Physiology
Water and electrolyte balance
The total body water has two main compartments: the extracellular fluid (ECF) and the intracellular fluid, which are separated by the cell membrane (16-18) (Figure 1.25).
The cell membranes are freely permeable to water but not to electrolytes and maintain the different solute composition of the two compartments. Sodium (Na+), chloride (Cl-), potassium (K+), phosphate (HPO42-) calcium (Ca2+), sulphate (SO42-), magnesium (Mg2+), and bicarbonate (HCO3-) ions are the main electrolytes in the human body. Interstitial fluid and blood plasma are similar in electrolyte composition, Na+ and Cl- being the major electrolytes. In the intracellular fluid, K+ and HPO4- are the major electrolytes (Table 1.2) (19).
ECF volume: this constitutes approximately 33-40% of the body water. The ECF volume is regulated by urinary sodium excretion
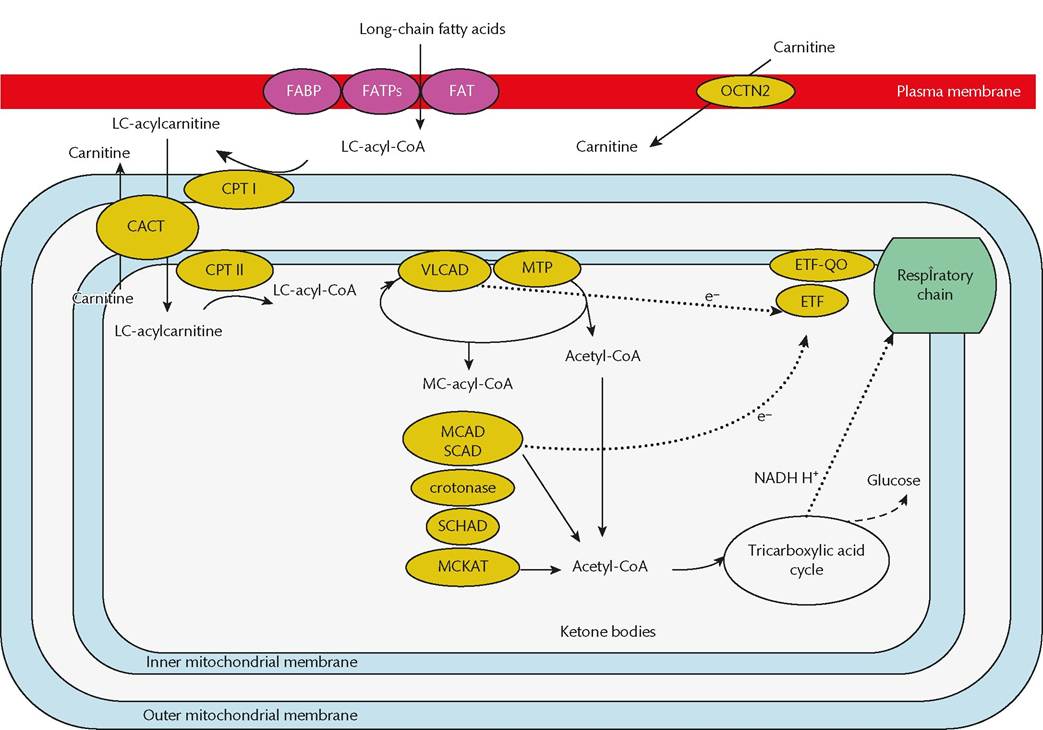
Figure 1.21 Simplified scheme of mitochondrial fatty acid oxidation. Fatty acids enter the mitochondria. Medium- and short-chain fatty acids enter independently of carnitine, but long-chain fatty acids need to be activated to coenzyme A and transferred to carnitine (CPT1) in order to cross the inner mitochondrial membrane (CACT). They are then transferred back to CoA esters in the mitochondrial matrix (CPT2). Beta-oxidation is catalysed by enzymes of different fatty acid chain length specificity (VLCAD, MTP, MCAD, SCAD, crotonase, SCHAD, and MCKAT). Electrons (e-) are passed to the respiratory chain either directly or via transfer proteins (ETF, ETF-QO). Acetyl-CoA can be oxidized in the tricarboxylic acid (Krebs) cycle or, in the liver, used to synthesize ketone bodies.
