Placental site trophoblastic tumour
PSTT is even rarer than choriocarcinoma. PSTT occurs in the reproductive age group and typically presents with non-specific symptoms of abnormal vaginal bleeding or amenorrhoea.
Although tumour load with PSTT is not reflected by hCG, free beta hCG is a reliable marker for PSTT especially in conditions where there is uncertainty about whether the patient has choriocarcinoma (high proportion of hyperglycosylated hCG) or PSTT (high proportion of free beta hCG) (39). Histologically, PSTT is composed predominantly of intermediate trophoblast, and chorionic villi are typically not seen. The monotonous population of implantation site intermediate trophoblast usually has significant cytological atypia and scattered mitotic figures (Figure 66.7). The trophoblastic tumour cells infiltrate the myometrium, and there is prominent lymphatic and vascular invasion. PSTT is less chemosensitive than choriocarcinoma. Hysterectomy is the main mode of treatment in most cases.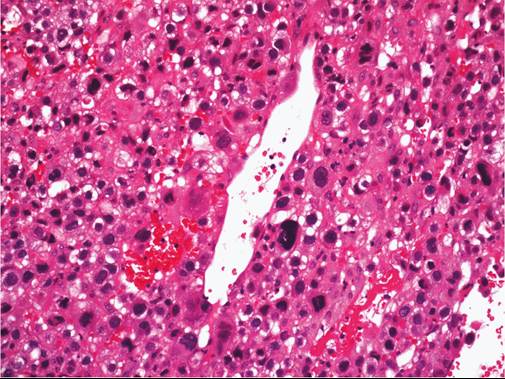
Figure 66.7 Photomicrographs demonstrating placental site trophoblastic tumour where a monotonous population of implantation site intermediate trophoblasts with significant cytological atypia and scattered mitotic figures are found.
Courtesy of Cheung AN, Department of Pathology, The University of Hong Kong.
However, fertility-preserving management such as uterine curettage, hysteroscopic resection, and chemotherapy may be considered in young patients with limited myometrial involvement. Fertility preservation is not appropriate for diffuse lesions. EP-EMA is the most commonly used chemotherapy. An interval from the antecedent pregnancy of more than 48 months seems to be the most significant adverse prognostic factor (40).
More on the topic Placental site trophoblastic tumour:
- Gestational trophoblastic disease
- Introduction
- REFERENCES
- Arulkumaran S., Ledger W., Denny L., Doumouchtsis S. (eds.). Oxford Textbook of Obstetrics and Gynaecology. Oxford University Press,2020. — 928 p., 2020
- Index
- Abbreviations
- Index