CLINICAL EVALUATION FOR CARDIAC DISEASE
While presence of a 'murmur' is the most recognized indicator of underlying heart disease, it should be remembered that:
• All murmurs are not organic and functional murmurs are common in infancy due to relatively higher blood volume passing through small size valves and
• Absence of murmur does not exclude heart disease, which may be absent in large shunts or cardiomyopathies.
Clinical assessment for a cardiac disease includes a detailed history, thorough clinical examination and relevant investigations, discussed in following sections. Common clinical indicators of cardiovascular disorders are enumerated in Table 17.1.
History taking in a suspected heart disease, must concentrate on following symptoms, which provide valuable clues about the diagnosis, etiology and severity of a cardiac illness as well as presence or absence of complications.
Breathlessness (Dyspnea) is an important symptom of heart disease, indicating compromised oxygen supply to tissues either due to impaired myocardial function or altered pulmonary blood flow. It may be present throughout the day or develops only on exertion and may be graded according to New York Heart Association (NYHA) grades as follows:
Grade I: Dyspnea on unaccustomed exercise,
Grade II: Dyspnea on usual day-to day activity,
TABLE 17.1: Common indicators of CVS disease
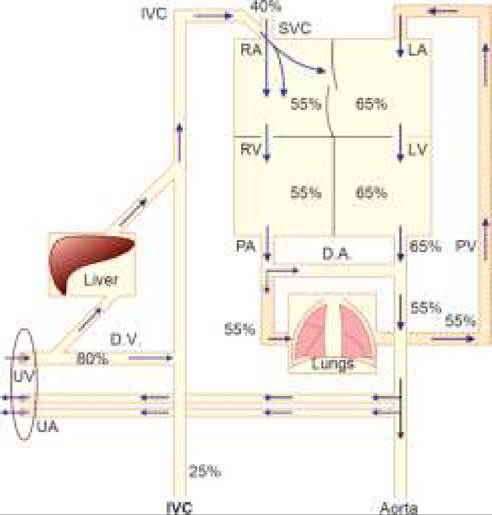
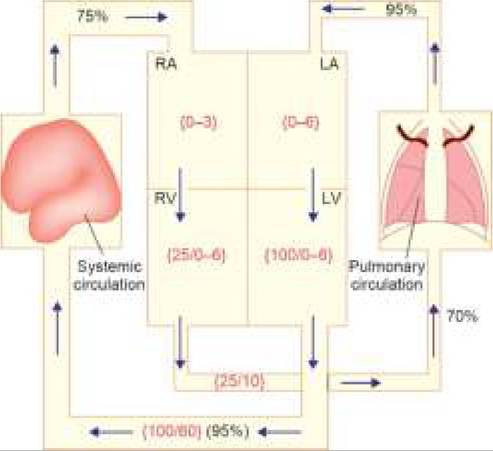
Fig. 17.5: Pressure relationships (mm Hg, in color) and oxygen saturation (% in black) in postnatal circulatory physiology.
• Clinical history
- Unexplained failure to thrive
- Ill sustained sucking on breast
- Dyspnea on exertion or rest
- Bluish discoloration on exercise/rest
- Recurrent chest infections
- Palpitation or chest pain
- Syncopal attacks
• Past history of rheumatic fever
• Family history of congenital heart disease
• Clinical signs
- CCF or LVF
- Cyanosis or cyanotic spells
- Abnormal heart sounds
- Abnormal murmurs
- Cardiomegaly
- Abnormal BP
• Signs of Co-existing disease
- Chromosomal/genetic disorders
- Intrauterine infections
- Other congenital defects
- Rheumatic fever
- Renal disease (hypertension)
- Systemic infections (myocarditis/pericarditis)
Grade III: Dyspnea even at minor activity but not at rest, Grade IV: Dyspnea at rest.
Severe dyspnea may also present as orthopnea, i.e., aggravation of breathlessness in lying down position. An orthopneic child prefers to sit on bed, even while in sleep.
Breathlessness in infants usually manifests with—(a) feeding difficulties, e.g. ill-sustained sucking or suck-rest- suck cycle with prolonged feeding time, and (b) feeding diaphoresis or excessive sweating over forehead due to sympathetic overstimulation due to exertion of feeding. Chest pain is not uncommon in many heart diseases due to breathlessness. However, chest pain of specifically cardiac origin is usually localized over precordium or left shoulder and may be due to pericardial or myocardial involvement.
