DEVELOPMENTAL MILESTONES
Neurological development is assessed in terms of the milestones, i.e. easily identifiable events representing maturation of certain physical functions, e.g. sitting or smiling, which are expected to be achieved by a normal child within certain age limits.
Milestones may be broadly divided into five major domains:1. Gross motor milestones, e.g. sitting, standing, etc.
2. Fine motor milestones, e.g. handling of objects, feeding himself, etc.
3. Personal-social milestones, e.g. interacting with others, expression of emotions, etc.
4. Adaptive (Cognitive) milestones, e.g. ability to explore environment and learn from experiences.
5. Linguistic milestones, e.g. development of speech.
A. Gross motor milestones reflect maturation of locomotor functions and require normal neurological development as well as adequate muscle mass and tone. These functions may be delayed in grossly malnourished children, despite adequate neurological functions.
While lifting the chin momentarily from bed in prone position is the earliest recognizable gross motor milestone (4 weeks), persistent neck (head) holding is not achieved before 3 months and may be considered as the first key gross motor milestone for practical purpose.
TABLE 2.7: Key gross motor milestones
Age Gross motor milestone
1 mo Lifts chin momentarily in prone position
3 mo Neck-holding
4 mo Roll-over from supine to prone position
5 mo Roll-over from prone to supine position
6 mo Sits with support (Tripod position)
8 mo Sits without support
9 mo Crawls, pulls to stand
10 mo Stands with support, creeps
12 mo Walks without support
15 mo Walks, creeps upstairs
18 mo Runs, walks backward
24 mo Walks up and down-stairs (two-feets/step)
36 mo Rides tricycle, climb stairs one-foot/step
48 mo Hops on one foot, goes down-stairs one-foot/step
60 mo Skips with both feet
Table 2.7 enlists key gross-motor milestones till 5 years of age.
B. Fine motor milestones reflect development of certain fine skills, required for day-to-day functions like play, eat, draw, etc. These milestones are more reliable indicators of neurological maturity, as such skills are governed by large cerebral area and usually not affected in nutritional disorders. Isolated delay in maturation of these milestones indicates cerebral palsy or peripheral nerve injury, e.g. Erb's paralysis.
Important components of fine motor development in order of maturity include - (i) hand-eye coordination, e.g. reaching out for objects, (ii) hand coordination, e.g. grasping an object voluntarily, (iii) hand-hand coordination, e.g. transfer of objects, and (iv) handmouth coordination, e.g. feeding himself/herself.
Holding an object when offered in hand (voluntary grasp) at 4 months of age may be considered as the earliest and easily identifiable fine motor milestone, which is possible to achieve only after disappearance of neonatal grasp reflex. Table 2.8 enlists key fine-motor milestones till 5 years of age.
C. Adaptive milestones, also termed as cognitive mile stones, denote the development of the ability to explore environment and learn from new experiences. Achievement of adaptive milestones needs normal cognitive functions as well as normal special senses, e.g. vision and hearing.
Visual fixation to a moving object (4-6 weeks) may be considered as the earliest adaptive milestone, checked by observing infant's eye movements in response to a bright moving object, e.g. a red-ring tied to a string. Other adaptive milestones include visual exploration (handregard) or oral exploration of body parts (mouthing) and learning from experiences, e.g. searching for a hidden toy
TABLE 2.8: Key fine motor milestones
Age Fine motor milestone
4 mo Voluntary grasp (hold objects when given),
5 mo Bidextrous reach for an object (both hands)
6 mo Unidextrous reach, transfer of objects between hands
9 mo Immature pincer-grasp (probes with forefinger)
10 mo Mature pincer-grasp, release of object on request
12 mo builds tower of 2 cubes
18 mo Scribbles, tower of 3-4 cubes
24 mo Tower of 6 cubes, imitates vertical and horizontal lines
30 mo Tower of 8 cubes
36 mo Tower of 8-10 blocks, copies ‘circle'
48 mo Builds bridge, copies ‘cross'
60 mo Copies ‘Triangle'
| TABLE 2.9: Key adaptive (cognitive) milestones | |
| Age | Adaptive (Cognitive) milestones |
| 4 wks | Fixes vision on moving object up to 45° |
| 2 mo | Follows a moving person |
| 4 mo | Hand-regard, excited to see a toy/food |
| 5 mo | Mouthing, hand-regard disappears |
| 6 mo | Searches for a dropped toy |
| 8 mo | Finds partially-hidden objects |
| 12 mo | Mouthing stops, looks at pictures |
| 15 mo | Turns 2-3 pages at a time |
| 18 mo | Turns single page at a time |
| 24 mo | Points to 4-6 body parts, matches shapes |
| 36 mo | Knows name and gender |
| 48 mo | Right-left discrimination |
| 60 mo | Counts till 10, identifies coins |
or matching the shapes.
Table 2.9 enlists key adaptive milestones till 5 years of age.Many adaptive milestones tend to disappear after the learning process is complete. Hand-regard, i.e. exploration of own hand appears at 3-4 months and disappears by 6 months (Fig. 2.10). Similarly, mouthing appears at 5-6 months and disappears by the end of infancy. Persistence of hand-regard beyond 6 months or mouthing beyond 12 months suggests delayed neurological development.
D. Psychosocial milestones, i.e. development of interpersonal relationship and social skills, depend on higher cerebral functions as well as external inputs, e.g. normal vision and social stimulation. Social smile (~6 weeks) may be considered as the earliest psychosocial milestone. Table 2.10 enlists key psychosocial milestones till 5 years of age.
Isolated delay in these milestones indicates intellectual disability, autism, visual impairment and emotionally deprived child, e.g. orphans.

Fig. 2.10: Hand regard.
TABLE 2.10: Key personal-social milestones
| Age | Personal-social milestones |
| 6 wks | Social smile |
| 3 mo | Recognizes mother |
| 4 mo | Smiles at mirror image |
| 6 mo | Stranger's anxiety, enjoys ‘peek-a-boo' |
| 9 mo | Waves ‘bye-bye' |
| 12 mo | Responds to name, plays simple ball game, parallel play |
| 15 mo | Jargon, points to desired object |
| 18 mo | Domestic mimicry (copies parents, e.g. sweeping) |
| 24 mo | Dry by day, asks for food, show toys to others |
| 30 mo | Washes hands, brushes teeth |
| 36 mo | Dry by night, share toys |
| 48 mo | Goes to toilet alone, group-play |
| 60 mo | Dresses/undresses independently |
TABLE 2.11: Key Linguistic milestones
Age Linguistic milestones
6 wks Turns head towards sound
3 mo Makes cooing sounds
4 mo Laughs aloud
6 mo Says monosyllables (ma, da)
9 mo Says bi-syllables (mama, dada)
12 mo Speaks with vocabulary of two meaningful words
18 mo has vocabulary of 8-10 words
24 mo Speaks 2-3 word sentences, uses pronouns (I,You)
36 mo Asks questions, tells name and gender
48 mo Sing songs, tells stories
60 mo Speaks grammatically correct sentences
E.
