DEVELOPMENTAL SKIN DISORDERS
All children have some or other developmental defects of skin, though most of them are of no clinical consequence. Some benign skin stigmata may point towards the more serious underlying problems due to common embryological insult, e.g.
sacral or spinal dimple (spina bifida occulta), patellar dimple (congenital rubella), loose skin folds over neck (Turner/Noonan syndrome), pre-auricular tags or sinuses (renal anomalies), accessory tragus (Goldenhar syndrome), etc.Some important developmental defects with primary skin involvement are as follows:
Aplasia cutis congenita, i.e. development absence of skin, presents as solitary or multiple, well-demarcated, noninflammatory ulcers or atrophic scars, usually over scalp. Depth of lesion may vary from minimal epidermal loss to deep lesions involving dermis, subcutaneous tissue and rarely, the bone. Most cases are isolated skin defects, thought to be due to intrauterine vascular insult and recover spontaneously. Large or deep lesions may be complicated with hemorrhage, infection or underlying meningitis. Surgical closure is rarely required.
Amniotic constriction bands present as partial grooving or complete amputation of body parts, e.g. limbs or digits, due to premature amniotic rupture following amniocentesis or blunt abdominal injury, leading to entanglement of fetal parts in shrivelled amniotic bands. More severe craniofacial defects, may be caused by vascular disruption due to constriction bands in embryonic life (Fig. 25.2).
Branchial clefts, sinuses or cysts present as lateralized* skin defects or swellings in neck, usually along the tract of second branchial arch. While some lesions are blind, others may open on the skin or in pharynx. Most of these lesions are asymptomatic, till complicated by secondary infections, which should be treated with antibiotics followed by surgical excision.
* Similar neck lesions in mid-line indicate thyroglossal cyst/sinus, which also move with deglutition.
Ectodermal dysplasia is a heterogeneous group of rare hereditary disorders involving almost all ectodermal tissues, e.g. skin, its appendages and teeth. Most cases are characterized by: (a) dry, hyperkeratinized skin,

Fig. 25.2: Amniotic constriction bands.
(b) absence of sweating, (c) hair abnormalities, and (d) abnormal dentition. Three important variants include:
a. Anhidrotic ectodermal dysplasia is an X-linked recessive disorder, with a triad of: (a) partial/complete absence of sweating due to deficiency of eccrine glands, (b) anomalous dentition, e.g. anodontia/ hypodontia with conical teeth, (c) hypotrichosis with sparse hypopigmented hair, eyebrows and eyelashes. These cases present in infancy with hyperpyrexic episodes (poor sweating) and recurrent respiratory infections (paucity of mucus glands), along with typical face (dental/hair abnormalities) and dry- wrinkled skin. Most of them die by 2 years due to hyperpyrexia or respiratory infections.
b. Hidrotic ectodermal dysplasia (Clouston syndrome) is much rare and presents with dystrophic nails, sparse hair and hyperkeratosis of palm/soles; but with normal sweating and dentition.
c. EEC syndrome, an autosomal dominant disorder with variable penetrance, denotes: (a) Ectrodactyly, i.e. spilt hand/feet, (b) Ectodermal dysplasia with dry skin, sparse hair, dysplastic nails, but normal sweating, and
(c) Cleftlip/palate.
Developmental vascular anomalies of skin may be divided into two groups: (a) proliferative hamartomas of vascular endothelium, e.g. hemangioma, and (b) vascular malformations, e.g. salmon patch, port-wine stain, etc. (Fig. 25.3).
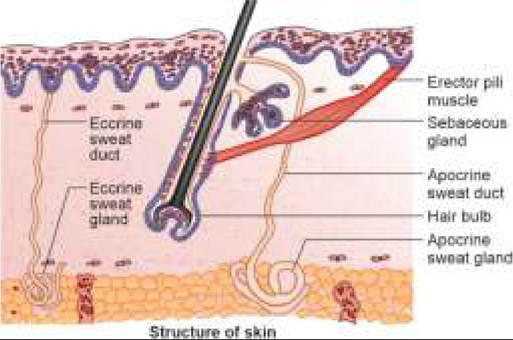
Fig. 25.3: Common hemangiomas in children: (A) Strawberry hemangioma; (B) Port wine stains; (C) Salmon patch; (D) Cavernous hemangioma.
Salmon patch (Stork-bites) are commonest vascular malformations, seen in ~40% newborns. Clinically, these lesions present at birth as small, diffuse, pale-pink telangiectatic macules over face, specially at glabella, upper eyelids and nape of the neck. Salmon patches are usually bilaterally symmetrical and tend to be more prominent during crying. Most of them fade away spontaneously by the end of first year.
Port-wine stains are permanent capillary malformations, presenting at birth as flat, well circumscribed, bright/ dark red macular lesions of variable size, usually in head and neck region. Unlike Salmon patch, port-wine stains are often large, unilateral and do not involute spontaneously. Rather, these lesions become darker and nodular over time. Treatment of choice is laser ablation in early infancy, to prevent accidental bleeding.
