ENVIRONMENTAL-MEDIATED AVAILABILITY OF VITAMIN D AND IMMUNE FUNCTION
The influence of either abnormal status or environmental-limiting availability of vitamin D hormone on several disease sustains the critical role of 1,25(OH)2D3/VDR pathway in normal immune system function.
Vitamin D deficiency, that tends to induce an over-grounded Th1 response, has been associated with susceptibility to autoimmune diseases such as rheumatoid arthritis, type-1 diabetes, systemic lupus erythematosus, psoriasis, inflammatory bowel disease and multiple sclerosis [114]. On the other hand, the over-induction of 1,25(OH)2D3/VDR pathway that precludes an accurate control of Th1 response and favour a Th2 response and a tolerogenic state, seems to predispose to allergic conditions [115,116]. Concerning 1,25(OH)2D3 involvements on susceptibility to pathogen infection, it has been reported that vitamin D insufficiency predisposes to bacterial and viral infections [7]. Susceptibility to Mycobacterium infection has been largely related to vitamin D deficiency [117]. Low levels of vitamin D compromise vitamin D-mediated immune modulations that, in the context of tuberculosis infection, can be detrimental by limiting the capability of MAC function to suppress intracellular growth of tuberculosis bacterium and compromising the production of microbe-killing cathelicidin [15].Seasonal Variation of Sunlight Exposure, Vitamin D and Immune Functions
Changes in immunological parameters have been described in tourist travelling to sunny countries without prior adaptation to UVB exposure. Subjects receiving substantial doses of UVB, as reflected by response to questionnaires, UVB dosimetry and increase in 25-hydroxyvitamin D3 show significant alterations in the immune system function [118]. A fashion hypothesis proposes a link between sunlight exposure, vitamin D availability and susceptibility to bacterial and virus infection.
Following this hypothesis, low sun exposure, due to limiting environmental conditions or in-house social behaviour, predispose to vitamin D insufficiency that could favour the acquisition of bacterial and viral infections. In line with this hypothesis, higher prevalence of tuberculosis infection has been found in Asiatic immigrants living in United Kingdom than in those living in their countries. From such a hypothesis, lowering the availability to sunlight in northern latitudes can preclude enough vitamin D synthesis, which predisposes Asian immigrants in the UK to tuberculosis infection [119]. Also, the seasonal variation of influenza infection has been linked to the seasonal variation of sunlight exposure-related vitamin D deficiency [120]. However, the effect of additional climatic conditions, such as humidity and temperature, as well as the detrimental effect of UV exposure on the survival of viral particles, cannot be ruled out [121]. A recent work evaluating meteorological conditions in relation to respiratory syncytial virus (RSV) infection reveals that RSV activity was inversely related to UVB [122], suggesting that vitamin D insufficiency during winter season increases susceptibility to respiratory infections, and implying that vitamin D supplementation can decrease their severity and occurrence. Nevertheless, a recent report was unable to detect any benefit of vitamin D supplementation in decreasing incidence or severity of respiratory infections during winter season [123]. Influence of seasonal variations in genital infections has also been detected in cervical smears screened for cervical carcinoma in The Netherlands [124]. Seasonal peaks for both Candida and Chlamydia were detected in fall season. In contrast, infections of Actinomyces and Trichomonas were more likely to occur in winter season. Concerning to Human Papiloma Virus the seasonal peak was observed in summer season. Complex interactions between host, infectious agent and environmental conditions can be taken into account to explain this pattern of seasonality. The contribution of season-dependent availability of vitamin D, if any, may be pathogen-specific.Environmental-Mediated Availability of Vitamin D and HIV Infection
