cell counts consistently gt;150-200 cells#8725;#956;L).18
More on the topic Opportunistic Infections:
- Opportunistic infections
- HIV Infection, Opportunistic Infections, and Vascular Disease
- Tuberculosis
- The treatment of HIV infection can be largely divided into: (i) specific antiviral agents that inhibit viral replication, (ii) measures that either treat or prevent (prophylaxis) its complications — namely opportunistic infections and tumours.
- Many cardiac complications in acquired immunodeficiency syndrome (AIDS) that may be faced by emergency department (ED) physicians are due to opportunistic infections or malignancy, but they may also be associated with other aspects of human immunodeficiency virus (HIV) disease and its treatment (Table 1) [1].
- Neurological complications of HIV-1 infection, due either to the immunosuppression (opportunistic infections and neoplasms) or the neurotropism of the virus, are common and add considerably to the morbidity and mortality of the infection
- Genitourinary Infections
- HERPETIC VIRAL INFECTIONS
- Hepatobiliary Infections
- Infective Endocarditis