Endocrinology
Mechanisms of actions of hormones
Cell surface receptors: hormones act in an autocrine, paracrine, or endocrine manner. Certain hormones (steroids, insulin-related growth factors, thyroid hormones) are bound to carrier proteins.
Only free hormone is active and can bind to specific receptors and have an effect. Neurotransmitters and peptide hormones act mainly through cell surface receptors.Steroid hormones, thyroid hormones, retinoic acid, and vitamin D act through nuclear receptors. Some of the receptors exist in the cytoplasm and some in the nucleus. Once these hormones bind to their receptors, they all act in the nucleus to alter gene expression.
Hypothalamus and pituitary
Embryologically, both the thalamus and the hypothalamus develop in the lateral walls of the diencephalon and the cavity becomes the
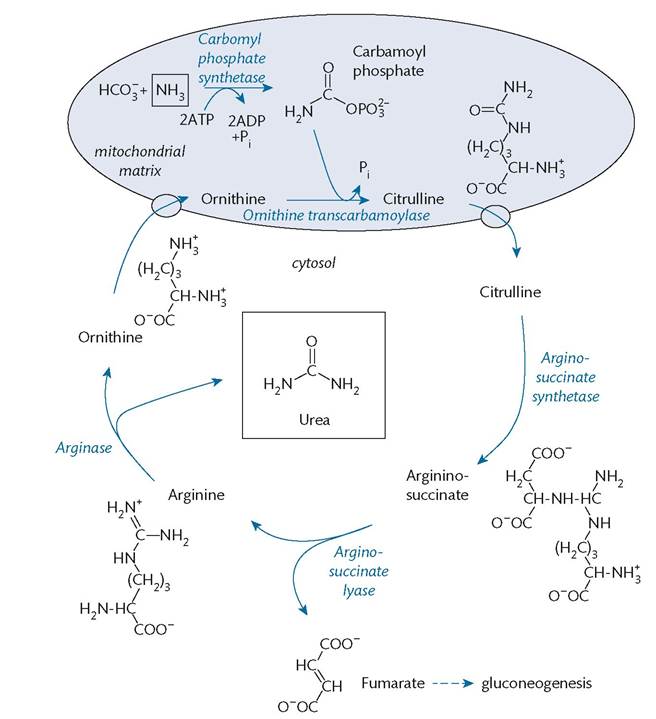
Figure 1.23 The urea cycle.
Reproduced from Neil Herring and Robert Wilkins, Biochemistry and metabolism, in: Basic Science for Core Medical Training and the MRCP, Oxford University Press (2015) with permission from Oxford University Press.
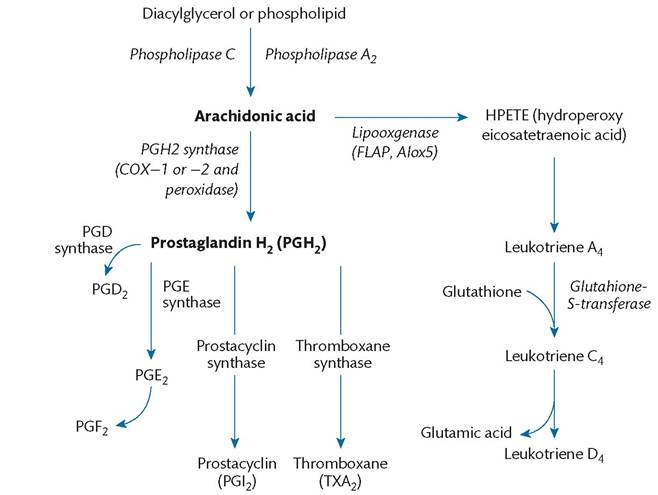
Figure 1.24 Pathways for metabolism of arachidonic acid into prostaglandins and leukotrienes.