There are few data relating sunlight and UVB exposure with HIV-1 infection that can allow us to evaluate their impact on the disease. Early studies were focused on UVB effect on HIV-1 virus replication. Transgenic mice expressing HIV Tat gene under the control of the HIV LTR, showed bolstered Tat protein expression in the skin after exposure to UV light [125]. This effect linked to UVB-mediated vitamin D synthesis was not investigated. However, concerns have been raised about potential adverse effects of UV radiation, as used in phototherapy and photo-chemotherapy, on HIV-1 infected persons. Several studies have been addressed to clarify this question that seems to discard any adverse effects of UV radiation on HIV infected patients under UV phototherapy [126,127]. Immunosuppressive effects of sunlight exposure have been also considered detrimental in the context of HIV infection, being proposed as a risk factor for progression to AIDS [9]. Epidemiological studies based on well-established HIV/AIDS cohorts have tried to address this question. Epidemiological data from the Multicenter AIDS Cohort Study (MACS) revealed that sunlight exposure is not associated with a decline in T-helper lymphocyte count or progression to AIDS [128]. Nevertheless, two studies based on the Amsterdam Cohort Study (ACS) on HIV and AIDS show contrasting results. The first study evaluated individual exposure of homosexual men to sunlight by means of a 2-year retrospective questionnaire that was given to some of the participants (n=57). In agreement with the previously mentioned study on MACS, exposure to sunlight does not produce adverse effect on CD4+ T-cell count, CD4+/CD8+ T cell ratio, and T-cell reactivity [129]. The same authors developed a second study by an extended number of subjects (n=557) from which they found lower levels in the mean number of CD4+ T cells and the mean CD4+/CD8+ ratio during summer and spring with seasonal effect being more prominent at a more advanced stage of the HIV/AIDS [130].
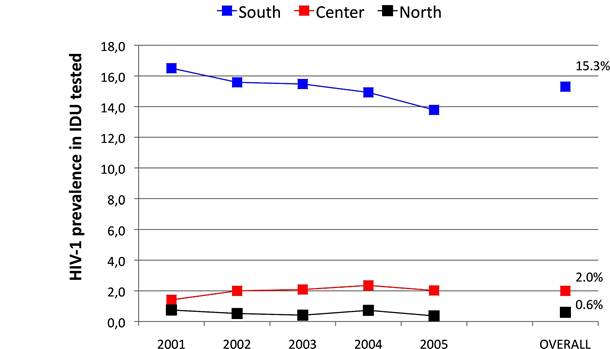
The spread of HIV infection in Europe has been mainly observed in intravenous drug users (IDU). In the early HIV epidemic the prevalence of HIV infection in IDU reached the highest values in the Mediterranean area such as Spain (>60%), French (30%) and Italy (23-31%), as well as in North-Atlantic countries such as Scotland (>64%) and Denmark (>20%) [131,132]. Social and political strategies for the prevention of HIV transmission among IDU were implemented from the beginning of the epidemic with encouraging results. As a consequence, a decrease in HIV prevalence has been observed in several countries, but this reduction seems to have stabilised lower prevalence values in the Northern region than in Southern region [131,132]. Based on public data from surveillance of HIV/AIDS infection in Europe [133], we have plotted in Fig. 6 the prevalence of HIV infection in IDU corresponding to selected European country regions: Southern region with latitude 55°N as for Scotland, Norway and Finland. All these countries belong to the European Union, except for Norway, and share common political, economical and social characteristics. Prevalence trends in the period 2001-2005 were highly stabilised for each region but larger values were observed in Southern (overall 15.3%) than in Central (2.0%) or Northern (0.6%) regions. Taken into account that prevalence of HIV infection in early epidemic was broadly extended in different European areas and that social and political strategies to prevent infection have been applied with equivalent intensities among different countries, the differential set-point pattern achieved was unexpected.
Years
Figure 6: Prevalence of HIV infection among injection drug users in Southern, Centre and Northern European regions. Mean prevalence of HIV infection in IDU subjects corresponding to selected European country regions: South
(latitude 55°N; Scotland, Norway and Finland) (black line).
