Pulmonary Hypertension
GENERAL PRINCIPLES
Definition
Pulmonary hypertension (PH) is defined by sustained elevation of the mean pulmonary artery pressure
(mPAP) to >20 mm Hg (at rest). 1
Classification
• PH is subcategorized into five major groups (Table 10-1):
î Group I—Pulmonary arterial hypertension (PAH)
î Group II—PH due to left heart disease
î Group III—PH due to lung diseases and/or hypoxia
î Group IV—PH due to pulmonary artery obstructions
î Group V—PH with unclear multifactorial mechanisms
• PAH is a specific group of disorders with similar pathologies and clinical presentation, and a high propensity for right heart failure in the absence of elevated left-sided pressures.
î Hemodynamic definition = mPAP > 20 mm Hg, pulmonary artery wedge pressure (PAWP) ≤ 15
mm Hg, and pulmonary vascular resistance (PVR) ≥ 3 Wood units 1
TABLE 10-1
CLINICAL CLASSIFICATION OF PULMONARY HYPERTENSION: DANA POINT (2008) CLASSIFICATION SYSTEM OF PULMONARY HYPERTENSION
Group I: Pulmonary arterial hypertension (PAH)
Idiopathic (IPAH)
Heritable (HPAH)
Drugs and toxin-induced: methamphetamines, fenfluramine, dasatinib
Associated (APAH)
• Connective tissue diseases
• HIV infection
• Portal hypertension
• Congenital heart disease (systemic-to-pulmonary shunt)
• Schistosomiasis
PAH long-term responders to calcium channel blockers
PAH with overt features of venous/capillaries (PVOD/PCH) involvement
Group II: Pulmonary hypertension (PH) due to left heart disease
PH due to heart failure with preserved LVEF
PH due to heart failure with reduced LVEF
Valvular disease
Group III: PH due to lung disease and/or hypoxia
Obstructive lung disease
Restrictive lung disease
Other pulmonary diseases with mixed restrictive and obstructive pattern
Hypoxia without lung disease
Developmental lung disorders
Group IV: PH due to pulmonary artery obstructions
Chronic thromboembolic PH
Other pulmonary artery obstructions
Group V: PH with unclear and/or multifactorial mechanisms
Hematologic disorders: myeloproliferative disorders, hemoglobinopathies
Systemic and metabolic disorders: sarcoidosis, PLCH, LAM, neurofibromatosis, glycogen storage disease, Gaucher disease
Others: tumoral obstruction, fibrosing mediastinitis, chronic renal failure on dialysis
Complex congenital heart disease
LAM, lymphangioleiomyomatosis; LVEF, left ventricular ejection fraction; PCH, pulmonary capillary hemangiomatosis; PLCH, pulmonary Langerhans cell histiocytosis; PVOD, pulmonary veno-occlusive disease.
Epidemiology
• PH is most often due to left heart disease (Group II) or parenchymal lung disease (Group III).
• Prevalence of idiopathic PAH (IPAH) (Group I) is 6-9 cases per million compared with overall PAH prevalence of 15-26 cases per million. 2, 3
î Average age of PAH patients is ~50 years. 2 - 4 IPAH patients tend to be even younger, with a mean age of ~35 years. 5
• IPAH and PAH associated with connective tissue diseases (CTD) are the most common subtypes. 4, 6
• Incidence of chronic thromboembolic pulmonary hypertension (CTEPH) (Group IV) may be as high as 4% among survivors of acute pulmonary embolism. 7
Pathophysiology
• PAH is suspected to develop in susceptible individuals who develop a comorbid condition (e.g., systemic sclerosis or portal hypertension), contract an infection (e.g., HIV), or get exposed to a culpable drug/toxin (e.g., fenfluramine, methamphetamines, or dasatinib).
î Mutations in bone morphogenetic protein receptor II (BMPR-II) gene account for ~70% of heritable PAH (HPAH). 8
î Mutations in the eukaryotic translation initiation factor 2 alpha kinase 4 (EIF2AK4) gene cause PAH with significant venous/capillary involvement (formerly known as pulmonary veno-occlusive disease). 9
î Other susceptibility factors are speculated to exist but have not been identified.
î Comprehensive gene panels are commercially available.
