Cervix
Squamous cell neoplasia
Cytological screening in high-resource countries decreased cervical carcinoma by 50% to 85%; however, worldwide, cervical cancer remains the fourth most common cancer in women.
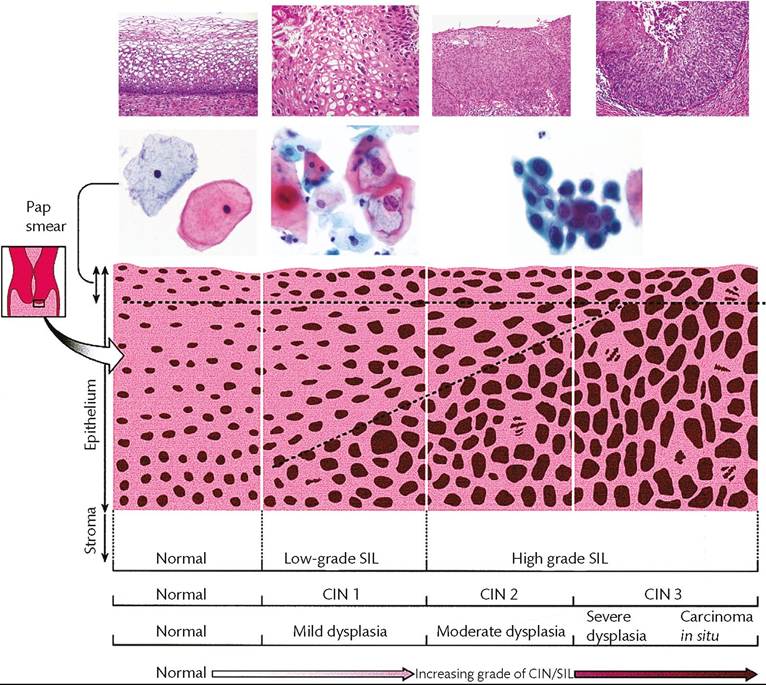
Figure 70.3 Inter-relations of naming systems in precursor cervical lesions. This chart integrates multiple aspects of the disease. It illustrates the changes in progressively more abnormal disease states and provides translation terminology for the dysplasia/carcinoma in situ (CIS) system, cervical intraepithelial neoplasia (CIN) system, and the Bethesda system. The scheme also illustrates the corresponding cytological smear resulting from exfoliation of the most superficial cells as well as the equivalent histopathological lesions (top row). SIL, squamous intraepithelial lesion.
Cervical squamous intraepithelial neoplasia (SIL)
Cervical squamous intraepithelial neoplasia SIL (CIN) is a spectrum of intraepithelial changes that begins with minimal atypia and progresses through stages of greater intraepithelial abnormalities to invasive squamous cell carcinoma. The terms CIN, dysplasia, CIS, and squamous intraepithelial lesion are commonly used interchangeably (1, 2) (Figure 70.3).
Epidemiology and molecular pathogenesis
HPV infection leads to CIN and cervical cancer. Low- grade SIL (CIN 1) is a permissive infection (i.e. HPV is episomal, freely replicates, and thereby causes cell death). Huge numbers of virus must accumulate in the cytoplasm before being visible as a koilocyte (Figure 70.3). In most cases of higher-grade SIL (CIN 2—3), viral DNA integrates into the cell genome. Proteins encoded by the E6 and E7 genes of HPV 16 respectively bind and inactivate p53 and Rb proteins, thereby invalidating their tumour suppressor functions.
After HPV integrates into host DNA, copies of the whole virus do not accumulate and koilocytes are absent in many cases of high-grade dysplasia and all invasive cancers. Cells in high-grade CIN usually contain HPV types 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 68. HPV types 16 and 18 are found in 70% of invasive cancers; the other high- risk types account for another 25% (4).Pathology
SIL (CIN) is nearly always a disease of metaplastic squamous epithelium in the transformation zone. The normal process by which cervical squamous epithelium matures is disturbed in CIN, as evidenced morphologically by changes in cellularity, differentiation, polarity, nuclear features, and mitotic activity. High-grade SIL (CIN 3) is synonymous with severe dysplasia and CIS. The sequence of histological changes from low-grade SIL (CIN 1) to high-grade SIL (CIN 2-3) is shown in Figure 70.3 (1, 2).
Clinical features
The mean age at which women develop SIL (CIN) is 24-27 years for low-grade SIL (CIN 1) and CIN 2, and 35-42 years for CIN 3. Based on morphological criteria, half of cases of CIN 1 regress, 10% progress to high-grade SIL (CIN 3), and less than 2% become invasive cancer. The average time for all grades of dysplasia to progress to high-grade SIL (CIN 3) is about 10 years. At least 20% of cases of high-grade SIL (CIN 3) progress to invasive carcinoma in that time (1).
