Speech and Language Disorders
Speech and language disorders in children can be conceptualized as falling into two categories: developmental and acquired. Within the category of developmental, we can also distinguish between developmental delay and developmental disorder.
Developmental language delay refers to delay in the acquisition and development of age-appropriate language skills, typically across all domains. This can be due to medical or psychosocial factors. A developmental language disorder is characterized by atypical development of language skills in one or more domains, often with aberrant or interrupted development. As noted previously, there are specific milestones associated with each age as a child acquires speech and language skills. It is important to monitor development and watch for any signs that might indicate delay or disorder. The following is a list of danger signals of communication problems by age (24):■ By 6 months
? Does not respond to the sound of others talking
? Does not turn toward speaker out of view
? Makes only crying sounds
? Does not maintain eye contact with caregiver
■ By 12 months
? Does not babble
? Does not discontinue activity when told “no”
? Does not follow gestural commands, such as “want up” or “give me”
■ By 24 months
? Does not say a meaningful word
? Does not refer to self by name
? Does not follow simple directions
? Does not talk at all at 2 years
? Vocabulary does not seem to increase
? Does not have any consonant sounds
? Does not answer simple yes/no questions
■ By 36 months
? Does not say whole name
? Does not seem to understand “what” and “where” questions
? Uses jargon a great deal
?Answers your question by repeating the question
?Continues to echo statements made by others
?Does not use two- to three-word utterances
? Points to desired objects rather than naming them
?Does not name any objects in pictures
?Leaves off the beginning consonants of words
?Cannot be understood even by parents
?Does not respond when you call name
An acquired language disorder is characterized by language deficits in one or more domains secondary to neurologic insult.
This can and often does result in aberrant development due to interruption in the normal course of language acquisition. When considering a speech and language disorder resulting from a congenital disorder such as cleft palate or Pierre Robin Sequence, classification becomes more difficult. The disorder does not fit the definition of a developmental delay, in that the development is atypical secondary to structural deficits. The disorder is also not considered acquired, as the structural deficit leading to the disorder occurred at birth, before the child began to develop language.Some common causes of loss or deterioration of language in childhood include head injury, unilateral cerebrovascular lesions, cerebral infections, brain tumors, seizure disorders, and cerebral anoxia. These disorders can result in acquired childhood aphasia (25). Acquired childhood aphasia is defined as a language disorder secondary to cerebral dysfunction in childhood appearing or occurring after a period of normal language development. The cerebral dysfunction may be the result of a focal lesion of one of the cerebral hemispheres, a diffuse lesion of the central nervous system (CNS) above the level of the brainstem (TBI, cerebral infection), a diffuse lesion related to convulsive activity, or unknown etiology Landau-Kleffner syndrome (LKS). In general, pediatric-acquired aphasia tends to be characterized by nonfluency, with primary deficits in verbal expression, with parallel deficits in written expression and auditory comprehension relatively intact.
Pediatric traumatic brain injury (TBI) can result in more generalized dysfunction secondary to diffuse axonal injury caused by acceleration forces. Although such damage can have a significant impact on a variety of brain functions, the damage, sustained at the axonal or cellular level, is often not detected by brain scans. The definition of TBI, written by the federal Division of Special Education as part of Public Law 101-476 (Individuals with Disabilities Act, or IDEA), was published in 1992 as the guideline for state departments of education to use in determining how to provide educational services to these children.
It reads as follows (26):“Traumatic Brain Injury” means an acquired injury to the brain caused by an external force, resulting in total or partial functional disability or psychosocial impairment, or both, that adversely affects a child's educational performance. The term applies to open or closed head injuries resulting in impairments in one or more areas, such as cognition; language; memory; attention; reasoning; abstract thinking; judgment; problem-solving; sensory, perceptual, and motor abilities; psychosocial behavior; physical functions; information processing; and speech. The term does not apply to brain injuries that are congenital or degenerative, or brain injuries induced by birth trauma (Federal Register, Vol. 57, no. 189).
Other common acquired disorders that can affect speech and language development include high-level spinal cord injury (SCI) and hearing loss. High-level SCI often affects some of the cranial nerves that are responsible for movement of the articulators necessary for speech production (Table 4.9) (27).
