Fusobacterium Necrophorum infection
KJELL HANDELAND
Department of Animal Health, Section of Wildlife Diseases, National Veterinary Institute, Oslo, Norway
Fusobacterium necrophorum infection occurs worldwide and has been associated with disease (necrobacillosis) in domestic mammals, especially ruminants, for more than a hundred years(1).
Fusobacterium necrophorum (Family Bacteroidaceae) is an obligately anaerobic, non-spore-forming, pleomorphic, Gram-negative bacterium that tends to form filaments1-1’2). The bacterium is a normal inhabitant of the mammalian alimentary tract and an opportunistic pathogen. Two major biotypes are recognized: Biotype A, F necrophorum subspecies necrophorum, and biotype B, F. necrophorum subspecies funduliforme. Fusobacterium n. funduliforme is the predominant inhabitant of the alimentary tract, whereas F n. necrophorum is the most pathogenic, and the type associated with classical necrobacillosis in animals.
Necrobacillosis has been reported in various wildlife species, mostly from continents other than Europe(3). In the past, this disease was recognized as a serious health problem in semi-domesticated tundra reindeer (Rangifer tarandus tarandus) in northern Scandinavia and Russia(4). Reports from European wildlife include free-living European bison (Bison bonasus) in Poland(5) and wild tundra reindeer in southern Norway(6).
Virulent strains of F n. necrophorum may be present in the intestinal tract of animals and spread into the environment via faeces, causing infection in the feet, for example, with further spread via discharges from open lesions. The risk of disease and pathogen transmission is especially high in herd-forming species, or following other types of animal congregation. In North America, outbreaks of necrobacil- losis in wild ruminants have been associated with concentrations ofanimals at water holes under drought conditions, and around feeding stations at times of food shortage1-3).
The genital form of necrobacillosis seen in free-living male bison in Poland was suggested to be linked to heavy faecal contamination of their winter feeding sites(5).The serious necrobacillosis problem that occurred previously in semi- domesticated tundra reindeer in northern Scandinavia was linked to the intensive herding practised at that time, with frequent gathering of animals in confined spaces(4). This regular crowding in small, muddy and faeces-contaminated areas apparently functioned as a good environment for the bacterium and site of transmission between animals, with digital necrobacillosis as the main
Infectious Diseases of Wild Mammals and Birds in Europe, First Edition. Edited by Dolores Gavier-Widen, J. Paul Duff, and Anna Meredith. © 2012 Blackwell Publishing Ltd. Published 2012 by Blackwell Publishing Ltd. Material authored by Paul Duff remains Crown Copyright.
clinical manifestation. Other clinical manifestations seen in these reindeer herds were oral, skin, genital, udder and eye infections; conditions that were considered secondary to digital necrobacillosis.
Outbreaks of digital necrobacillosis occurring recently in wild tundra reindeer in southern Norway were apparently associated with extended periods of precipitation and high air temperature during the summer(6). Permanently damp pastures presumably improve the survival of the bacterium in the environment and predispose to digital skin infection. Skin that is damp for long periods is more vulnerable to abrasions, creating suitable entrance sites for the bacterium.
Fusobacterium necrophorum gains entrance through epithelial defects or small wounds in the skin or alimentary tract and proliferates in the subepithelial connective tissue. Growth is stimulated by the presence of facultatively anaerobic bacteria, e.g. Actinomyces pyogenes and Staphylococcus aureus, which provide lowered oxygen tension in the tissue. Pathogenicity is linked to the production of various toxins, with leucotoxin and endotoxin considered the major virulence factors(1,2). Necrobacillosis lesions may occur in almost any part of the body but are most frequently recognized in the feet (digital necrobacillosis) and mouth (oral necrobacillosis).