Linguistic milestones require normal hearing, normal central functions as well as healthy organs of phonation. Hearing impairment is the most common cause of delayed language development. Startle response to a sudden sound in newborns suggests hearing ability. Appearance of monosyllables (6 months) may be considered as earliest proper linguistic milestone, though a younger infant is also able to make non-specific vocalizations, e.g. cooing sounds or laughs aloud. Table 2.11 enlists key linguistic milestones till 5 years of age. Some other important aspects of language development are also discussed in Chapter 3.8.It is re-emphasized that pin-pointing the precise age of appearance for a particular milestone is neither possible nor desirable, due to continuous maturation of these functions.
2.7 DEVELOPMENTAL ASSESSMENT
Developmental assessment is an integral part of every child's health check-up, even if apparently normal. However, it is not necessary to perform exhaustive developmental assessment in every child and the depth of assessment must vary, according to perceived risk of abnormality.
In practice, developmental assessment must be conducted in a step-wise manner, as follows:
a. Informal developmental surveillance of all children during health care visits;
b. Development screening of all children at scheduled intervals;
c. Formal developmental assessment in children with abnormal screening results.
This chapter deals with informal developmental surveillance of all under-five children during regular well-baby clinic/immunization/health-care visits, as well as development screening of all children at scheduled age-intervals, in order to identify children who need in-depth formal assessment, discussed in Ch 3.5.
Development surveillance is a continuous and informal process, not to draw a line between normal and abnormal, but merely to identify high-risk children, who need referral for early developmental screening and/or follow-up. Three important components of informal development surveillance include:
• Ask the parents about age of achieving milestones (developmental history);
• Observe the baby's performance and behavior in the clinic (developmental observation);
• Elicit common age-appropriate milestones (developmental examination).
Developmental history must be obtained by a reliable caretaker, preferably mother, to find out the age of achieving common milestones in different domains, with following principles:
• Record achievement of various milestones in all domains with the age of attainment.
• Compare actual age of attainment with expected age of attainment (Table 2.8 to 2.12) with due consideration for normal variations. In preterm, corrected age should be used to assess adequacy of milestones till the end of infancy.
• Denote the results as developmental age in different fields separately, rather than averaging out to calculate developmental quotient on this informal assessment.
• Record all milestones sequentially, starting from neonatal period irrespective of the age, in cases with suspected neurodevelopmental problems to get an idea about the age from which milestones began to falter.
However in apparently normal children, it is timesaving to begin with last few milestones that the child should have achieved at present chronological age in each domain and go backwards only if the last expected milestone/s have not been achieved.
• In cases with abnormal development, find out if a milestones was never achieved (Delay) or has been lost after the initial achievement (Regression). Regression of milestones is an important clue to neurodegenerative disorders.
Mother and child protection (MCP) card, used by ASHA/Anganwadi workers throughout India, includes a simple tool for monitoring of the child's development. On this card, ASHA/ AWW/other field health workers have to simply mark a tick or cross against the pictorially depicted milestones at different ages (2-3, 4-6, 7-9, 10-12, 18, 24, and 36 months). This chart also provides parenting tips to stimulate development as well as red-flag signs (Table 2.12) to identify children for referral for formal developmental assessment.
Developmental observation involves observing the child's behavior and interaction with others while waiting in the clinic or approached by mother/doctor.
Some important milestones which can be assessed by simple observations are as follows:• Observe an infant from a distance in the waiting room for behavior for personal-social milestones, e.g. social smile (6 weeks), eye-contact (3 months) enjoys mirror image (4 months) hand-regard, (4-6 months) mouthing (5-12 months), searching for a dropped rattle/toy (6 months), attempting to find a partly-hidden toy (8 months) and waving bye-bye (9 months).
• Observe an older child while playing for interaction with others, e.g. enjoying peek-a boo (6 months), plays/ throws ball (12 months), parallel play despite presence of other children (12 months), pointing to a desired toy or object (15 months), mimicry (18 months) showing toys to others (24 months) and sharing toys with others (36 months).
• Observe for gross-motor milestones, e.g. sitting with/ without support, standing with/without support. Crawling/creeping, walking, going up/ down stairs, etc.
• Observe when approached by mother/others, e.g. excitement with limb movement when approached by mother, i.e. recognition of mother (3 months) or crying when approached by the examiner, i.e. stranger anxiety (6 months), etc.
• Listen him/her for linguistic milestones cooing sounds (3 months), laugh aloud (4 months), monosyllables (6 months), bisyllables (9 months) jargon (15 months), two meaningful words (12 months), 8-10 meaningful
| TABLE 2.12: Red-flag signs for development delay on informal developmental surveillance* | |
| At 3 months | At 6 months |
| No social smile | No head control |
| No Startle response to sounds | Cannot sit up with support |
| No eye to eye contact when fed/ cuddled | Does not grasp things within reach |
| Persistent squinting >2 months | Does not track a moving object with head/eyes |
| Persistent limb stiffness/arching of head | Does not vocalize, e.g. ‘ah,..eh,..oo..' |
| Cortical thumb | Unable to raise head in prone position |
| At 9 months | At 12 months |
| No roll-over | No pincer-grasp |
| Cannot sit without support | Does not stretch hands to be picked up |
| Does not turn towards the sound (Out of sight) | Does not respond to own name |
| Does not utter monosyllables, e.g. ‘ma.. pa.. ba'. | Does not search for half-hidden toys |
| Tilts head always to one side, whenlooking at objects | Does not play social games, e.g. Peek-a-boo |
| At 18 months | At 24 months |
| Cannot stand without support | Does not walk steadily while pulling a toy |
| No response to gestures, lives in own world | Does not respond to gestures. e.g. bye-bye |
| Cannot put small objects in a container | Cannot scribble |
| Does not use both hands for everyday activity | Does not point to body parts |
| Does not point finger to a named object, | Does not use two word phrases - 'give milk' |
| Does not say single words, e.g. 'mama, papa' | Does not understand/ follow simple instructions |
| At 36 months | |
| Has troubles climbing up/down stairs | |
| Cannot play "pretend" games | |
| Cannot eat without help | |
| Continuous drooling/ unclear speech | |
| Does not communicate meaningfully, repeats others' speech | |
| Does not speak simple 3-word sentences, e.g. ‘mummy give milk' | |
*Based on Mother and Child protection card (MCP)
TABLE 2.13: Development assessment kit
words (18 months), 2-3 word sentences (24 months) and complete sentences (60 months).