When SIL (CIN) is discovered, colposcopy, together with a Schiller test, delineates the extent of the lesion and indicates the areas to be biopsied. Diagnostic endocervical curettage also helps to determine the extent of endocervical involvement. Women with low-grade SIL
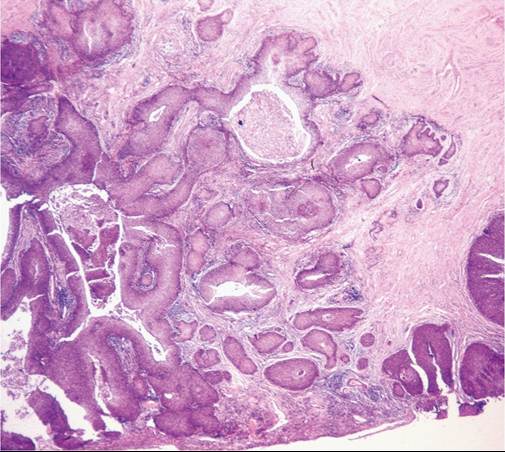
Figure 70.4 Microinvasive squamous cell carcinoma. The tumour invades 5 mm deep and 4 mm wide. This tumour is stage IA2 according to FIGO's classification.
(CIN 1) are often followed conservatively (i.e. repeated Pap smears plus close follow-up).
High-grade lesions are treated according to the extent of disease. The loop electrosurgical excision procedure, cervical conization (removal of a cone of tissue around the external os), cryosurgery, and (rarely) hysterectomy may be performed (1).Microinvasive (superficially invasive) squamous cell carcinoma
This is the earliest stage (IA) of invasive cervical cancer. In this setting, stromal invasion usually arises from overlying SIL (CIN) (Figure 70.4). Staging of microinvasive disease is based on width and depth of invasion, defined as follows:
• Invasion less than 3 mm (stage IA1) or 5 mm (stage IA2) below the basement membrane.
The earliest invasive changes (‘early stromal invasion’) appear as tiny irregular epithelial buds emanating from the base of high-grade SIL (CIN 3) lesions. These small (<1 mm) tongues of neoplastic epithelial cells do not affect the prognosis of high-grade SIL (CIN 3) lesions; hence, both can be treated similarly with conservative surgery. In the 2009 International Federation of Gynecology and Obstetrics (FIGO) classification, early stromal invasion was excluded from stage IA1. Some gynaecological oncologists further limit microinvasive carcinoma to tumours lacking lymphovascular invasion. Stage IA2 tumours are associated with lymph node metastases in about 8% of cases whereas those that invade up to 3 mm (stage IA1) have only a 1-2% risk of lymph node metastases. Conization or simple hysterectomy generally cures microinvasive cancers less than 3 mm deep (1-3).
Invasive squamous cell carcinoma
Pathology
Early stages of cervical cancer are often poorly defined lesions or nodular and exophytic masses. If the tumour is within the endocervical canal, it can be an endophytic mass, which can infiltrate the stroma and cause diffuse cervical enlargement. Most tumours are non-keratinizing, with solid nests of large malignant squamous cells and no more than individual cell keratinization. Most remaining cancers show nests of keratinized cells in concentric whorls, so-called keratin pearls.
Cervical cancer spreads by direct extension, through lymphatic vessels and only rarely by the haematogenous route. Local extension into surrounding tissues (parametrium) results in ureteral compression (stage IIIB); the corresponding clinical complications are hydroureter, hydronephrosis, and renal failure secondary to ureteric obstruction— the most common cause of death (50% of patients). Bladder and rectal involvement (stage IVA) may lead to fistula formation. Metastases to regional lymph nodes involve paracervical, hypogastric, and external iliac nodes. Overall, tumour growth and spread are relatively slow, since the average age for patients with high-grade SIL (CIN 3) is 35-40 years; for stage IA carcinoma, 43 years; and for stage IV, 57 years (1-3).
Clinical features
HPV testing is the most reliable screening test for detecting cervical cancer, and is supplanting cytology in some screening algorithms in women aged over 25 years. Co-testing with HPV testing and cytology is also recommended in women aged over 30 years. Where HPV testing is not available, the Pap smear remains the most commonly used screening test, but quality assurance is a vital component of such screening programs.
The clinical stage of cervical cancer is the best predictor of survival. Overall 5-year survival is 60%, and by each stage it is as follows: I, 90%; II, 75%; III, 35%; and IV, 10%. About 15% of patients develop recurrences on the vaginal wall, bladder, pelvis, or rectum within 2 years of therapy. Radical hysterectomy is favoured for localized tumour, especially in younger women; radiation therapy, chemotherapy, or combinations of the two are used for more advanced tumours (1-3).
Endocervical adenocarcinoma
This tumour makes up 20% of cervical cancers. The incidence of cervical adenocarcinoma has increased recently, with a mean age of 56 years at presentation. Most tumours are of the endocervical cell (mucinous) type. These tumours are often associated with adenocarcinoma in situ and are frequently infected with HPV types 16 and 18 (1, 2).
Adenocarcinoma in situ generally arises by the squamocolumnar junction and extends into the endocervical canal. Associated highgrade squamous cell CIN occurs in 40% of cases of adenocarcinoma in situ. Invasive adenocarcinoma typically presents as a polypoid or papillary mass. Adenocarcinoma of the endocervix spreads by local invasion and lymphatic metastases, but overall survival is somewhat worse than for squamous carcinoma.