• Chest pain in pericarditis typically aggravates in supine position and relieves on sitting and leaning forward.
• Chest pain due to coronary involvement is common in children with severe aortic stenosis, ALCAPA (Anomalous coronary artery from pulmonary artery) or acquired coronary blockade, e.g. in vasculitis and hyperlipidemic states.
Palpitation refers to patient's awareness or feeling of tachycardia, usually in cases of impending/established CCF or arrhythmia. Palpitation is also common in high- output CCF, e.g. anemia, thyrotoxicosis, fever and other disorders of hyperdynamic circulation, e.g. AR or PDA. Failure to thrive is common in cyanotic CHD or acyanotic CHD with increased pulmonary blood flow, due to poor feeding and breathlessness, leading to decreased oxygen and metabolic substrate supply for thriving. However, nutritional factors must be excluded in all cases.
Swelling (Edema) in heart disease is a sign of impending or established CCF, due to increased hydrostatic pressure and consequent leak of fluid in interstitial compartment. Cardiac edema typically - (a) begins from dependent parts of the body, i.e. sacrum in infants and dorsum of foot in older children, and (b) is more prominent in evenings after the whole day of cardiac exertion.
Bluish discoloration (Cyanosis) in a heart disease generally indicates right-to-left shunt (cyanotic heart disease), with following noteworthy features:
• Cyanosis is usually absent at birth in right to left shunts due to presence of PDA during first few days of life allowing enough flow to reach pulmonary circulation.
These cases are also termed as duct-dependent and appearance of cyanosis indicates closure of ductus.• Children with right to left shunts and substantial RV outflow obstruction often present with cyanotic spells (Ch 17.5.3).
• Appearance of cyanosis in a previously acyanotic child with left to right shunt may be an indicator of reversal of shunt or Eisenmengerization (C 17.5.2).
Fever in a cardiac disease may be an indicator of infective endocarditis or rheumatic fever, though may also be due to recurrent chest infections in presence of increased blood flow or coincidental causes.
Peripheral signs have important diagnostic values in a heart disease and must be assessed carefully before proceeding on cardiac examination. Important peripheral signs are as follows:
Pulse is usually assessed by three-finger palpation over radial artery at ulnar border of wrist, for: (a) rate, (b) rhythm, (c) volume, (d) character, (e) tension. In newborns or infants, heart rate (HR) is counted on chest rather than the pulse rate. Important characteristics of pulse include:
• Rate varies with age and physiological state, e.g. sleep and exercise. As a simple rule, normal HR is 120/ minutes till 1 year of age; and then drops at a rate of 10/min/every 3 years, i.e. 110 at 3 years, 100 at 6 years, 90 at 9 years and 80 at 12 years.
± Tachycardia may be physiological during exercise or excitement or pathological, e.g. fever, CCF, rheumatic carditis, myocarditis, early shock, arrhythmia, poisoning (atropine), etc.
± Bradycardia may be physiological in athletes or pathological, e.g. enteric fever, heart blocks, raised intracranial pressure, digitalis toxicity, etc.
• Rhythm is normally regular, except respiration related variations-HR decreases during inspiration due to negative intrathoracic pressure gt; increased systemic venous return gt; better diastolic filling of RV gt; #8593; stroke volume gt; #936;HR and increases during expiration due to positive intrathoracic pressure gt; reduced systemic venous return gt; reduced diastolic filling of RV gt; ^stroke volume gt; #8593;HR.
For important rhythm abnormalities (arrhythmia), see Chapter 17.10.• Vo lume of the pulse represents systolic blood pressure (BP) that normally falls during inspiration despite better diastolic filling of RV due to pooling of blood in expanded lungs gt; reduced pulmonary venous return gt; reduced LV stroke volume; and increases during expiration due to squeezing of lungs gt; increased pulmonary venous return and gt; increased LV stroke volume. Common abnormalities include:
Low-volume pulse in shock, aortic stenosis.