Developmental examination of a young child is tricky and must be performed before the systemic examination, when child is playful and not apprehensive. Information already obtained by developmental history (if reliable) and simple observation needs not be elicited. No rigid pattern should be followed for developmental examination, which may begin informal assessment of vision and hearing, eliciting fine motor and adaptive/cognitive milestones and lastly, gross-motor milestones, which might disturb the child. A short list of items required for developmental assessment is given in Table 2.13.
A tentative protocol of developmental examination of a child is as follows:
• Elicit or check vision by dangling a red-ring attached to a string in the visual field (follows till 45° at 4 weeks
• Red ring on a string (6-7 cm diameter)
• Small bell
• Paper pellets
• Nine red cubes ~1'' each
• Paper and crayon
• Picture-book with thick pages
• Doll and mirror
• Plastic cup with spoon (Small)
• Shape-board with common shapes
and 180° at 8 weeks), and following the mother's movement (2 months)
• Elicit or check hearing using a small bell for turning the head towards sound (6 weeks) or response to the name-call (12 months).

Fig. 2.11: Pincer grasp.
• Elicit fine motor milestones in an infant by:
- Offer a red ring to observe for voluntary grasp (4 months), bidextrous approach with both hands (5 months) unidextrous approach with one hand (6 months), transfer of object (6 months) and release of object on request (10 months).
- Offer a paper pellet to observe for the maturity of pincer grasp (9-10 months) (Fig. 2.11).
• Elicit fine motor milestones in an older child by:
- Offer a cube to see stacking, e.g. tower of 2 cubes (12 months), 3 cubes (18 months), 6 cubes (24 months) 8 cubes (30 months), 9-10 cubes (36 months) and making a bridge (48 months).
- Offer a paper and crayon to see for scribbling (18 months) and imitating vertical/horizontal lines (24 months), circle (36 months), cross (48 months) and triangle (60 months).
