EVALUATION IN RENAL DISEASE
Etiology of renal disease in childhood varies according to the age. While congenital malformations are commonest renal/urinary tract problems in newborns and infancy, older children usually present with acquired problems, e.g.
nephrotic syndrome, acute glomerulonephritis and UTI.Common clinical indicators of renal/urinary tract disease are:
• Urinary abnormalities, e.g. abnormal color (hematuria, pyuria) or abnormal volume of urine, e.g. (anuria/ oliguria or polyuria).
• Micturation abnormalities, e.g. dysuria, frequency, incontinence or secondary enuresis, retention or weak stream of urine, etc.
• Local abnormalities, e.g. lumbar abdominal mass, ureteric colic, etc.
• Systemic abnormalities, e.g. edema, hypertension, growth failure, acidosis, etc. Renal edema is soft and pitting, typically prominent: (a) over face and periorbital region, and (b) during mornings.
Laboratory evaluation in a renal disease depends on probable etiology, though some important and specific investigations in nephrology are discussed here.
Urine examination is considered as the window of renal disease. A freshly voided sample should be used within one hour of collection to avoid misleading results, due to disintegration of formed elements, e.g. cells and bacterial overgrowth. If delay is unavoidable, urine can be stored at 4°C in refrigerator after adding a few drops of acetic acid. Early morning sample is preferred as it is most concentrated and has a lower pH that preserves the formed elements.
Collection of urine sample: Mid-stream clean-catch collection is the most widely used method for this purpose in toilet-trained children. While collections from adhesive urine bags or condom-catheters may be used for biochemical studies, these urine samples are unsuitable for microbial studies due to frequent contamination. Collection of sterile sample in younger children requires either urinary catheterization or suprapubic puncture.
Suprapubic puncture is the safe and reliable method to obtain uncontaminated urine sample in infants (Ch 32.6). Important components of urine examination are as follows:I. Gross examination for:
• Quantity: A normal child passes ~2-3 ml of urine/kg/ hr. Anuria (complete cessation of urine) or Oliguria (lt;1 ml/kg/hr or 500 ml/1.73 m2/day) indicates renal failure or obstructive uropathy. Polyuria (gt;4 ml/kg/hr) may be due to functional polydipsia or pathological, e.g. diabetes insipidus, chronic renal failure and renal tubular acidosis.
• Color: Urine is normally pale yellow in color, due to presence of urobilin and urochromes. Common color abnormalities include:
- Dark-yellow, due to concentrated urine, caro- tenemia, icterus, etc.
- Red (cola-color) due to: (a) hematuria (b) hemoglobinuria, (c) myoglobinuria, (d) porphyria, or (e) ingestion of drugs, e.g. rifampicin, beet-root of food dyes.
- Black, in severe hemolysis, e.g. black-water fever, or alkaptonuria
- Cloudy, due to heavy pyuria or phosphaturia.
• Odor: Fresh urine has a slightly aromatic odor, which changes to strong ammoniacal smell on standing, due to decomposition of urea into ammonia. A strong fruity-odor indicates presence of ketone bodies.
• Reaction: Freshly voided urine is acidic (normal pH: 6.0-6.5) due to presence of weak organic acids; but turns alkaline on standing due to formation of ammonia. Alkaline pH of fresh urine indicates UTI due to proteus organisms.
• Specific gravity (Normal: 1.003-1.030) is tested by floating a urinometer in a glass cylinder, 3#8725;4th full of urine sample. Dependent on the solute-load, urinary specific gravity is decreased in diabetes insipidus and increased in proteinuria, glucosuria or high- solute excretion. In end-stage renal disease, it may be constant at 1.010, due to loss of concentration capacity.
II. Biochemical examination for:
• Proteins: Normal child does not excrete more than 150 mg of proteins in urine per day, which include low molecular weight tubular proteins, e.g.