CACT, carnitine acylcarnitine translocase; CPT1, carnitine palmitoyltransferase 1; CPT2, carnitine palmitoyltransferase 2; ETF, electron transfer flavoprotein; ETF-QO, electron transfer flavoprotein ubiquinone oxidoreductase; FATPs, fatty acid transport proteins; FABP, plasma membrane fatty acid-binding protein; FAT, fatty acid translocase; LC-acyl-CoA, long-chain acyl-CoA; MCAD, medium-chain acyl-CoA dehydrogenase; MC-acyl-CoA, medium-chain acyl-CoA; MKAT, medium-chain acyl-CoA thiolase; MTP, mitochondrial trifunctional protein; OCTN2, high-affinity sodium-dependent carnitine transporter; SCAD, short-chain acyl-CoA dehydrogenase; SCHAD, short-chain 3-hydroxyacyl-CoA dehydrogenase; SC-thiolase, short-chain acyl-CoA thiolase; VLCAD, very-long-chain acyl-CoA dehydrogenase.Reproduced from Elaine Murphy, Yann Nadjar, and Christine Vianey-Saban, Fatty Acid Oxidation, Electron Transfer and Riboflavin Metabolism Defects, in: Inherited Metabolic Disease in Adults: A Clinical Guide (eds. Carla E. M. Hollak and Robin Lachmann) Oxford University Press (2016) with permission from Oxford University Press.
primarily mediated by the renin-angiotensin-aldosterone and sympathetic nervous systems, which promote sodium retention, and the secretion of natriuretic peptides, which promotes sodium excretion.
Intracellular fluid volume: in normal adults, the intracellular fluid volume constitutes approximately 60-67% of the total body water. Potassium salts are the main intracellular solutes. The main regulating factor is the relative osmolarity of the interstitial fluid, which is determined by the balance between water intake and excretion (20).
Acid-base balance
pH is the negative of the base 10 logarithm of the hydrogen ion concentration. A low pH indicates a high hydrogen ion concentration (i.e. an acidic solution). A high pH represents lower hydrogen ion concentrations (i.e. alkaline solutions). The normal pH in human tissues is 7.36-7.44. A pH value of 7.4 represents a hydrogen ion concentration of 0.00004 mmol/L.
The Henderson-Hasselbalch equation describes the relationship of hydrogen ion, bicarbonate, and carbonic acid concentrations. The partial pressure of carbon dioxide (PCO2) is controlled by respiration. Short-term changes of pH may be controlled by changing the depth of respiration. The bicarbonate concentration can be altered by the kidneys.
Buflers: a buffer solution is one to which hydrogen or hydroxyl ions can be added with little change in the pH. A simple buffering system is the equilibrium between carbonic acid and bicarbonate ions in the blood (Figure 1.26). A major buffering system of the blood involves amino acids with different chemical side chains, and which ionize at different pH values (Figure 1.27). Haemoglobin has
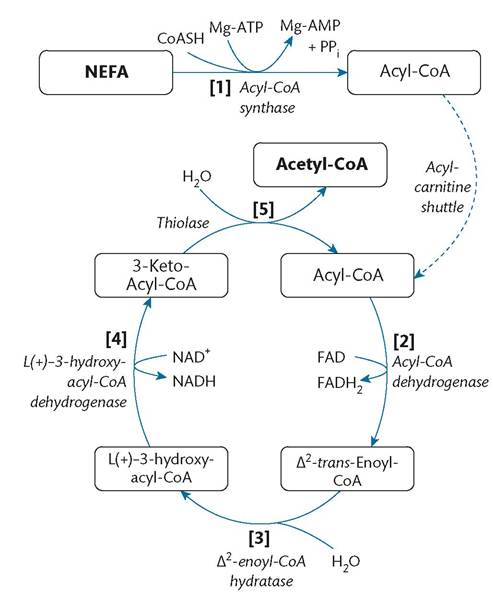
Figure 1.22 The beta -oxidation cycle of fatty acids. In the first instance, a cytosolic non-esterified fatty acid (NEFA), liberated from triglyceride stores by lipolysis, is esterified to coenzyme A (CoASH) to form an acyl-CoA molecule that can be imported into the mitochondrial matrix via the acyl-carnitine shuttle. The initial formation of the acyl-CoA complex requires the hydrolysis of magnesium (Mg)-ATP to Mg-AMP and pyrophosphate (PPi), where the spontaneous decay of the PPi to two inorganic phosphate (Pi) molecules prevents the acyl-CoA synthase reaction from reaching equilibrium.