- Offer a bright picture-book with thick pages to see whether he looks at pictures (12 months), turns 2-3 pages at a time (15 months) or turns single page at a time (18 months)
- Check/ask mother for the ability to feed with a spoon (15 months) or cup (18 months), pulling out of shoes (18 months), attempts to undress (24 months), brush (30 months) and helps to dress (36 months).
• Elicit adaptive/cognitive milestones by:
- Ask him/her to point body parts (18-24 months), name and gender (36 months), right/left side discrimination (48 months), to sing a nursery rhyme (48 months) or tell a story (48 months) and count up to 10 coins (60 months).
- Offer a doll and ask to point 4-6 parts of the doll (24 months).
• Elicit gross-motor milestones by history as well as:
- Assess the neck-control in infants popular development screening test in India, based on Baroda norms, using 17 test milestones (Fig. 2.13). This test provides the upper (97th percentile) age-limits for development of test milestones, beyond which a baby may be considered as developmentally retarded. It is designed for easy to use by community level health worker for mass screening and takes around 5 minutes to complete.
Other commonly used development screening tests include Age and stage questionnaire (ASQ-3)- a parent-completed questionnaire, Rashtriya Bal swasthya Karyakram (RBSK) screening tool, and Goodenough- Harris Draw-a-man test, etc.
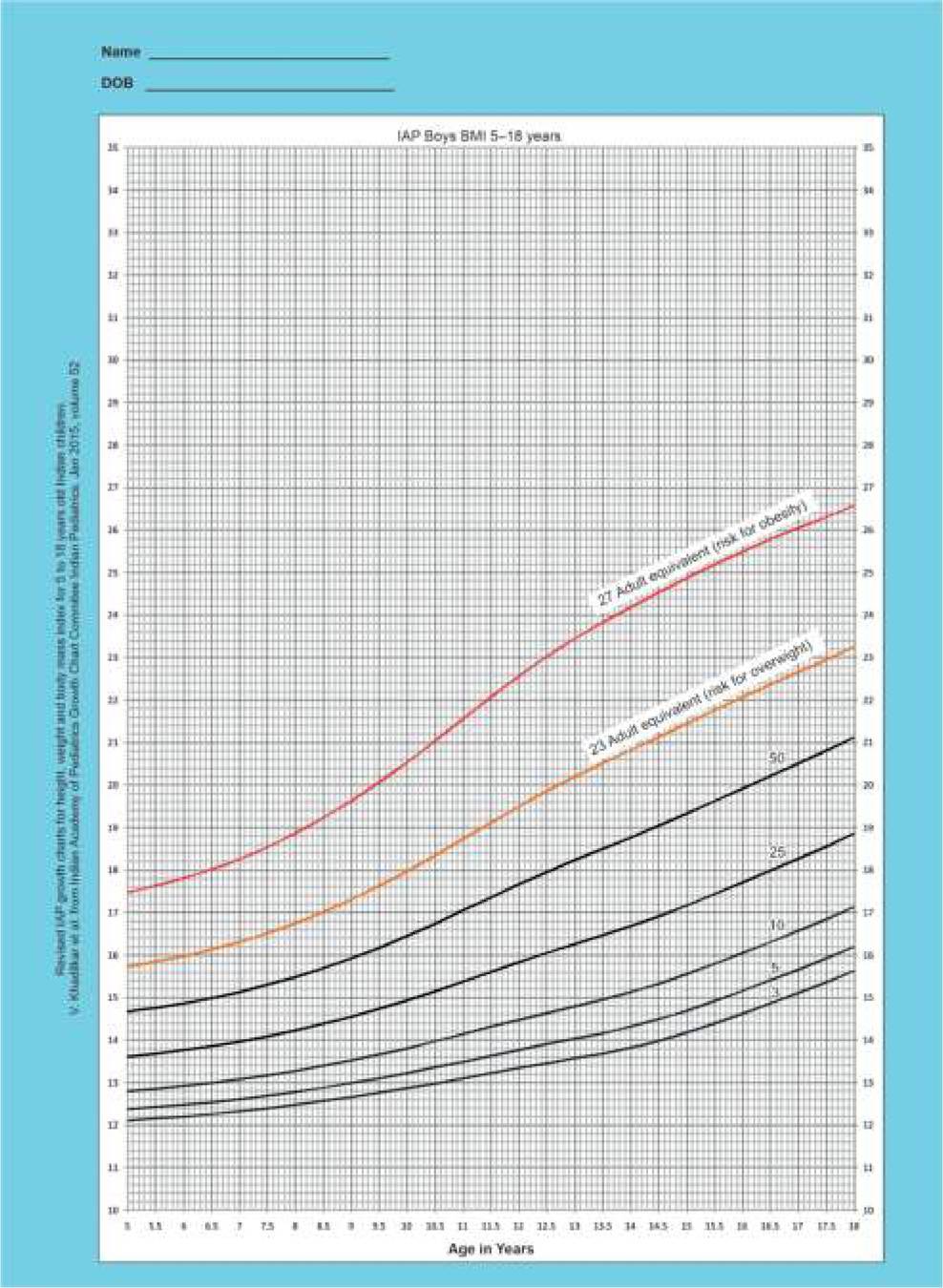
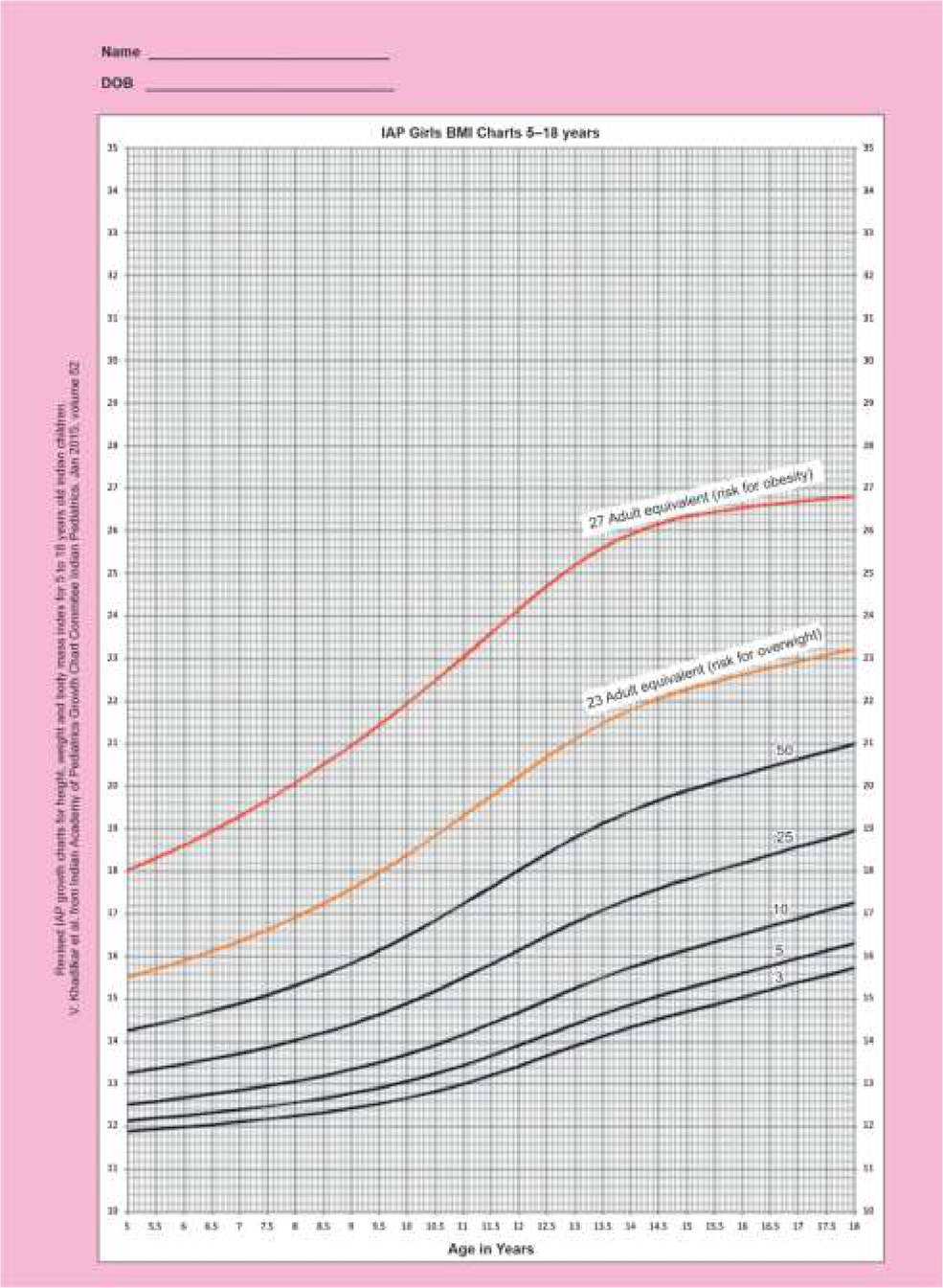
1. Khadilkar et al. Revised IAP Growth Charts for Height, Weight and Body Mass Index for 5- to 18-year-old Indian Children, Indian Pediatrics. 2015;52:47-55.
2. WHO Multicentre Growth Reference Study Group: WHO Child Growth Standards: Length/ height-for-age, weight- for age,weight-for-length, weight-for-height and body mass index-for-age: Methods and development. Geneva, World Health Organization, 2006. Available at: http:/ / www. who.int/nutrition/publications/child growth standards_ technical_report_1 / en/.
3. Nair MKC. Development and Validation of Trivandrum Development Screening Chart for Children Aged 0-6 years, Indian J Pediatr. 2013;(80):(S2).