Two important syndromes associated with port-wine stains are as follows:
• Sturge-Weber syndrome, i.e. facial port-wine stain with intracranial hemangioma, (Ch 18.14)
• Klippel-Trenaunay-Weber syndrome, i.e. port-wine stain over limbs with underlying bony/soft tissue hypertrophy and venous varicosities.
Infantile (Strawberry) hemangioma is a superficial capillary hemangioma, presenting as bright-red, well- demarcated plaque or nodule over face, scalp or upper chest. Unlike port-wine stains, these lesions are raised above the surface and can be easily blanched on pressure.
These hemangiomas are present at birth or appear soon after, and expand rapidly (and may ulcerate/bleed) during next few months, before entering into a stationary phase and subsequent regression by 5-7 years in most cases.
Considering the benign course, no specific therapy is indicated except in cases with: (a) deep-seated or very large lesions, (b) pressure symptoms affecting vision, feeding or respiration.
Conventional treatment for rapidly proliferating lesions has been oral steroids (Prednisolone 2-3 mg/ kg/d as single morning dose) for 4-6 weeks followed by gradual tapering.
Steroids are postulated to have an inhibitory effect on the production of vascular endothelial growth factor (VEGF) by stem cells. High-dose pulse methylprednisolone IV 30 mg/kg/day infused slowly for 3 days may be used for life-threatening situations, e.g. large hemangioma blocking airways.Oral propranolol (2 mg/kg/day) for 6-9 months is emerging as preferred option in relatively stable cases, which acts by inducing vasoconstriction of feeding vessels as well as inhibition of VGEF production Response is obvious within few days with change of color and softening of lesions.
Other options in non-responders are: (a) intra-lesional steroids, (b) sclerotherapy, (c) surgical excision, and
(d) laser therapy.
Kasabach-Merritt syndrome refers to a large infantile hemangioma with thrombocytopenia, microangiopathic hemolytic anemia and DIC, due to mechanical destruction of blood cells.
Cavernous hemangiomas of skin are deep-seated and ill- defined, appearing as cystic/firm, compressible lesions with normal or bluish overlying skin. These lesions also follow the same course as strawberry hemangiomas (expansion gt; stationary gt; regression). However, considering the proximity with deeper vital structures, treatment with oral steroids (as discussed earlier), sclerotherapy or surgical excision is often required.
Ichthyosis denotes a rare group of hereditary skin disorders, all characterized by abnormal keratinization or cornification of skin, i.e. hyperkeratosis.
Abnormal thickening of S. corneum (N:10-50 mm) and delayed shedding of keratin leads to formation of dry adherent scales, either all over or on selected parts of skin. Apart from cosmetic problems, this horny skin with limited elasticity also affects mobility of underlying structures, e.g. joints and muscles, leading to disfigurement and disabilities in severe cases. Itching may be present.
Ichthyosis is also the part of many autosomal recessive syndromes, e.g. Sjoren-Larson syndrome (with mental retardation and spasticity), Refsum syndrome (with chronic polyneuritis and sensory organ defects) and Rud syndrome ( with mental retardation, sexual infantilism and epilepsy).
Some important types of ichthyosis are as follows: Ichthyosis vulgaris is the commonest (1:300) and mildest ichthyosis with autosomal dominant inheritance. While normal at birth, these cases present in early infancy with dry, rough skin and mildly pruritic scaling, usually limited to extensor aspects of limbs (Fig. 25.4).
Lesions are more pronounced in winter season and tend to improve or disappear with age. Scaling may be diminished by use of bath oils and application of an
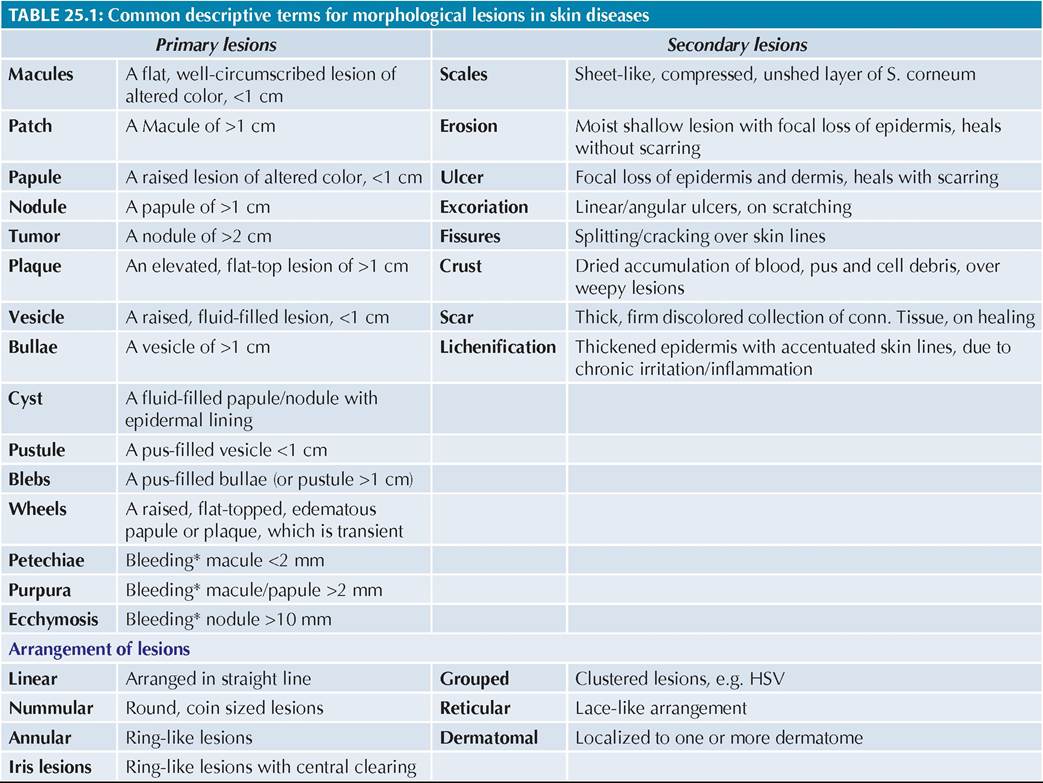
Fig. 25.4: Ichthyosis.
