Thoracic cavity
The thoracic cavity or thorax is divided into the right and left pleural cavities by a double layer of pleura known as the mediastinum. Each pleural cavity is lined
by a single Inyer of serous membrane.
the plcurnl ιncnι- braιιe I Fig. 8.5).'Hiis secretes a small amount of serous or waterv Iluid whose function is to reduce frictionW
between the pleural surfaces as the lungs move during respirat ion. 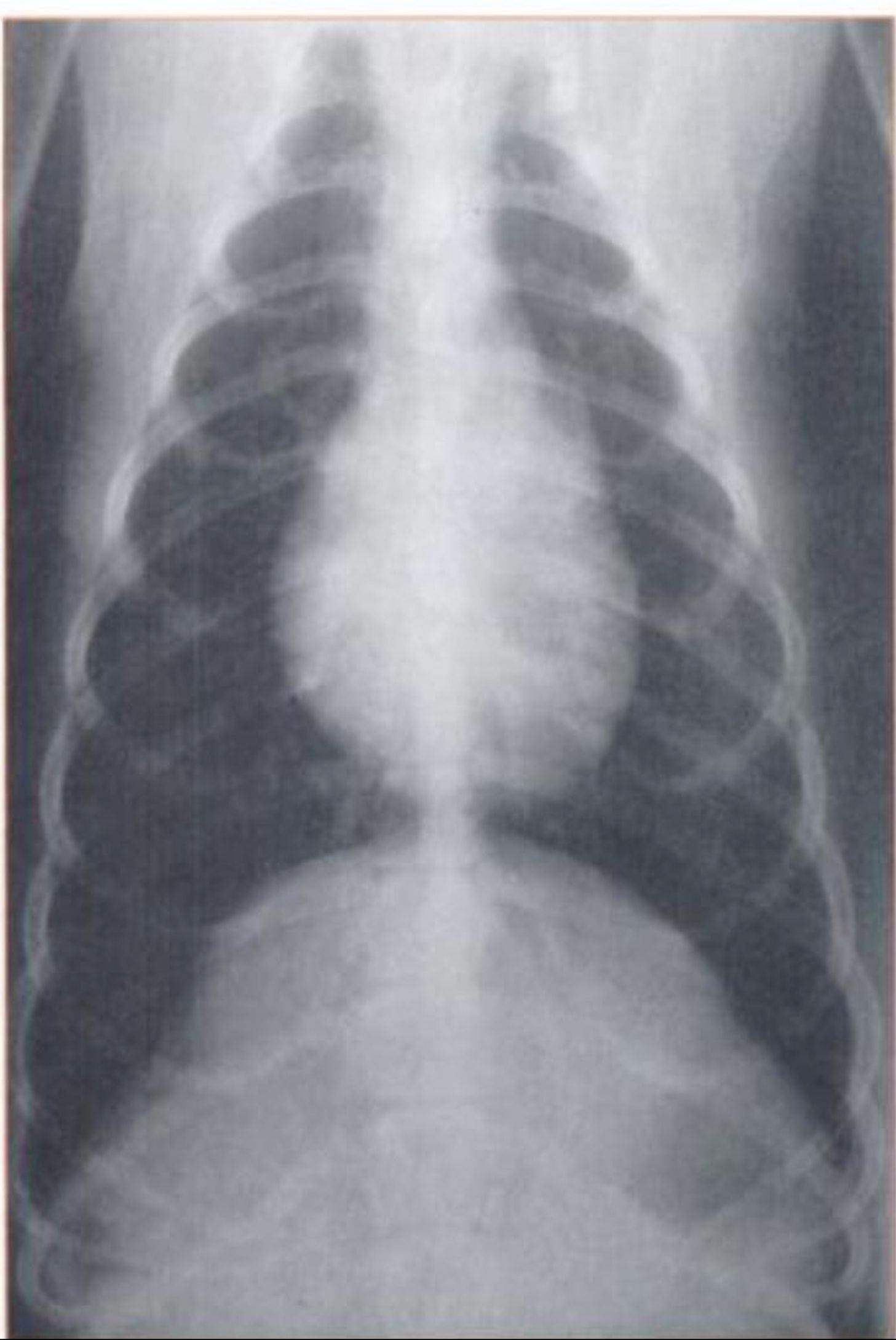
If the pleural cavity becomes occupied by anything other than a vacuum, e.g. air (pneumothorax), blood (haemothorax) or pus (pyothorax), the ability of the lung to inflate fully will be impaired and the animal will show signs of respiratory distress (dyspnoea).