Tamm- Horsfal proteins (No albumin). Significant proteinuria is defined as the urinary protein excretion exceeding 150 mg/day (gt;100 mg/m2/day), which may be qualitatively detected by heat coagulation test, sulphosalicylic acid test or dipsticks or quantitatively by Esbach's method.Heat coagulation test: Take ~10 ml of urine in a test tube and heat the upper column. Appearance of turbidity indicates either phosphaturia or albuminuria. Add 2-3 drops of 10% acetic acid. Disappearance of turbidity indicates phosphaturia that persists in proteinuria. Severity of proteinuria may be graded by visibility of printed-paper through turbid solution (Table 21.1).
Sulfosalicylic acid test: Take ~5 ml of urine and add 5 drops of 10% sulfosalicylic acid. Allow the sample to stand for 5-10 minutes. Turbidity indicates proteinuria, which can be graded as in Table 21.1.
Dipstick method uses special reagent strips, impregnated with tetrabromophenol blue buffered with citrate. When dipped in urine, proteins bind the strip-dye to change its color from yellow to green, which is then compared with color code pasted on the container for semiquantitative values. Proteinuria other than the albuminuria is not detected on dipstick method.
Note: Heat coagulation, sulfosalicylic or dipstick tests may be false-positive in presence of concentrated or alkaline urine, gross hematuria or drugs, e.g. penicillin; or false-negative in diluted urine sample.
Es bach's method is used for quantitative estimation of urine proteins. Esbach's albuminometer is filled with urine sample (acidified and diluted to sp. gravity lt;1.010) till mark 'U', and then topped by Esbach's reagent till mark 'R'. Albuminometer tube is then corked and allowed to stand for proteins to settle down. Height of the precipitate after 24 hours indicates protein excretion in gm/L. 24-hour urinary protein excretion may then be calculated by multiplying this gm/L value with 24-hour urine output.
• Glucose (sugar): Glucosuria indicates diabetes melli- tus or lower renal threshold for glucose excretion (Normal:180 mg/dl), e.g.
in renal tubular acidosis. Its presence is generally tested by Benedict test or dipsticks.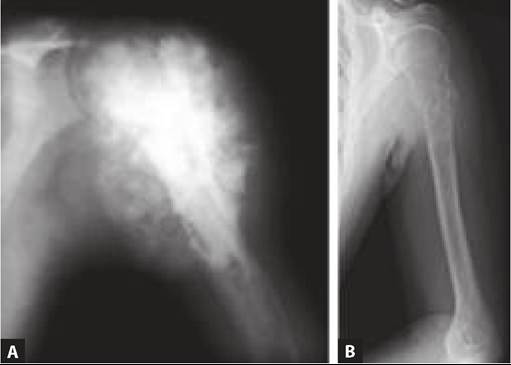
**Place a lined paper behind the tube and look though it.
Benedict test: Add 8 drops of freshly voided urine in 5 ml of Benedict's reagent (alkaline CuSO4 solution). Boil the mixture for 2 minutes to note the color change, if any. Presence of sugar in urine reduces blue CuSO4 into insoluble yellow Cu2O. Results are graded as-1+ (cloudy) green, 2+ (yellow), 3+ (orange) and 4+ (brick red). Benedict test may be false-positive in presence of other reducing substances, e.g. lactose, fructose, etc. or drugs, e.g. salicylates, vitamin C, etc.
Dipstick uses a cellulose strip impregnated with glucose oxidase, peroxidase and ortho-toluidine. When dipped into glucose positive urine for 30 seconds, color changes to blue due to oxidation of glucose in urine and release of H2O2.
• Ketones (acetoacetate, #946;-hydroxybutrate) are intermediate products of fat metabolism. Ketonuria is commonly seen in diabetes mellitus or starvation, which may be detected by Rothera's test or Gerhardt test.
Rothera's test: Saturate 5 ml of urine with ammonium sulfate in a test-tube and add 1 crystal of sodium nitroprusside. When liquor ammonia is added via the side of the tube, a violet color develops at the junction, suggesitve of ketonuria.
