Bulla Infusion and Topical Therapy
Removal of the mucus and pus within the tympanic bulla during the treatment of otitis media allows topical medications to penetrate in and around the thickened, folded mucoperiosteum.
The use of aqueous formulations of non-ototoxic topical antibiotics, steroids, or antifungals placed on the mucoperiosteum hastens recovery from otitis media. Topical levels of these drugs may be many times the level that can be achieved using parenteral therapy, even when there is severe hyperemia of the mucoperiosteum. Antibiotic concentrations are high in inflamed tissues because the increased blood flow allows increased serum levels of antibiotic to perfuse the inflamed tissue. But even these levels may not achieve the MIC necessary to kill the bacterial target.Infusing drugs into the bulla is an effective method of providing long-acting high- concentration effects. The tympanic bulla in the dog and cat is a deep, blind pouch. When the bulla is filled with antibiotic, the fluid cannot escape easily. Because of the small diameter of the swollen auditory tube and its location high on the medial wall of the bulla, drainage from the auditory tube is unlikely. Depending on the amount of eardrum present, fluid has to traverse a jut in the petrous temporal bone, which forms the floor of the horizontal ear canal and extends into the bulla. Fluid escape from the bulla is difficult and requires severe changes in head position to allow drainage through the eardrum. If a myringotomy incision was made, it would be difficult for fluid to escape the middle ear because of the surface tension across the incision. There may be a small movement of the infused antibiotic solution into the external ear canal, which actually may be beneficial, but the majority of the topical antibiotic solution can remain within the bulla for several days after infusion.
The antibiotic, antifungal, or corticosteroid solution is infused into the bulla through a small catheter placed into the bulla until the fluid overflows into the external ear canal.
During the first bulla infusion, less than 1 cc of solution can be infused into the inflamed bulla. The entire procedure of flushing, suctioning, and bulla infusion should be repeated weekly during therapy. With each successive treatment, the mucoperios- teum should retract slightly, increasing the volume of fluid the bulla can accommodate.With successive recheck visits, the eardrum and the horizontal canal should be examined for fluid, mucus, and pus. If there is fluid within the bulla, it should be flushed out and the bulla suctioned to prepare it for reinfusion. When the weekly examination reveals a dry canal and little liquid within the bulla, the inflammation and infection within the bulla has subsided (Figure 14-14).
At this point, bulla infusion treatments can be discontinued. Subsequent 2-week rechecks should reveal a healing eardrum.
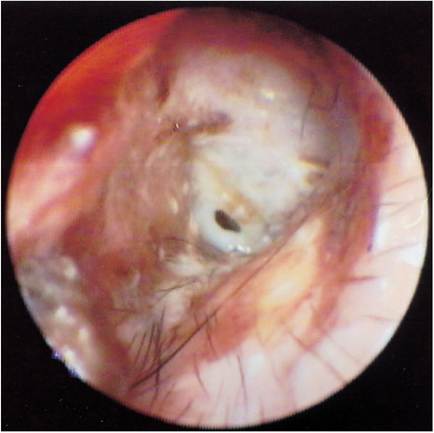
Figure 14-14
When otitis media resolves, the mucoperiosteum stops mucus and pus production and the ear canal is dry on subsequent examinations.
Topical therapy of otitis media in the author’s practice is 75% successful. A small number of chronic otitis media cases require total ear canal ablation and bulla osteotomy in spite of proper medical therapy.
The basis for topical therapy is that oral antibiotic levels in the bulla cannot approach topical levels. Even resistant organisms cannot survive the extremely high topical levels that can be achieved in the middle ear. For example, oral enrofloxacin at high levels (20 mg/lb daily) may achieve no more than 4 to 6 μg∕ml in the bulla, but infusing 1 ml of injectable enrofloxacin provides 22,700 μg∕ml. Even recommended off-label dilutions of injectable enrofloxacin of 1:1, 1:2, and 1:4 provide extremely high concentrations within the bulla. The limitation of topical therapy is that bulla infusion must be repeated at intervals frequent enough to maintain peak antibiotic levels.
Daily infusion would be ideal,15 but weekly treatment seems adequate.Much has been made of the use of the inhibitory quotient (IQ) for determining the efficacy of parenteral antibiotic therapy. The IQ is determined by dividing the tissue level of the antibiotic (Cmax) by the MIC of the bacteria.16 The tissue level is determined by the drug insert supplied with the antibiotic. The MIC is provided by the laboratory. High IQ values have been associated with a lower development of resistant bacteria. By definition, if the IQ is greater than 8 to 10, the antibiotic dose is optimal. For ciprofloxacin and marbofloxacin, resistant Pseudomonas organisms have an MIC greater than 2 μg∕ml, so to achieve the proper IQ, a middle-ear tissue level of 16 μg∕ml is necessary. For enrofloxacin, the laboratories usually consider greater than 4 μg∕ml “resistant,” so a 32-μg∕ml concentration would be necessary. It is doubtful whether oral doses of these medications can achieve these levels in the middle ear. Sensitive bacteria with low MICs may be adequately treated with systemic drugs that can reach the bulla.
If there is a resistant infection, the veterinarian should try to determine whether oral therapy alone is appropriate. For example, in a resistant Pseudomonas middle ear infection, if the MIC of the bacteria is reported as 3 μg∕ml (resistant) for enrofloxacin and the tissue level within the bulla using very-high-dose oral enrofloxacin (20 mg∕kg once daily) is 6 μg∕ml, the IQ is only 2. This indicates a suboptimal dose of oral antibiotic, although it is being administered at the highest recommended dose. Resistant organisms result from suboptimal antibiotic doses.
More on the topic Bulla Infusion and Topical Therapy:
- Topical Ototoxicity
- Flushing and Suctioning the Bulla
- Infusion ofHinduism and Bonda Religion into One Another
- Safe Drugs for the Tympanic Bulla
- Tympanic Bulla
- Imaging of the Tympanic Bulla
- PARENTERAL FLUID THERAPY
- Physical and Occupational Therapy
- Speech Therapy
- FETAL THERAPY
- Duration of Therapy