CHILDHOOD TUBERCULOSIS
Tuberculosis (TB) continues to be major public health problem in India and recent years have witnessed resurgence of disease due to spread of HIV infection and emergence of multi-drug resistance.
However, India is committed to eliminate tuberculosis by the year 2025, ahead of WHO-target for global TB elimination by 2030. Magnitude of problem: Natural course of tuberculosis may be divided into two stages:a. Primary infection that may or may not progress to disease state and
b. Active disease, due to spread of primary infection, re-activation of latent primary infection or re-infection in later life.
Accordingly, the magnitude of problem is ascertained by the frequency of either infection or disease. Recent TB report 2023 suggests estimated prevalence of disease in India as 312 per lakh population, including 5.6% children below 14 years of age. However, ~30-40% children by this age are Tuberculin-positive, suggesting a large pool of latent infections. Year 2022 has reported ~13% rise in newly detected cases vs previous year, perhaps due to delayed medical attention in COVID years and increase in the case detection/notification under National Tuberculosis Elimination Programme (NTEP).
Epidemiology: Mycobacterium tuberculosis—an obligate aerobe, is characterized by hallmark acid-fastness, i.e. capability to resist decolorization by acid or alcohol on staining. Presence of a lipid-rich cell wall resists intracellular killing and hence, the organism may survive for many years intracellularly within phagocytes and macrophages, even after extracellular destruction.
Genus Mycobacterium includes two broad groups— (a) Typical mycobacteria, e.g. M. tuberculosis, M. bovis, etc. and (b) Atypical mycobacteria. While atypical mycobacteria can also produce similar disease specially in immunocompromised hosts, the term tuberculosis is reserved for disease caused by typical mycobacteria, of which M.
bovis is rare in India.Atypical mycobacteria are classified as: (i) photochromogens, e.g. M. kansasii, (ii) scotochromogens, e.g. M. scrofulaceum, (iii) nonphotochromogens, e.g. M. intracellulare, and (iv) rapid growers, e.g. M. fortuitum.
Primary infection is most common in early childhood with important risk factors being malnutrition, low socioeconomic status and absence of BCG vaccination.
Overcrowding and history of contact in the household are two most important environmental factors for natural infection.
Source of infection is usually an adult sputum-positive household contact. While effective therapy reduces the infectivity of index case by 90% within 48 hours, intermittent discharge of organisms in sputum may continue for 3 months (or longer in drug-resistant cases). Pediatric cases are seldom infective, unless having endobronchial or cavitatory lesions.
Mode of transmission is usually a direct person-to person droplet infection, or rarely via indirect contact with contaminated fomites. Newborns of infected mother may be infected via transplacental infection or after aspiration of infected amniotic fluid at birth.
Portal of entry: Lung is the commonest portal of entry in acquired infections, including in newborns due to aspiration of amniotic fluid at birth. However, congenital transplacental infection may be first lodged in liver.
Pathogenesis (Natural history) of infection depends on previous exposure and presence of cell-mediated immunity (CMI). In most cases of childhood infections, when infection is often primary and CMI is absent, infection progresses in following manner:
• Formation of primary complex: After airborne entry, bacilli are primarily lodged in peripheral subpleural alveoli around the right interlobar fissure (due to sluggish air current in this region) and multiply in alveolar spaces and ducts. About 20% cases have more than one primary lesion. In transplacentally infected infants, primary lesion forms in liver with similar course.
First protective response to infection is nonspecific local inflammatory reaction to attract macrophages, which attempt to ingest and destroy invading pathogens. However, presence of unique sulfatides molecules in mycobacterial cell wall inhibits phagocytic activity and many organisms escape intracellular destruction and in fact, multiply intracellularly.
During this period of uninhibited growth, bacilli either remain concentrated in parenchymal lesion (Ghon lesion-a pulmonary granuloma of ~1 cm size with central necrosis and surrounding mononuclear infiltration, epitheloid cells and giant cell formation) or carried to regional lymph nodes via local lymphatics. The term primary complex includes: (i) parenchymal (Ghon) lesion, (ii) draining lymphatics, and (iii) regional lymph node infection.
Till adequate and specific immune response develops in next 8-12 weeks (as discussed below), local lesion progresses relentlessly with intense tissue reaction. During this period, intermittent bacteremia is common with hematogenous seedling of distant organs (extrapulmonary tuberculosis).
• Immunological response: Four different types of specific immunological responses develop in next 8-12 weeks, which determine the further course of disease:
- Specific macrophage-mediated response: After initial non-specific macrophage response, small population of lymphocytes with capability to recognize specific mycobacterial antigens proliferate and secrete lymphokines and other inflammatory mediators, to enhance the bactericidal activity of activated macrophages and trigger humoral/cellular response.
- Humoral response: Although tubercular infection provokes a robust antibody response, humoral immunity plays negligible role to protect from progression of disease.
- Cell-mediated immunity (CMI), i.e. T-cell mediated immune response is the most important protective response to arrest primary lesion. Development of adequate CMI leads to healing of primary complex, while inadequate CMI permits unhindered progression.
Persistence of adequate CMI is essential to keep healed lesions in check, as intracellular pathogen often survive in these lesions and maybe reactivated during immunocompromised states, e.g. malnutrition, diseases, e.g. measles, whooping cough, HIV, etc. and steroid or cytotoxic therapy.
- Delayed tuberculin hypersensitivity (DTH) is a potentially harmful response that arrests the mycobacterial growth but provokes intense tissue reaction and destruction due to release of bacterial breakdown products and inflammatory mediators like TNF-, hydrolytic or proteolytic enzymes, oxidation intermediates, etc. DTH is also responsible for tuberculin positivity and other hypersensitivity manifestations (Table 10.16).
• Fate of primary complex after initial 6-10 weeks (Table 10.17), depends on the balance between protective CMI and destructive DTH in the host:
- In gt;90% cases, development of adequately CMI heals primary lesion with calcification.
- In cases with inadequate CMI, (e.g. in malnutrition), healing is incomplete with progression of disease (see below, spread of primary lesion). Even in partially healed lesions, viable organisms may persist for many years.
- In cases with excess DTH (with/without adequate CMI), local reaction is so intense as to cause excessive tissue destruction and cavity formation. Uncommon in primary infection, it is the major pathological mechanism of adult or reactivation TB.