.All the structures lying in the pleural cavities are covered in the pleural membrane and it is named according to the structures it is covering. The pleural cavity lies between the two layers of pleural membranes and contains a vacuum and a small volume of pleural Iluid.
Type of pleura
Diaphragmatic
Pulmonary or visceral
Costal or parietal Mediastinal
Structures covered
Cranial aspect of the diaphragm Right and left lungs - outlines each lobe
Inner side of the ribs
Mediastinum
Most of the organs in the thorax lie in the space between the two layers of mediastinal pleura, i.e. the heart and its associated blood vessels, trachea and oesophagus (Fig. 8.10). The mediastinum of the dog and cat is quite tough and forms a complete barrier
Fig.8.7 VcntnxkXMl fdd∙ogr,ιpħ of.ι dogs thoraxThe lungs arc full of air and.ιppc υ dark on the X ray.
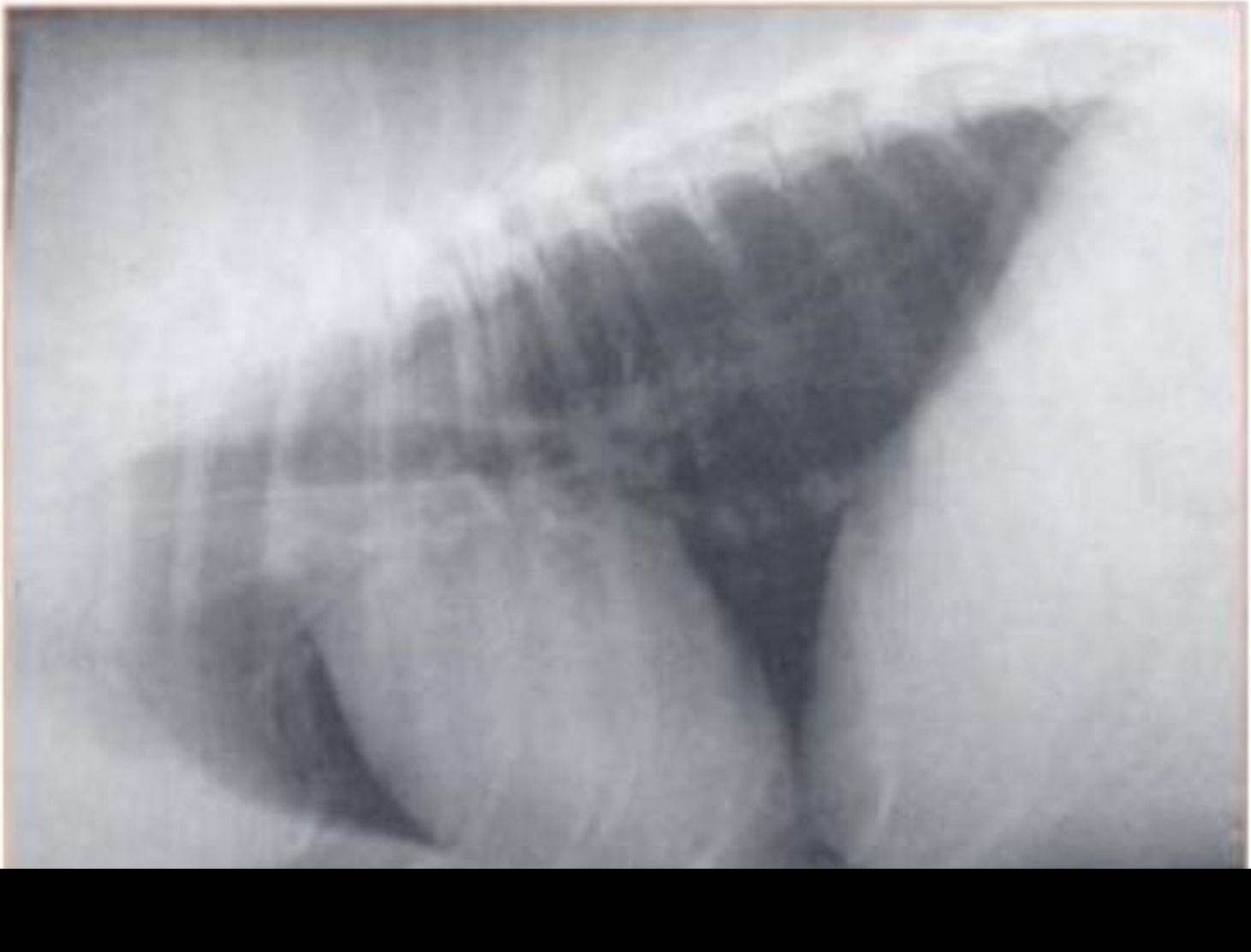
Fig. 8.8 Litoral radiograph of a dog's thorax The lungs appear dark on the ?-∙∙ r, due to a∣r.
and.i∣∣o∙λ the other structures to be visualised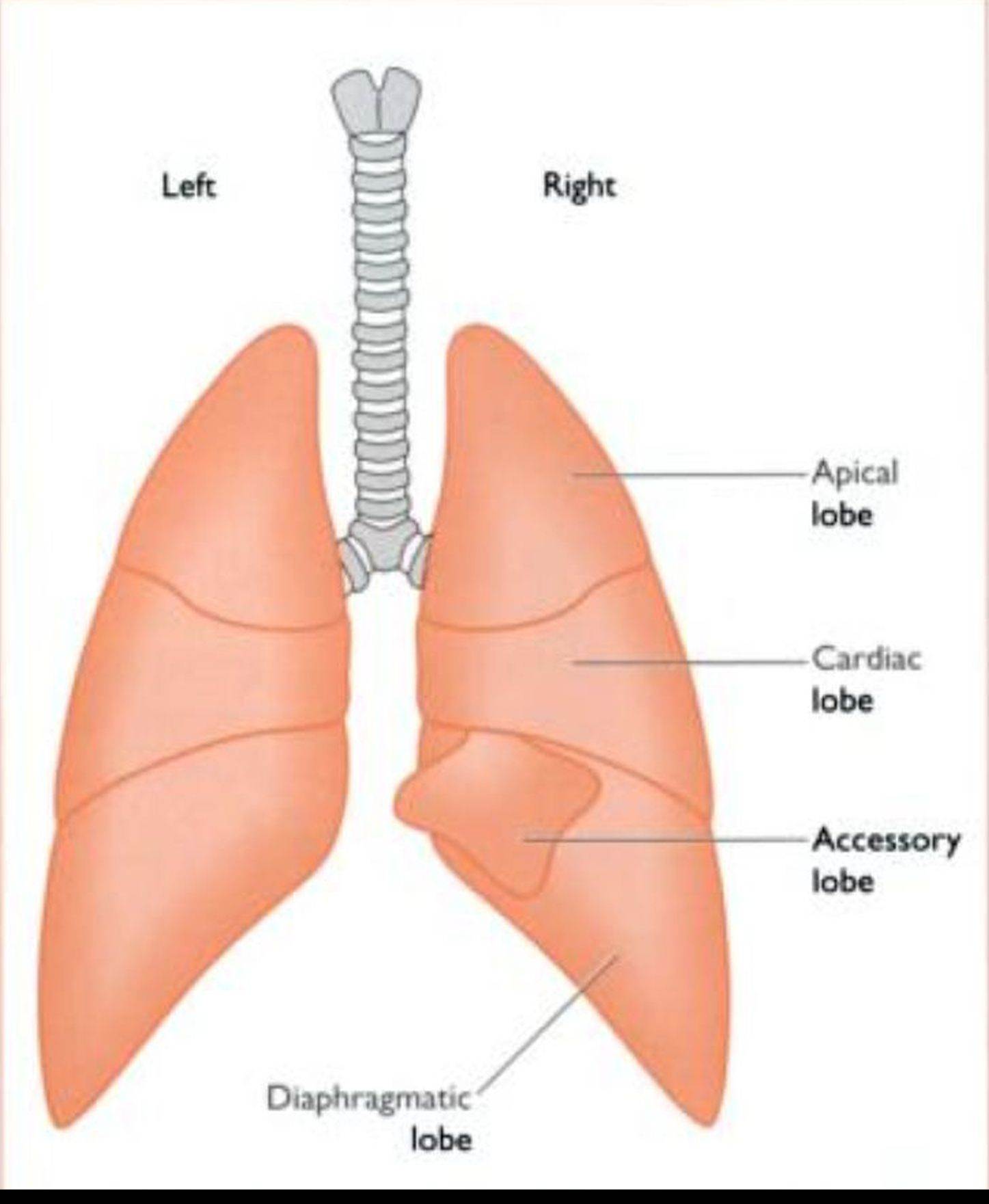
Fig. 8.9 The d∣v∣s∣on of the lungs into lobes by deep fissures.
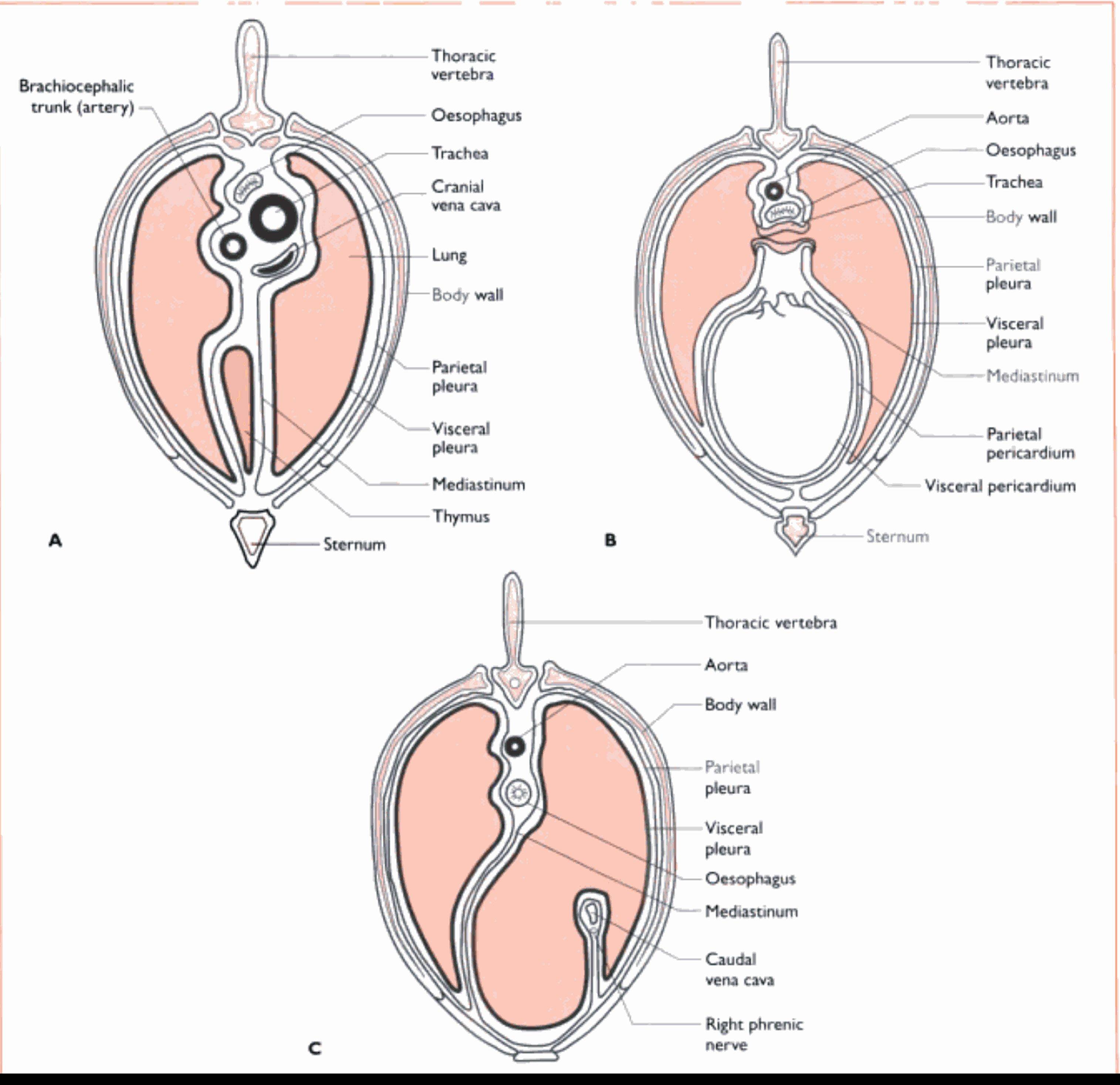
Fig. 8.10 Cross-section of the tħintake and expulsion of gases, a complex system of control of respiration has evolved.
Wilhin lhe pons and medulla of the hindbrain Ihere arc respinιtorι∣ centres responsible for the control of inspiration and expiration. They are the pneumo- tax Ic and upneustic centres which control expiration and the Inspiratort/ centre which controls inspiration. Impidses from lhe inspiratory centre travel to lhe diaphragm via lhe phrenic nerve and to the intercostal muscles via the intercostal nerves and bring about inspiration. Expiralion is mainly passive but impulses from lhe expiratory centres may assist in expiration. These centres inhibit each other and cannot work Simullaneously. They are responsible for the basic rhythm of respiration.
The rale and depth of respiration is controlled by receptors within lhe body:
Stretch receptors - lie within the walls of the bronchi and bronchioles and monitor the degree of stretching of the bronchial tree. When lhe lung is distended Ihey send impulses via the vagus nerve to the inspiratory centre of the brain. Further inspiration is inhibited and expiration is stimulated via the apncustic centre. This is known as the Hering-Breuer rellex and it prevents Overinllation of the lungs.
Chemoreceptors:
- Periphenil - these are known as the north (located in lhe walls of the aorta, close to the heart I and the carotid (located in the walls of the carotid artery I boro-mandibιdar joint. In carnivores the action of the joint is scissor-likc to shear Ilesh off the bones of their prey.
The upper and lower jaws are linked by skin, forming the checks, under which lie the muscles of mastication (sec Ch.
