Neuromuscular Junction Disorders
Infantile Botulism
Infantile botulism primarily occurs in infants 2-6 months of age. Clinical findings include diffuse weakness, hypotonia, weak cry, poor feeding, constipation, and occasionally respiratory distress.
The onset is fairly rapid. Electrophysiologic studies may show a reduced CMAP amplitude, preserved motor conduction velocities and SNAPs, and abnormal repetitive nerve stimulation findings at high rates of stimulation (Fig. 7.11). One study demonstrated an incremental response to repetitive nerve stimulation at rates of 20-50 Hz in 92% of infants with infantile botulism (22). The mean increment was 73%, with a range of 23% to 313%. With the lower-frequency stimulation (2-5 Hz), variable changes occurred, but the majority of infants showed decremental responses. A recent study demonstrated that the isolation of Clostridium botulinum from stool obtained by enema effluent was actually more sensitive for the diagnosis of infant botulism than electrodiagnostic studies (102).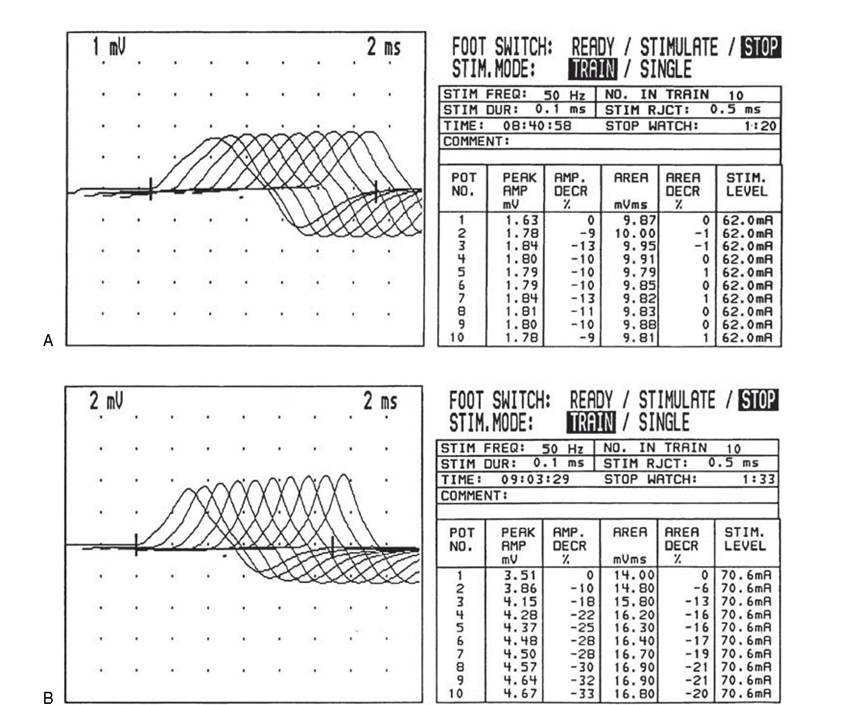
Figure 7.11 High frequency repetitive nerve stimulation in a 7-week-old infant with marked progressive weakness, respiratory failure, and botulism. (A) Several days into the course, the repetitive stimulation study of the ulnar nerve at 50 Hz is normal; however, the compound muscle action potential amplitude is severely reduced (1.63 mV). (B) Twelve days later, the infant is slightly improved clinically. A repeat study of the ulnar nerve at 50 Hz is diagnostic of infantile botulism with a 33% increment obtained between first and tenth stimuli. Clostridium botulinum was isolated from the stool.
EMG in infants with botulism demonstrates abnormal spontaneous rest activity with fibrillation potentials and positive sharp waves and short-duration, low- amplitude MUAPs (22).
Transient Neonatal Autoimmune Myasthenia Gravis
This disorder is caused by passage of antibodies from myasthenic mothers to their fetuses. Infants often
present with hypotonia and respiratory distress. The diagnosis may be made by repetitive nerve stimulation studies. Given that normal infants exhibit less neuromuscular reserve than older children or adults, repetitive stimulation studies in this clinical setting utilizes rates of 2-5 Hz almost exclusively. A decrement of greater than 8% to 10% between the first and fifth CMAP in the train is considered positive for myasthenia. The combination of repetitive motor nerve stimulation and edrophonium or neostigmine testing may improve the accuracy of the diagnosis (103). If a decremental response is obtained, the repetitive nerve stimulation may be repeated at 30-120 seconds after administration of edrophonium utilizing a stimulation rate of 2-5 Hz. Near complete repair of the decremental response may be evident in the myasthenic infant (Fig. 7.12). Serologic antibody testing may be helpful if the mother has documented antibodies. Transient neonatal myasthenia gravis is self-limited, with a reported duration of 5-47 days, with a mean duration of 18 days (104).