- Spread of primary lesion: In children with poor CMI and/or high DTH, primary lesion may
TABLE 10.16: Hypersensitivity manifestations in TB
• Tuberculin positivity
• Phylectenular conjunctivitis
• Erythema nodosum
• Aseptic (Lincoln's) meningitis
• Pleural effusion
TABLE 10.17: Possible fates of primary infection
• Complete healing with/without calcification
• Local progression
- Progressive primary complex
- Segmental/lobar pneumonia
- Pleural effusion
• Endobronchial spread
- Consolidation
- Collapse
- Emphysema or pneumothorax
• Hematogenous spread
- Acute miliary TB
- Protracted disseminated TB
- Localized extra-pulmonary TB
• Lymphatic spread
- Cervical lymphadenopathy
- Abdominal lymphadenopathy
• Reactivation in later life
- Fibrocaseous tuberculosis (adult type) progress locally (progressive primary complex), invade neighbouring bronchi (endobronchial disease) or vessels (miliary disease) (Fig.
10.2). Regional mediastinal/hilar nodes may also enlarge to compress the bronchi or rupture into them.#9632; Progressive primary complex is the least severe form of disease, characterized by slowly progressive concentric lesion (coin lesion) or segmental bronchopneumonia.
#9632; Endobronchial rupture of parenchymal or nodal lesion leads to the discharge of infective material into bronchial lumen, with following consequences: (a) diffuse spread to lung, i.e. bronchopneumonia, or (b) complete block of bronchus, i.e. collapse of distal lung, or (c) partial block of bronchus to act as a ball-valve mechanism, i.e. emphysema in distal lung.
#9632; Hematogenous spread may occur during early bacteremia at the time of primary infection or late bacteremia, due to invasion of vessels traversing infected lung tissue. Further course depend on the number of organisms leaked into blood stream. Sudden and heavy bacteremia may produce more serious miliary tuberculosis, while intermittent mild bacteremia may be silent or present later with disseminated or extrapulmonary tuberculosis.
Invasion of extrapulmonary organs leads to formation of satellite tubercular lesions (granulomas) in different tissues, sometimes termed as Rich's focus in brain, Simond's focus in spleen and liver, Sheehan's focus in adrenals, etc. Most of these lesions remain silent for long time or progress slowly over 3-5 years to manifest as extrapulmonary TB.
#9632; Lymphatic spread via continuous channels from mediastinal nodes to cervical or abdominal nodes as well as direct spread of pulmonary/pleural lesion to ribs or spine, are other important modes of spread for tubercular disease.
• Re-activation/Re-infection tuberculosis is primarily seen in adolescents/adults and follows a different course than primary infection (Table 10.18). Local response in these cases is modified by presence of prior DTH, leading to intense tissue reaction with cavitation. Reactivation/reinfection pulmonary lesions often develop in apical (Ruhl's lesion) or infraclavicular region (Assman's focus).
Clinical spectrum of tuberculosis is extremely wide, depending on the type and extent of lesion and includes: Primary complex is basically a radiological diagnosis and most cases are asymptomatic except mild constitutional symptoms, e.g. low-grade fever and anorexia. Mild dry
TABLE 10.18: Primary vs Reactivation TB
| Differences | Primary | Reactivation* |
| Common age | lt;5 years | gt;7-8 years |
| Source of infection | Exogenous | Endogenous |
| CMI | Absent | Usually low |
| DHT | Absent | Present |
| Lung focus | Sub-pleural | Apical |
| Mode of healing | Calcification | Fibrosis |
| Mediastinal nodes | Enlarged | Minimal |
| Bacillary load | Low | High |
| Infectivity | Rare | Common |
| Hematogenic spread | Common | Rare |
*or re-infection
Fig. 10.2: Various types of pulmonary tubercular lesions in children.
cough may be present due to compression of airways by enlarged mediastinal nodes.
Pulmonary tuberculosis, other than primary complex, presents with:
• Constitutional symptoms, e.g. mild evening-rise fever, anorexia, weight loss, night sweats, etc.
• Respiratory symptoms, e.g. dry/wet cough, respiratory distress, wheezing or stridor. Chest pain indicates pleural involvement.
• Signs of local disease, depending on the type of lesion.
In NTEP, pulmonary tuberculosis (PTB) refers to:
• Any confirmed or clinically diagnosed case of TB involving lung parenchyma or tracheobronchial tree, including intrathoracic lymphadenopathy (mediastinal or hilar), without radiological abnormalities in the lung.
• Miliary TB (discussed later) is classified as PTB due to lesions in the lungs.
• PTB with extrapulmonary disease (discussed later) is also classified as PTB.
• Extensive pulmonary tuberculosis refers to severe pulmonary bilateral cavitatory disease or extensive parenchymal damage on chest X-ray.
Miliary tuberculosis is the most serious manifestation (mortality gt;50%), usually presenting within first year of primary infection with acute onset of:
• High fever with severe toxemia
• Moderate/severe dyspnea, disproportionately more than lung signs, e.g. crepts/ronchi
• Signs of distant lesions, e.g. hepatosplenomegaly, meningitis (30%), etc.
Diagnosis of miliary tuberculosis rests on characteristic X-ray, i.e. diffuse fine (lt;2-3 mm) miliary mottling (snowstorm appearance) and/or extrapulmonary disease. D/D of similar X-ray findings includes Pneumocystis carinii pneumonia, tropical eosinophilia, Loeffler syndrome, pulmonary hemosiderosis and fungal infections of lung.
Disseminated tuberculosis refers to relatively more insidious form of hematogenous or lymphatic spread of infection, characterized by symptomatic or asymptomatic involvement of at least two non-contiguous sites, i.e. either pulmonary and one extrapulmonary or two extrapulmonary

Fig. 10.3: Diagnostic algorithm for pulmonary tuberculosis in children.
1despite adequate nutrition or failure of nutritional rehabilitation in SAM children
2miliary, cavitatory or hilar/paratracheal lymphadenopathy
3for seven days (Amox/Co-amox), skip this step if already received
NAAT: Nucleic acid amplification test
sites. Most cases manifest after 3-5 years of primary infection due to slow evolution of extrapulmonary lesions.
Extrapulmonary tuberculosis (EPT) may be due to: (i) hematogenous spread during bacteremia, (ii) lymphatic spread via connecting channels, e.g. cervical/abdominal lymphadenopathy, or (iii) direct spread to adjacent tissues, e.g. rib or spine. While EPT may involve any organ, important lesions include: (a) early EPT with CNS or GIT disease, and (b) late EPT after 4-5 years with osteoarticular, genitourinary or skin disease. Common forms of EPT in children, e.g. lymphadenitis, meningitis, osteoarticular or abdominal disease have been discussed in respective chapters.
In NTEP, EPTB refers to:
• Any bacteriologically confirmed or clinically diagnosed case of TB involving organs other than the lungs, including pleura, peripheral lymph nodes, abdomen, genitourinary tract, skin, joints and meninges.