4. Nair MK, et al. Trivandrum Developmental Screening Chart. Indian Pediatr. 1991;28(8):869-72.
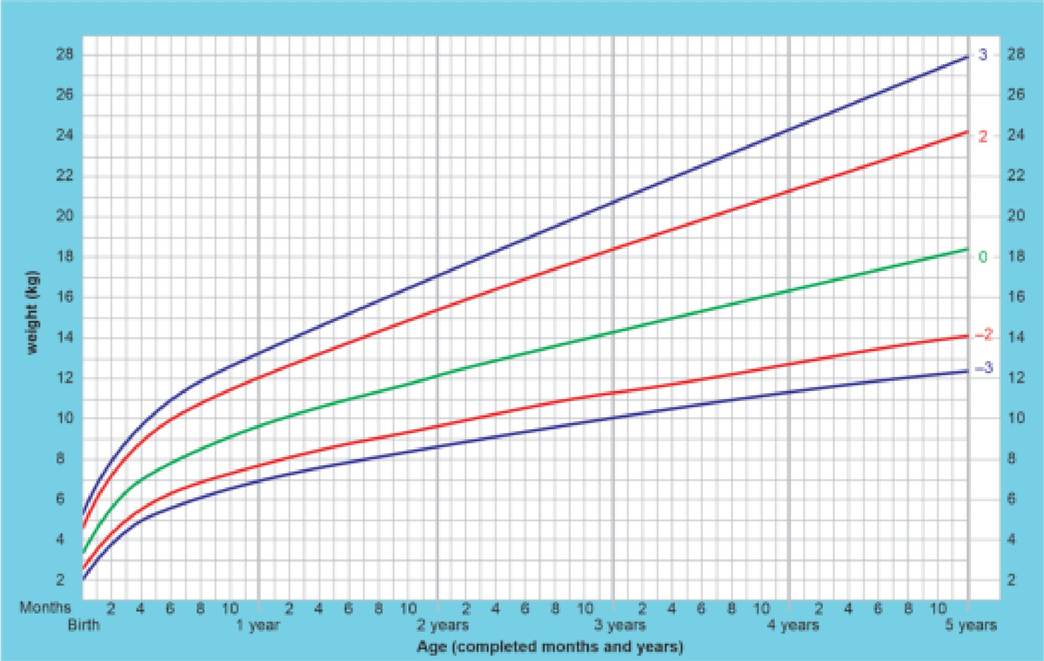
Appendix 2.1: WHO child growth standards (Z-score): Weιght-for-age: Birth to 5 years (boys).
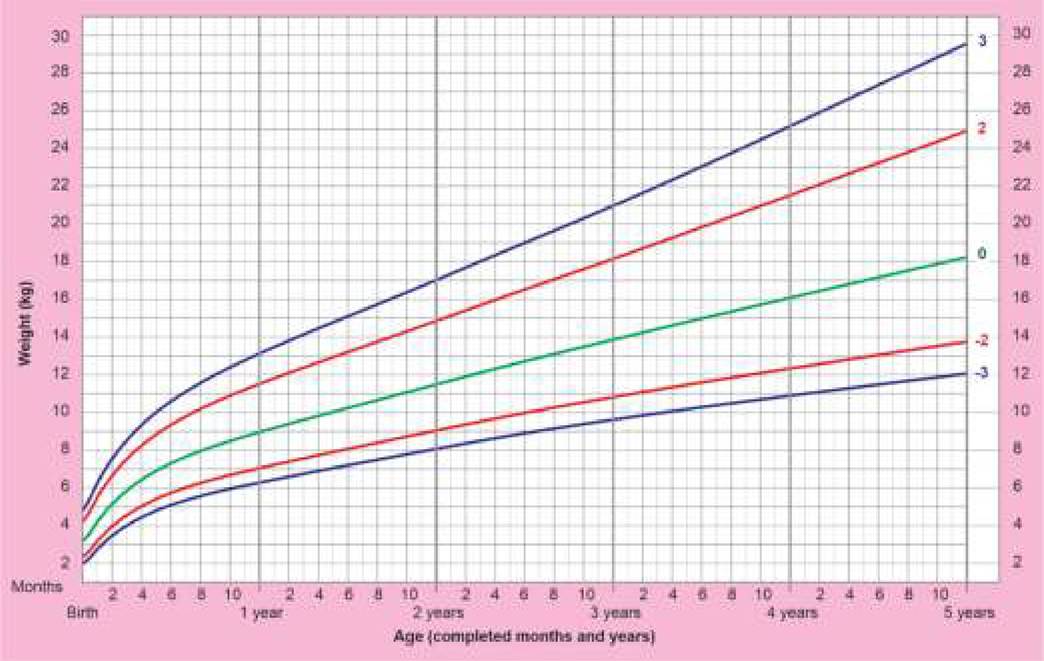
Appendix 2.2: WHO child growth standards (Z-score): Weight-for-age: Birth to 5 years (girls)
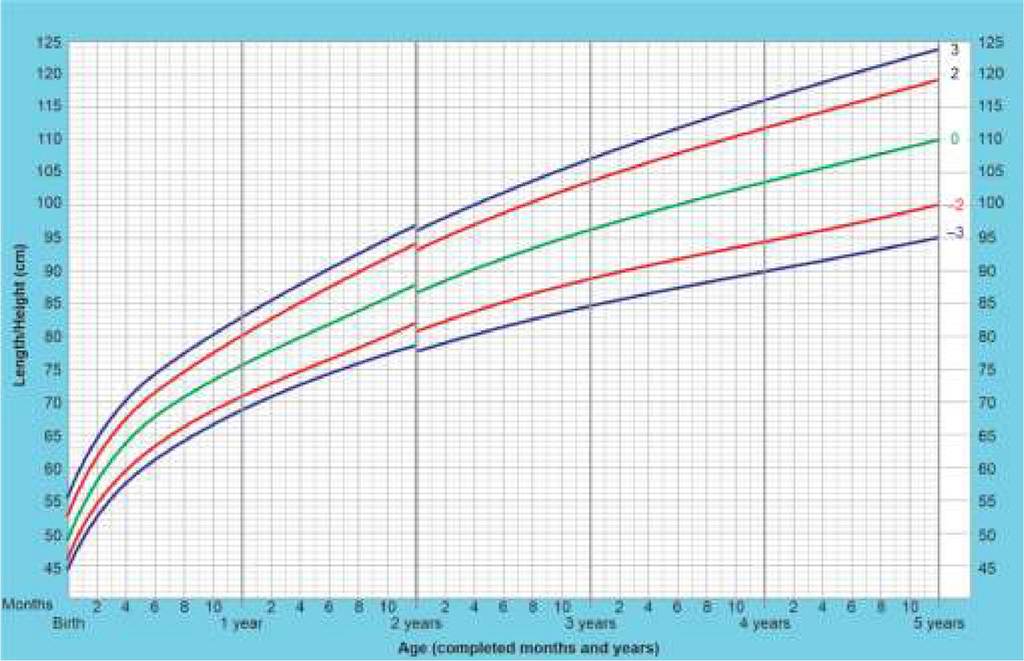
Appendix 2.3: WHO child growth standards (Z-score): Length/Height-for-age: Birth to 5 years (boys).