With regard to hearing loss, if children acquire hearing loss during the period of speech and language acquisition, they are at significantly increased risk for communication disorders.
There are many congenital disorders that can have an impact on speech and language development. Some of the most common include cerebral palsy, cleft palate/ craniofacial anomalies, hearing loss, and autism.
Cerebral palsy (CP) is defined as a group of disorders of development of movement and posture, causing
4.9
Cranial Nerves Involved in Speech and Swallowing
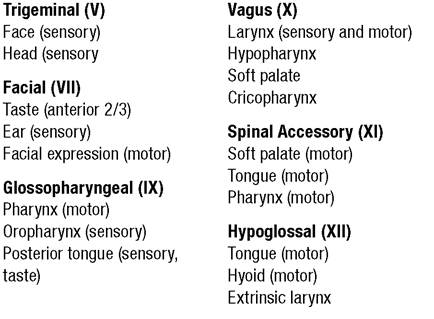
Soutce: From Ref. 17.
activity limitation, that are attributed to nonprogressive disturbances that occurred in the developing fetal or infant brain. The motor disorders of cerebral palsy are often accompanied by disturbances of sensation, cognition, communication, perception, and/or behavior, and/or by a seizure disorder (28).
CP may significantly affect tone, which in turn affects ability to use those muscles appropriately to perform the necessary movements for speech production. As noted previously, speech production is a complex motor act requiring precise coordination of muscle groups, including respiratory, phonatory, and articulatory systems. When abnormal tone is present, either hyper- or hypotonicity, this interferes with coordination both within and across these systems, resulting in motor speech dysfunction, specifically dysarthria. The most common types of dysarthria associated with cerebral palsy include spastic, ataxic, and hyperkinetic (see Table 4.4).Children with spastic cerebral palsy are more likely to exhibit imprecise articulatory contacts, strained/ strangled voice quality, and reduced rate. Children with ataxic cerebral palsy typically exhibit irregular articulatory breakdown, harsh vocal quality, incoordination of the respiratory stream, and reduced rate. Children with athetoid cerebral palsy exhibit imprecise articulatory contacts, harsh vocal quality, incoordination of the respiratory stream, and transient increased rate.
Treatments for hypertonicity, such as intrathecal baclofen, selective dorsal rhizotomy, and various oral medications, may have an influence on speech and communication. These treatments frequently result in improvements, but in some cases may worsen impairment (29,30). Authors of this chapter report clinical observations of improved breath support for voice production and improved articulation with intrathecal baclofen therapy.
The presence of combined motor and cognitive impairments makes assessment of communication difficult. There is great need for a standard classification system along the lines of the Gross Motor Classification System (GMFCS) (31) and Manual Ability Classification System (MACS) (32). Van Tubbergen and Albright developed a five-level ordinal scale to classify levels of expressive language: the ExPRS (Expressive Production Rating Scale) (33).
Like the GMFCS and MACS, the ExPRS provides a descriptive classification system for expressive communication, including the use of alternative or augmentative communication (Table 4.10). Further investigation on the reliability and validity of the ExPRS is needed to enhance its potential in transdisciplinary settings.Cleft palate and other craniofacial anomalies involving the oral cavity most typically affect a child’s articulation as well as resonance. A cleft palate
4 Expressive Production Rating
Scale (ExPRS)
Child's communication: Mark the item that best describes your child's typical abilities:
___ Speaks in a generally age-appropriate way; minor limitations, if any.
___ Speaks with some difficulty; speech may be slow or somewhat difficult to understand by a new listener.
___ Speaks with significant difficulty; speech is slow or quite difficult to understand by a new listener.
___ Communicates independently with limitations; individual uses adapted techniques such as signing or an augmentative communication device.
___ Communication is severely limited even with the use of augmentative technology.
Source: From Ref. 33.
prevents ability to valve the airstream at the level of the palate, making it impossible to close off the nasal passage during speech. This results in hypernasal speech. A number of other syndromes, such as velo- cardiofacial syndrome (also known as DiGeorge syndrome), affect the ability of the soft palate to function properly, resulting in velopharyngeal incompetence, in turn resulting in impaired resonance (hypernasality).