• Severe EPTB refers to neurotuberculosis in all age groups and other forms of EPT in children lt;15 years (except peripheral or mediastinal lymphadenopathy without signs of compression).
Diagnosis: Detection of M. tuberculosis on direct smear or culture from infected body fluids/tissues, e.g. sputum, CSF, etc. is the gold standard for diagnosis, though yield is
| TABLE 10.19: Diagnostic tools in tuberculosis | |
| Supportive | Confirmatory |
| • TT/IGRA • Radiodiagnosis X-rays USG, CT/MRI • Biochemistry Exudative body fluids ADA/TSA levels • Histopathology Aspiration cytology Tissue biopsy | • Bacterial diagnosis Direct smear (Ziehl-Neelsen stain) Solid culture: LJ Media Liquid culture: BACTEC, MGIT • Molecular diagnosis CB-NAAT (x-pert Mb) Line probe assay (LPA) |
TT: Tuberculin test, IGRA: Interferon Gamma Adenosine deaminase (ADA) and tuberculostearic acid (TSA)
poor in children due to difficulties in specimen collection and paucibacillary nature of disease.
NTEP 2022 has proposed a diagnostic algorithm for diagnosis of PTB in children (Fig. 10.3) as well as for some other types of EPTB. Diagnosis in microbiologically negative cases must be made cautiously, supported by clinical or epidemiological indicators as well as indirect investigations (Table 10.19).
• Clinical suspicion is the key for early diagnosis of TB, based on: (a) history of contact with sputum-positive case, (b) absence of BCG vaccination, (c) presence of malnutrition, (d) poor socioeconomic status with overcrowding, and (e) suggestive clinical picture.
TABLE 10.20: Common radiological features in TB
Mediastinal lymph nodes with ill-defined lung shadow
• Primary complex
• Progressive P. complex (large lung shadow)
Localized homogenous opacities
• Consolidation (large segmental, trachea central)
• Collapse (trachea gt; same side)
• Cavity (round/coin lesion, air/fluid level +)
• P. effusion (trachea gt; opp. side, obliterated CP angle)
Non-homogenous opacities
• Bronchopneumonia (large, irregularly distributed)
• Miliary (tiny, bilateral, uniformly distributed)
• Bronchiectasis (segmental honey-Coomb lesion)
Hyperleucent lesions
• Pneumothorax (trachea gt; opposite side, no BVM)
• Emphysema (trachea normal, BVM +)
BVM: Bronchovesicular markings
According to NTEP 2022 guidelines, Children with presence of any one of the following three clinical indicators are considered as Presumptive Pediatric Tuberculosis, with/without history of contact in preceding 2 years:
- Persistent fever for gt; 2 weeks without a known
cause
- Persistent cough for gt; 2 weeks, and/or
- Weight loss of gt;5% or no weight gain for gt;3 months, despite adequate nutrition and no apparent cause.
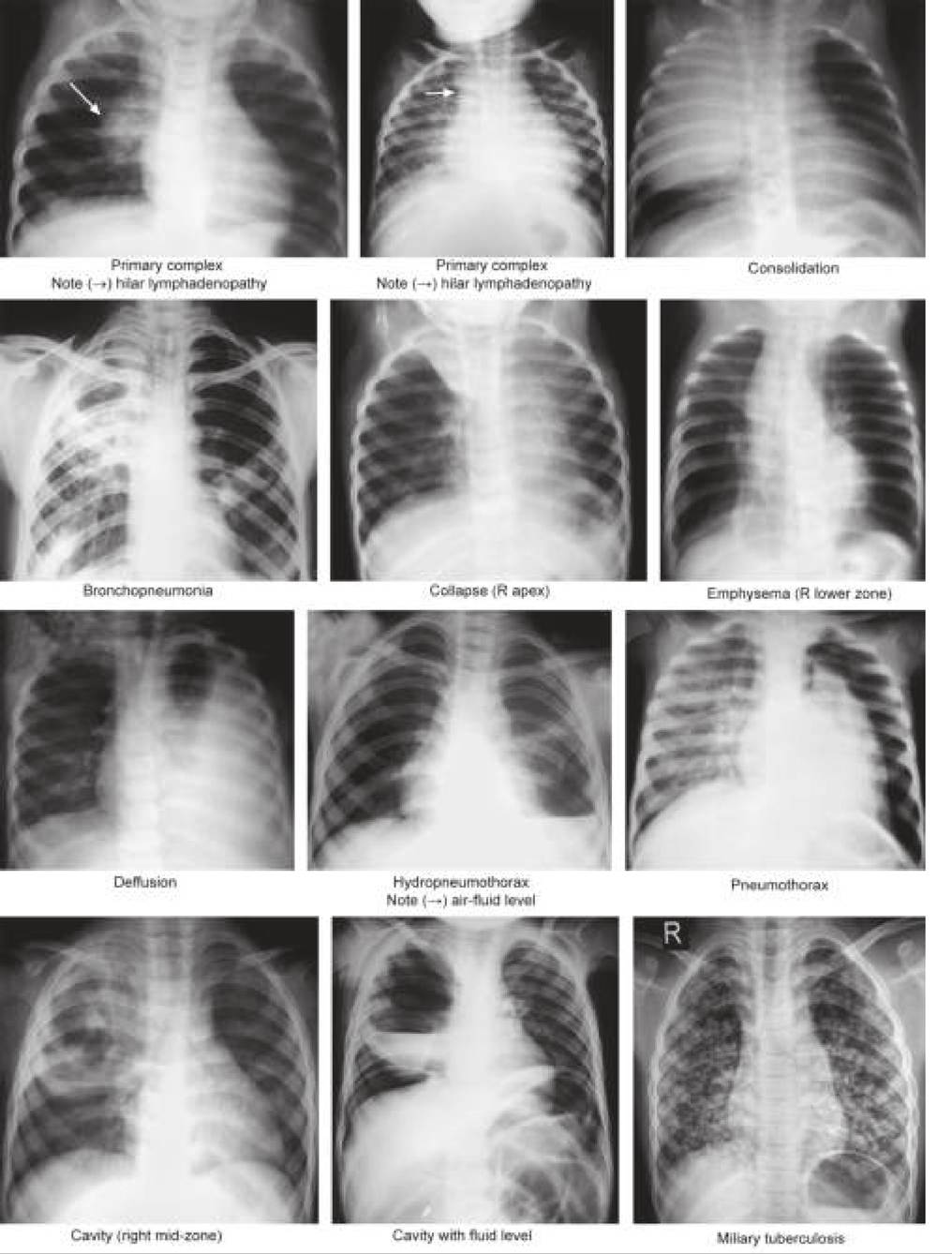
• Radiological diagnosis: Chest X-ray is the base-line investigation in children with presumptive PTB, (Table 10.20) interpreted as follows:
- Chest X-rays highly suggestive of the PTB include those with: (a) miliary pattern, (b) hilar or paratracheal lymphadenopathy with/without parenchymal involvement, and/or (c) fibrocavitary lesions (Fig. 10.4). All presumptive cases with these radiological patterns are considered as probable cases and should be subjected to bacteriological confirmation. Even if microbiologically negative, these children may be treated as clinically-diagnosed tuberculosis, after exclusion of alternative causes. Specificity of diagnosis increases with positive TST or history of contact in preceding two years.