B
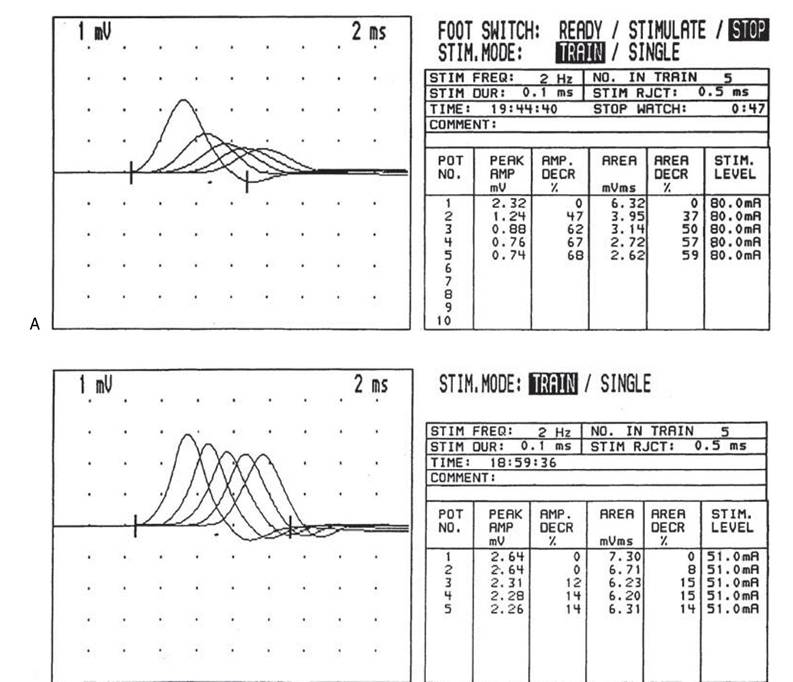
Figure 7.12 Low-frequency repetitive nerve stimulation study of the ulnar nerve in a 2-week-old infant with respiratory failure secondary to congenital myasthenia. (A) At baseline, a 68% decrement in amplitude and a 59% decrement in area is present between first and fifth stimuli with a stimulation frequency of 2 Hz. (B) Twenty minutes after intravenous neostigmine is given, the initial compound muscle action potential has improved from 2.32 to 2.64 mV and the decrement has improved to 14%. The infant was treated with Mestinon and later extubated.
Toxic Neuromuscular Junction Disorders
Medications can interfere with neuromuscular transmission by inhibiting the release of acetylcholine, impairing the function of acetylcholinesterase (AChE), or binding directly to the acetylcholine receptor.
Two drugs that may produce clinically significant weakness in normal children are magnesium and organophosphates (105,106).Congenital Myasthenic Syndromes
Numerous presynaptic and postsynaptic congenital myasthenic subtypes exist, which are described in the pediatric neuromuscular disease chapter. These disorders often show decremental responses at high rates of stimulation, whether they are pre- or postsyn- aptic. Typically, the decremental responses are greater at higher rates of stimulation. Standard repetitive nerve stimulation studies do not adequately distinguish pre- synaptic from postsynaptic subtypes, but they do help diagnostically (Fig. 7.13).
Based on clinical findings, repetitive nerve stimulation studies, and/or stimulated single-fiber EMG, a strong clinical suspicion of a neuromuscular junction disorder, such as a congenital myasthenic syndrome, might warrant further elucidation of the specific subtype of presynaptic or postsynaptic abnormality with application of a motor point biopsy. Ultra-structural evaluation of the neuromuscular junction (NMJ) with electron microscopy is usually performed on a biopsy of the deltoid or biceps, including the muscle region containing the-NMJ (the “motor point”). For in vitro electrophysiologic and immunocytic chemical studies of the neuromuscle junction, a short muscle is usually removed from origin to insertion along with its motor branch and NMJ. Muscles obtained have included the anconeus muscle near the elbow, the external intercostal muscle, and the fifth or sixth intercostal space near the anterior axillary line or the peroneus tertius muscle in the lower extremity. Often, patients undergo simultaneous biopsy of the deltoid (for EM) and motor point biopsy of the anconeus or intercostal muscle (for in vitro electrophysiologic studies). The in vitro electrophysiologic studies often allow specific delineation of the congenital myasthenic syndrome into one of the numerous specific subtypes.
