Systemic therapy in gynaecological malignancies
Epithelial ovarian cancer
EOC is the most common type of ovarian cancer and comprises five histological subtypes: high- and low-grade serous, mucinous, clear cell, and endometrioid, each with distinct pathological morphology and predicted clinical outcome (Figure 67.1).
Treatment algorithms have clumped all subtypes of ovarian cancer for many years, but were largely driven by the clinical behaviour of the most frequent subtype, high-grade serous. It has been only within the last few years that subtype- specific treatments are being considered. As a consequence, level 1 evidence for rare subtypes remains elusive and recommendations have been based on expert opinion and consensus statements.Following surgery, systemic treatment with a DNA-damaging agent (cisplatin or carboplatin) in combination with a taxane (paclitaxel) for six cycles has remained the mainstay oftreatment for several decades in the first-line setting. The defined number of cycles was established initially, like most other indications for chemotherapy, on the concept of log-cell kill from the Skipper-Schobel-Wilcox and Goldie-Coldman models of cell growth kinetics and validated by lack of improvement in overall survival by increasing the number of cycles. Chemotherapy primarily damages rapidly proliferating cells and thus, is effective only in that proportion of tumour cells within the cell growth cycle. Following first-line therapy, duration of progression-free interval identifies likelihood of successful rechallenge to platinum agents and this has led to a simple and internationally used treatment algorithm. Specifically, disease recurrence less than 3 months from completion of therapy is refractory and highly resistant; recurrence within 6 months is considered resistant; and greater than 6 months as sensitive to rechallenge with platinum agents. For platinum-r esistant disease, subsequent treatment with alternate single-agent chemotherapies is an option, albeit with modest activity, and includes weekly paclitaxel, liposomal doxorubicin, or gemcitabine.
First-line chemotherapy after surgery
The outcome in women who receive chemotherapy after surgery is dependent on the effectiveness of surgery and the presence or absence of residual disease. The most commonly used systemic therapy regimen post surgery has been with a combination of carboplatin and paclitaxel and this has been accepted as the standard of care (5). Carboplatin is administered at a dose based on renal clearance, calculated as the area under the curve (AUC) of six (6), and paclitaxel at a dose of 175mg∕m2 over 3 hours (6). This regimen, derived from well-conducted randomized clinical trials was extensively compared with other variations which assessed alternate platinums, taxanes, and combinations (three or more chemotherapy drugs vs. two), but has emerged as the best tolerated regimen. Ovarian cancer consensus guidelines by the Gynecologic Cancer InterGroup (GCIG) have also validated the use of this regimen as the control arm for future clinical trials. The most common schedule of administration is every 3 weeks, with prior confirmation of haematological and biochemistry parameters, particularly renal function. Recent studies have investigated the potential role of dose-dense chemotherapy using a weekly paclitaxel regimen (7). Given the features of ovarian cancer evolution and peritoneal extension, intraperitoneal chemotherapy has been explored after optimal debulking surgery to potentially increase overall survival and progression-free survival from advanced ovarian cancer (8).
Neoadjuvant chemotherapy
The timing of chemotherapy in relation to surgery has been the subject of intense investigation and debate over the past 20 years. The initial paradigm of surgery followed by chemotherapy was challenged as there were many patients who either were not surgical candidates or had disease that was very extensive and not debulkable. In this setting, chemotherapy was seen to be an effective way of controlling disease given the likelihood of response and allowed a second opportunity for surgery after an ‘interval’.
This alternate sequence of chemotherapy followed by surgery and completion chemotherapy has gained considerable traction and has been shown to be effective in two prospective randomized clinical trials (9, 10) that are landmark studies in defining treatment sequence. However, there remain important questions and challenges mainly based on patient selection, such as the question of best sequence if patients can be debulked at outset that will be addressed in a planned randomized trial being led by the AGO group. It is also intriguing that disease biology and not simply surgical skill may in fact be very important in determining debulkability (11).Maintenance therapy
Given the ‘relapse-response’ pattern with shorter disease-free intervals with each subsequent line of therapy, a maintenance approach with well-tolerated chronic therapy to keep disease under control has been developed. For maintenance therapy to be acceptable, it has to improve outcome for patients, without significantly compromising quality of life. For HGSOC, incorporating complementary mechanisms of action beside standalone chemotherapy such as targeting angiogenesis and deficiencies in the homologous recombination repair pathway have been successful strategies.