Gerhardt test: Add 10% ferric chloride solution (drop-by-drop) in 5 ml urine, till a precipitate forms. Filter the solution and add more ferric chloride to the filtrate. Development of brownish- red color indicates presence of ketones or salicylates, which may be differentiated by using a boiled sample. Negative test with boiled urine indicates ketonuria, which remains positive in salicylaturia.
• Bile pigments are present in urine during hepatic disorders and tested by Fouchet test, Foam test or Gmelin test.
Fouchet test: Add 2.5 ml of BaCl2 in 5 ml of fresh urine and filter. Drip 1-2 drops of Fouchet's reagent over filtered precipitate. A green or blue color indicates presence of bile pigments.
Foam test: Shake 10 ml of urine in a test-tube vigorously. Development of yellow foam on the top indicates presence of bile pigments.
Gmelin test: Add equal volume of urine gradually into frac12; inch column of yellow nitric acid in a test-tube. Appearance of a green band/ring at the junction indicates presence of bile pigments.
• Bile salts are also present in liver diseases and tested by Hay's sulfur test.
Hay's sulfur test: Sprinkle a pinch of sulfur powder over the urine sample in a test tube. Sinking of sulfur particles indicate reduced surface tension of urine due to presence of bile salts.
• Blood: Presence of hematuria or hemoglobinuria is biochemically detected by Benzidine test or Dipsticks. Benzidine test: Mix 2-3 ml of saturated benzidine solution (in glacial acetic acid) with equal volume of urine and add H2O2 to mixture. Development of blue color indicates presence of blood.
Dipstick test: When a reagent-coated cellulose strip is dipped into urine, chromogen is oxidized to give a green-blue color due to pseudoperoxidase activity of hemoglobin.
III. Microscopic examination: 10-15 ml of urine is centrifuged at the rate of 3000 rpm for 5 minutes and
supernatant is poured-off. Concentrated sediment is then examined microscopically for following cellular elements:
• RBCs appear as small, refractile, non-nucleated bodies. Presence of gt;5 RBCs/hpf in centrifuged urine or gt;1-2 RBCs in uncentrifuged sample indicates significant hematuria.
• Leukocytes appear as bigger and nucleated bodies. Isolated presence of leukocytes is insignificant but presence of gt;5 WBCs/hpf along with bacteriuria suggests UTI. Most of these leukocytes are polymorphs. Presence of eosinophils in urine on Hansel's staining sample suggests allergic interstitial nephritis.
RBCs appear dysmorphic in glomerular lesions.• Epithelial cells originate in renal tubules or lower urinary tract and appear as large polygonal and mononuclear cells. Presence of large number of epithelial cells in urine indicates tubular injury.
• Bacterial contamination is common in wrongly collected or stale urine sample. However, presence of even a single bacteria/hpf in fresh uncentrifuged urine from suprapubic collection indicates significant bacteriuria.
• Casts are formed in distal tubules and collecting ducts due to coagulation of albuminous material or embedding of degenerated cells in a matrix of tubular (Tamm-Harsfall) proteins. Usually cylindrical in shape, casts may be further classified according to composition as-RBC casts in glomerular hematuria, WBC casts (pus cells) in upper UTI, epithelial casts in tubular disease, fatty casts in nephrotic syndrome, Granular casts suggestive of disintegrated cells in matrix and hyaline (waxy) casts, suggestive of coagulated protein matrix alone without cellular component. Hyaline and granular casts are normally present in urine but increased in fever, after exercise and heavy proteinuria, e.g. nephrotic syndrome.
• Crystals, suggestive of urolithiasis, are occasionally also present in normal urine and may be made up of-oxalates (prism or dumb-bell shaped), phosphates (envelope shaped), uric acid/urates (orange or reddish spikes), cystine (refractile hexagons), etc.