Reproduced from Gary A. Rosenberg, Glucose, Amino Acid, and Lipid Metabolism, in: Molecular Physiology and Metabolism of the Nervous System: A Clinical Perspective, Oxford University Press, (2012) with permission from Oxford University Press.
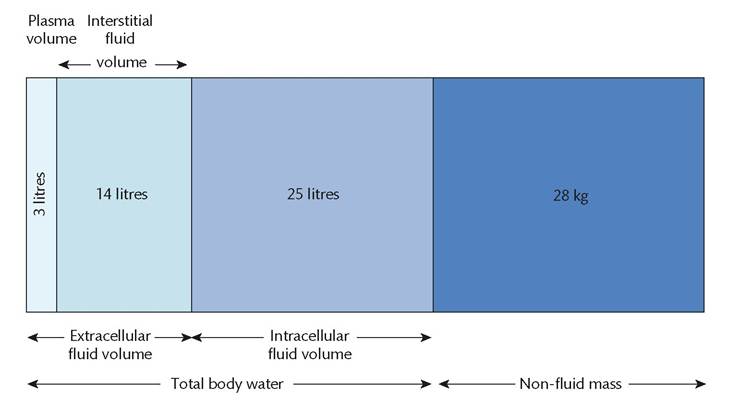
Figure 1.25 Body fluid compartments.
Reproduced from Anthony Delaney, Physiology of body fluids, in: Oxford Textbook of Critical Care (eds. Andrew Webb, Derek Angus, Simon Finfer, Luciano Gattinoni, and Mervyn Singer) Oxford University Press (2016), with permission from Oxford University Press.
third ventricle. The pituitary develops in close association and is made up of two parts: adenohypophysis, the anterior pituitary, and neurohypophysis, the posterior pituitary. The anterior pituitary develops from the ventral ridges of primitive neural tube, which are pushed forward by the developing Rathke's pouch. By 7 weeks of gestation, the sella floor has formed and the pituitary starts to form under the influence of the hypothalamus. The posterior pituitary is in contact with the hypothalamus while the anterior pituitary is connected to the hypothalamus via a portal system. The hypothalamus, pituitary stalk, and pituitary are supplied by carotid arteries via the superior and inferior hypophyseal arteries (Figure 1.30).
The posterior pituitary is a ventral extension of the central nervous system, where the hypothalamic hormones oxytocin and vasopressin are released (Boxes 1.1 and 1.2).
Thyroid
Embryologically, this is the first endocrine gland to develop. Its development starts 24 days after fertilization. It develops from the floor of the primitive pharynx as ‘thyroid diverticulum'. Thyroid hormone secretion starts at about 11 weeks of pregnancy.
Table 1.2 Average electrolyte composition of body fluid compartments
| Electrolyte | I ICF (mmol/L) | I ECF (mmol/L) | I Plasma interstitial | |||||||||||||||||||||||||||||||
| Sodium | 10 | 140 | 145 | |||||||||||||||||||||||||||||||
| Potassium | 155 | 3.7 | 3.8 | |||||||||||||||||||||||||||||||
| Chloride | 3 | 102 | 115 | |||||||||||||||||||||||||||||||
| Bicarbonate | 10 | 28 | 30 | |||||||||||||||||||||||||||||||
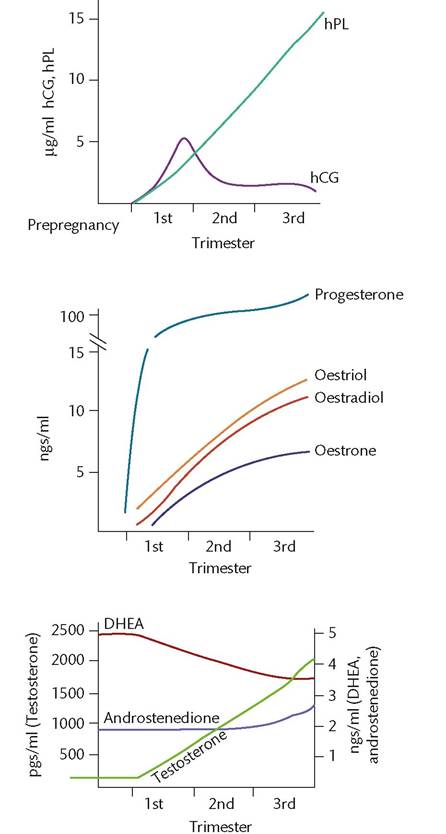
| Calcium (ionized) | feedback), which interacts with melanocortin receptors in the skin (21, p. 112). Effects of pregnancy and lactation The placenta can synthesize and secrete proteins but cannot synthesize steroids. Several maternal serum hormone changes occur during pregnancy (Figure 1.33). Placental proteins: human chorionic gonadotropin (hCG) peaks at 10 weeks. Human placental lactogen (hPL) rises with placental weight. It induces insulin resistance. Oestrogens (oestradiol, oestriol, and oestrone) are synthesized in the placenta from DHEA produced by the fetus and increase to term. Androgens are derived from the fetoplacental unit and testosterone levels rise tenfold. Progesterone is mainly synthesized by the corpus luteum in the first 2-3 months of pregnancy. Levels rise up to term. Pituitary hormones: LH and FSH decline while prolactin rises to term. Thyroid hormones (total T4 and T3) rise during the first trimester and then plateau. Cortisol increases to three times prepregnancy values and aldosterone plateaus at 34 weeks. Several hormones during pregnancy stimulate breast growth (oestrogen, progesterone, hPL, prolactin, cortisol, and insulin). High concentrations of oestrogens inhibit lactation. After delivery, when the oestrogen levels fall, lactation is initiated by prolactin. Prolactin promotes milk formation and is released from the anterior pituitary. Prolactin is also released in response to suckling. Box 1.2 Pituitary hormones • Luteinizing hormone • Follicle-stimulating hormone • Proopiomelanocortin (POMC) • Adrenocorticotropin • Beta-endorphin • Melanocyte-stimulating hormone (MSH) • Thyrotropin • Prolactin • Growth hormone Pharmacokinetics Pharmacokinetics refers to how a drug moves through an individual's body (22). A drug's pharmacokinetics includes absorption, distribution, metabolism, and elimination, which affect the drug's concentration at the site of action and its effect. Clearance is the volume of blood from which a drug is completely eliminated in a period of time. It depends on liver metabolism or renal blood flow. Volume of distribution is the volume of fluid into which a drug distributes. It depends on protein binding and liquid solubility. Half-life is the time taken for the concentration of drug in blood to fall by half. Bioavailability is the proportion of drug, which reaches the systemic circulation unchanged. First-pass metabolism involves the metabolic breakdown of a drug during its first pass through the liver. In steady-state concentration, the peak and the trough blood concentrations of the drug remain the same with repeated equal doses.Pharmacodynamics Pharmacodynamics refers to an individual's therapeutic response to a drug and is determined by the drug's affinity and activity at its site of action. Drugs mainly act on four different targets: 1. Receptors 2. Enzymes 3. Membrane ionic channels 4. Metabolic processes such as DNA synthesis. Drug metabolism Most drugs are metabolized in the liver. Water-soluble drugs are excreted by the kidneys. Lipid-soluble ones pass across the cell membrane of the hepatocytes and then access microsomal P450 enzymes. Drug metabolism in the liver involves simple oxidation, which creates hydroxyl groups and conjugation of these with various sulphate, acetyl, methyl, and glycyl groups. These processes increase solubility and facilitate renal excretion. The mechanisms involved in renal excretion are filtration at the glomerulus, transport through the epithelium of the kidney tubules, and diffusion. Renal clearance is important as it affects the plasma concentration of the drug. Drug interactions Drugs can interact with each other. Enzyme inducers and enzyme inhibitors are common examples of such interactions. Enzyme inducers: carbamazepine, phenobarbitone, phenytoin, griseofulvin, and rifampicin belong to this category. These drugs increase the activity of enzyme systems. Drugs metabolized by the same enzymes are metabolized and eliminated more rapidly. As a result, their plasma concentrations will fall with possible clinical implications. Efficacy of oral contraceptives is reduced by enzyme inducers. Enzyme inhibition: drugs such as erythromycin, metronidazole, sulphonamides, and cimetidine have the potential to increase
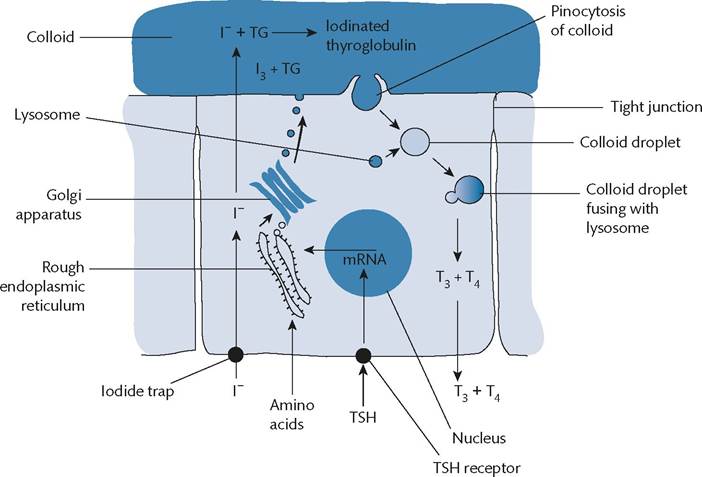
