Premature ovarian insufficiency
Premature ovarian insufficiency (POI), previously known as premature ovarian failure, is defined as the loss of normal ovarian function before the age of 40 years. Approximately 1% of women in the United Kingdom will experience an early loss of ovarian function secondary to a number of aetiologies.
About 1 in 1000 women under the age of 30 years, are affected.Causes of POI
There are three main identifiable causes of POI—genetic, autoimmune, or iatrogenic:
• Genetic conditions include a strong maternal family history; 45X, 46XX, and 46XY POI; and POI associated with galactosaemia and FMR1 (fragile X mental retardation 1) gene premutations.
• Women with an autoimmune predisposition may develop autoimmune POI, with or without other autoimmune diseases (diabetes mellitus, Addison's disease, thyroid disease).
• Women with iatrogenic menopause form an increasingly large group. These are women whose treatments for cancer (hormonal, chemotherapy, and/ or radiotherapy) have brought about an earlier menopause.
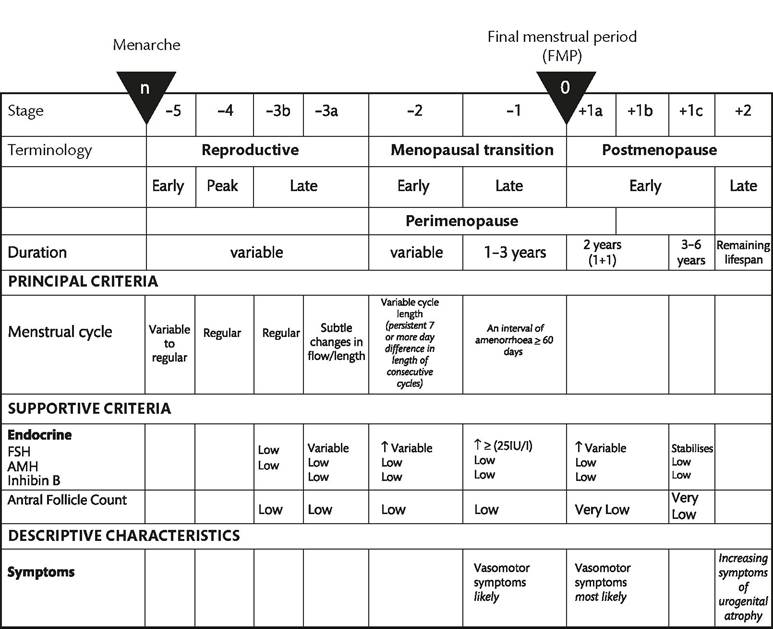
Figure 46.1 The STRAW+10 staging system for reproductive ageing in women.
Reproduced from Executive summary of the Stages of Reproductive Aging Workshop + 10: addressing the unfinished agenda of staging reproductive aging. Harlow SD, Gass M, Hall JE, Lobo R, et al. for the STRAW+10 Collaborative Group. Climacteric 2012;15:105-114.
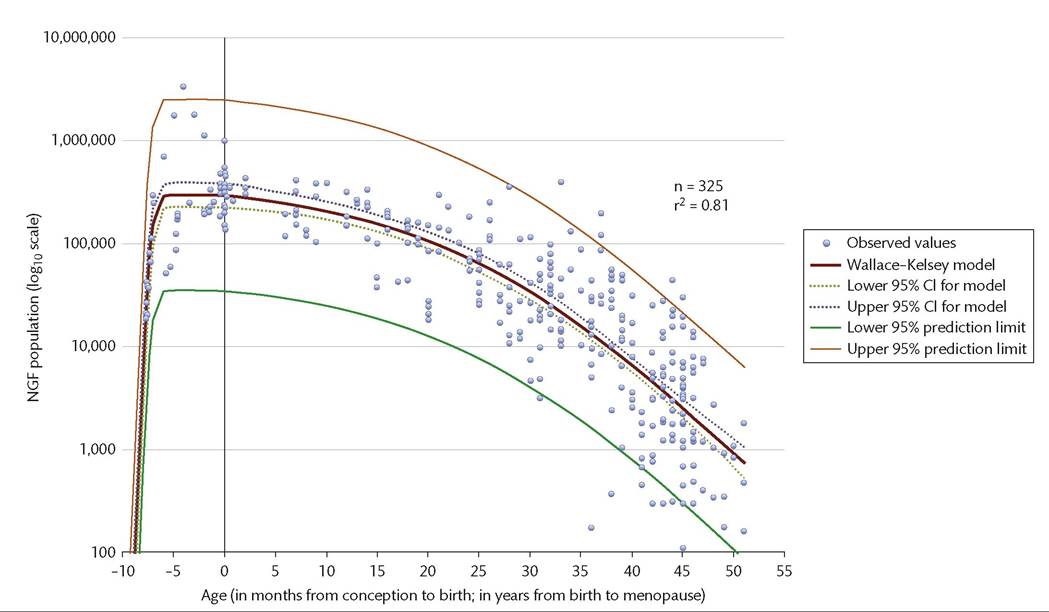
Figure 46.2 The number of non-growing follicles from conception to the menopause.