IV. Microbiological studies: A fresh uncontaminated urine sample is essential for microbiological cultures, best obtained by supra-pubic puncture or urinary catheterization. However, a clean-catch mid-stream sample is adequate in older children, if collected properly. Presence of any growth from supra-pubic sample is significant, while a colony count of gt;105 organisms/ ml is considered as diagnostic of UTI on midstream/catheter sample (Ch 21.15).
Renal imaging studies are indicated to identify anatomical renal/urinary tract abnormalities as well as to assess the excretory function.
Plain X-rays of KUB region are of limited value in renal disease, mainly used to detect renal calculi. However, relevant X-rays may be useful to detect co-existing spinal pathology in neurogenic bladder or metastatic bone disease with osteodystrophy or positioning of various catheters and stents.
Intravenous pyelography (IVP) is rarely used now a days to assess renal anatomy and excretory function. After IV injection of an ionic contrast material, e.g. urografin or conray (tri-iodinated benzoic acid compounds), serial films are taken at 1-5 minutes (for renal perfusion), 15 minutes (for renal excretion) and 1-3 hours (for lower urinary tract). IVP is not very useful in newborns due to their inability to concentrate the contrast medium or in chronic kidney disease.
Ultrasonography (USG) is the most widely used imaging investigation in urinary tract disorders to detect—(a) anatomical abnormalities, e.g., congenital anomalies, hydronephrosis, tumors, etc., (b) medical renal diseases, indicated by loss of cortico-medullary differentiation (normally, cortex is less echogenic than medulla), (c) vascular abnormalities by color Doppler studies, and (d) pre-biopsy localization of kidney. Prenatal USG is very useful to detect urinary tract abnormalities in fetus. Micturating cystourethrogram (MCU) is indicated in a suspected case of vesicoureteric reflux or lower urinary tract abnormalities. It involves introduction of contrast dye into bladder via a catheter or suprapubic puncture, followed by films taken during actual voiding. Oblique and lateral films are needed to detect posterior urethral values.
CT/MRI studies are selectively used to delineate: (a) anatomical abnormalities, (b) mass lesions, e.g. tumors, abscesses or hematomas, and (c) non-functioning kidney. Radionuclide imaging (renal scan) are rapidly replacing conventional contrast studies, e.g. IVP, in functional evaluation of urinary tract. Common types of renal scans used in practice are:
• DTPA (99mTc DTPA) or (99mTcMAG-3) scan for dynamic evaluation of excretory functions, as these agents are rapidly filtered and excreted in urine. This scan is especially useful to detect obstructive urinary tract lesions and renovascular abnormalities.
• DMSA (99mTc) scan for static structural evaluation of renal parenchyma, as this agent is sufficiently concentrated in renal tubular cells and very slowly excreted in urine. It is especially useful to diagnose structural abnormalities and cortical scarring.
Renal function tests include tests for assessment of: (a) glomerular filtration (b) renal blood flow, (c) concentration capacity, (d) urinary acidification capability, and (d) other functions.
• Glomerular filtration is assessed by direct calculation of GFR or indirectly by rise in blood urea and serum creatinine levels.
- Glomerular filtration rate (GFR) is measured by calculating the urinary clearance rate of a substance, which is freely filtered from glomeruli but neither reabsorbed nor secreted from tubules, e.g. inulinlt; a fructose polymer.
However in practice, GFR (ml/min/1.73m2) is usually estimated by Schwartz formula using serum creatinine and height values, as follows:
GFR = K x height in cm/serum creatinine in mg/dl
Whereas K is 0.33 in infants with birth wt lt; 2.5 kg, 0.45 in infants, 0.55 in older children and adolescent girls and 0.70 in adolescent boys.
Normal GFR increases with age from ~20-30/ min/1.73 m2 at birth to ~120 ml/min/1.73 m2 in adults.