Figure 1.31 The cellular processes involved in the synthesis and subsequent release of the thyroid hormones. Note that thyroid-stimulating hormone (TSH) stimulates both the synthesis of thyroglobulin (TG) and the secretion of triiodothyronine (T3) and thyroxine (T4).Reproduced from Neil Herring and Robert Wilkins, Endocrinology, in: Basic Science for Core Medical Training and the MRCP, Oxford University Press (2015) with permission from Oxford University Press. the efficacy of other drugs by enzyme inhibition. For example, sulphonamides can lead to phenytoin toxicity. Effect of pregnancy and breastfeeding on drug metabolism Drugs can affect the developing fetus by direct action on the fetus causing birth defects, by affecting the placenta and limiting the supply of nutrients and oxygen to the fetus, and by causing premature labour (Table 1.3) (23). Drugs that do not cross the placenta are heparin, insulin, and curare. Fluid retention and decreased protein concentrations tend to increase the volume of distribution, which in turn causes a decrease in the plasma concentration of the drug. In pregnancy, renal blood flow increases and liver metabolic pathways get induced. Anticonvulsants such as phenytoin and carbamazepine undergo increased drug clearance. Plasma levels fall significantly. Lithium and ampicillin are both eliminated by the kidney and their clearance increases by 100% during pregnancy, requiring increased doses. Commonly used drugs, which can be safely administered to a breastfeeding mother, are non-narcotic analgesics, penicillins, cephalosporins, methyl-dopa, beta-blockers, phenytoin, carbamazepine, and sodium valproate. Drugs which should be avoided during breastfeeding include: • laxatives: can cause diarrhoea in neonates • amiodarone: may affect the neonatal thyroid • barbiturates: can cause drowsiness • benzodiazepines can cause drowsiness and failure to thrive • lithium: can cause hypotonia and cyanosis • carbimazole and methimazole: can suppress the neonatal thyroid. Teratogens and organogenesis Drugs that are commonly implicated in fetal malformations include: • cytotoxic anticancer drugs • antiepileptic drugs • some antirheumatic drugs • antibiotics • oral hypoglycaemic agents • some antihypertensives • tranquilizers. Retinoic acids are vitamin A analogues, which are used in the treatment of acne. These drugs can cause major malformations including craniofacial, cardiac, thymic, and central nervous system defects. Cytotoxic anticancer drugs: these inhibit rapid cell growth and are detrimental to fetal growth. Methotrexate and antifolate drugs may cause cleft palate and other abnormalities. Thalidomide should also be avoided in pregnancy. Phenytoin causes a variety of abnormalities including cleft lip/ palate, microcephaly, hypertelorism, and fingernail hyperplasia as well as growth deficiency. Sodium valproate is associated with neural tube defects. Carbamazepine causes similar defects as phenytoin. The incidence of fetal abnormality is around 10% with the anticonvulsants. Aspirin is not the analgesic of choice but may still be used in pregnancy (24, 25). However, doses higher than 500 mg/day are contraindicated after 24 weeks of gestation. Aspirin administration during the last weeks of pregnancy may be associated with postpartum haemorrhage and intracranial bleeding of the newborn. Cyclooxygenase-2 inhibitors should be avoided during pregnancy.