In recent years, many of the subtypes have been mapped to specific gene loci, and increasingly, molecular genetic studies are being used for diagnostic purposes.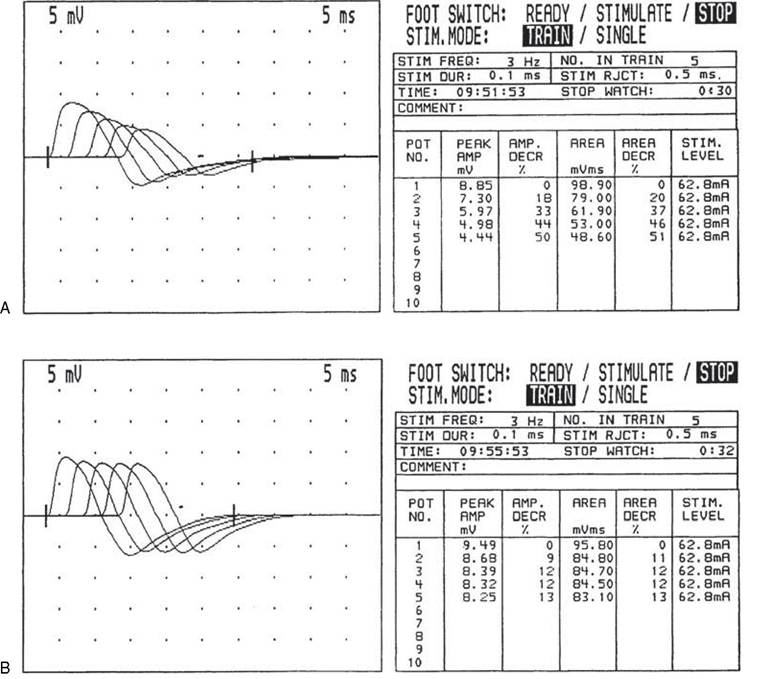
Figure 7.13 Low-frequency repetitive nerve stimulation study of the axillary nerve in a 12-year-old child with presynaptic congenital myasthenia. The active electrode is placed over the deltoid with stimulation at Erb's point using a block stimulator. (A) A 50% amplitude decrement is obtained between the first and fifth stimuli with 3 Hz stimulation frequency. (B) After a 30-second isometric contraction of the deltoid, the amplitude decrement has improved to 13%. The child was later confirmed to have a presynaptic congenital myasthenia by motor point biopsy of the anconeus muscle.
Myasthenia Gravis
Myasthenia gravis presents in adolescents more frequently than younger children. Muscle weakness typically increases with exertion but improves with rest and anticholinesterase medication. The disorder is an autoimmune etiology due to circulating antibodies that bind to the postsynaptic membrane. While elevated acetylcholine receptor antibody levels may be diagnostic, a significant percentage of cases with autoimmune myasthenia gravis may have nondetectable circulating antibodies. Electrophysiologic studies demonstrate abnormal decremental responses at low rates of stimulation (2-3 Hz). The limb is well immobilized. A supramaximal train of three to five stimuli is applied. Typically, patients exhibit a smooth, reproducible decrement of the evoked synapse of greater than 8% to 10%. The defect in neuromuscular junction transmission can be enhanced by exercise, which results in postactivation facilitation. Often, there is an increased decremental response obtained two to four minutes after exercise with low rates of stimulation (2-3 Hz). This is due to postactivation exhaustion (21). Proximal muscles may show increased sensitivity versus distal muscles.
Children with ocular myasthenia frequently exhibit normal responses with distal repetitive nerve stimulation studies, and sensitivity of the repetitive nerve stimulation (RNS) study is enhanced by use of a more proximal shoulder girdle muscle (eg, axillary or spinal accessory nerve) or by study of the facial nerve. Combining the diagnostic yield, patient comfort, and technical ease, the choice of muscle for RNS should be ulnar to the abductor digiti minimi, followed by spinal accessory to the trapezius for patients with predominant limb weakness; facial nerve to the nasalis and spinal accessory to the trapezius in oculobulbar; and facial to the nasalis in ocular myasthenia (107).Lambert-Eaton Syndrome
This presynaptic neuromuscular junction disorder usually found in adults with small cell carcinoma of the bronchus has been described in children. Approximately 5% of all cases occur in children. The amplitude of the single evoked CMAP is low. With low rates of repetitive nerve stimulation, a decremental response is often obtained. After exercise or tetanic contractions, there is facilitation of the potentials by as much as 100% to 200%.
More on the topic Neuromuscular Junction Disorders:
- TECHNICAL FACTORS OF NEEDLE ELECTROMYOGRAPHY
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- Peripheral Vascular Disease
- Motor Speech Disorders
- CHAPTER 41 HARMFUL ALGAL BLOOMS INCLUDING Cyanobacterial toxicosis
- Chapter 8 Maternal medicine and infections