- Chest X-rays with other lesions, e.g. consolidation, non-homogenous shadows or bronchopneumonia, etc. are considered as non-specific (Fig. 10.4). They must receive a 7-days course of antibiotics before repeat skiagram. Cases without improvement on repeat X-ray should be tested bacteriologically and if negative, need further evaluation to exclude other causes.
- Normal chest X-ray practically rules out the pulmonary disease and child must be assessed for EPT or alternate causes or referred to higher center for further assessment.
Other imaging investigations, e.g. USG, CT/ MRI and bone scans are useful to delineate the extent of pulmonary or extrapulmonary disease.
• Bacteriological diagnosis is the gold standard for diagnosis with choice of specimen depending on the site of tubercular lesion. As sputum collection is difficult in young children: (a) early morning gastric aspirate after overnight fasting, (b) induced sputum after 3% saline nebulization and chest percussion, or
(c) bronchoalveolar lavage is advised. Bacteriological diagnosis depends on:
- Direct smear exam for AFB in sputum or other body fluids by conventional Ziehl-Neelsen staining (Table 10.21) or more sensitive fluorescent fluorochrome staining may also be used for rough quantitative assessment of bacillary load (1+, 2+, 3+). Smears are frequently false negative in children due to paucibacillary disease, specially if bacillary load is lt;10,000 bacilli/ml. Yield may be enhanced by centrifugation of specimen. Presence of AFB on smear is highly suggestive but cannot differentiate M. tuberculosis from other acid-fast organisms.
- Bacteriological cultures are more sensitive with detection threshold of ~10 bacilli/ ml. Cultures also allow species-identification and drug sensitivity testing (DST).
#9632; Conventional cultures using solid Lowenstein- Jensen media take longer time, i.e. about 3-6 weeks for isolation of organisms and another 2-4 weeks for DST and hence, have been gradually replaced by.
#9632; Rapid liquid-culture methods, e.g. automated radiometric culture assay (BACTEC) or mycobacterial growth indicator tube (MGIT) systems, which allow isolation of organisms in 1-3 weeks and DST in further 3-5 days.
#9632; Mycobacterial growth indicator tubes (MGIT) is a rapid culture technique in which culture tubes have oxygen-sensitive fluorescent compound at the bottom. Initially, large amount of dissolved oxygen in media quenches emissions from the compound. Later, actively respiring mycobacteria consume the oxygen and allow the fluorescence to be detected by automated instruments.
• Molecular diagnosis is as reliable as bacteriological diagnosis, involving detection of mycobacterial DNA using cartridge-based nucleic acid amplification tests (CBNAAT) or Line probe assays (LPA).
- Cartridge-based nucleic acid amplification test or CBNAAT (Xpert-RIF or Truenat) is the first test of choice for confirmation of diagnosis under NTEP guidelines due to rapid results (1-3 days) and ability to detect very low bacterial load, with sensitivity and specificity of gt;95% in smear-positive and 40-70% in smear-negative cases.
However, CBNAAT cannot differentiate living from dead organisms in treated cases and contamination of samples by blood or pus may lead
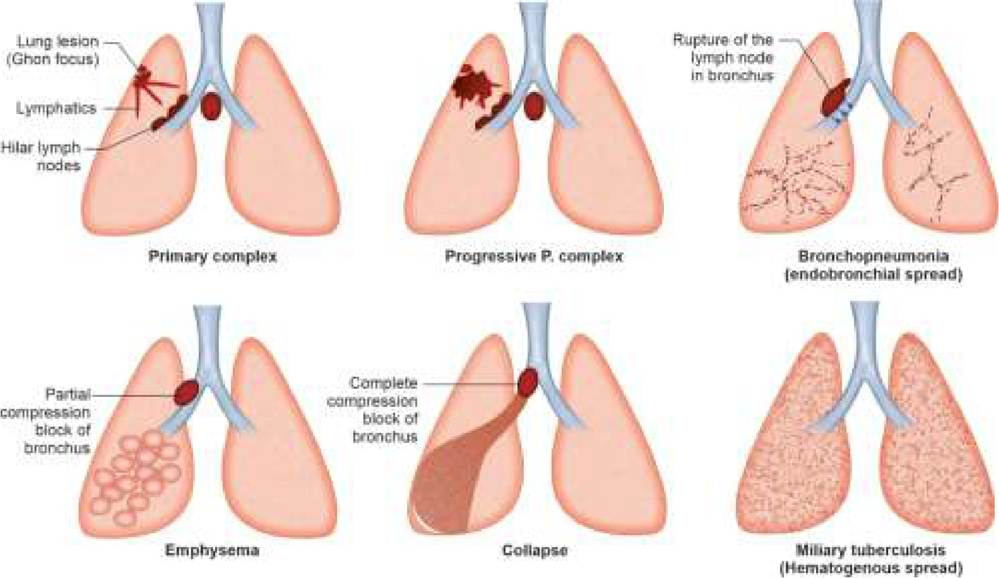
Fig. 10.4: Common X-ray findings in pulmonary tuberculosis.
TABLE 10.21: Ziehl-Neelsen staining for AFB - method
• Dry the slide (15-30 minutes) and fix over a flame
• Cover with carbolfuchsin and heat till vapours rise
• Leave for 5 minutes, then rinse in running water
• Stain with 25% sulfuric acid (2—4 minutes), then rinse
• Stain with 0.1% methylene blue (30 seconds), then rinse
• Examine under high power and oil immersion
used as a proxy for multidrug resistance disease (MDR-TB).
- Line probe assay (LPA) are molecular tests to detect MTb complex and rapid diagnosis of Rifampicin and INH resistance by first-line LPA (LPA-FL) and resistance to fluoroquinolones and other second- line drugs by second-line LPA (LPA-SL). LPA needs many DNA copies (gt;10,000 per ml) for detection and can be used only on smear-positive or culture isolates with processing time of ~72 hours each for both LPA-FL and LPA-SL.