Lesions produced are cellulitis and progressive peripheral coagulative necrosis linked to vasculitis, thrombosis and ischaemia. In digital necrobacillosis, gross lesions include swelling of the foot and cutaneous sinus tracts with sparse discharge of pus(6). Subcutaneous tissues are inflamed and thickened with focal necrosis, and tendons, tendon sheaths, joints and periosteum of the digital bones are often affected. Occasionally, secondary necrotic foci may be found in the mouth, rumen, liver and lungs. Microscopically, digital lesions are characterized by deep skin ulcers with centrally located necrotic tissue, bordered by a zone of oedema and intense inflammation with granulation tissue and fibrosis. Bone lesions are characterized by necrosis, fibrosis and bone proliferation. Elongated filamentous bacteria can be seen at the periphery of the necrotic areas, even with standard haematoxylin and eosin stains.
I n primary oral necrobacillosis, areas of necrosis may occur in various soft tissues of the mouth cavity, and may also affect the mandibular bones(7). Oral necrobacillosis frequently leads to secondary foci of infection (necrosis) in the lower alimentary tract, especially the rumen, and in the liver.
The protective immunological response to F necro- phorum infection is weak, and no effective vaccine has been developed(2). However, in bovine digital necrobacil- losis naturally acquired immunity seems to inhibit reinfection by the same strain for at least 6 months(8). Some protective acquired immunity also seems to occur after outbreaks among wild ungulates(6).
Clinical signs observed in digital necrobacillosis include swelling and lameness in one or several feet. The severity of signs varies from immobility, when several limbs are heavily affected, to the slight and transient signs caused by mild infections. Clinical signs of oral necrobacillosis include excess salivation, as well as problems in chewing and swallowing food.
Oral infection also predisposes to aspiration of infectious materials and subsequent fusobac- terial pneumonia. Spread of infection via the general circulation may terminate in septicaemia and rapid death.Therapeutically, penicillins, tetracyclines and macrolides are efficient against F necrophorum if administered at an early stage of infection(2).
A confirmatory diagnosis is dependent on isolation of F. necrophorum using anaerobic culture techniques. Even under optimal laboratory conditions, F necrophorum can be difficult to isolate as a result of culture dominance by facultative anaerobic bacteria. In such cases, direct detection of the bacterium in tissues using fluorescence i n situ hybridization is a useful diagnostic technique (Figure 37.1).
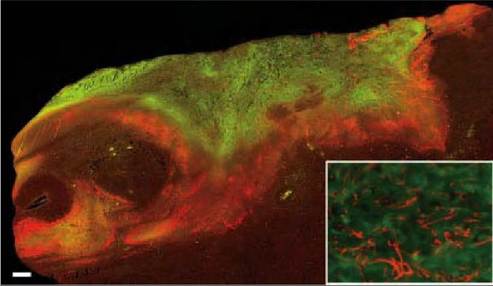
FIGURE 37.1 Digital necrobacillosis in wild reindeer. Fluorescence in situ hybridization of a necrotic skin lesion: multiple microcolonies of F necrophorum (red fluorescence) invading the surrounding connective tissue (brown colour). Debris with only a few F. necrophorum is characterized by green autofluorescence. Insert: detail showing multiple filamentous F necrophorum within the lesion. Scale bar = 400 μm. (From Handeland et al., 2010)(6).
Feeding of free-living and captive wildlife, in muddy and faecally contaminated areas should be avoided. Fuso- bacterium necrophorum is also associated with anaerobic infections in humans, especially in the oral cavity(2). However, subspecies necrophorum, which causes classical necrobacillosis in animals, does not seem to be involved in human infection1-9). Therefore, the zoonotic potential of animal necrobacillosis can be regarded as negligible.
More on the topic Fusobacterium Necrophorum infection:
- suttonella ornithicola sp. NOV. INFECTIONS OF SPECIES OF TIT AND LONG-TAILED TITS
- Arcanobacterium infections
- Corynebacterium bovis Infection: Coryneform Hyperkeratosis; Scaly Skin Disease
- Clostridium piliforme Infection: Tyzzer’s Disease
- Clostridium piliforme Infection: Tyzzer’s Disease
- 5 Appendices
- BIBLIOGRAPHY FOR BACTERIAL INFECTIONS