Antiangiogenics in ovarian cancer
Tumour-associated angiogenesis and targeting the microenvironment has been an effective strategy. The advent of antiangiogenics heralded an important era in ovarian cancer therapy. Ovarian cancer is very dependent on angiogenesis for growth and has shown important prognostic reliance on microvessel density. Ovarian cancer is a disease which produces excessive amounts of VEGF leading to the hallmarks of disease such as capillary leakiness and ascites. Early studies with bevacizumab, a humanized monoclonal antibody against VEGF, showed single-agent activity and symptoms benefit with control of ascites. Early studies were also challenging due to complications related to bowel perforation and fistulization, related to bowel involvement with disease.
Antiangiogenesis has since been extensively incorporated in therapy in different settings— first line for high-r isk patients and the platinum-s ensitive and platinum-resistance setting in combination with chemotherapy and followed by maintenance therapy (12).In a first-line setting, the Gynecologic Oncology Group (GOG) 218 (13) and ICON7 (14) provided evidence for improvement of disease control and progression-free survival with the addition of bevacizumab to carboplatin and paclitaxel. Both these studies demonstrated that progression-free survival was significantly improved with the addition of bevacizumab concurrently with carboplatin and paclitaxel chemotherapy, followed by maintenance bevacizumab. The doses of bevacizumab used in the two trials were different—7.5 mg/ kg in ICON7 and 15 mg/kg in GOG 218, with some differences in duration of maintenance period. ICON7 further demonstrated that the benefit is greatest in women with high risk of recurrence defined by suboptimally debulked stage III/IV or non-operated patients (15). In this setting, addition of bevacizumab may improve median overall survival by 9.4 months. This has now led to the approval of bevacizumab for treatment of women with advanced ovarian cancer in a first-line setting. In the platinum-s ensitive (OCEANS study) and -resistant recurrence setting (AURELIA), two phase III trials with bevacizumab prescribed until disease progression or intolerance, a significant benefit for maintenance on disease control rate was shown (16, 17). The benefit of adding and/or continuing an antiangiogenic agent has also been validated in other settings such as platinum-sensitive recurrent disease, and platinum-resistant disease with bevacizumab, as well as proof of principle activity with other antiangiogenics such as AMG386, pazopanib, and cediranib (18, 19). Bevacizumab has received regulatory approval for ovarian cancer in a first-line setting, as well recurrent disease and is currently the most widely used antiangiogenic added to chemotherapy around the world.
PARP inhibitors
DNA repair defects consistent with homologous recombination repair dysfunction are referred to as the ‘BRCAness phenotype’. Two randomized phase II trials testing the PARP inhibitor olaparib as maintenance therapy—prescribed as long as patients were benefiting from therapy—have demonstrated a marked improvement in progression- free survival for recurrent platinum-sensitive HGSOC patients, particularly for those patients with BRCA1/2 mutations (20, 21). Based on disease vulnerability, olaparib, a PARP inhibitor treatment has been approved following response to platinum-based chemotherapy in BRCA1∕2-mutated ovarian cancer. Several randomized phase III trials confirmed the benefit of PARP inhibitor in high grade serous ovarian cancer with BRCA1/2 mutations and beyond (ref: PMID:31099893) This existing treatment strategy in ovarian cancer has been largely driven by activity in HGSOC but response to cytotoxic chemotherapy varies according to the histological subtypes (22). Patients with HGSOC and BRCA1∕2 mutation have been described as more sensitive to standard chemotherapy; while chemoresistance has been reported in low-grade serous, mucinous, and clear cell ovarian cancer.