• PAH involves a complex interplay of factors resulting in progressive vascular remodeling with endothelial cell and smooth muscle proliferation, vasoconstriction, and in situ thrombosis at an arteriolar level. Vessel wall changes and luminal narrowing restrict the flow of blood and lead to higher-than-normal pressure as blood flows through the vessels, which is quantifiable by an elevated PVR. 10
î Elevated PVR results in increased afterload for the right ventricle (RV), which increases RV wall tension and work, leading to reduced RV contractility, decreasing cardiac output and progressive exercise intolerance.
° The RV has limited ability to hypertrophy and tolerates high afterload poorly, causing “vascular- ventricular uncoupling” and eventual RV failure and death.
• Mechanisms of PH in Groups II-V vary and include high postcapillary pressures, hypoxemia-mediated vasoconstriction, vascular remodeling, parenchymal destruction, thromboembolic narrowing or occlusion of large arteries, compression of proximal vasculature, and hyperdynamic states leading to increased circulatory flow.
• Combined pre- and postcapillary PH describes situations when multiple conditions lead to elevated pressures in the left-sided heart chambers (postcapillary) and simultaneous abnormalities in the pulmonary arterial side (precapillary).
î Hemodynamic definition = mean PAP > 20 mm Hg, PAWP > 15 mm Hg, and PVR ≥ 3 Wood units 1
Prevention
Yearly screening transthoracic echocardiogram (TTE) is indicated for high-risk groups including individuals with known BMPR-II mutation, scleroderma, portal hypertension undergoing liver transplantation evaluation, and congenital systemic-to-pulmonary shunts (e.g., ventricular septal defects, patent ductus arteriosus).
• More formal screening algorithm for early detection of PAH in scleroderma is available. 11
DIAGNOSIS
Clinical Presentation
• Symptoms include dyspnea (most common), fatigue, palpitations, exertional dizziness, syncope, chest pain, lower extremity swelling, and increased abdominal girth (ascites).
• Explore underlying exposures (i.e., methamphetamines, chemotherapeutic agents) 1 or associated conditions (e.g., CTDs, left-sided cardiac disease, parenchymal lung diseases, obstructive sleep apnea syndrome [OSAS], and venous thromboembolism).
• Auscultatory signs of PH include prominent second heart sound (loud S2) with loud P2 component, RV S3, tricuspid regurgitation, and pulmonary insufficiency murmurs.
• Signs of right heart failure are jugular venous distention, pedal edema, hepatomegaly, pulsatile liver, and ascites.
• Examination findings of underlying conditions linked to PH include skin changes of scleroderma, stigmata of liver disease, clubbing (congenital heart disease), aortic/mitral murmurs, and abnormal breath sounds (parenchymal lung disease).
Diagnostic Testing
• Confirm clinical suspicion and determine etiology of PH, while gauging the severity of the condition.
• Acute illnesses can cause mild elevations of pulmonary artery systolic pressure (PASP) (with nocturnal supplemental oxygen. 17
• Symptoms of sleep-disordered breathing and daytime hypercarbia should be evaluated with polysomnography (PSG).
IMAGING
• CXR:
î Central pulmonary arteries and RV enlargement
î Clues to specific PH diagnosis include the following:
■ Decreased peripheral vascular markings or pruning (PAH)
■ Large pulmonary vasculature throughout lung fields (congenital-to-systemic shunt)
■ Regional oligemia of pulmonary vasculature (chronic thromboembolic disease)
■ Interstitial infiltrates (ILD)
■ Hyperinflated lungs (chronic obstructive lung disease)
• Ventilation-perfusion (V/Q) lung scan:
î Critical for excluding chronic thromboembolic disease but could also be abnormal in PAH with venous/capillary involvement and fibrosing mediastinitis.
î Presence of one or more segmental mismatches should warrant CT angiography or pulmonary angiography. 15
• Chest CT scan:
î Angiogram can confirm CTEPH, if initial screening V/Q scan is suspicious, and also helps determine surgical feasibility; CT should generally not be used to screen for CTEPH.
î High-resolution images to assess for interstitial or bronchiolar disease.
• Pulmonary angiography can be done safely in severe PH and confirms CTEPH and determines surgical feasibility.
• Cardiac MRI:
î Provides RV anatomic and functional information, including ventricular volumes, ejection fraction, and stroke volume index, which have prognostic value.
18î Identifies cardiac anomalies associated with PAH (if TEE contraindicated).
DIAGNOSTIC PROCEDURES
• Lung biopsy is usually prohibited by severe PH or RV dysfunction if present; rarely performed when suspecting PAH associated with venous/capillary involvement.
• Right heart catheterization:
î Esse ntial whe n PAH suspe cte d and pulmonary vasodilators be ing conside re d.