Congenital hearing loss can have a significant impact on the development of speech and language, depending on the severity of the loss. Speech and language disorders resulting from hearing loss may affect multiple areas of communication, including language comprehension, syntax, vocabulary, and articulation. The nature and extent of communication disorders in children with hearing impairment are influenced by type and degree of hearing loss, causative factors, age at onset, cognitive status, and environment.
Early identification and intervention are critical to maximize potential for developing communication skills in children with hearing loss. Intervention can include provision of hearing aids, environmental modifications (eg, FM or frequency modulation systems in the classroom), aural habilitation/rehabilitation, sign language, total communication (combination of auditory- vocal language, signs, gesture, and speech reading), or surgical implant (cochlear implant).Autism is one of the fastest-growing childhood disorders in our nation today. The current estimate is that 1 out of every 150 children is diagnosed with autism. The spectrum of autism disorders is broad, including pervasive developmental delay—not otherwise specified, autism, Asperger’s syndrome, Rett’s disorder, and childhood disintegrative disorder. Within the DSM IV criteria (34), the current classification system used to diagnose children with an autism spectrum disorder,
deficits in some aspect of communication are present in all the disorders; in fact, 10 of the 15 characteristics listed to characterize autism are directly related to communication.
Organized according to presence/absence of communication, they are as follows:
■ Five criteria relating to language:
? delay in, or total lack of, the development of spoken language (not accompanied by an attempt to compensate through alternative modes of communication such as gesture or mime)
? in individuals with adequate speech, marked impairment in the ability to initiate or sustain a conversation with others
? stereotyped and repetitive use of language or idiosyncratic language
? lack of varied spontaneous make-believe play or social imitative play appropriate to developmental level
? delays or abnormal functioning in language as used in social communication, with onset prior to age 3 years
■ Five criteria relating to social interaction:
? marked impairment in the use of multiple nonverbal behaviors, such as eye-to-eye gaze, facial expression, body postures, and gestures, to regulate social interaction
? failure to develop peer relationships appropriate to developmental level
? a lack of spontaneous seeking to share enjoyment, interests, or achievements with other people (eg, by a lack of showing, bringing, or pointing out objects of interest)
? lack of social or emotional reciprocity
? delays or abnormal functioning in social interaction, with onset prior to age 3 years
■ Five criteria relating to patterns of behavior, interests, and activities:
? encompassing preoccupation with one or more stereotyped and restricted pattern of interest that is abnormal either in intensity or focus
? apparently inflexible adherence to specific, nonfunctional routines or rituals
? stereotyped and repetitive motor mannerisms (eg, hand or finger flapping or twisting, or complex whole body movements)
? persistent preoccupation with parts of objects
? delays or abnormal functioning in symbolic or imaginative play, with onset prior to age 3 years
In addition to delayed development of receptive and expressive language, the hallmark characteristic for children with autism is a deficit in the pragmatics, or use, of language. These children typically have impaired reciprocal social interaction and, in more severe cases, lack intent to communicate.
More on the topic Speech and Language Disorders:
- SPEECH AND LANGUAGE DISORDERS
- SPEECH AND LANGUAGE DEVELOPMENT AND DISORDERS
- Within the field of communication sciences and disorders, we think of communication as broadly comprised of speech and language.
- Speech and Language Acquisition
- Motor Speech Disorders
- Contribution of Articulatory/Resonatory Dysfunction to Speech Disorders
- Contribution of Respiratory Dysfunction to Speech Disorders
- Contribution of Phonatory Dysfunction to Speech Disorders
- Language Deveionment In Disorders of Communication and Orai Motor Function
- Track Three: Government Speech and Subsidies of Speech
- Russian Language versus Ukrainian Language
- Constitutio Medievalis: The Politics of Language and the Language of Politics in the 1710 Constitution
- Speech Therapy
- Speech-Generating Devices
- P Keerthi Kundana, Mona Gajre, Alpana Kondekar, Mukesh AgrawalNeurological disorders account for ~15-20% of hospitalizations, which may be divided into three major categories: (a) central nervous system disorders, involving brain and spinal cord, (b) neuromuscular disorders involving peripheral nerves and muscles, and rare disorders of autonomic nervous system.
- God’s Speech
- Speech Components