Introduction
Current treatment paradigms are based on understanding cancer biology and its influence on the aetiology, development, and growth of cancer. This has also shaped therapeutic strategy with evidencebased integration of surgery, radiation, and systemic therapies in solid tumour and haematological malignancies (1).
There is a complex interplay between genomic, immune, and proteomic disturbances in the development and behaviour of cancer (1). Cancer is the culmination of a variety of insults to the genome—some heritable in nature and therefore transmittable between generations; while others are non-heritable or somatic, and as such are found only in tumour tissue. The coordinated evasion of highly sensitive immune surveillance, and the reprogramming of cellular signalling, protein expression/production, and resetting of the local tumour microenvironment have all been shown to contribute to the development and evolution of disease. Understanding these elementary biological processes—and vulnerabilities when these go awry—can be exploited to improve precision with systemic therapies and are the identified hallmarks or roadmap for contemporary anticancer drug development (2, 3). Improved understanding of these biological hallmarks of cancer have heralded the era of precision or targeted therapy in oncology. In gynaecological malignancies, the advances and clinical adoption of targeted therapies now mean that precision medicine is achievable as an appropriate standard in diseases such as high-grade serous epithelial ovarian cancer (EOC) (Figure 67.1). New standards of care are beginning to be established, with targeted agents complementing chemotherapy. Improvement in outcome has to be meaningful, with validated outcomes which include overall survival and progression-free survival in randomized trials for the majority of new agents, but also can include meaningful improvement in response in others (4). In addition, for non-curative therapy, there is increased awareness and appropriate assessment of quality of life and symptoms with development of tools to track patient- reported outcomes (4).Gynaecological cancers affect any organs of the reproductive tract and may arise in the peritoneum, ovaries, fallopian tubes, uterus, cervix, vagina, and vulva. Cancers of the cervix, endometrium, and ovary have a major global impact in terms of incidence and mortality (GLOBOCAN 2012 data (available at http://gco.iarc.fr/)). There is a very large spectrum of gynaecological malignancies, including epithelial as well as non-epithelial tumours, which range in incidence from common to extremely rare. Understanding risk, development, and disease biology will allow for the development of treatment strategies to prevent, detect early, and treat cancers more effectively.
Systemic therapy
The goals of systemic therapy are context dependent and can be broadly categorized into improving likelihood of cure, controlling disease, and palliation of active disease. Systemic therapy to improve cure is generally through treatment administered before or after locoregional therapy (surgery or radiation) and is termed neoadjuvant or adjuvant. The choice of systemic therapy, schedule, frequency, sequence, and combinations has and continues to be refined with prospective clinical trials with, in general, gradual improvements in cancer control. Implementation and changes in standard of care therapy requires rigor in assessment and validation of impact. Standard of care chemotherapy guidelines for neoadjuvant, adjuvant, and palliative treatment are currently used across the world and refined through meta-analyses, consensus conferences, and evidence-based reviews such as those by the Cochrane collaboration, the National Institute for Health and Care Excellence (NICE) in the United Kingdom (https://www.nice.org.uk/), Cancer Care Ontario (https://www.cancercare.on.ca/), British Columbia Cancer Agency (http://www.bccancer.bc.ca/), and the National Comprehensive Cancer Network (NCCN) (https://www.nccn.org/). These provide a rich repository of validated and updated information, including the evidentiary analyses for recommendations, and should be foundations of treatment decisions.