Non-epithelial ovarian cancers
Non-EOCs which include sex cord-stromal and other such as germ cell are categorized as rare and treatment guidelines have been extrapolated from EOC, but are not based on level 1 evidence (23). Given the rarity of this disease type, expert gynaecological pathology review is essential for diagnosis. Consensus guidelines by the GCIG form an excellent repository of information on therapy and management, and should be referred to.
Endometrial cancer
Endometrial cancer is the fifth most common female cancer globally, accounting for 4.8% of all cancers (GLOBOCAN 2012). Contrary to ovarian cancer, the majority of endometrial cancer patients present with operable early- stage disease with 5-year survival of approximately 80%.
Optimizing adjuvant therapy, usually carboplatin and paclitaxel particularly in high- and intermediate- risk patients, is currently an active area of research. Adjuvant radiotherapy is currently the standard of care for the International Federation of Gynecology and Obstetrics (FIGO) stages IB to II with intermediate risk of relapse. Many advocate chemotherapy for those with stage III disease or poor prognostic histology based on GOG 122 (24) and confirmed in other studies (25). The role of chemotherapy in addition to radiotherapy for high-risk, higher stage, and poor prognostic histology is being further investigated in the phase III studies PORTEC3, GOG 249, and GOG 258. For patients inoperable at presentation or diagnosed with metastatic or recurrent disease, treatment options are limited. The most active agents in chemotherapy-naive endometrial cancer patients are platinum, taxanes, and anthracyclines with response rates of 20-30% (26). The first-line regimen is often based on carboplatin and paclitaxel. Prior radiation potentially complicates delivery by compromising penetrance and impacting bone marrow reserve. Triplet regimens have demonstrated a superior response rate at the cost of increasing toxicity(27). Results are expected from GOG 209 shortly, but preliminary data suggest that doublet therapy (carboplatin/paclitaxel) is similar to triplet. Response rates after first-line chemotherapy are disappointing. Various agents have been tested in a number of small phase II trials
(28). The maj ority of monotherapy trials have shown minimal activity with response rates varying from 0% to 12% including; doxorubicin or weekly paclitaxel is usually used in this situation.
Endometrial cancer has been divided into type I (endometrioid) and II (serous, clear cell, and carcinosarcoma) subtypes reflecting their grade and aggressiveness. Type I tumours expressing oestrogen (ER) or progesterone (PR) receptors may be indicative of slow growth and favourable survival (29). A significant proportion of endometrial cancers, particularly the type I subtype, express ER or PR and thus make hormonal therapies an attractive therapeutic option. Progestins remain the main hormone treatment available; however, other agents include tamoxifen (a selective oestrogen receptor modulator), gonadotropin-releasing hormone agonists, and aromatase inhibitors (29) are commonly used sequentially. Recent data showed potential benefit of immune therapy in the subgroup of patients diagnosed with recurrent Microsatellite Instability-High (MSI) endometrial cancer (ref: PMID: 30787022).
Cervical cancer
The fourth most common female cancer worldwide, cervical cancer has the fourth highest mortality rate among cancers in women (GLOBOCAN 2012). The leading risk factor for disease is human papillomavirus (HPV) infection (30-33); specifically, subtypes 16 and 18, which have been associated with high-grade dysplasia and cancer, and confer an 11-16.9 times increased risk of development of high-grade cervical intraepithelial neoplasia (CIN) (34- 36). Routine screening for cytological dysplasia includes the Papanicolou (Pap) test with a growing body of evidence to show the incorporation of HPV DNA testing for higher likelihood of detecting early disease (37). Two histological subgroups have been described, the
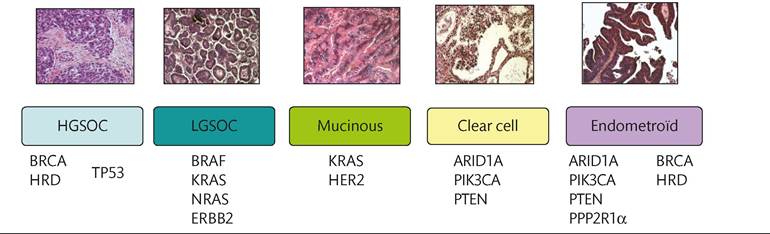
Figure 67.2 Epithelial ovarian cancer histological subtypes.
most common being squamous cell carcinoma and cervical adenocarcinoma (Figure 67.2).