Pulsus paradoxus due to exaggerated inspiratory drop in BP and pulse volume during inspiration exceeding 10 mm Hg. This leads to complete disappearance of peripheral pulse during inspiration with an apparent difference between HR and pulse rate (paradox). It is seen in compressive conditions over heart, limiting diastolic filling during inspiration, e.g. constrictive pericarditis, CCF, status asthmaticus, tension pneumothorax, etc.
• Character: Normal pulse has a small, anacrotic 'a' wave (early systole) followed by big tidal 't' wave on up-stroke (late systole) and a dicrotic notch 'n' (closure of aortic valve) followed by a dicrotic 'd' wave on down-stroke (reflected flow from closed aortic valve). Normally, only 't' wave is palpable. Common abnormalities of pulse character include:
- Thready pulse, in impending shock.
- Water-hammer pulse, i.e. a large bounding pulse that disappears suddenly, associated with wide pulse pressure (gt;40 mm) due to leak from arterial side (aortic run-off), e.g. in—(a) cardiac causes, e.g. AR, PDA, ruptured coronary sinus, etc. or (b) peripheral causes, e.g. large arteriovenous fistula, anemia, beriberi, etc. Water-hammer pulse is best felt at radial artery with elevated arm that accentuates arterial emptying by retverse flow.
- Anacrotic pulse, i.e. slow-rising and low-volume pulse that appears to be beating twice due to prominent 'a' wave, seen in aortic stenosis.
- Pulsus alternans, i.e. alternate strong and weak pulses due to myocardial dysfunction, is seen in myocarditis, cardiomyopathy, left ventricular failure and supraventricular tachycardia.
Other abnormalities, e.g. dicrotic pulse, pulsus bisferens, etc. are rare in children.
Blood pressure (BP) should be recorded with appropriate methodology, discussed in Ch 17.12. Important BP characteristics in children include:
• Normal BP varies with age, sex and body size. American Academy of Pediatrics, 2017 has suggested age-and sex-dependent screening cut-off values for normal blood pressure in children, above which detailed evaluation is warranted (see Table 17.39).
• Normal pulse pressure (SBP-DBP) is lt;25-30 mm Hg. Wide pulse pressure of gt;40 mm indicates causes of waterhammer pulse, discussed earlier.
• Systolic BP is ~5-10 mm less in inspiration than in expiration (see pulse-volume changes). More than 10 mm drop in inspiratory BP indicates causes of pulsus paradoxus, discussed earlier.
• BP in relative higher (~10 mm) in lower limbs than in upper limbs due to more muscle mass and consequently higher vascular resistance. Higher BP in upper limb than in lower limbs, indicates coarctation of aorta, aortoarteritis, Takayasu disease, etc., while unequal BP in both arms suggests pre-ductal coarctation of aorta.
Temperature must be recorded in all cardiac cases on admission and periodically for early diagnosis of superadded infections, e.g. pneumonia. Persistent mild to moderate fever may also be an indication of rheumatic fever or infective endocarditis.
Respiratory rate in a cardiac case is increased to maintain tissue oxygen supply despite compromised pulmonary perfusion in cases of increased or decreased pulmonary
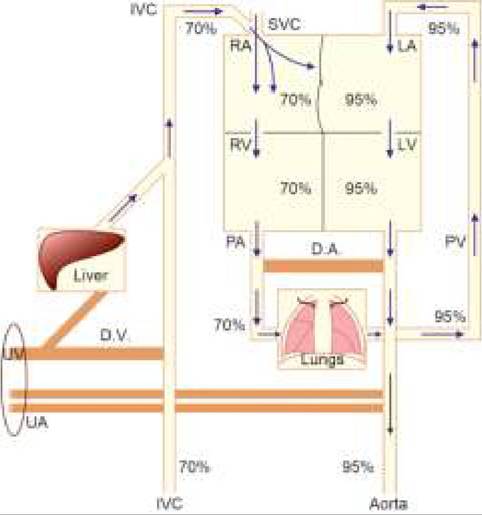
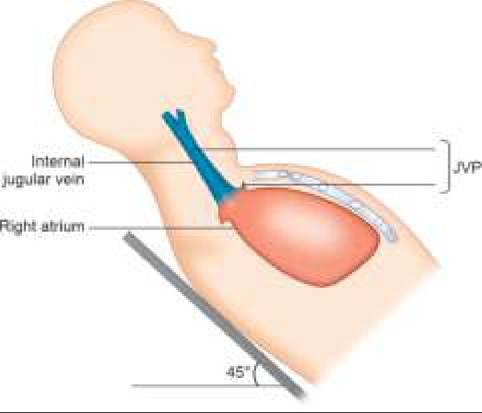
Fig. 17.6: Jugular venous pressure (JVP).
blood flow or impending or established CCF. RR varies with age and a RR of gt;60#8725;min below 2 mo of age, gt;50/ min from 2-12 mo and gt;40#8725;min in older children is considered as abnormal.