î Confirms PH because TTE can be inaccurate. 19
î Excludes left heart disease by measuring end-expiratory PAWP and systemic-to-pulmonary shunts (by noting “step-up” in oxygen saturations).
■ Measure direct LV end-diastolic pressure if PAWP not reliable, especially in patients older than 65 years.
î Reduced cardiac output and elevated mean right atrial pressure (RAP) are important predictors of mortality.5
î Acute fluid challenge (7 mL/kg over 5 minutes) can unmask LV dysfunction that could be etiology of mild PH. 20
• Acute vasodilator testing recommended when IPAH, HPAH, or drug/toxin-induced PAH suspected, unless extreme right heart failure present (mean RAP > 20 mm Hg).
î Use short-acting vasodilator, such as IV adenosine or inhaled nitric oxide. 21
î Significant response is acute drop in mPAP ≥ 10 mm Hg and concluding mPAP < 40 mm Hg with stable or improved cardiac output. 21
î Only acute responders should receive long-term CCBs (see “Treatment” section).
TREATMENT
• Supplemental oxygen to keep arterial saturations (>89%) to avoid hypoxic vasoconstriction. Normoxemia may not be possible with significant right-to-left intracardiac shunting.
• In-line IV filters to prevent paradoxical air emboli in patients with large right-to-left shunts.
• Deep Valsalva maneuvers raise intrathoracic pressure and reduce central venous return (e.g., vigorous exercise, severe coughing, straining during defecation, or micturition) and high altitudes (>5000 ft) because of low inspired concentration of oxygen.
• Avoid pregnancy because of hemodynamic alterations that further strain the RV
• Pulmonary rehabilitation is recommended for treated PAH patients who remain limited due to physical deconditioning.
• Management of PH depends on the specific category of PH.
î Group II PH should receive appropriate therapy for underlying causative condition with the goal of minimizing postcapillary pressures.
î Group III PH should receive treatment for specific condition, for example, bronchodilators for obstructive lung disease, immunomodulators, or antifibrotics for ILD, noninvasive ventilation for OSAS or obesity hypoventilation syndrome, and supplemental oxygen.
■ Select PH-ILD patients can benefit from the inhaled pulmonary vasodilator, treprostinil.
î CTEPH is usually treated by pulmonary thromboendarterectomy or percutaneous balloon angioplasty at specialized centers and requires careful evaluation to determine best intervention. 22, 23 Inoperable or persistent CTEPH (after intervention) benefit from medical therapy.
Medications
• PAH patients are candidates for vasomodulator/vasodilator therapy (see Table 10-2).
î Four categories of PAH-specific therapies with unique mechanisms of action:
■ Endothelin receptor antagonists block endothelin-1's effect on pulmonary artery smooth muscle cells, thus abrogating vasoconstriction and cellular growth.
TABLE 10-2
Vasomodulatorzvasodilatory therapy for pulmonary arterial
HYPERTENSION
| Drug | Therapeutic | Route | Dosing | Adverse | Cautions | |||||||||||
| Class | of | Range | Effects | |||||||||||||
| Delivery | ||||||||||||||||
| Nifedipine, | Calcium channel | PO | Varies | Peripheral | Use only in | |||||||||||
| amlodipine, diltiazem | blockers | by patient tolerance | edema, hypotension, fatigue | patients who are vasoresponsive during acute vasodilator challenge; avoid if low cardiac output or decompensated right heart failure | ||||||||||||
| Sildenafil Tadalafil | Phosphodiesterase type 5 inhibitor | PO | 20 mg TID 40 mg/d | Headache, hypotension, dyspepsia, myalgias, visual disturbances | Avoid using with nitrates or protease inhibitors | |||||||||||
| Riociguat | Soluble guanylate cyclase stimulator | PO | 2.5 mg TID | Hypotension | Avoid using with nitrates; approved for PAH and CTEPH, i.e., inoperable or persistent after endarterectomy | |||||||||||
| Bosentan | Endothelin receptor antagonist | PO | 125 mg BID | Hepatotoxic, teratogen, peripheral edema | Monthly liver function monitoring; avoid using with glyburide and glipizide | |||||||||||
| Ambrisentan | Endothelin receptor antagonist | PO | 5 10 mg/d | Teratogen, peripheral edema | Fluid retention, particularly in older patients | |||||||||||
| Macitentan | Endothelin receptor antagonist | PO | 10 mg/d | Teratogen, peripheral edema | Monitor for anemia | |||||||||||
| Iloprost Treprostinil | Prostacyclin analogue | IH | 2.5-5 μg 6-8/d ≥9 breaths QID | Cough, flushing, headache, trismus | Suboptimal adherence due to dosing frequency; overnight drug holiday | |||||||||||
| Selexipag | Prostacyclin receptor agonist | PO | 200 1600 μg BID | Headache, jaw pain, diarrhea, extremity pain | Hyperthyroidism | |||||||||||
| Treprostinil | Prostacyclin | SC, IV, | Varies | Headache, | With | |||||||||||
| analogue | or PO | by patient tolerance | jaw pain, diarrhea, extremity pain | continuous parenteral use, catheter-related complications (IV); site pain/reaction (SC); GI distress with PO use | ||||||||||||
| Epoprostenol | Prostacyclin analogue | IV | Varies by patient tolerance | Headache, jaw pain, diarrhea, extremity pain | Continuous parenteral agent; very short half-life; catheter-related complications (IV); high- output state at higher doses | |||||||||||
CTEPH, chronic thromboembolic pulmonary hypertension; GI, gastrointestinal; IH, inhaled; PAH, pulmonary arterial hypertension; PO, oral.