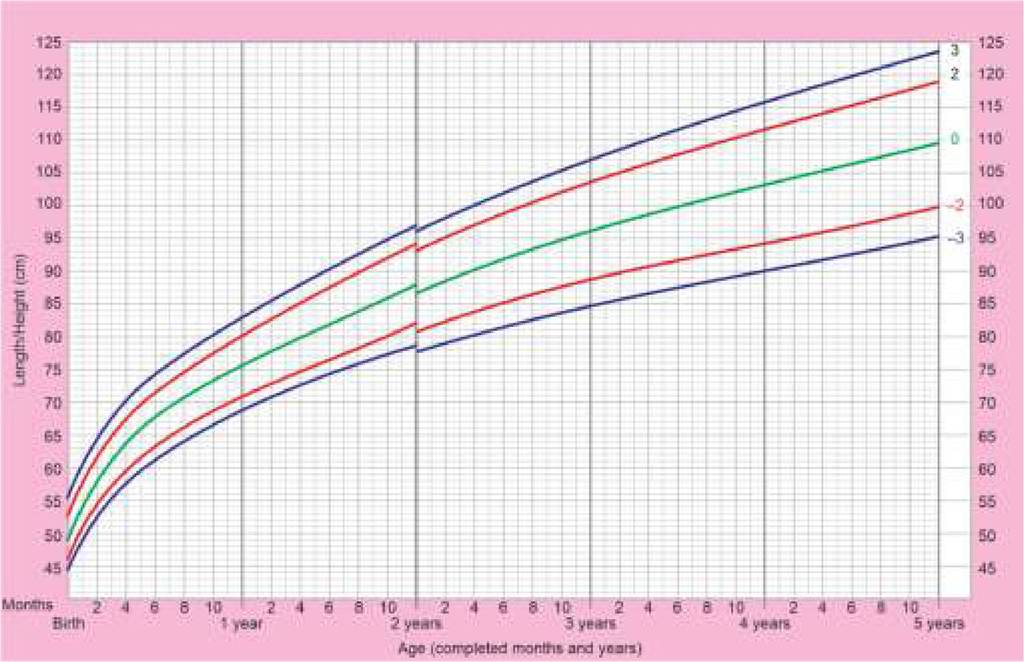
Appendix 2.4: WHO child growth standards (Z-score): Length/Height-for-age: Birth to 5 years (girls).
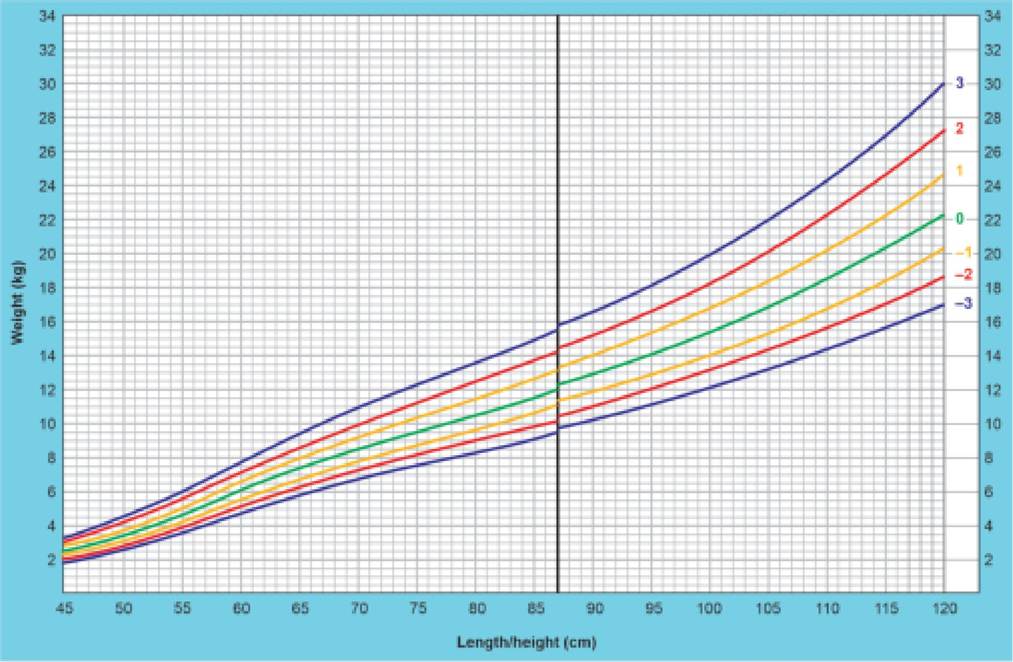
Appendix 2.5: WHO child growth standards (Z-score): Weight-for-length/height: Birth to 5 years (boys).
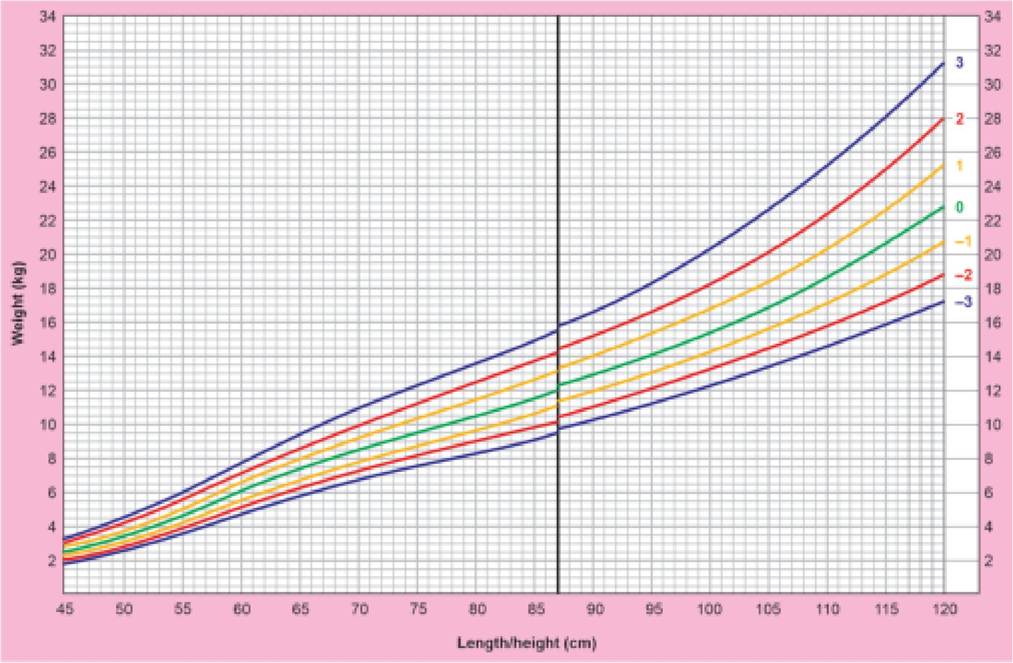
Appendix 2.6: WHO child growth standards (Z-score): Weight-for-length/height: Birth to 5 years (girls).