In NTEP, LPA-FL is indicated in all cases of confirmed tuberculosis and LPA-SL in cases of RR- TB or or INH resistance.
• Histopathological diagnosis is commonly used to confirm the diagnosis of EPT, using fine needle aspiration cytology (FNAC) or biopsy of the suspected lesion, showing presence of chronic inflammatory infiltration, giant cells and caseation. These specimens should also be used for microbial diagnosis and drug sensitivity/resistance testing.
• Tuberculin sensitivity test (TST) is a simple, widely used test to detect latent tuberculosis based on the presence of delayed type of hypersensitivity (DTH) against tuberculosis—an indicator of prior natural infection or BCG vaccination.
Tuberculin is a protein suspension of M. tuberculosis, available as purified protein derivative (PPD), with antigen load denoted as test units or TU (1 TU = 0.00002 mg PPD). Considering variable potencies of PPD derived from different strains, WHO recommend use of a standardized PPD-S, derived from RT-23 strain and stabilized with an additive Tween 80. In India, 2 TU of PPD-S is recommended for TST.
Mantoux test (MT) is the commonly used method for TST (others include heaf test or tine test), done and interpreted as follows:
- 0.1 ml of PPD-S (2 U) is administered intradermally using a TT syringe on volar aspect of forearm to raise a wheal of ~5-8 mm at the site of injection. This wheel subsides in 15-30 minutes and no reaction is visible locally for next 6-8 hours. In presence of DTH either due to previous natural infection or BCG vaccination, a local induration appear after 6-8 hours and peaks at 48-72 hours, associated with erythema.
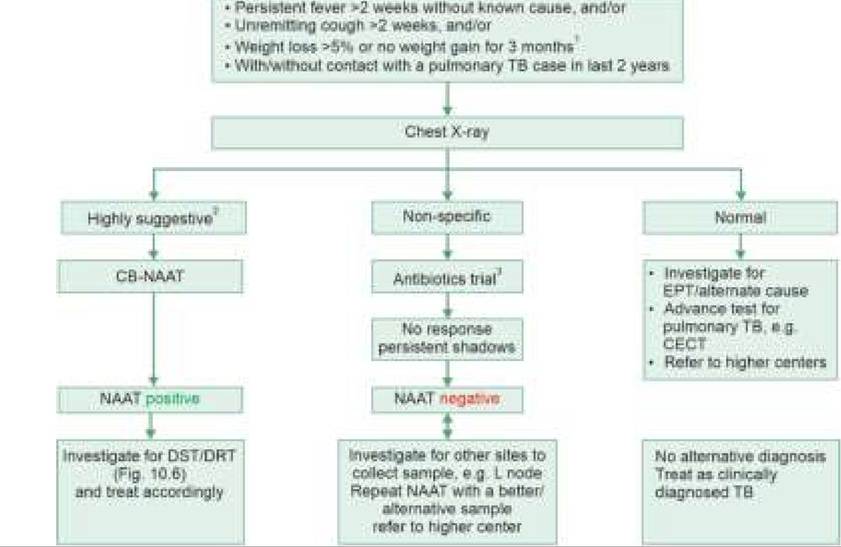
Fig. 10.5: Tuberculin (Mantoux) test.
- Size of this induration (not erythema) should be read after 48-72 hours (up to 7 days), by a ball-point method, in transverse direction (Fig. 10.5).
- An induration of 10 mm is considered as positive (5 mm in HIV infected), suggestive of previous natural infection. BCG is unlikely to produce an induration of gt;5 mm.
- Diagnostic errors in TST include:
#9632; False negative TST in: (1) severe disease, e.g. military tuberculosis or tubercular meningitis, (2) severe malnutrition, (3) infection-induced anergy-up to 3 months after pertussis or measles, (4) immunocompromised states, e.g. HIV, (5) recent infection, as TT conversion takes 2-3 months after infection, (6) technical errors, e.g. inactive tuberculin, subcutaneous injection, etc.
#9632; False positivity is rare, due to: (1) use of higher PPD strength for testing, (2) presence of non- tubercular mycobacterial infections, e.g. atypical mycobacteria or leprosy, and (3) secondary infection at the site.
- TST alone should not be used for diagnosis of tuberculosis but only to support the diagnosis of: (a) latent TB, (b) bacteriologically negative cases. It is also used to - (c) test the success of BCG vaccination,
(d) identify the need for BCG vaccination in older TST-ve children, and (e) measure the prevalence of infection in the community.
- A new C-TB test to detect tuberculin skin sensitivity is in pipeline, which is not affected by prior BCG vaccination.
• Interferon gamma release assay (IGRA), commercially available as TB quantiFERONgold® or TB Spot® is an in vitro test to detect interferon (IFN)-gamma production by mononuclear cells in response to M. tuberculosis antigens. Like TST, positive IGRA test also indicates presence of TB infection but does not confirm the presence of disease. IGRA is expensive but unlike TT, does not require repeat visit for test reading or crossreact with BCG vaccination.
• Biochemical investigations are not diagnostic but may be used differentiate tubercular from pyogenic
etiology in EPT, e.g. CSF, ascites or pleural/pericardial effusions.
Tubercular exudate is characterized by: (a) strawcolour appearance, (b) cobweb formation on standing due to high fibrinogen content, (c) predominant lymphocytic leukocytosis, and (d) lesser elevation of proteins than in pyogenic exudate.
Other useful biochemical markers include presence of elevated adenosine deaminase (ADA) and tuberculostearic acid (TSA) levels in exudates—produced by degradation of lymphocytes and tubercular bacilli respectively.
• Serodiagnosis of tuberculosis involves detection of specific TB antigens (A60) or antibodies (IgM/IgG) in body fluids, though none of them differentiates infection from active disease and have no role in diagnosis of tuberculosis.
In NTEP 2022,
• Confirmed TB refers to a bacteriologically confirmed case on smear microscopy, culture or WHO recommended rapid diagnosis test, e.g. XpertMTB/RIF.
• Clinically diagnosed TB refers to a case, which is not bacteriologically confirmed but has been diagnosed as having active TB by a medical practitioner, who has decided to give full course of TB treatment. It includes cases dignosed on the basis of X-rays, suggestive history and extra-pulmonary disease without laboratory confirmation.
• Probable TB refers to at least one sign or symptom (unexplained fever, cough, weight loss) with chest X-ray consistent with tuberculosis and one of the following: (a) response to TB therapy, and/or (b) documented exposure and/or immunological evidence of TB infection.