Data obtained from public surveillance of HIV/AIDS infection in Europe [136] among 2002 to 2005 period. Prevalence trends in 2001-2005 for South Central and North regions were 15.3%, 2.0% and 0.6%, respectively.Prevalence of HIV infection in Eastern European countries is growing dramatically and no latitudinal distribution can be observed. Probably, in the early spread of the epidemic, such as happened in the western European countries in the 80’s, socioeconomic, behavioural and political factors exert the main effect on prevalence. Later, we can expect a plateau on prevalence, such as observed in western countries, in which “intrinsic” factors determined the prevalence set point. The question we address is: what are those “intrinsic” factors? Behavioural and cultural singularities, that characterise each European region, could be critical, although, we cannot exclude that environmental factors such as sunlight exposure/UVB radiation, and the associated bolstering of HIV replication and immunosuppressant effect, can be involved on the determination of the prevalence set point.
It is well known that sensibility to the sunlight/UVB exposure effects varies among human populations depending on geographical location and skin colour. It is considered that evolutionary forces acting on skin colour variability in humans are strongly related with sunlight/UVB exposure [133].
Darker skin subjects are protected from sunburn and UVB-related damages, while they can have compromised vitamin D metabolism, even at high latitude regions. On the contrary, clear skin subjects are vulnerable to sunburn and UVB-related damages, whereas they can reach regular vitamin D metabolism, including in low irradiated regions.
It was stated that cutaneous photolysis of 7-dihydrocholestorol to cholecalciferol in the skin was strongly reduced in winter season in Boston (42°N), while cholecalciferol production occurred throughout the year in Los Angeles (34°N) and San Juan de Puerto Rico (18°N) [134].
Calculation of the time required to have enough amounts of vitamin D for a healthy vitamin D status has been modelled in the customizable web site “http://nadir.nilu.no/~olaeng/fastrt/VitD_quartMED.html” [135]. In the winter season (i.e. December) at 42°N a subject with skin type 1 (Caucasian, very sensitive, always burns easily, never tans, very fair skin tone) needs a minimum of 50 min to reach 1000 IU (daily recommended dose). In contrast, a subject with skin type VI (dark-skinned black) will need 24h of solar exposition to reach this minimal level. Values changed at the summer season (i.e. July) in which subjects with skin type I and VI only need 4 and 18 minutes, respectively, to reach the recommended minimal. At lower latitudes (i.e. 35°N) the capability to synthesise functional vitamin D is not limiting for people with skin type I, that need 25 min in December and 3 minutes in July, and lightly limiting for those with skin type VI, that need 2 hours and 13 min in December and 16 min in July. Lightly coloured skin persons may likely access to any beneficial effect of vitamin D production, while darker coloured persons will be protected from any detrimental effect.In an attempt to evaluate this proposition we have searched in the literature for epidemiological studies evaluating prevalence of HIV infection on light and dark coloured people living at different latitudes. Unfortunately, there are not many studies of this nature from which we can extract information needed, but a recent epidemiological study of HIV prevalence in civilian applicants for the United States of America military service can help us in this way [137]. This was an exhaustive analysis of the geographical distribution of HIV infection throughout the US territory in which they have studied 5.7 million of subjects (79% White and 21% African-American) who applied for US military service between 1985 and 2003. The authors searched for spatial HIV clustering of data, discriminating between White and African-American groups. They have found three main clusters for the White data, one located in the Northeast area of New York and New Jersey, a second in the Southeast area around Huston, Texas and a third cluster in the Southwest area of Los Angeles, California (Fig. 7). Nevertheless, data from African-American subjects reveals two stronger clusters in the Northeast area of New York-New Jersey and Washington DC and an additional cluster in the Southwest area of Los Angeles, but no cluster was detected in the Southeast area around Houston (Fig. 7). It is remarkable that the two coincident cluster areas between White and African-American correspond to two of the most populated areas in USA, whereas the discordant cluster corresponds to a more rural area. The high population density in these regions and the aggregation behaviour of human beings contribute to the spread of HIV infection among equals. We can interpret that in highly populated areas, social, behavioural and economic factors overcome any additional factor affecting susceptibility to infection. When these factors are less prominent, hidden factors can emerge. Then, environmental factors, such as sunlight exposure, could reveal their protective or detrimental effect on HIV infection in susceptible subjects. The cluster detected in the Southern area around Houston, affecting only White subjects, seems to indicate that, in a highly sunlight exposed and low populated area, white people are more susceptible to infection than African-American. We are conscious that any conclusion derived from an exploratory analysis like this must be taken with caution, but we hope that this could encourage the design of new epidemiological analysis trying to clarify this question.