■ Phosphodiesterase 5 inhibitors block enzyme that shuts down nitric oxide-mediated vasodilation.
■ Soluble guanylate cyclase stimulator activates the downstream signal of nitric oxide and induces vasodilation.
■ Prostacyclin pathway activators, including prostacyclin analogues and prostacyclin receptor agonists, induce vasodilation, inhibit cellular growth, and inhibit platelet aggregation.
î Choice of PAH-specific therapy should be individualized by severity of condition based on established risk assessment tools that are available online (see Figure 10-2 and Table 10-3).
■ REVEAL 2.0 and REVEAL Lite calculate a weighted score based on multiple variables (such as PAH subtype, demographics, New York Heart Association [NYHA] functional class, 6MW distance, natriuretic peptides, hemodynamics, vital signs) and determine low, intermediate, or high risk for death. 24, 25
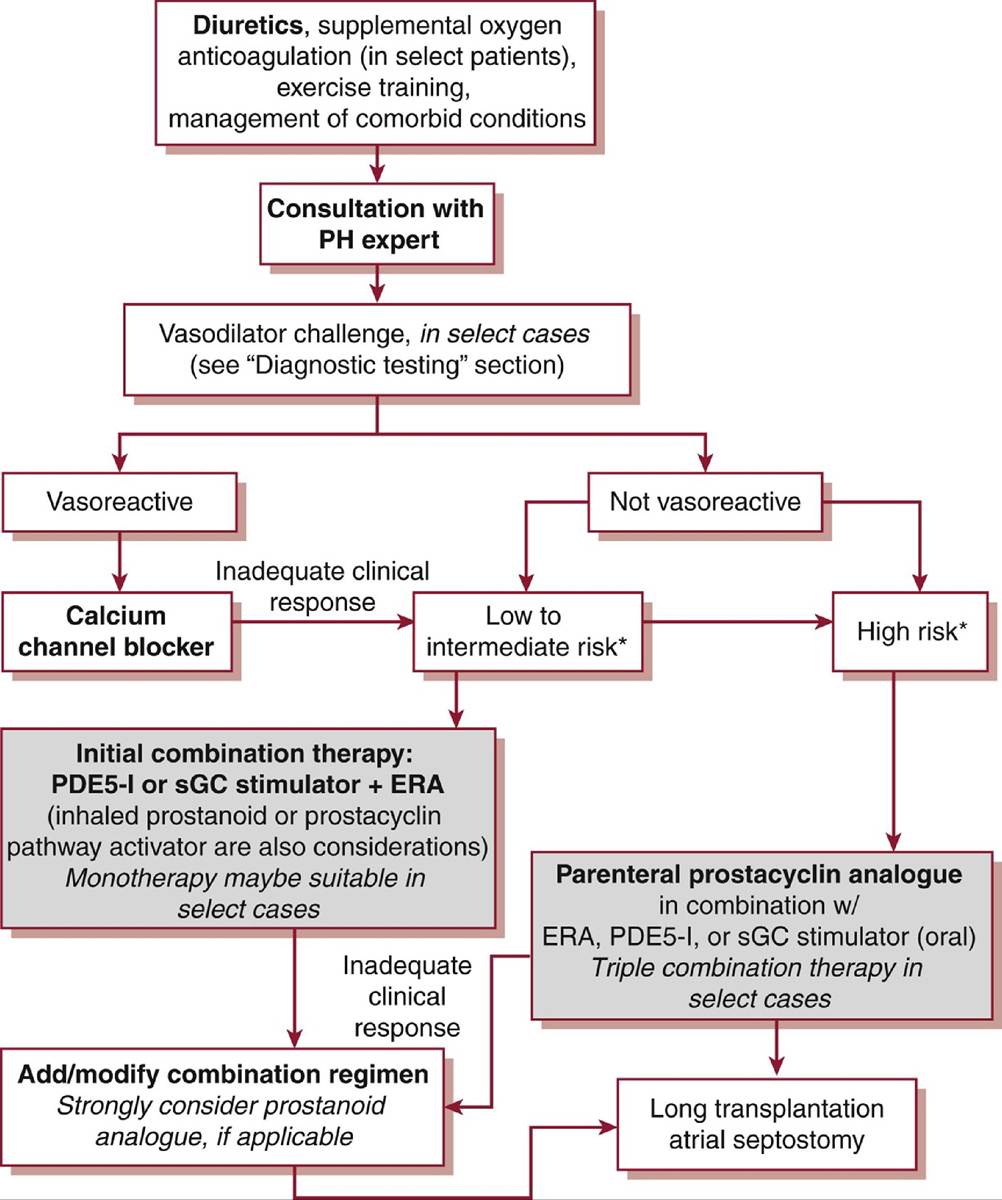
Figure 10-2 Algorithm for management of pulmonary arterial hypertension,ERA, endothelin receptor antagonist; PDE5-I, phosphodiesterase type 5 inhibitor; PH, pulmonary hypertension; sGC, soluble guanylate cyclase. *Risk determined by composite assesment of predictors of survival (see “Treatment” section).
TABLE 10-3
VALIDATED RISK ASSESSMENT TOOLS IN PAH

Hypertension Registry
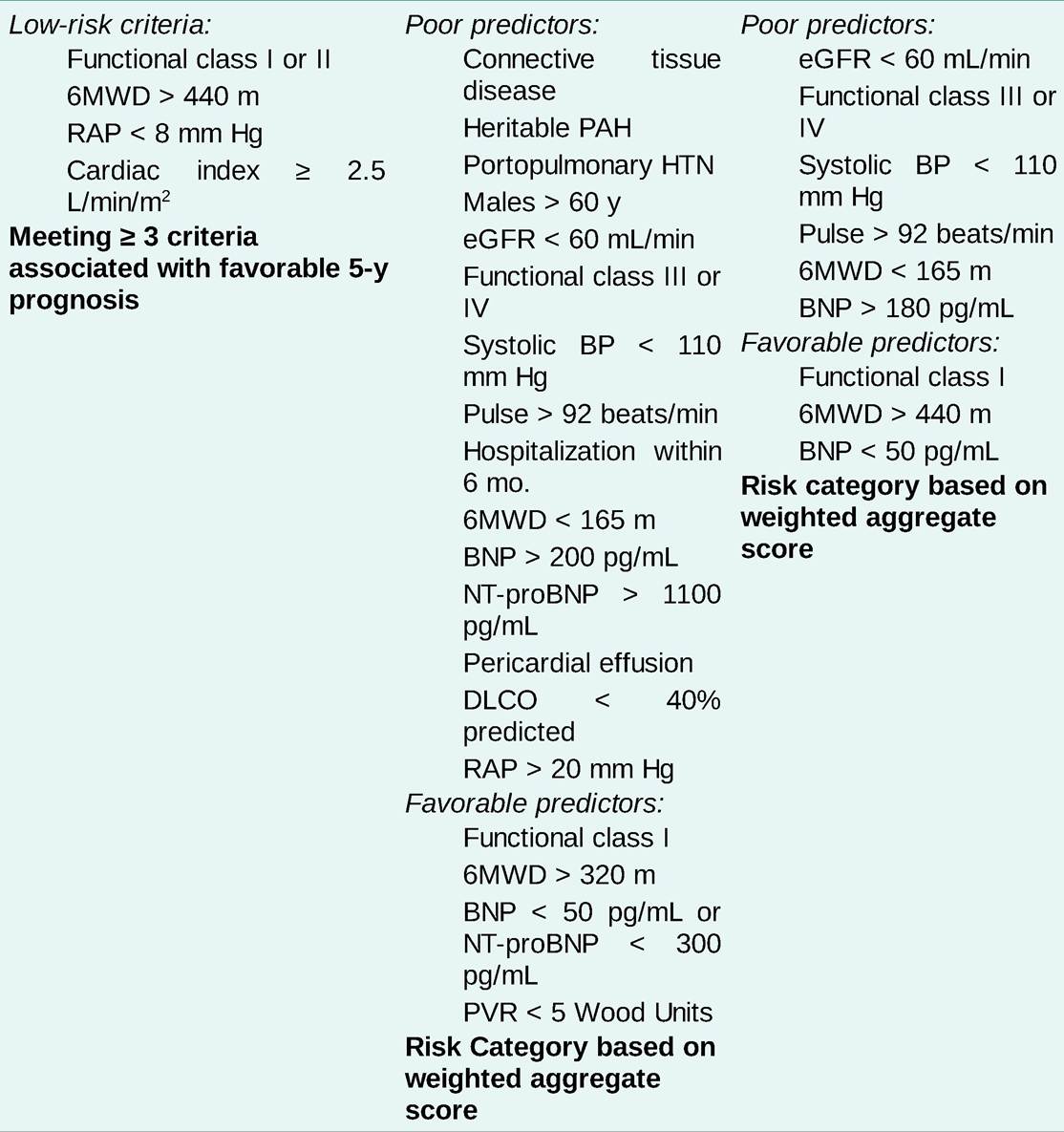