Reproduced from Wallace WH, Kelsey W. Human ovarian reserve from conception to the menopause. PLoS One 2010;5:e8772.
In most women, the cause of an early menopause is unknown.
POI is associated with decreased bone mass and fractures, an increased risk of premature death from cardiovascular disease, as well as dementia and Parkinsonism (3-5).
There is also fertility compromise associated not only with the loss of ovarian function but, in those with prepubertal POI, inadequate uterine morphology.As well as managing clinical and physical issues, these young women need support and holistic care with a number of psychosocial issues, such as infertility, sexuality, and psychological distress.
Diagnosis of POI
The diagnosis should be based on the presence of menstrual disturbance and biochemical confirmation. Take into account previous medical or surgical treatment, and family history when diagnosing premature ovarian insufficiency.
The European Society for Human Reproduction and Embryology (6) recommend diagnosing premature ovarian insufficiency in women aged under 40 years based on:
• oligo/amenorrhoea for at least 4 months, and
• elevated FSH level greater than 25 IU/L on two occasions more than 4 weeks apart.
Anti-Mullerian hormone testing should not routinely be used to diagnose premature ovarian insufficiency, although this test is widely used in reproductive medicine as a means of assessing the woman's ‘ovarian reserve' and likely response (or lack of it) to gonadotropin stimulation prior to in vitro fertilization.
Management of POI
Treatment should be multidisciplinary, with consideration given to prevention of potential morbidities, reproductive healthcare including fertility and contraception, and the provision of counselling and emotional support. Ideally, these women should be seen in dedicated clinics, with ease of access to a multidisciplinary team.
It is widely accepted that the mainstay of treatment of POI is sex steroid replacement. 17β-oestradiol is preferred to ethinylestradiol or conjugated equine oestrogens for oestrogen replacement (6). Patient preference for route and method of administration of each component of hormonal replacement therapy (HRT) must be considered when prescribing, as should contraceptive needs. About 50% of young women with spontaneous POI experience intermittent and unpredictable ovarian function (7), although there is only a 5-10% chance of spontaneous conception (8). This is vital when considering treatment, as HRT is not a contraceptive, therefore, the combined oral contraceptive pill may be the treatment of choice, rather than HRT. Both provide bone protection, but HRT may provide a beneficial effect on blood pressure compared to the combined oral contraceptive pill (9). Treatment should be continued at least until the average age of menopause.
Concerns regarding the potential risks of using HRT, following the Women's Health Initiative (WHI) and the Million Women Study publications, are not relevant to this group of women since the ovarian failure occurs prematurely and there is no evidence to suggest that risk of breast cancer will exceed that of normally cycling women of similar age.
More on the topic Premature ovarian insufficiency:
- Premature ovarian insufficiency
- REFERENCES
- I AMENORRHEA
- 39 Evaluation of Amenorrhea
- I OSTEOPOROSIS ^470 ^485 ^508 ^571
- Arulkumaran S., Ledger W., Denny L., Doumouchtsis S. (eds.). Oxford Textbook of Obstetrics and Gynaecology. Oxford University Press,2020. — 928 p., 2020
- Chapter 35 Human Sexuality
- Abbreviations