Jugular venous pressure (JVP) corresponds well with RA pressure, when assessed in semi-reclining position (45°) and measured correctly (Fig.
17.6). JVP may be difficult to appreciate in young children, due to shorter neck and struggling child. It may be erroneously high in supine position or low in upright position. Important characteristics of JVP are:• Normal JVP is 3-4 cm of water, raised in: (a) CCF, (b) constrictive pericarditis, (c) SVC obstruction, and (d) status asthmaticus.
• JVP changes with respiration, being less in inspiration (negative intrathoracic pressure facilitates venous return) than in expiration (high intrathoracic pressure opposes venous return). In pericardial tamponade, JVP rises paradoxically in inspiration due to raised intra-pericardial pressure (Kussmaul's sign).
• Hepatojugular reflux: If a pressure is applied over liver for 30 seconds, JVP initially increases due to the increased venous return but falls rapidly, due to the capacity of normal myocardium to accommodate extra blood. Sustained elevation of JVP (gt;1 minute) denotes positive hepatojugular reflux, seen in early CCF.
• Normal JVP consists of 3 positive (a,c,v) and 2 negative (x,y) waves. Unlike adults, these waves are difficult to appreciate in children, except in tricuspid atresia, when giant 'a' waves (due to atrial contraction against absent TV) are present.
Cyanosis, i.e. quot;bluish discoloration of nails and/or mucus membranesquot; indicates increased amount of reduced hemoglobin (gt;5gm/dl) in capillary blood. Note that cyanosis may be absent in severe anemia despite severe hypoxia, due to low hemoglobin levels.
TABLE 17.2: Causes of cyanosis
• Central cyanosis
- Cardiac: Rt to Lt shunt, Eisenmengerization
- Pulmonary: Respiratory failure, severe asthma
- Abnormal Hb: Methemoglobinemia, HbM disease
- Physiological: High altitude
• Peripheral cyanosis
- Physiological: At birth, cold exposure
- Hypoxia
- Circulatory shock
- Polycythemia
• Differential cyanosis
- PDA with shunt-reversal (only in lower limbs)
- PDA with TGA (only in upper limbs)
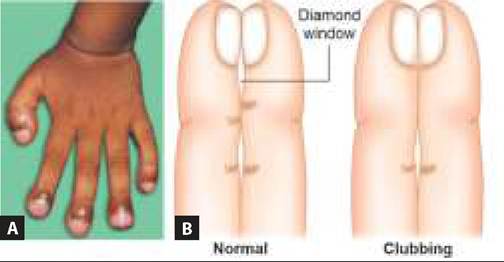
Fig. 17.7: Clubbing : (A) Clinical picture; (B) Schamroth sign.
Clinically, cyanosis is best visible on nails and mucus membranes, e.g. lips, tongue and palpebral conjunctiva, with three clinical types (Table 17.2):
• Peripheral cyanosis, visible on nails but not on mucus membranes, usually indicates local vascular stasis. Peripheral cyanosis is usually transient and disappears rapidly on warming/rubbing of limb to improve the local circulation.
• Central cyanosis, visible on nails as well as on mucus membranes, does not disappear easily with above measures. Central cyanosis may be due to pulmonary and cardiac etiology, further differentiated by hyperoxia test-reduction of cyanosis (or increase in PaO2 gt;60 over basal value) after 100% oxygen inhalation for 10-30 minutes, indicates pulmonary etiology. Cardiac cyanosis does not improve substantially after hyperoxia test.
• Differential cyanosis is seen only in upper or lower limbs and indicates Rt gt; Lt shunt at PDA level.
