Opportunistic infections
Box 8.4 Focal lesions in AIDS
Ģ Toxoplasmosis
Ģ Primary CNS lymphoma
Ģ Tuberculoma
Ģ PML
Toxoplasma gondii
Toxoplasmsosis in HIV infection is usually a reactivation of latent infection in individuals who have been exposed previously to the organism.
The clinical presentation is with headache with rapidly evolving focal neurological deficits over one to two weeks which include hemiparesis, dysphasia, visual field deficits, movement disorders (chorea/athetosis, parkinsonism) and seizures. Rarely, toxoplasmosis may affect the spinal cord and present with a myelopathy or a cauda equina syndrome. Blood serology for T. gondii is only helpful if negative since this makes the diagnosis less likely. Patients should have their toxoplasma serology documented at the first diagnosis of HIV infection. The risk of developing toxoplasma encephalitis in IgG seropositive patients is between 12% and 30%. These patients should be offered primary prophylaxis with co-trimoxazole at CD4 counts below 200.
Figure 8.2 T2-weighted MRI scan showing multiple rounded or oval abscesses before treatment in cerebral toxoplasmosis
CT/MRI shows multiple enhancing lesions with mass effect in the region of the basal ganglia and at the grey/white interface. A response to treatment is seen in 85% by day 7 and in over 90% by day 14. Repeat imaging should be performed after two weeks even if there is clinical improvement in cases of mixed pathology.
In patients with significant mass effect and cerebral oedema who are in danger of coning, additional treatment with dexamethasone will be necessary. A deterioration after this has been tailed off makes it necessary to consider a biopsy.
Box 8.5 Meningitis in HIV infection
Fungal
Ģ Cryptococcus neoformans
Bacterial
Ģ Mycobacterium tuberculosis
Ģ Listeria monocytogenes
Ģ Streptococcus pneumoniae
Ģ Treponema pallidum
Viral
Ģ HIV
Ģ Herpes simplex, herpes varicella zoster
Cryptococcus neoformans
C.
neoformans is a ubiquitous organism acquired by inhalation. Patients with meningitis may present acutely or insidiously over days or weeks with a headache, general malaise, confusion or seizures. The classical signs of meningism Ś neck stiffness, photophobia and Kernig's sign Ś are frequently absent.Brain imaging is usually normal but MRI may reveal small abcesses Ś cryptococomas. The CSF cell count and protein may be normal and the diagnosis is confirmed by the presence of cryptococcal antigen in the CSF in 95% of cases. India ink staining is positive in 75%. 85% of cases are culture positive Ś the gold standard. Measurement of the serum cryptococccal antigen is a useful screening tool in patients presenting with headache or fever but should not be considered definitive.
Box 8.6 Poor prognostic features of AIDS-related cryptococcal meningitis
Ģ Relapse episode
Ģ CSF cryptococcal Ag titre > 1:10 000
Ģ Positive India ink preparation
Ģ Hyponatraemia
Ģ Culture of extrameningeal cryptococcus
Intracranial hypertension in the absence of mass lesions or hydrocephalus is an important cause of mortality and visual failure in approximately 20%. This is managed by repeated lumbar punctures or by the insertion of a lumbar or ventricular drain.
JC virus
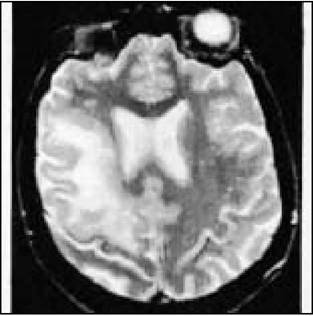
Figure 8.3 T2-weighted MRI scan showing large area of high signal in one hemispheric white matter with no mass effect. Biopsy proved progressive multifocal leukoencephalopathy
Progressive multifocal leucoencephalopathy (PML) results from reactivation of the JC virus in immunosuppressed individuals. 80% of the general population will have been exposed to this virus as a banal childhood upper respiratory infection and have positive serology.
The presentation is with slowly evolving focal neurological deficits such as a hemiparesis, visual field and language problems and incoordination due to cerebellar involvement.