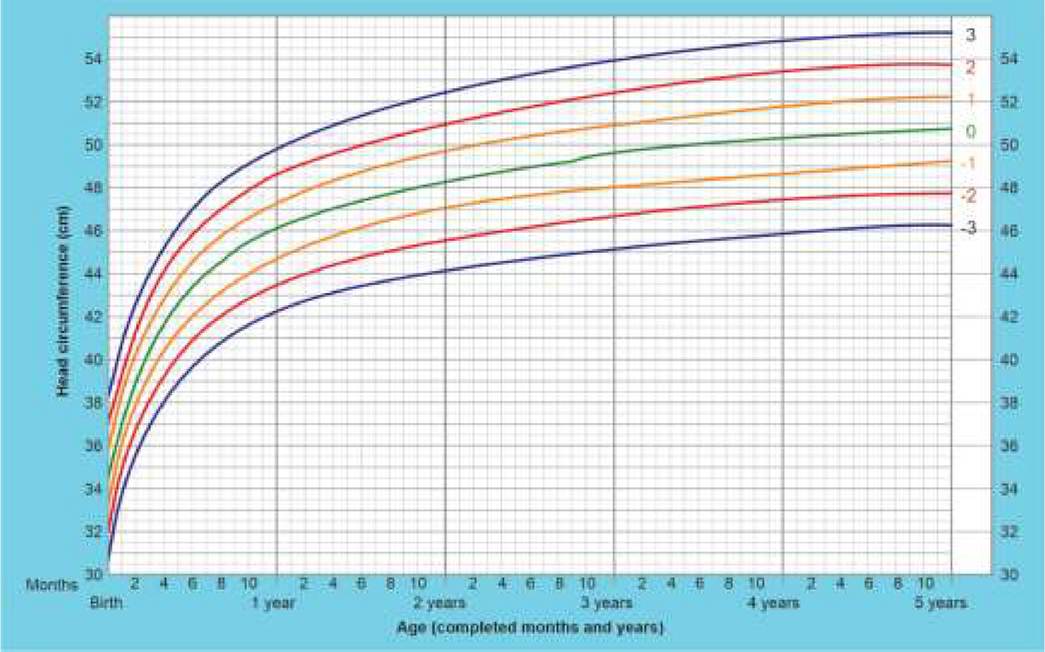
Appendix 2.7: WHO child growth standards (Z-score): Head circumference-for-age: Birth to 5 years (Boys).
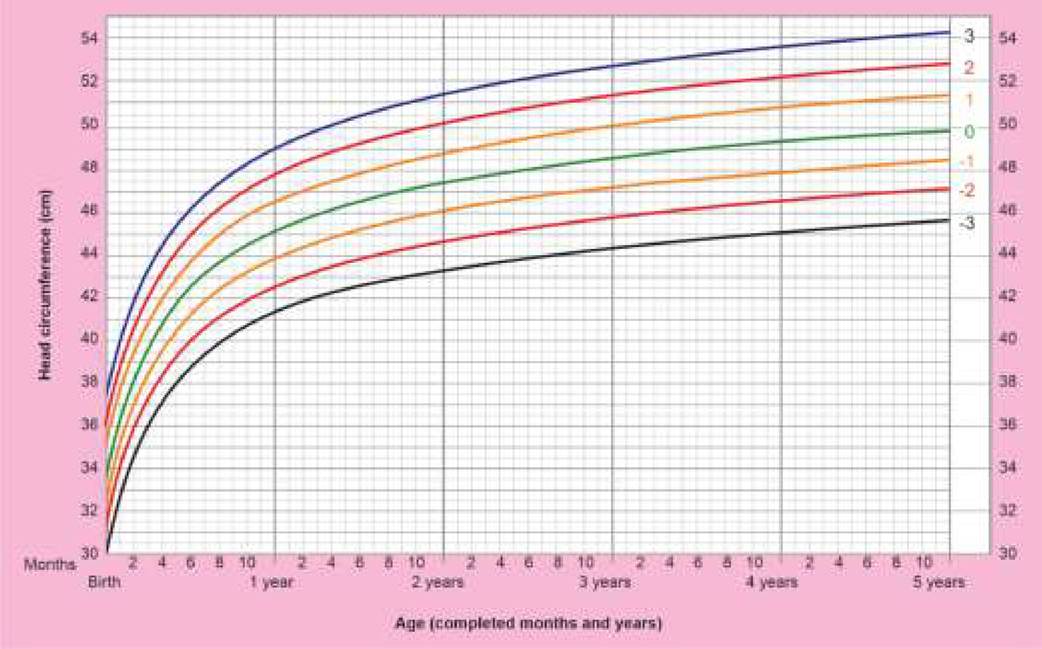
Appendix 2.8: WHO child growth standards (Z-score): Head circumference-for-age: Birth to 5 years (Girls).