Clubbing is the ‘bulbous enlargement of the soft nailbed', due to dilatation of underlying blood vessels, opening up of deep AV fistulas, and associated interstitial edema/ tissue hypertrophy at finger-tips. Of varied etiology (Table 17.3), exact stimulus for these changes is unclear, probably relates to localized tissue hypoxia due to septic/aseptic micro-emboli. While clubbing usually develops only after gt; 6 months of persistent pathology, it may develop within 4-6 weeks in infective endocarditis.
Severity of the clubbing is graded as:
I. Softening of nail bed on palpation
II. Obliteration of angle at nail bed (Schamroth sign)*
III. Increased horizontal/vertical curvature of nails (Parrot-beak or drumstick appearance)
IV. Hypertrophic osteoarthropathy, i.e. painful swelling of hands/wrist with subperiosteal bone formation.
*Schamroth sign: Opposition of dorsal surfaces of two opposite terminal phalanges normally leaves a diamond-shaped aperture that disappears in clubbing (Fig. 17.7).
Other important peripheral signs in heart disease, e.g. arthritis, subcutaneous nodules, etc. in rheumatic fever or Osler nodes, Janeway lesions, etc. in infective endocarditis are discussed in respective chapters..
Cardiac examination: Examination of heart includes inspection, palpation, percussion and auscultation over the precordium. Location-wise, various cardiac findings are denoted in terms of various precordial area (Table 17.4). Note that these areas do not necessarily over-lie corresponding valves but represent the best sites to heart auscultatory abnormalities originating from them.
Inspection includes visual examination for: (a) precordial bulge, (b) apex impulse, (c) pulsations, (d) dilated veins or other visible abnormalities.
Precordial bulge may be due to: (a) cardiomegaly,
(b) large pericardial effusion, and (c) recurrent chest infections suggestive of increased pulmonary blood flow. Apex impulse, may not be well visualized in chubby children or pericardial effusion, or displaced in dextrocardia or ventricular hypertrophy.
Dilated chest veins indicate: (a) SVC obstruction, due to mediastinal mass, or (b) IVC obstruction, due to thoracic or abdominal lesions.
Visible pulsations may be diffuse (thin chest wall) or localized in tricuspid area/epigastrium (RVH), pulmonary area (PAH) suprasternal notch or neck (AR) or right hemithorax (dextrocardia).
Palpation confirms the inspection findings as well as provides additional information about: (a) apex beat, (b) parasternal heave, (c) diastolic shock, and (d) thrill.
ICS: Intercostal space
Apex beat is the outermost point of the cardiac impulse, normally located in 5th intercostal space within midclavicular line. It is relatively higher (4th space) in young infants due to small thoracic cage and developmental RV dominance. Important abnormalities include:
• Abnormal location:
- Outward and downward in LVH.
- Outward but not downward in RVH.
- On right side in dextrocardia or dextroversion.
• Abnormal character:
- Tapping (localized, forceful and ill-sustained) due to RVH, e.g. MS.
- Heaving (diffuse, forceful and well-sustained) due to LVH with systolic overload, e.g. AS, MR.
- Hyperdynamic (diffuse, forceful but ill-sustained) due to LVH with diastolic overload, e.g. AR.
Parasternal heave, i.e. palpable systolic impulse at left lower parasternal area indicates RVH.
Diastolic shock, i.e. palpable second heart sound (S2) in pulmonary area indicates pulmonary hypertension.
Thrills, i.e. palpable murmurs, felt like purring of cat sensation indicate organic murmur gt;grade III (see Table 17.6) and interpreted accordingly.
Percussion is of limited value in children, except that— (a) left cardiac dullness, extending beyond the apex beat indicates pericardial effusion, and (b) dull note in left 2nd parasternal space indicates pulmonary artery dilatation suggestive of PAH.
Auscultation over precordium relates to—(a) normal heart sounds, (b) abnormal sounds, e.g. opening snap, clicks and pericardial rub, and (c) murmurs.
Normally, four heart sounds (HS) are produced during cardiac cycle, though III and IV HS are not easily audible, best recorded on phonocardiography.
First HS (S1) denotes closure of atrioventricular mitral and tricuspid valves (MV/TV)) signifying end of the diastole. Normal S1 is a low-pitched sound, best heard at mitral area. Important S1 abnormalities include:
• Loud S1 due to forceful closing of MV/TV, before complete emptying of atria in disorders with increased atrial volume, e.g. (a) MS/TS, (b) hyperdynamic states, e.g. anemia, thyrotoxicosis and (c) Lt gt; Rt shunts.