- Blood urea nitrogen (BUN) (N: 20-40 mg/dl) is a widely used indicator of glomerular function, though it becomes abnormal only when gt;75% of renal function is lost. Urea is synthesized in liver from ammonia-an excretory product of protein catabolism.
Apart from glomerular diseases, BUN may also be increased due to: (a) increased protein absorption after GIT bleeds, (b) excessive endogenous protein breakdown in hypercatabolic states, muscle trauma or steroid therapy, (c) decreased renal blood flow, e.g. dehydration, shock, etc. BUN levels are reduced in low protein intake and severe liver disorders.
- Serum creatinine (N: 0.4-0.8 mg/dl): Creatinine is produced endogenously at a near-constant rate by the metabolism of creatine and phosphocreatine in muscles. As its excretion doesn't depend of pre- renal factors (except muscle mass), serum creatinine is a better indicator of GFR than BUN, specially in early renal disease with limited loss of glomerular function. Creatinine levels are also used to adjust drugs dosages in renal failure. Serum creatinine may be falsely low in cases with severe muscle wasting, e.g. malnutrition.
• Renal blood flow (N: 500-600 ml/min), although rarely indicated in clinical practice, is measured by assessing the plasma clearance rate of substances, which are completely filtered during the first passage through the kidney, e.g. para-aminohippurate (PAH) or 99mTc MAG-3.
• Urinary concentration capacity is measured as urinary osmolality after standard water deprivation test. After overnight water deprivation, a normal child can concentrate the urine gt;900 mOsm/kg. Inability to concentrate gt;300-500 mOsm/kg indicates possibility of central or nephrogenic diabetes insipidus, which may be further differentiated by vasopressin challenge test (Ch 22.2.4). Substantial improvement in concentration capacity after nasal/IM desmopressin (DDAVP) indicates central diabetes insipidus, while failure to do so indicates nephrogenic disease.
• Urinary acidification capacity is impaired in tubular disorders and is assessed by urine acidification tests, e.g. ammonium chloride loading test, i.e. oral administration of NH4Cl (0.1-0.15 g/kg) to achieve systemic acidosis, followed by pH estimation of all urine samples passed over next 6 hours.
Renal biopsy, being an invasive procedure, is indicated only in select cases with unexplained renal disease, where precise diagnosis is essential for therapy/prognosis.
Indications for renal biopsy generally include: (a) steroid-resistant nephrotic syndrome, (b) progressive renal failure, (c) unexplained persistent hematuria or proteinuria, (d) suspected inherited/metabolic renal disease, (e) follow-up in chronic renal disease or renal transplant.
Procedurally, a Vim-Silverman needle with Franklin modification or tru-cut needle is used for renal biopsy after USG localization of kidney (Ch 32.6). Obtained material should be sent for routine microscopy (in formalin), electron microscopy (in glutaraldehyde) and immuno-fluorescent studies (in saline). A specimen is considered adequate if it contains gt;10 glomeruli on light microscopy.
Contraindications for renal biopsy include: (a) solitary functioning kidney, (b) ectopic kidney, (c) bleeding diathesis, (d) severe acute renal failure, and (e) severe hypertension.
Complications: While transient hematuria up to 48 hours is inevitable after renal biopsy, significant complications develop in ~10% cases, including: (a) gross/persistent hematuria, (b) perirenal hematoma, and (c) infection. Complete bed rest and BP/output monitoring is essential for first 24 hours after biopsy, to detect complications.
21.3
More on the topic EVALUATION IN RENAL DISEASE:
- CLINICAL EVALUATION OF GIT DISEASE
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- Macrovascular Complications of Diabetes Mellitus
- 4 Preconception Counseling and Prenatal Care
- ACUTE KIDNEY INJURY
- 3 Critical Care
- Nausea and Vomiting
- Chapter 22 Cardiovascular and Respiratory Disorders
- CHAPTER 41 HARMFUL ALGAL BLOOMS INCLUDING Cyanobacterial toxicosis
- 22 Hepatic lipidosis in a cat