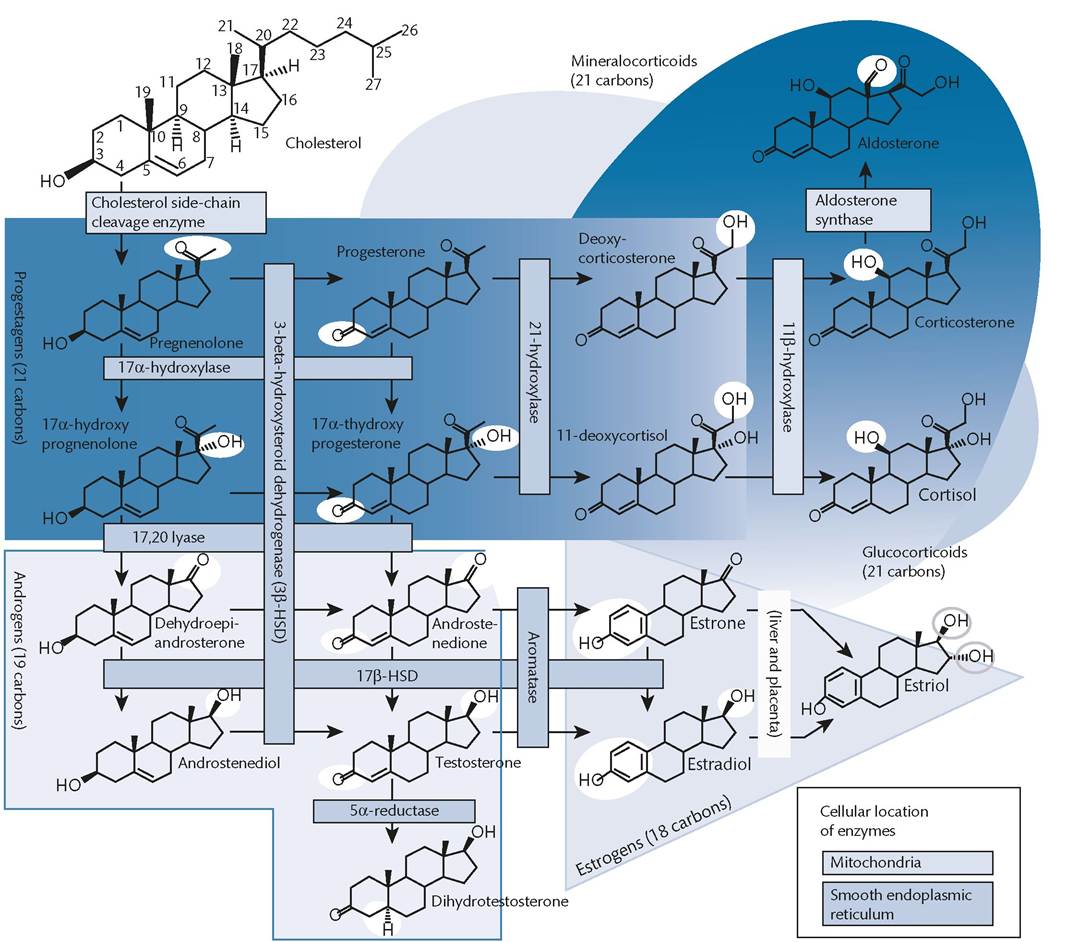
Figure 1.32 Steroidogenesis. Reproduced from Neil Herring and Robert Wilkins, Endocrinology, in: Basic Science for Core Medical Training and the MRCP, Oxford University Press (2015) with permission from Oxford University Press. The use of non-steroidal anti-inflammatory drugs is contraindicated as it may cause closure of the ductus arteriosus in utero, prolonged pregnancy, and postpartum haemorrhage. Lithium can cause cardiac abnormalities when given in the first trimester, such as Ebstein's anomaly. The antiviral agent ribavirin is contraindicated in pregnancy and ciprofloxacin is not recommended. The antibiotics streptomycin, kanamycin, and gentamicin may cause deafness in the fetus. Tetracyclines may damage tooth growth in children under the age of 8. They may also lodge in the bone and should be avoided in pregnancy. Statins are not recommended in pregnancy. Angiotensin-converting enzyme inhibitors can damage the fetal kidney and cause oligohydramnios and neonatal anuria. Warfarin is a coumarin anticoagulant. Fetal warfarin syndrome has been associated with warfarin exposure in pregnancy, with the highest risk between 6 and 12 weeks of gestation. Warfarin is associated with chondrodysplasia punctata, central nervous system defects, intracerebral haemorrhage, intellectual disability, and eye anomalies (optic atrophy). In summary, the following rules should be considered when prescribing in pregnancy or lactation (26, 27): • Prescribe only when absolutely necessary. • Do not prescribe lower or higher doses than necessary. • Avoid medications known to be contraindicated or newly released medications. • Choose drugs that do not cross the placenta.
Figure 1.33 Hormonal changes during the three trimesters of pregnancy. DHEA, dehydroepiandrosterone; hCG, human chorionic gonadotrophin; hPL, human placental lactogen. Reproduced from Austin Ugwumadu, Endocrinology, in: Basic Sciences for Obstetrics and Gynaecology, Oxford University Press (2014) with permission from Oxford University Press.