This chapter will focus on current approaches to precision medicine in gynaecological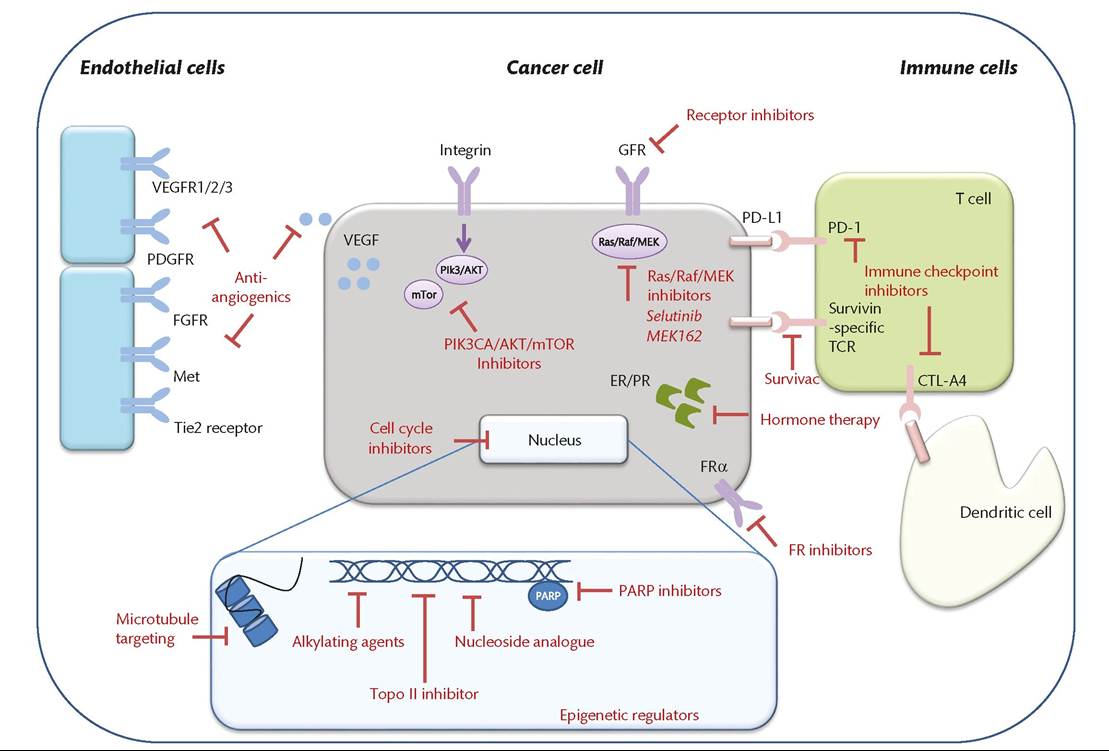
Figure 67.1 Molecular targets of therapeutics in gynaecological cancer.
cancers, with an overview of recent trials which have led to approvals for targeted agents, as well as ones presently underway. It will also include a matrix approach integrating tumour biology, targets, and target-specific therapy.
Improvements in the understanding of cancer biology have facilitated the advent of target- directed precision therapies that are driven by tumour origin, biological subtype, and molecular characterization. The earliest target-directed therapy in gynaecological cancers was hormonal therapy. The backbone of systemic chemotherapy for the past four decades has been with platinum compounds. More recently, identification of tumour vulnerabilities has been exploited to direct therapy. Contemporary examples of tumour vulnerabilities includes an increasingly deeper understanding of cell cycle properties and the DNA repair pathway, and these constitute specific targets for the development of novel therapies. Poly(ADP ribose) polymerase (PARP) inhibitor treatment, has been approved in women with platinum sensitive high-grade serous ovarian cancer (HGSOC) with confirmed BRCA1/2 mutations. Targeting the microenvironment is a rapidly developing area of research, based on tumour-specific neoangiogenesis capacity and more recently, the role of immune cells and complex cellular interactions that have been effectively leveraged for anticancer-directed treatment. Bevacizumab, a recombinant humanized monoclonal antibody directed against the vascular endothelial growth factor (VEGF), a proangiogenic cytokine, has also been approved in ovarian and cervical cancers.
The deregulation of different pathways, such as PI3K, HER, or MAPK, needs further investigation to define the clinical impact and the specific subgroup of patients who may have benefit from these therapies.
For example, targeting PI3K/AKT/mTOR and the angiogenic pathways in endometrial cancer have been associated with intriguing clinical activity, but balancing this with toxicity has challenged clinical development. Presently, hormonal therapy remains the only approved ‘targeted’ therapy in endometrial cancer. Overcoming hormone resistance is an active area of investigation. Vulval and vaginal cancers are rare entities and the level of evidence for treatment modalities remains poor and tends to be adapted from cervical cancer. As such, clinical trials are needed in these cancers, as well as rare tumours, to truly define future therapy. Given the heterogeneity of the gynaecological disease, novel hypotheses are under investigation and include stem cell-like population, the role of tumour metabolism, and epigenetic modulation.Gynaecological malignancies can be subdivided into multiple subtypes of cancer, which individually have distinct behaviour and response patterns to standard and targeted therapy. Well-designed translational clinical trials that analyse response, define the appropriate treatment schedule or combination, explore, and eventually validate potential predictive biomarkers help stratify gynaecological cancers based on behaviour and response to therapy. This necessitates defining biomarkers that are integral, integrated, or exploratory, alongside rigor in trial conduct. Importantly, this also requires collaboration and long-term follow-up for efficacy as well as safety data to achieve meaningful improvement in the prognosis of women with gynaecological cancers.
More on the topic Introduction:
- Introduction
- INTRODUCTION TO REASONING IN THE SNAP EXAM
- Introduction
- INTRODUCTION TO REASONING IN THE XAT
- INTRODUCTION
- Introduction
- Introduction
- Introduction
- Introduction
- Introduction