Management of tuberculosis depends on the type and severity of the disease, DST and patient characteristics. For the sake of clarity, it has been discussed in following sections:
a. Anti-tubercular drugs
b. Anti-tubercular regimens
c. Supportive and symptomatic therapy
d. Monitoring and follow-up
A. Antitubercular drugs may be broadly divided into:
• First-line drugs are highly effective and least toxic, used in the majority of cases and include four drugs - Isoniazid (H), Rifampicin (R), Pyrazinamide (P), Ethambutol (E). Streptomycin is no longer used as first-line drug (Table 10.22).
• Second-line drugs are less effective and more toxic, used only in cases with resistance to one or more first- line drugs. These drugs are classified in three groups, based on their efficacy and experience in treatment of drug-resistant cases (Table 10.23). While all three
Maximum dose*: H 300 mg, R 600 mg, Z 2000 mg, E 1500 mg All drugs given orally as single dose on empty stomach.

drugs from Group A and one or two drugs may be included in second-line regimen, Group C drugs should be added only if Group A/B drugs cannot be used due to resistance or intolerance.
Bedaquiline is the heart of second-line anti- tubercular regimen at present, except that it is not licensed for used in children below 5 years.
B. Antitubercular regimens: Multi-drug therapy is the cornerstone of anti-tubercular therapy, based on following considerations:
• Each case has different types of bacillary populations in the same lesion, including extracellular or intracellular organisms and slow-growing or rapidly- growing organisms. Some drugs act better on some bacillary sub-populations than others. H and R act best on fast-growing bacilli, Z on intracellular organisms and R on extracellular slow-growing bacilli.
• An effective drug regimen should use a mix of these drugs to attack all sub-populations of organisms. Ethambutol, though bacteriostatic drug with poor efficacy, is largely included in these regimens to prevent development of resistance to other drugs.
• An effective drug regimen should only include the drugs for which phenotypic sensitivity has been demonstrated on cultures or the resistance has not been detected on molecular testing. Indian data has shown maximum resistance to H (13%) followed by R (7%) and rarely to second-line other drugs (2-3%).
• An effective drug regimen should not contain less than four drugs at a time. In fact, drug-resistant cases usually need more than 5-6 drugs due to relatively less efficacy of second-line drugs.
• Since the emergence of drug-resistant mutations is higher in early stages of treatment due to higher bacillary load, antitubercular regiments are usually biphasic - including an:
- Intensive phase (IP) to rapidly decrease the bacillary load, reduce infectivity and prevent deterioration and death, and a
- Continuation phase (CP) to eliminate residual bacilli and reduce the risk of treatment failure and relapse. As fewer bacilli are left after IP, continuation phase usually needs fewer drugs.
• Since the dividing time of TB bacilli is ~21 hours, all drugs should be administered once a day, with no role of intermittent chemotherapy, unlike practiced earlier.
Universal Drug ResistanceZSensitivity Testing: NTEP 2022 recommends selection of appropriate drug regimen based on DST/DRT profile of cases, irrespective of previous treatment status (unlike previous protocols). All cases should be offered universal testing as per following algorithm (Fig. 10.6):
• Two appropriate body fluid / tissue specimens should be collected from every patient and sent to laboratory in a cold chain - one for the CBNAAT and another for culture and sensitivity (preferably MGIT). EPTB samples should not be collected in formalin.
• Based on CBNAAT report, cases are divided into MTB detected (confirmed) or not detected (negative/ presumptive). Confirmed TB cases are also further divided into - Rifampicin sensitive (RS-TB) or
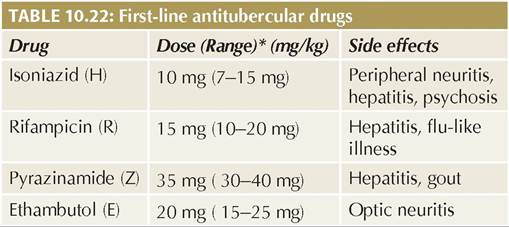
Fig. 10.6: Diagnostic algorithm for suspected drug resistant tuberculosis in children
*For discordance for RR between NAAT and FL-LPA, repeat NAAT at LPA laboratory
**Repeat NAAT in cases of RR-TB in a treatment-naive case
FL-LPA: First line-line probe assay, SL-LPA: Second line-line probe assay, for other abbreviations, see text
Rifampicin-resistant (RR-TB). If RR is detected with a very low level in a patient with low clinical suspicion, it should be confirmed on a repeat sample.
• All cases of RS-TB should be started on first-line regimen (discussed later) and tested by LPA-FL to confirm R-sensitivity and detect H-resistance. In case of LPA-FL showing:
- H-sensitivity, continue with first-line ATT.
- H-resistance, first-line ATT must be revised to H-mono/poly regimen, (discussed later) along with asking for LPA-SL.
- Discordance with CBNAAT report in terms of R-sensitivity, CBNAAT should be repeated from another good sample.
• All cases of RR-TB should be subjected to LPA-SL to detect resistance to fluoroquinolones (Flq) and second- line injectable (SLI) drugs.
• Treatment should be initiated on the basis of LPA results, which may need to be modified later according to DST on liquid culture (LC-DST).
Drug Resistant Tuberculosis (Nomenclature): For the treatment purpose, all tuberculosis cases are classified on the basis of drug-resistance pattern, as follows:
• Mono-resistant (MR-TB), with resistant to one first-line drug only.
• Isoniazid-resistant (Hr-TB), with resistance to INH but susceptibility to RMP.
• Poly-drug resistant (PDR-TB), with resistance to more than one first-line drugs, other than both H and R.
• Rifampicin resistant (RR-TB), with resistance to R, with/ without other drugs.
• Multidrug-resistant MDR-TB). With resistance to both H and R, with/without resistance to other drugs. All cases of RR-TB are considered as H-resistant as well unless proved otherwise, hence, should be treated as MDR-TB.
• Pre-extensively drug-resistant TB (Pre-XDR-TB), including MDR/RR-TB with resistance to fluoroquinolones (levoflox or moxiflox).
• Extensively drug-resistant TB (XDR-TB), including MDR/RR-TB with resistance to fluoroquinolone and at least one additional second-line drug from Group A, i.e. Bedaquiline and/or Linezolid.