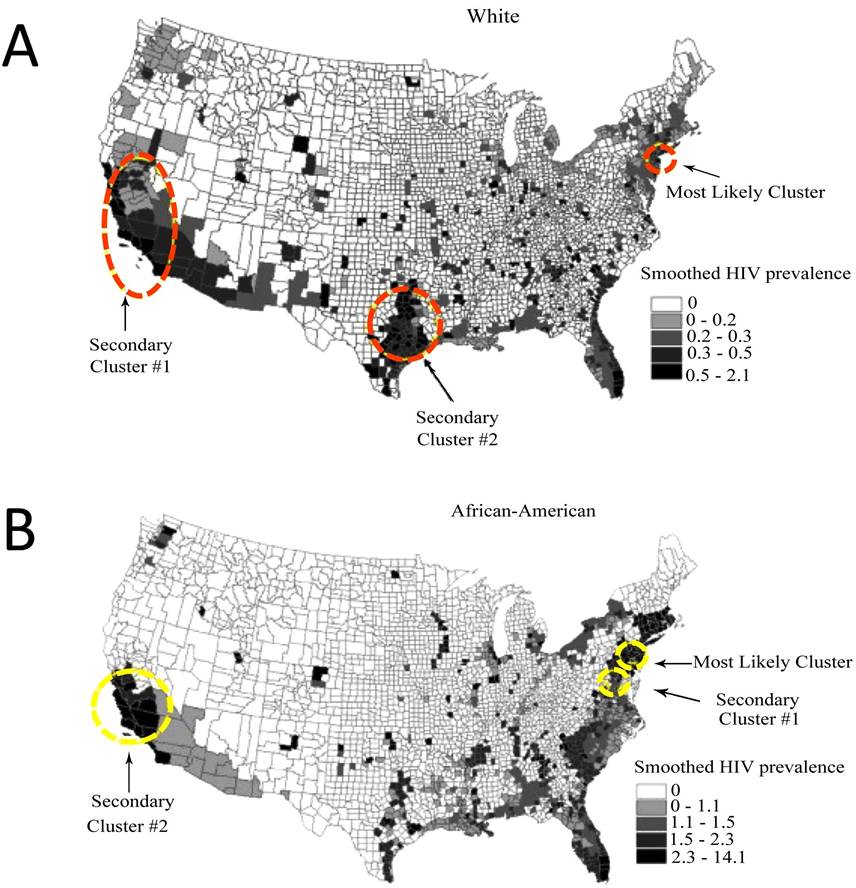
Figure 7: HIV prevalence and clusters among white (A) and African-American (B) civilian applicants for Unites States military service. Reproduced by permission from Bautista CT, Sateren WB, Sanchez JL, Singer DE and Scott P. Geographic mapping of HIV infection among civilian applicants for United States military service. Health & place 2008;14:608-15 [137].
Vitamin D Status and HIV Infection
There is a great concern about vitamin D status in the general population. Vitamin D deficiency has been recognised as a general problem of pandemic dimension. Few foods contain enough quantities of vitamin D and precursors, whereas cultural and social behaviours limit the access to photoproduction of vitamin D precursors in the skin. Following this, synthesis of 25(OH)D3 can be compromised limiting the synthesis of the 1,25(OH)2D3 active form. It is well established that serum levels of 25(OH)D3 but not 1,25(OH)2D3 are indicatives of the vitamin D status.