• Soft or muffled S due to inadequate closure of MV in-(a) MR, or (b) rheumatic carditis.
TAPVR: Total anomalous pulmonary venous return, *see text
• Absent S1 due to tight MS.
• Split S1 in right bundle branch block due to delayed closure of TV.
Second HS (S2) is produced by closure of semilunar aortic and pulmonary valves (AV/PV), signifying the end of systole. S2 is best heard in pulmonary and aortic area, and has two distinct components - A2 and P2, corresponding to the closure of AV and PV respectively. As aortic ejection is more forceful due to thicker LV, AV closes earlier than the PV and hence, A2 component is heard earlier than the P2, leading to splitting of S2.
Splitting of S2 changes with respiration. During inspiration, split is wider due to negative intrathoracic pressure gt; pooling of blood in pulmonary vasculature
gt; #936; pulmonary venous return gt; #936; LV end-diastolic volume
gt; early closure of AV gt; early A2. During expiration, split is narrow or absent due to increased intrathoracic pressure
gt; #936; systemic venous return gt; #936; RV end-diastolic volume
gt; early closure of PV gt; early P2.
Intensity and splitting of S2 has significant diagnostic value in cardiology (Table 17.5). In ASD and total anomalous pulmonary venous return (TAPVR), atria are already dilated to maximum capacity, unable to accommodate extra flow during these respiratory changes. Hence, S2 split is wide and fixed in these cases. Third HS (S3) is rarely audible in normal children and indicates rapid early diastolic filling of ventricles due to large atrioventricular pressure gradient, e.g. in MR, TR or CCF. It is best heard in left lateral position, just after S2. Presence of S3 is often indicated by Gallop or Triple rhythm — a bad prognostic sign in CCF.
Fourth HS (S4) is produced by atrial contractions just before the S1 and is rarely audible in children, except in Ebstein's anomaly.
Opening snap, heard in MS, is a sharp high-pitched sound at mitral area, immediately after S2. It indicates snappy opening of MV to facilitate early-diastolic emptying of LV. Shorter the interval between S2 and opening snap, more severe is the MS. Opening snap is absent in very tight MS or calcified MV.
TABLE 17.6: Grades of murmur
TABLE 17.7: Causes of functional murmurs
I Inaudible, except on phonocardiography
II Faint, but audible murmur
III Easily audible murmur, but without thrill
IV Murmur with thrill
V Loud murmur, audible with ring of stethoscope
VI Very loud murmur, audible even if stethoscope is lifted up from the chest wall
Systolic ejection clicks are high-pitched, click-like sounds in aortic/pulmonary area, immediately after S1, due to forceful ejection of blood from overloaded ventricles into great vessels. Aortic ejection click, best heard in Erb' area (3rd Left parasternal space), indicates AS, severe AR or Coarctation of aorta. Pulmonary ejection click, best heard in pulmonary area during expiration, indicates PS or dilated pulmonary artery due to pulmonary arterial hypertension.
Pericardial rub, due to rubbing of inflamed pericardial layers in pericarditis, is audible in both systolic and diastolic phase. It may be differentiated from murmurs by—(a) scratchy character, (b) accentuation in sitting position and on pressure from stethoscope, and
(c) rapidly changing character, not lasting for gt;2-3 days. Murmurs indicate turbulence in the blood flow either due to-(a) normal flow across a narrowed valve or septal defect, or (b) increased flow across a normal valve in hyperdynamic states, e.g. anemia or in pathological shunts, e.g. VSD, PDA, etc.
All murmurs must be assessed for their—(a) location over precordium, (b) relationship with cardiac cycle, (c) intensity (Table 17.6), (d) character or pitch, (e) radiation to other sites, e.g. axilla (MR), clavicle (PDA), neck (AS), etc., and (f) changes with respiration, posture or other physiological events.
Important effects of physiological events on murmurs include:
• Left-sided murmurs are prominent in expiration, as pulmonary venous return increases due to raised intrathoracic pressure. Right-sided murmurs accentuate in inspiration as systemic venous return increases due to negative intrathoracic pressure.