emollient/lubricant with a keratolytic agent, e.g. salicylic acid.
X-linked ichthyosis due to steroid sulfatase deficiency, is seen only in males and present at 3-6 months with development of large dark-brown scales all over body, sparing palms and soles. Corneal opacities are common. Harlequin fetus, most severe autosomal recessive ichthyosis is obvious at birth with marked thickening and cracking of skin, which covers the baby with horny plates and leads to severe disfigurement, e.g. ectropion, flat facial contour, limited joint mobility and breathing difficulties due to poor stretchability of skin. Most cases die in neonatal period/early infancy due to respiratory problems or excessive fluid loss from breaks in stratum corneum.
Collodion baby is an at-birth manifestation of many forms of ichthyosis (commonest lamellar ichthyosis).
Clinically, these newborns are covered with a thick, taut and oily-parchment like membrane (collodion) at birth, which deforms the face with ectropion, flattened nose/ears and fixed lips with open mouth. Membrane cracks with initial respiratory efforts and sheds in large sheets, revealing underlying ichthyotic (or rarely normal) skin.
Management includes nursing in high humidity environment and topical application of lubricants to facilitate membrane shedding and correction of complications, e.g. dehydration, dyselectrolytemia, aspiration and hypothermia.
Many collodion babies die in neonatal period due to aspiration of membranous material, hypothermia or dehydration (due to altered skin permeability), though final prognosis depends on the type of ichthyosis.
Ehlers-Danlos syndrome is a group of genetically inherited connective-tissue disorders, all characterised by quantitative deficiency of collagen. Depending on mode of inheritance and clinical presentation, 10 different types are known, with all or some of the following features:
a. Hyperelasticity, fragility and easy bruisability of skin.
These cases may develop large ecchymosis and gaping ulcerations after trivial trauma, which heal with difficulty, leaving large scars and keloids.
b. Hypermobility of joints (hyper-gymnasts).
c. Systemic manifestations due to defective collagen, e.g. aneurysms, internal organ ruptures (intestines/ bladder), corneal rupture, fragile bones, etc.
Most of these disorders are not fatal but morbidity may be high. Treatment is non-specific including avoidance of trauma, pregnancy (risk of uterine rupture) and surgical procedures (risk of wound dehiscence). Oral ascorbic acid (vitamin C) may be useful in some cases.
Cutis laxa is a congenital disorder of probably dermal elastin, characterized by marked laxity (but not elasticity)
of skin. Depending on the severity of defect, these cases present with:
a. Premature sagging of facial skin or loose skin folds hanging from face and neck ((senile or blood-hound appearance). Unlike Ehlers-Danlos syndrome, skin elasticity is normal.
b. Systemic manifestations, e.g. hoarse cry (vocal cord laxity), multiple hernia, rectal prolapse, recurrent emphysema and cardiac lesions, e.g. valvular dila- tation/regurgitation. Most cases also have growth retardation, sexual infantilism and ligamentous laxity. While some cases manifest at birth, others present
later after febrile illnesses or allergic/inflammatory skin disorders (acquired cutis laxa). Life span may be shortened by systemic complications.
Pseudoxanthoma elasticum is a multi-systemic disorder of elastic tissue due to a genetic defect with abnormal glycosaminoglycan deposition over elastic fibers, predominantly affecting skin, eyes and vascular system.
Clinically, skin manifestations begin in childhood with characteristic linear/reticular confluent plaques of tiny yellow papules (plucked chicken-skin appearance), over flexural regions, e.g. neck, axilla, inguinal folds and antecubital fossa. Gradually, skin may acquire velvety texture and droops in lax, inelastic folds. Mucus membranes may be involved. Involvement of vascular connective tissue may cause cerebral/coronary occlusions in adulthood.
25.3
More on the topic DEVELOPMENTAL SKIN DISORDERS:
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- Skin, Soft-Tissue, and Bone Infections Purulent Skin and Soft-Tissue Infections (Furuncles, Carbuncles, Abscesses)
- ECZEMATOUS SKIN DISORDERS
- Disorders of Skin
- CASE 211: Motives and Reasons
- Physical Examination