Source data from Rubin P. Prescribing in pregnancy. In: Warrell DA, Cox TM, Firth JD (eds) Oxford Textbook of Medicine. Oxford: Oxford University Press; 2010. Ultrasound is an ideal means for imaging soft tissues and fluid collections commonly encountered in obstetric and gynaecological clinical practice. The interaction between ultrasound waves and tissues can be described in terms of reflection, scattering, refraction, and attenuation. The last three factors decrease the magnitude of the ultrasound wave. Reflection occurs when a wave front reaches a tissue boundary/ interface with another medium, causing the wave front to return into the medium from which it originated (the transducer). The magnitude of the reflected wave is dependent on the acoustic impedance of the tissue: Acoustic impedance = tissue density ? propagation velocity Tissues with increased density reflect a greater proportion of the ultrasound beam. The magnitude of the reflected beam received by the transducer is also dependent upon the angle between the ultrasound beam and tissue interface. Refraction occurs when a wave front travelling through a medium reaches an interface with another medium of different acoustic impedance and then passes through it (Figure 1.34). Diffraction occurs when a wave encounters an obstacle that has a diameter comparable to its wavelength. There is bending of waves around small obstacles and spreading out of the waves as they pass through small openings (Figure 1.35).
More medical literature on Medic.Studio
More on the topic Endocrinology:
-
Infectious diseases -
Internal diseases -
Obstetrics and Gynaecology -
Pediatrics -
Veterinary medicine -
-
Conflictology -
Ecology -
Economy -
Finance -
History -
Law -
Medicine -
Philosophy -
Religious studies -
|