Reproduced from Austin Ugwumadu, Biochemistry, in: Basic Sciences for Obstetrics and Gynaecology, Oxford University Press (2014) with permission from Oxford University Press.
a high buffering value and is found in higher concentrations than the plasma proteins.
Calcium homeostasis
Calcium is essential for several biological functions in the human body. Calcium is distributed in bones (99%), intracellular fluids (1%), and ECF (0.1%). The overall body Ca2+ balance is maintained through the intestinal absorption, renal reabsorption, and bone metabolism (Figure 1.28).
The ionized calcium concentration of ECF is closely regulated by the parathyroid hormone-vitamin D system acting on the kidneys, intestine, and bone. ECF Ca2+ is required for blood coagulation and maintenance of plasma membranes. It is also an important source of intracellular Ca2+, which is required for several cellular functions. Channels control the transport of Ca2+ in and out of cells. Parathyroid cells respond to alterations in ECF Ca2+ levels with parathyroid hormone secretions having an effect on Ca2+ transport in kidney and bone. Homeostasis is also maintained through the renal production of 1,25-dihydroxy vitamin D, which modulates Ca2+ transport in intestine and bone.
Respiration
Alveolar ventilation is 350 mL/breath and the tidal volume is 500 mL/breath. The difference, 150 mL, is the anatomical dead space (Figure 1.29).
The total lung capacity is approximately 5 L. Of this, 1.5 L, the residual volume, remains at the end of forced expiration. The volume of gas, 3.5 L, inhaled from forced expiration to forced inspiration is the vital capacity. At rest, the pressure between the visceral and parietal pleura is -3 mmHg. During quiet inspiration, the chest expands and the pressure in the intrapleural space decreases to -6 mmHg. Expiration is passive with relaxation of the diaphragm and muscles of the chest wall.
Transportation mechanisms
Transport of substances within cells and across cell membranes is achieved via diffusion, solvent drag, filtration, osmosis, non-ionic diffusion, carrier-mediated transport, and phagocytosis.
Diffusion is a process whereby a gas or substance in solution expands to fill the volume available to it. Gaseous diffusion occurs in the alveoli of the lung and liquid diffusion occurs in the renal tubules.
Solvent drag is the process whereby bulk movement of solvent drags molecules of solute with it.
In filtration, substances are forced through a membrane by hydrostatic pressure. Osmosis is the movement of molecules of a solvent across a semipermeable membrane from a less concentrated solution into a more concentrated one.
Non-ionized diffusion is transport in a non-ionized form. Cell membranes consist of a lipid bilayer with specific transporter proteins embedded in it. Lipid-soluble drugs can cross the lipids of the blood-brain barrier or placenta by this process.
Carrier-mediated transport occurs across a cell membrane using a specific carrier. If the transport is down a concentration gradient, this is known as facilitated transport. If the carrier-mediated transport is up a concentration gradient, this is known as active transport.
Phagocytosis involves the incorporation of solid and liquid substances by the cell wall engulfing them. The cell appears to ‘swallow’ these substances.