The circulating concentration of 25(OH)D3 is a good reflection of both exposure to sunlight and dietary intake of vitamin D precursors. Although there is not a general consensus about the optimal serum concentration of 25(OH)D3, vitamin D deficiency is considered when 25(OH)D3 serum levels are below 20 ng per millilitre (50 nmol per litre). However, other authors consider vitamin D insufficiency for serum concentrations between 20 to 30 ng per millilitre (50-75 nmol per litre) and sufficiency for values greater than 30 ng millilitres. Although occurring in rare circumstances, 25(OH)D3 can produce intoxication when serum levels are greater than 150 ng per millilitre (375 nmol per litre) [138].
According to these definitions more than a million people worldwide are affected by deficient/insufficient status [139]. Among them, elderly, postmenopausal women and children are the most significant groups at risk. Environmental factors, sunlight exposure, latitude and season; nutritional factors, diet, fortified foods and dietary intake; behavioural factors, life style (i.e., indoor-outdoor) and clothing; demographic factors, age and finally, healthy factors can affect vitamin D status. HIV infection has been recognised as a risk factor for Vitamin D insufficiency. Deficiency in micronutrients has been early described for HIV/AIDS patients as a common feature, mainly in those with advanced disease [140].
Abnormal levels of 1,25(OH)2D3 have been described in symptomatic HIV infected patients (CDC stage IV) while near to normal levels were observed in asymptomatic (CDC stage II/III). Serum levels of the active hormone were directly correlated with CD4+ cell counts in blood and inversely correlated with survival.
On the other hand, 1,25(OH)2D3 levels have not been correlated with vitamin D deficiency as determined by serum levels of 25OHD3 [141,142]. Disturbances in bone remodelling have been described in patients with advanced disease, mainly related with an increased activity of TNF-α or direct HIV-effect on osteoblasts or osteoclasts precursors. As TNF-α may inhibit the effects of 1,25(OH)2D3 on osteoblasts function [143], decreased levels of 1,25(OH)2D3 may boost TNF- α function and disturbing bone metabolism in HIV infection [144].
Decreased activity of vitamin D metabolic enzymes has been described in patients treated with protease inhibitors (PI). PI inhibits enzymatic activity of 25- and 1,25-hydroxylase enzyme (CYP27A1 and CYP27B1, respectively) and, to a lower extend, 24-hydroxylase (CYP24A1) enzyme activity. In in vitro assays with the human monocyte- MAC cell line THP-1 inhibition of 1,25-hydroxylase activity was of 80% by ritonavir, 66% by indinavir and 32% by nelfinavir [145,146]. Impaired vitamin D metabolism during PI-based HAART regimens may be responsible for the higher risk of bone dysfunction in patients under this treatment protocol [147,148].
The true relevance of vitamin D deficient/insufficient status in HIV infected patients must be considered in the context of the general/healthy population. As stated in the epidemiological study based on the Reaching for Excellence in Adolescent Health (REACH) cohort, the prevalence of vitamin D insufficiency in HIV infected urban younger and control-matched subjects were not different [12].
Improvement of vitamin D status in HIV-infected patients by vitamin D supplementation has been studied in several clinical trials, with the aim of improving bone metabolism. Vitamin D supplementation does not show side effects on immune parameters as reflected by the absence of significant changes of CD4+ cell count and percentage after one year of vitamin D supplementation [10,149]. On the other side, in the same HIV individuals it was not possible to estimate the effect of vitamin D treatment on virus replication since all individuals were under anti-retroviral therapy [10,149].
More on the topic ENVIRONMENTAL-MEDIATED AVAILABILITY OF VITAMIN D AND IMMUNE FUNCTION:
- ENVIRONMENTAL-MEDIATED AVAILABILITY OF VITAMIN D AND IMMUNE FUNCTION
- 1 Availability of management agreements
- INTERFERENCE WITH THYMIC FUNCTION
- FOREWORD
- Physiological changes to thekidney during healthy pregnancy