Treatment Regimen: NTEP-2022 recommends following Regimens for Childhood TB, depending on DST/DRT (Table 10.24):
• First-line regimen for All RS-TB (without H-resistance) including four drugs for 2 month of intensive phase and three drugs for 4 months for continuation phase (2HRZE + 4 HRE) with following considerations:
- Continuation phase is extended to 10 months in cases of neurotuberculosis or spinal tuberculosis, with total duration of 12 months. (Intensive phase is not extended)
TABLE 10.24: TB treatment regimen as per DST/DRT
1. RS-TB with No H resistance
All cases 2 HRZE +4HRE*
2. RS-TB with H mono/poly resistance
All cases (6 ) Lfx R E Z ( No intensive/maintenance phase)
3. RR/MDR TB (No FQ Resistance)
(Non-extensive/Non-Diseminated PTB, Non-severe EPTB)
| Age gt;5 yrs/15 kg | IP (4-6 mo) Lfx, Cfz, Z, E, Hh, Eto, Bdq (6 mo) CP (5 mo) Lfx, Cfz, Z, E |
| Age lt; 5 yrs/15 kg (Shorter oral regimen) | IP (4-6 mo) Mfxh, Km/Am, Cfz, Z, E, Hh, E CP (5 mo) Mfxh, Cfz, Z, E |
4. RR/MDR TB, but No FQ Resistance (Extensive/Disseminated PTB, severe EPTB)
| Age gt; 5 yrs/15 kg (Longer oral regimen) | (18-20) Lfx, Lzd, Cfz, Cs, Bdq (6 mo or more) (Replace Bdq with Dlm in children 6-1 7 years) |
| Age lt; 5 yrs/15 kg | Replace Bdq with any group C drugs |
5. Pre-XDR TB with FQ Resistance
Customized treatment with expert consultation
6. XDR TB with Resistance to FQ + one more group A drug
Customized treatment with expert consultation
*Extent continuation phase to 10 months for Neuro/Spinal TB **Extend to 9 months for extensive disease, uncontrolled co-morbidity, ExPT or any change in regimen due to resistance/intolerance. Extend to 12 months for Spinal and Neuro TB.
Ak: Amikacin; Bdq: Bedaquiline; Cfz: Clofazimine; Cs: Cycloserine; Dlm: Delanamid; Eto: Ethionamide; FQ: Fluoroquinlone Hh: High dose INH; Km: Kanamycin; Lfx: Levofloxacin; MDR: Multidrugresistant; Mfx: Moxifloxacin; IP: Intensive phase; CP: Continuation phase
- First-line regimen is also used for all: (a) cases with clinically-diagnosed TB or (b) cases who have been treated in the past even with history of treatment failure, default or recurrence, provided they are RS-TB at present.
- Fixed-drug combinations (FDCs) are available under NTEP for first-line regimen and preferred due to simplified treatment and no risk of missing one or more of combination drugs.
• H-resistant TB, with/without resistance to other first-line drugs, should be treated with a monophasic regimen of four drugs (6 LfxRZE) for six months, i.e.: (a) replacing INH with Levofloxacin, and (b) no continuation phase.
• RR-/MDR-TB without resistance to second-line drugs should be treated with different regimens including second-line drugs depending on the severity of disease and age of the child (Table 10.24). These regimens with higher pill burden and toxicity profile need longer duration of treatment. In case of intolerance to component drugs in second-line regimen, management has to modified in consultation with experts to decide the replacement sequence.
• Pre-XDR/XDR TB must be managed with tailor-made regimens in consultation with experts, replacing resistant drugs with group C drugs.
Probable or clinically diagnosed MDR-TB, with risk factors, e.g.: (a) close contact with a person having MDR-TB, treatment failure, death on treatment, (b) prior treatment with second-line drugs, and (c) no response to first-line regimen after excluding other cause of non-response, must also be managed in consultation with experts. In these cases, drug regimen is usually decided based on the drug sensitivity pattern of the likely source-case, if possible.
C. Supportive therapy includes adequate nutrition, management of co-morbidities, symptomatic treatment and treatment of complications, e.g. hydrocephalus, electrolyte imbalance, etc. Some specific issues in supportive management are as follows:
• Pyridoxine: Isoniazid interferes competitively with pyridoxine metabolism and may result in peripheral neuropathy. NTEP recommends pyridoxine supplementation (10 mg/day) to all children on INH- containing regimen.
• Steroids help in selected cases by reducing of excessive inflammatory damage and exudation, and facilitating intracellular penetration of drugs. Prednisolone (PO 2 mg/kg/day q8hr) is used for 2-4 weeks followed by gradual tapering only in: (a) tubercular meningitis, (b) military tuberculosis, (c) extensive endobronchial tuberculosis, (d) pericarditis, (e) large pleural effusion with distress and (f) immune reconstitution inflammatory syndrome (IRIS).
• Surgery may be indicated in large tubercular lesions to remove residual lesions after completion of antitu- bercular therapy, e.g. in lymphadenitis, segmental/ lobar lung lesions or extrapulmonary tuberculosis.
D. Monitoring andfollow-up: All children on ATT should be closely monitored for disease response, compliance and treatment, including clinical and laboratory followup. Clinical follow-up is advised even after completion of treatment for 2 years.
Clinical follow-up must focus on: (a) changes in clinical symptoms and signs, (b) physical examination, including weight record, (c) side-effects of medications, (d) adherence to treatment.
Laboratory investigations are needed only if indicated clinically, except repeat microbiological testing of respiratory secretions at the end of IP and CP, if possible. Liver function test are not routinely required without evidence of hepatopathy. Follow-up chest radiographs should be performed only at the end of therapy or earlier if no clinical improvement. Some important issues on follow-up are as follows:
• Treatment interruptions in the first-line regimen up to four weeks are managed by resuming the therapy, though missed doses of IP should be completed before starting CP and missed doses of CP should be completed by extending the duration of therapy.
However, in cases with longer interruption (gt;4 weeks), patient must be re-investigated for resistance profile, as in fresh case.
• No-response or deterioration during follow-up: All cases who do not respond satisfactorily or deteriorate on ATT are not due to drug resistance. Common causes of treatment failure include: (a) incorrect diagnosis in a clinically diagnosed case, (b) lack of adherence to therapy, (c) incorrect drugs or dosages, (d) inability to retain drugs, e.g. vomiting after medications,
(e) comorbidities, and (f) paradoxical upgrading reactions, apart from drug resistance. All cases with poor response should be evaluated for these cases.
• Paradoxical upgrading reactions (PUR) refers to enlargement of existing lesions or unexpected appearance of new lesions during apparently adequate antitubercular therapy. These reactions usually develop after 3-12 weeks of the initiation of therapy and lasts for ~2 months before spontaneous resolution. PUR represent improvement of local immunity and accumulation of inflammatory exudates at previously small or invisible lesion and may present with new lesions or increase in size of existing lesions, e.g. lymph nodes, pulmonary infiltrates, pleural effusion, tuberculoma, etc. Lack of systemic symptoms suggests paradoxical reaction, though diagnosis should never be made without excluding DR-TB.