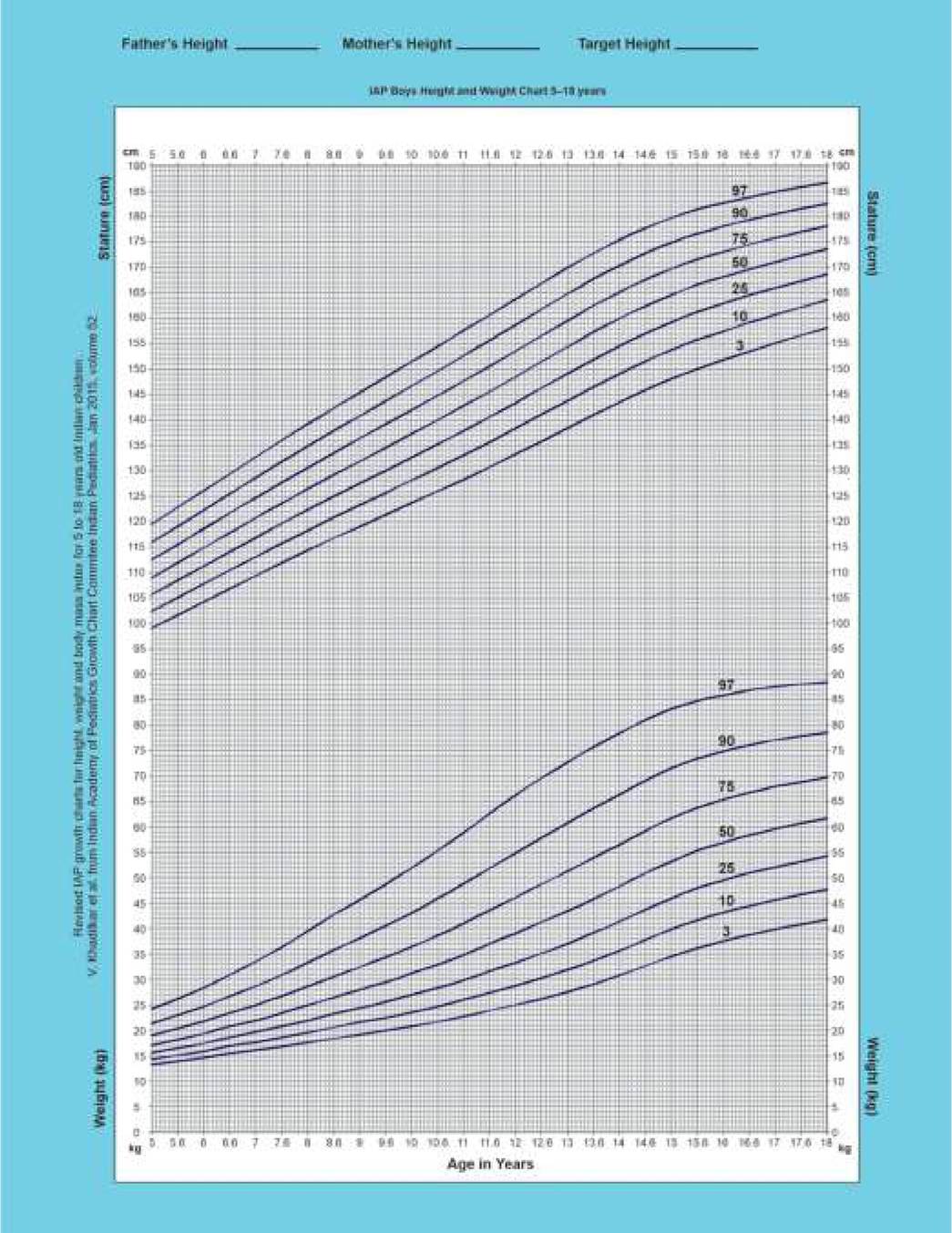
Appendix 2.9: IAP growth charts (percentiles): Weight and Height: 5-18 years (Boys).
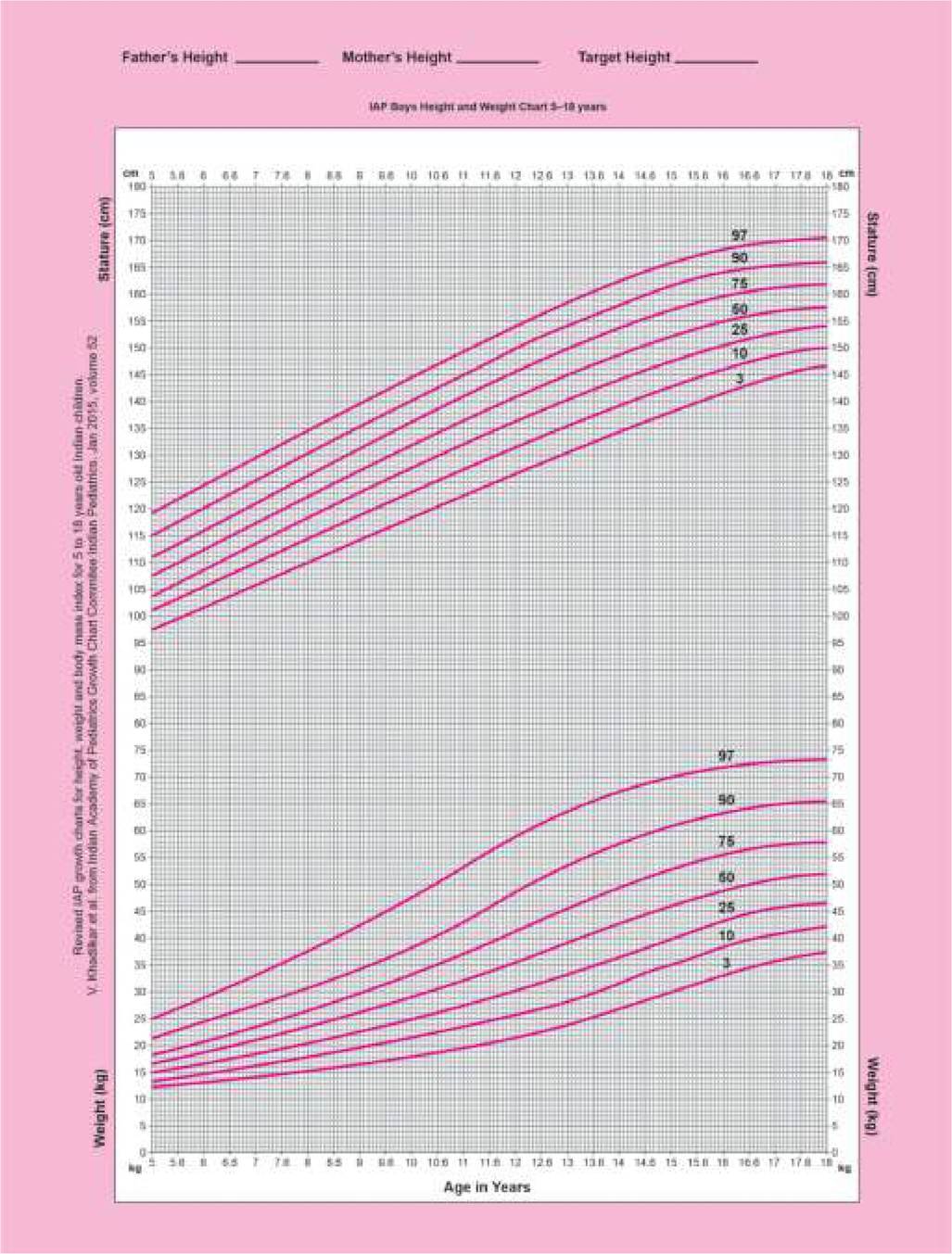
Appendix 2.10: IAP growth charts (percentiles): Weight and height: 5-18 years (Girls).
More on the topic DEVELOPMENTAL MILESTONES:
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- I ENDOMETRIOSIS ^595