• All murmurs except in mitral valve prolapse (MVP) or hypertrophic cardiomyopathy (HCM) are louder in supine than in standing position. MVP and HCM murmurs are best audible in squatting position.
• All murmurs, except in severe HCM, become louder on exercise.
• Most murmurs, except in MVP and HCM, decrease in intensity and duration on Valsalva maneuver.
Murmurs of VSD, MR and AR (LV volume-overload) become louder when systemic vascular resistance is
• Developmental (normal infants)
- Still's murmur*
- Axillary systolic murmur*
• Hyperdynamic circulation
- Normal newborns
- Severe anemia
- Fever
- Thyrotoxicosis
- Beriberi
- A-V fistula
*see text
raised by inflating a BP cuff over the arm, 20 mm above the systolic pressure.
Etiologically, murmurs may be functional (without underlying heart disease) or organic.
Functional murmurs are present in ~15-20% infants, due to developmental immaturity or hyperdynamic states (Table 17.7). These murmurs are characterized by - (a) soft systolic nature, (b) absence of thrill, (c) localized, and
(d) absence of other abnormalities. Common functional murmurs in children are:
• Still's murmur, a mid-systolic murmur at apex and lower left sternal border with typical musical quality, e.g. vibrating string, produced by vibration of semilunar valves or ventricular walls.
• Ejection systolic murmur at pulmonary area, due to sudden opening of pulmonary valve. This murmur is more prominent in cases with severe anemia.
• Systolic murmur at axilla and back in newborns, due to sharp angulation of pulmonary arteries at the origin from common trunk.
• Early systolic carotid bruit over clavicles, due to sudden gush of blood in carotids.
• Venous hum-a low-pitched, soft, continuous murmur over jugular veins, is common in severe anemia. It is best heard in sitting position with head turn on opposite side, accentuated by exercise and obliterated by distal pressure over neck veins.
Organic murmurs are essentially associated with an anatomical or pathological defect in heart. Depending on their relationship with cardiac cycle, these murmurs may be divided into:
A. Diastolic murmurs are almost always organic and originate either during forward flow through atrioventricular valves (usually mid-or late-diastolic), or regurgitant flow through semilunar valves (usually early-diastolic). Common causes of diastolic murmurs are:
• Early-diastolic (EDM) in AR or PR.
• Mid-diastolic (MDM) in MS, TS or flow murmurs in VSD, MR and TR.
• Late-diastolic (LDM) in MS or TS.
Note that all named murmurs are diastolic, e.g.
• Graham Steell's murmur, an EDM in pulmonary area, due to pulmonary hypertension.
• Carey Coombs murmur, an apical MDM in rheumatic carditis, due to mitral valvulitis.
• Austin flint murmur, an apical MDM in AR, due to functional MS.
B. Systolic murmurs originate during the forward flow through semilunar valves (usually early-or midsystolic), the regurgitant flow through atrioventricular valves, or from Lt gt; Rt shunts (usually pansystolic). Systolic murmurs may be functional or organic, though presence of thrill almost always indicates an organic murmur. Common causes of organic systolic murmurs include:
• Pan-systolic (PSM) in VSD, MR or TR
• Ejection systolic (ESM) in AS, PS, TOF, or flow murmurs in AR and pulmonary hypertension.
• Late systolic (LSM) in mitral valve prolapse.
C. Continuous murmurs are heard in Lt gt; Rt shunts or aortic regurgitant lesions with large pressure gradient, that persists even during systole. Important causes of continuous murmurs include:
• PDA or aorto-pulmonary window,
• Blalock-Taussig shunt,
• ASD with MS (Lutembacher syndrome),
• AR with AS or VSD,
• Coronary AV fistula or ruptured sinus of Valsalva,
• Bronchial collaterals or AV fistulas, common in cyanotic CHDs.
17.3
More on the topic CLINICAL EVALUATION FOR CARDIAC DISEASE:
- CLINICAL EVALUATION OF GIT DISEASE
- CLINICAL SPECTRUM
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- Cardiac Malignancy
- LABORATORY EVALUATION IN CNS DISEASE
- REVIEW OF FORENSIC ASSESSMENT INSTRUMENTS
- Parkinson Disease
- Cat Scratch Disease (Bartonellosis)
- Contributors
- CONGESTIVE CARDIAC FAILURE