• Drug-induced liver injury (DLI) may develop in ~5% cases on first-line regimen, usually within first month of starting treatment due to three hepatotoxic drugsINH, RMP and PZA. While routine liver function tests are not necessary, all suspected cases must be investigated for liver functions.
DLI is diagnosed in presence of any one of the following:
• gt; 5 times elevation in AST / ALT values in asymptomatic patient,
• gt; 3 times elevation in AST / ALT values with gt; times elevation in bilirubin levels or
• Symptomatic patient.
Management of DLI includes withholding the offending drugs, e.g. RMP and PZA, and repeat LFT after a week. Withdrawn drugs are restarted in gradually increasing doses if AST / ALT drops lt; 2 times, in order of R followed by Z with AST/ALT monitoring every 3 days.
However, quot;Hepatosafe'' therapy with alternative drugs is indicated in seriously sick patients with DLI, e.g. meningitis or military disease, using minimum three drugs - Streptomycin, Fluoroquinolone and Cycloserine.
In case of the recurrence of DLI, alternative treatment options with prolongation of treatment must be considered.
Prevention: Apart from public health measures to control airborne infections, important preventive measures to control TB in children include:
• Early detection and treatment of infectious cases,
• Airborne infection control practices,
• Contact screening and TB preventive therapy (TPT), and
• BCG vaccination.
TB preventive therapy (TPT) is indicated using single drug-INH PO 10 mg/kg/day (7-15 mg/kg/day range) in children lt;10 years and 5 mg/kg/day in older children (gt; 10 years) for 6 months, after ruling out the active disease, to all:
• All household contacts lt; 5 years of age of a bacterio- logically confirmed PTB within past 3 months, irrespective of BCG or nutritional status,
• All household contacts gt; 5 years of age of a bacterio- logically confirmed PTB, irrespective of the age, if they are positive on TT/IGRA.
• All HIV-infected children gt;1 year of age irrespective of the degree of immunosuppression, antiretroviral treatment or previous TB treatment.
• All HIV-infected infants lt;1 years of age, in contact with a pulmonary tuberculosis case.
• Babies born to mother diagnosed with tuberculosis during pregnancy.
• Other risk-groups individuals, e.g. those on immunosuppressive therapy, dialysis, planned for transplant, if they are positive on TT/IGRA.
TPT in contacts of MDR-TB, after exclusion of active disease depends on the sensitivity profile of contact case as follows:
• Contacts of RR-TB but FQ sensitive patients should receive TPI with Levofloxacin for 6 months (PO 15-20 mg/kg/day to max 75/mg/day).
• Contact of H-resistant R sensitive cases should receive RMP PO 15 mg/kg/day for 6 months (20 mg/kg/d above 10 years).
Congenital Tuberculosis
Congenital TB is not uncommon in Indian children though female sterility due to maternal genitourinary tuberculosis prevents many cases.
Mode of infection in these cases is either: (a) transplacental infection after placental lesion in mother (primary focus in liver), (b) aspiration of infected aminotic fluid (primary focus in lungs).
Clinically, congenital TB may be asymptomatic or presents as neonatal septicemia during 2nd-3rd weeks of life with fever, respiratory distress, hepatosplenomegaly, lymphadenopathy and meningitis (in 20-30%).
Diagnosis depends on maternal history of tuberculosis, placental examination for tubercles, clinical suspicion, neonatal chest X-ray and rarely, demonstration of AFB/
NAAT from gastric aspirate or bronchial lavage. TT is negative at birth in infected cases (but becomes positive by 2-3 months).
Management depends on clinical or radiological evidence of disease in the newborn. Separation from mother and avoidance of breastfeeding to prevent postnatal infection is not recommended, even in sputum positive mothers. NTEP/ IAP recommends that:
• All babies born to tubercular mother should be breastfed, though mother should practice cough-etiquettes.
• All babies should receive BCG vaccinated at birth, without prior TST.
• Babies with normal chest X-ray at birth should receive TPT with single drug INH PO 10 mg/kg/day for 6 months with/without Pyridoxine, if mother is having RS-TB. TPT is not recommended if mother is having RR/MDR-TB.
• Babies with abnormal chest X-rays at birth, should be treated as per DST/DRT.
• Simultaneous treatment of mothers must be ensured.
Prevention of congenital TB largely depends on early diagnosis and treatment of disease in pregnant women. Streptomycin, due to risk of vestibular damage in newborn, is contraindicated during pregnancy.
National Tuberculosis Elimination Programme (NTEP)
National Tuberculosis Elimination Programme (NTEP) is the current version of Revised National Tuberculosis Control Programme (RNTCP, 1995), to fulfill the vision of National Strategic Plan (NSP), i.e. to achieve quot;TB-free Indiaquot; by the year 2025 (Five years ahead to global target in 2030).
Elimination refers to (a) achieve 80% reduction in disease burden, i.e. incidence and prevalence of disease lt;44 and lt;65/lakh population respectively, and (b) 90% reduction in mortality, i.e. lt;3/lakh population.
Objectives: NSP rests on four pillars of interventions- DETECT, TREAT, PREVENT, BUILD. Accordingly, NTEP aims to:
• Achieve 90% notification rates
• Achieve 90% success rates for new cases and 85% for re-treatment cases
• To improve successful outcome of treatment of DR- TB cases
• To achieve decreased morbidity and mortality of HIV- associated TB
• To improve outcomes of TB care in private sector.
Operationally, NTEP is a centrally sponsored program under National Health Mission, managed by Central TB division, Ministry of Health and Family Welfare.
Activities: Some novel aspects of NTEP include:
• Screening of all cases with presumed TB disease, using standard screening (Fig. 10.3)
• Confirmation of diagnosis using standard algorithms and necessary investigations.
• Universal drug-resistance and sensitivity testing for all confirmed cases (Fig. 10.6)
• Standard treatment regimens, depending on resistance/ sensitivity profile (Table 10.24)
• Provisions for nutritional support and direct benefit transfer, to ensure compliance and manage comorbidities.
• Use of Nikshya (NI- Nil, Kshya- TB) app - a web based information management system to ensure quality surveillance and monitoring.
10.14
More on the topic CHILDHOOD TUBERCULOSIS:
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- HEPATOMEGALY
- LUNG ABSCESS
- INFORMING INTERVIEW
- Introduction
- Feet
- A MODEL AND ALGORITHM FOR EQUAL-OPPORTUNITY POLICY
- Particularities of Field Paratuberculosis Vaccination Evaluation
- BRONCHIAL ASTHMA
- CHRONIC GLOMERULONEPHRITIS