Picornavirus Infection: Mouse Encephalomyelitis Virus Infection
Mouse encephalomyelitis virus (MEV) belongs to the family Picornaviridae, genus Cardiovirus, which also includes the serologically related encephalomyocarditis virus (EMCV). EMCV has a less-selective host range and can infect wild mice, but is not known to infect laboratory mice.
MEV is commonly referred to as mouse poliovirus or Theiler's virus, after its initial discoverer, Max Theiler. There are numerous strains of MEV that infect mice, including TO (Theiler's original), GDVII, FA, BeAn, and DA, among others. Some of these strains have been studied extensively as models for viral encephalitis and demyelination, resulting in emphasis on neurologic disease, which is only rarely a component of natural infection.Epizootiology and Pathogenesis
MEV is a widespread infectious agent among wild and laboratory mice throughout the world. MEV is regarded as a mouse virus, but sera from rats and guinea pigs may react with MEV due to infection with related viruses. MEV was initially isolated from paralytic mice in the 1930s by Max Theiler. In spite of the emphasis on neurovirulence, MEVs are primarily enteric viruses. Virus excretion from the intestine is highly variable among mice, but it is often prolonged and intermittent. Transmission is inefficient, often with only a small percentage of seropositive mice within a population. In utero infection does not occur, and maternal antibody plays an important role in protecting pups. Infected mice develop a transient viremia that is limited by host immune response. Occasionally, virus gains access to the central nervous system. Vascular endothelial cells appear to serve as a conduit for entry into the brain, but there is also evidence for axonal transport of virus.
MEVs can be divided into two groups, based upon their experimental neurovirulence. Virulent strains of virus, such as GDVII or FA, induce severe fatal encephalitis, regardless of route of inoculation.
Most other strains are less virulent and can cause biphasic disease, consisting initially of acute poliomyelitis, followed later by late- onset demyelinating disease. Virus can persist in the central nervous system for over a year, but virus titers decline markedly, and residual virus is restricted to white matter, where it replicates in macrophages, leukocytes, astrocytes, and oligodendrocytes. Immune attack on infected white matter results in demyelination and motor dysfunction, with gait disorders, tremors, ataxia, extensor spasm, urinary incontinence, and other signs. The neurological manifestations of MEV are grossly overemphasized because of their experimental value. Under natural conditions, usually only 1 in 1,000-10,000 infected immunocompetent mice develops clinical signs of the nervous system, and this is invariably flaccid paralysis associated with the acute, poliomyelitis phase. However, in immunodeficient mice, exposure to MEV may result in high morbidity and mortality. Experimental susceptibility to MEV-induced demyelinating disease has been demonstrated in SJL, DBA/2, C3H/He, SWR, and PLJ strains, whereas BALB/c, B6, A, and 129 strains are resistant. Genetic susceptibility to demyelination is polygenic, but linked to H-2d haplotype in some strains.
FIG. 1.40. Mouse with posterior paresis due to natural infection with mouse encephalomyelitis virus (MEV).
Pathology
MEV replicates in enterocytes, but intestinal lesions are not present. During the acute central nervous system (poliomyelitis) phase, mice may present with posterior paresis (Fig. 1.40). Virus attacks neurons and glia of the hippocampus, thalamus, brain stem, and spinal cord. Neuronolysis, neuronophagia, microgliosis, nonsuppurative meningitis, and perivasculitis are typical changes seen microscopically. These changes are most prevalent in the brain stem and ventral horns of the spinal cord (Fig.
1.41). During the demyelinating phase of experimental disease, foci of demyelination are present in the white matter of the spinal cord, brain stem, and cerebellum. Demyelinating lesions are not a likely component of natural infections. Acute myositis and focal myocarditis were observed in mice inoculated intraperitoneally with the DA strain of MEV, emphasizing the polytropism of the virus. The naturally occurring disease is much more devastating in immunodeficient mice, with high morbidity and mortality. In SCID mice, lesions are characterized by marked vacuolation and enlargement of affected neurons, particularly in the brain stem and ventral horn region of the spinal cord. Vacuolation of adjacent astrocytes and oligodendrocytes, with minimal to no inflammatory cell response, is another feature of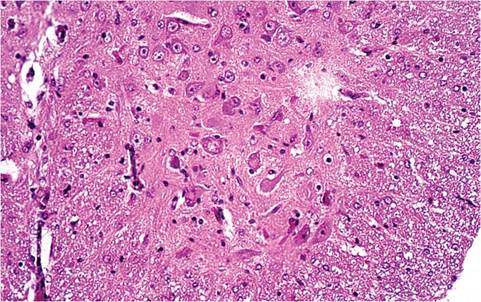
FIG. 1.41. Spinal cord from the mouse depicted in the previous figure. There is acute neuronolysis in the ventral horn.
the disease in SCID mice. Similar changes have been observed in the gray and white matter of nude mice.
Diagnosis
MEV infection is usually diagnosed serologically. There is extensive antigenic cross-reactivity between EMCV and MEV, but the former is not prevalent in laboratory mice. Antibodies to the two groups of virus can be differentially discriminated by serum neutralization. This method can also be used to discriminate between MEV strains, but that has no practical value. Seropositive mice should be considered to be actively infected with virus. Diagnosis can also be achieved by neurological signs and lesions in the small percentage of infected mice that develop central nervous system disease. MEV is not very contagious, requiring large sample sizes to accurately detect infection within a colony. Virus can be grown in cell culture, but isolation is difficult from adult mice. PCR amplification from tissue, particularly intestine and mesenteric lymph node, can also be used to diagnose active infection. Because of its low contagious potential, MEV can be eliminated from a colony of immunocompetent mice over time by test-and-slaugh- ter at the cage level, if appropriate safeguards are taken against contamination of mice in adjacent cages. Differential diagnoses for neurological disease include trauma, neoplasia, otitis, MHV, LDV in immunodeficient C58 or AKR mice, and polyoma virus.
More on the topic Picornavirus Infection: Mouse Encephalomyelitis Virus Infection:
- LJUNGAN virus infection
- Salmonella enterica Infection: Salmonellosis
- Arterivirus Infection: Lactate Dehydrogenase-Elevating Virus Infection