4). These muscles lie over the temporomandibular joint and give strength to the biting action. The entrance to the mouth is closed by the lips.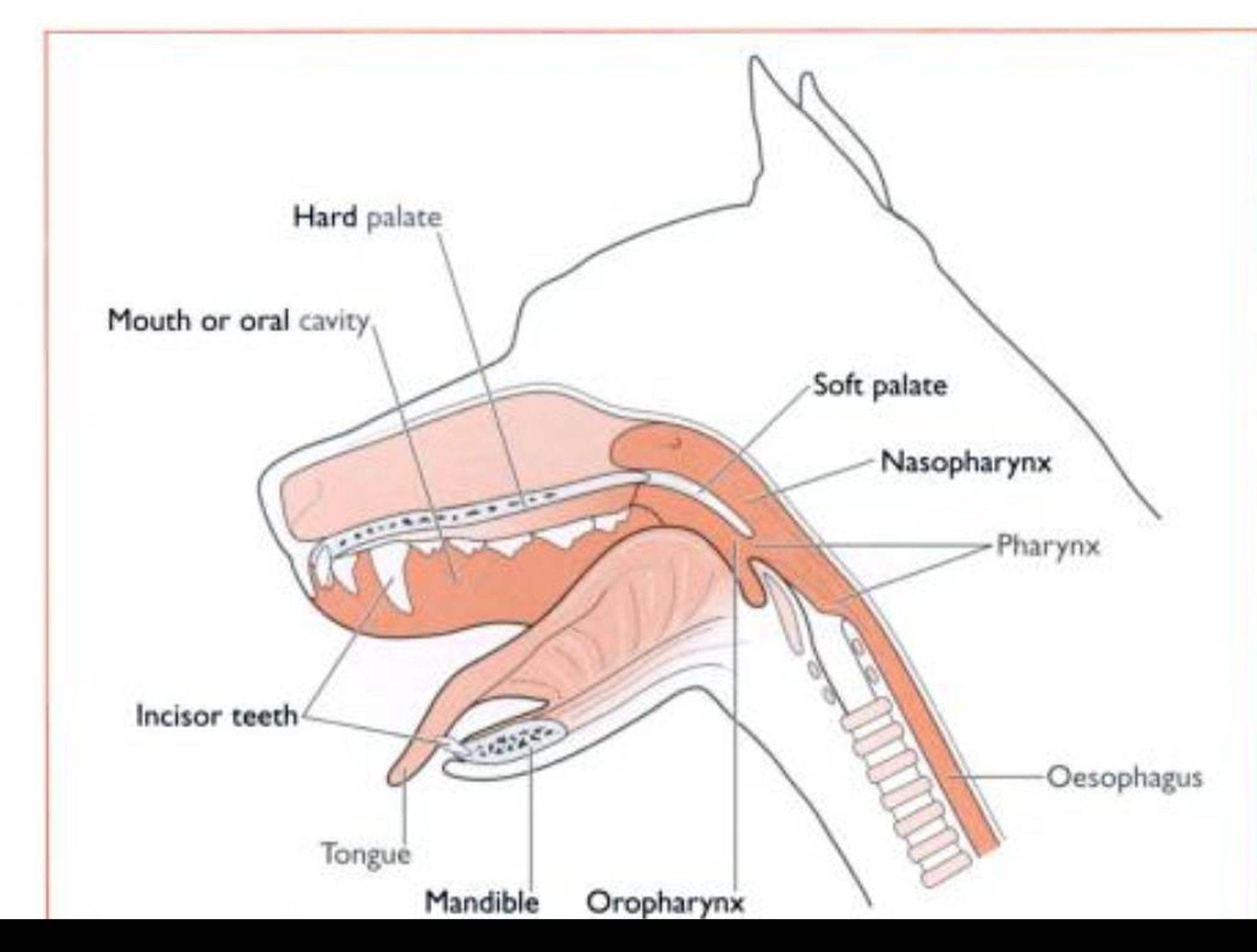
Fig. 9.3 Lateral view of the dog's bead to show the oral c⅛vt//digestive system
composed of muscle covered in skin. rΓhc upper lip is split vertically by a division known as the philtrum (Fig. 8.1).
The entire oral cavity is lined by a layer of mucous membrane. It is reflected on to the jawbones, forming the f∣ιιms. The mucous membrane covers the hard palate and extends over a flap of soft tissue at the back of the oral cavity - this is the soft ∣xιlate which extends cau- dal∣v bet ween the oral and nasal cavities and divides the
■F
pharynx into the oropharynx and nasopharynx (Fig. 9.3).