Early-stage cervical cancer is managed either by surgery (for those diagnosed with FIGO stage IA/B1 disease) or by a combination of low-dose platinum chemotherapy administered concurrently with radiotherapy followed by intracavitary brachytherapy. 'The evidence for this came from several randomized clinical trials of radiation therapy versus chemotherapy/radiation, led by the National Cancer Institute (United States), cooperative groups such as the GOG, and the Southwest Oncology Group (38). The National Cancer Institute released a clinical alert in the late 1990s, which set the new standard as chemotherapy in combination with radiation therapy (39, 40). Patients diagnosed with metastatic disease or recurrence after initial treatment have poor outcomes with 5-year survival rates between 5% and 15%. In this setting any treatment is palliative and first-line systemic therapy is based on cisplatin doublet combination.
In the GOG 204 trial, the four-arm study compared cisplatin in combination with paclitaxel, vinorelbine, gemcitabine, or topotecan (41). Outcomes were similar in all arms with a non-significant trend in favour of cisplatin/paclitaxel (overall survival at 12.9 months compared to the other three arms 10-10.3 months) and similar overall response rates. In a further randomized phase III clinical trial conducted by the Japanese GOG (JGOG) carboplatin in combination with paclitaxel was found to be non-inferior to cisplatin/ paclitaxel (42). Besides standard chemotherapy, bevacizumab was assessed in combination in a large randomized phase III trial (GOG 240). The addition of bevacizumab to chemotherapy increased the objective response rate from 36% to 48% (P = 0.008) and the overall survival benefit compared to a standard regimen (overall survival increased from 13.3 to 17 months) (43). A significant improvement in progression-free survival was also seen (8.2 vs 5.9 months; hazard ratio for disease progression 0.67; 95% confidence interval 0.54-0.82). Bevacizumab was associated with a reasonable toxicity profile. The side effects were consistent with those previously known to be associated with bevacizumab, and included hypertension, febrile neutropenia, and thromboembolism, or formation of blood clots. Specifically, treatment with bevacizumab was associated with more grade 3-4 bleeding, thrombosis/embolism, and gastrointestinal fistula (8.6%). This overall survival improvement has led to the United States Food and Drug Administration-approved anti- VEGF agent, bevacizumab, for the treatment of advanced stage, persistent, or recurrent cervical cancer in combination with chemotherapy. No biomarkers of response were identified. At the time of relapse, there is no standard of care second-line options. In June 2018, Pembrolizumab, a programmed death-1 (PD-1) inhibitor has been granted approval by the FDA for the treatment of patients with advanced, PD-L1+ cervical cancer progressing after chemotherapy (ref: PMID:30943124)
Rare malignancies-vagina and vulval
The incidence of vaginal and vulval cancers is low rendering these particularly rare diseases. Published NCCN guidelines for vulval cancer suggest chemotherapy for advanced, recurrent/metastatic disease with cisplatin, or cisplatin in combination with vinorelbine or paclitaxel (44). There is no standard chemotherapy for vulval cancer, and reports describing the use of this modality in the setting of metastatic or recurrent disease are anecdotal. Working from regimens used for anal or cervical squamous cell cancers, chemotherapy has been studied in combination with radiation in the neoadjuvant setting or as primary therapy in advanced disease. Chemotherapy regimens have included various combinations of 5-fluorouracil (5- FU), cisplatin, mitomycin-C, or bleomycin.
Taken together, response rates remain low in the majority of gynaecological cancers and as such, an increasing trend in histological subtype specific and molecular basis of clinical trials is in motion.