Occasionally patients develop a dementia in association with these focal abnormalities. Symptoms and signs of raised intracranial pressure are absent although headache may be a feature.Blood serological testing is unhelpful. Cranial CT shows non-enhancing areas of low attenuation in the white matter. MRI shows characteristic scalloping abnormalities at the grey/white interface with no mass effect or enhancement. The diagnosis may be confirmed by isolating JC virus by polymerase
chain reaction (PCR) techniques in the CSF in 75% of cases. If this is negative, a brain biopsy may need to be performed. This typically shows areas of focal demyelination, bizzare enlarged astrocytes and abnormal oligodendrocytes with inclusions which stain for JC viral antigens.
Box 8.7 Clinical signs and symtoms in PML
Ģ Motor function abnormalities (including hemiparesis)
Ģ Mental status charges
Ģ VIIth cranial nerve palsy
Ģ Cerebellar syndrome
Ģ Language disorders (dysphasia)
Ģ Visual problems (for example hemianopia)
Ģ Seizures
There is at present no specific treatment for PML. Cytosine arabinoside has been shown to be ineffective but trials are underway looking at the efficacy of drugs such as cidofovir (an anti CMV drug) and alpha interferon. Improvement in immune function with HAART has resulted in significantly better survival times.
Cytomegalovirus
Over 90% of HIV-infected individuals have serological evidence of CMV infection. The neurological complications, which occur at CD4 counts below 50/mm3, include retinitis, a cauda equina syndrome, an encephalitis and a mononeuritis multiplex. Apart from retinitis, the other complications occur infrequently.
CMV retinitis
The initial presentation of CMV retinitis depends upon the location Ś patients may be asymptomatic, complain of floaters, lose peripheral vision or if the lesions are centred around the macula, have poor visual acuity. Patients will often have evidence of CMV disease elsewhere such as colitis and such patients need to be screened for retinitis regularly.
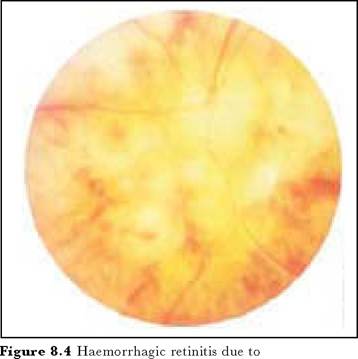
cytomegalovirus
On fundoscopy, there is a perivascular yellow-white infiltrate with retinal haemorrages. The differential diagnosis includes retinal complications of toxoplasmosis, lymphoma, syphilis, herpes zoster and herpes simplex.
CMV polyradiculopathy
This well-recognised syndrome presents over a period of days with back pain followed by the development of a progressive flaccid weakness of the legs with sensory loss and sphincter disturbance. Imaging studies which are essential to exclude compressive lesions due to, for example, lymphoma are normal or may show thickened nerve roots. The CSF shows a characteristic neutrophil pleocytosis which is unusual in a viral infection. Without treatment there is a progression of the neurological deficits, with death in 2 or 3 months.
CMV encephalitis
Although evidence of CMV infection is often found in the brains of patients dying from AIDS, the clinical correlates are unclear. A CMV encephalitis needs to be considered in patients presenting with a rapidly progressive encephalitis with cranial nerve palsies and seizures. CMV may be isolated from the CSF using PCR.
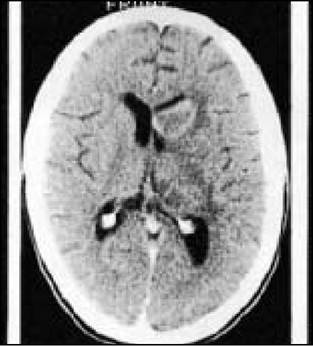
Figure 8.5 Enhancing right frontal mass lesion due to lymphoma
More on the topic Opportunistic infections:
- Opportunistic infections
- Opportunistic Infections
- HIV Infection, Opportunistic Infections, and Vascular Disease
- Opportunistic Infections
- Tuberculosis
- The treatment of HIV infection can be largely divided into: (i) specific antiviral agents that inhibit viral replication, (ii) measures that either treat or prevent (prophylaxis) its complications Ś namely opportunistic infections and tumours.
- Many cardiac complications in acquired immunodeficiency syndrome (AIDS) that may be faced by emergency department (ED) physicians are due to opportunistic infections or malignancy, but they may also be associated with other aspects of human immunodeficiency virus (HIV) disease and its treatment (Table 1) [1].
- Neurological complications of HIV-1 infecŁtion, due either to the immunosuppression (opportunistic infections and neoplasms) or the neurotropism of the virus, are common and add considerably to the morbidity and mortality of the infection
- The Natural History of HIV Infection
- Genitourinary Infections