6MWD, six-minute walk distance; BNP, brain natriuretic peptide; BP, blood pressure; DLCO, diffusing capacity for carbon monoxide; eGFR, estimated glomerular filtration rate; HTN, hypertension; NT-proBNP, N-terminal pro b-type natriuretic peptide; PAH, pulmonary arterial hypertension; PVR, pulmonary vascular resistance; RAP, right atrial pressure.
■ French Registry method tallies the number of low-risk characteristics (including NYHA function class I or II, 6MW distance > 440 m, RAP < 8 mm Hg, cardiac index > 2.5 L/min/m2); ≥3 criteria signifies low-risk category and predicts improved survival. 26
î Combination therapy regimens with medications from more than one class of therapy are the preferred approach, even for newly diagnosed patients. 27
■ Because of the complexity of some therapies, an individual's comorbid conditions, cognitive abilities, and psychosocial factors must also be considered.
î Close monitoring and regular risk assessment is needed as deterioration often occurs, requiring alternative/additional medical and possibly surgical intervention.
• Diuretics, often in combination (e.g., loop diuretic + aldosterone antagonist), lessen right heart failure and symptoms.
• Anticoagulation:
î Chronic anticoagulation may improve survival in IPAH, while benefits in other PAH subtypes are unclear. 28, 29
î Warfarin is dosed to target international normalized ratio of 1.5-2.5. 21
î Anticoagulant therapy is not urgent and bridging therapy is unnecessary.
• Inotropes, such as dobutamine and milrinone, are used in extremely decompensated states.
Surgical Management
• Lung transplantation or heart-lung transplantation:
î For PAH patients who remain in advanced functional class III-IV despite maximal medical therapy, which usually includes a parenteral prostanoid.
î Group III PH also impacts timing of transplant in parenchymal lung diseases.
î Because the RV recovers after isolated lung transplantation, heart-lung transplantation is usually reserved for complex congenital heart defects that cannot be repaired.
• Atrial septostomy:
î Palliative right-to-left intracardiac shunt created percutaneously in cases of severe right heart failure (i.e., syncope, hepatic congestion, prerenal azotemia) refractory to medical therapy.
î Despite arterial oxyhemoglobin desaturation and hypoxemia, oxygen delivery increases from improved LV filling and cardiac output.
• Septal defect closure:
° Intracardiac defects with significant net left-to-right shunting can be closed percutaneously or surgically.
î Criteria for closure are evolving and some patients may be candidates after a period of treatment with pulmonary vasodilator therapy. 30
Prognosis
The 1-, 3-, and 5-year survival rates in PAH are 85%, 70%, and 55%, respectively. 31, 32
More on the topic Pulmonary Hypertension:
- Preconceptional evaluation of women with heart disease
- CONGENITAL LUNG MALFORMATIONS
- Lung parenchyma
- Respiratory Failure
- There is a reason why financial technology startups are taking off now instead of 20 years ago.
- Mitral Stenosis
- Macrovascular Complications of Diabetes Mellitus
- 4 Preconception Counseling and Prenatal Care
- Chapter 9 Obstetric conditions