HYDROCEPHALUS
Hydrocephalus is defined as enlargement of the ventricular system of the brain, due to an imbalance between production and absorption of the CSF.
CSF physiology: The normal volume of CSF is ~50 ml in infancy and ~150 ml in adults, which is in a state of dynamic equilibrium, i.e.
formed and absorbed at the rate of ~20 ml/hour.CSF is an active ultrafiltrate of plasma, mainly formed within cerebral ventricular system by the choroid plexus of lateral, third and fourth ventricle, under neurogenic and autonomic control. Adrenergic and cholinergic stimuli decrease or increase CSF production, respectively. Extrachorial CSF production (lt;30%) occurs in subarachnoid space and through capillary endothelium in brain parenchyma.
CSF flows forward due to a pressure gradient between intraventricular space (150 mm H2O) and superior sagital sinus (90 mm H2O). After formation, CSF flows from the lateral ventricle through the foramina of Monro into the third ventricle and then through the narrow aqueduct of Sylvius into the fourth ventricle, where it exits the ventricular system via paired foramina of Luschka and midline foramina of Magendie, to enter in subarachnoid cisterns. In subarachnoid space, CSF baths cerebral convexities before absorption mainly by sub-arachnoid villi and minimally by lymphatic channels, nerve root sheaths (Schwann space) and choroid plexus itself. The spinal subarachnoid space communicates with the intracranial subarachnoid space by basal cisterns (Fig. 18.7).
Pathogenesis: Hydrocephalus may be caused by:
• Increased production of CSF, e.g. choroid plexus papilloma.

Fig. 18.7: Normal CSF flow.
• Obstruction to CSF pathway within ventricular system, i.e. obstructive hydrocephalus.
• Obliteration of the subarachnoid cisterns or malfunction of the arachnoid villi, i.e.
communicating hydrocephalus.• Dilatation of ventricles with normal or even low CSF pressure is rarely seen in neurodegenerative disorders or cortical atrophy (low-pressure hydrocephalus).
Etiology: Hydrocephalus may be congenital or acquired (Table 18.26). Some common causes are as follows:
Congenital aqueduct stenosis, i.e. branching or forking of the aqueduct between III and IV ventricle, is the commonest cause of congenital hydrocephalus. It is usually caused by intrauterine viral infections (specially mumps), though few cases are inherited (X-recessive) or associated with neural tube defects/neurofibromatosis. Aqueduct stenosis may be rarely acquired following post-meningitic or post-hemorrhagic gliosis.
Dandy-Walker malformation is characterized by cystic dilation of the IV ventricle and hydrocephalus due to atresia of the foramina of Lushka and Magendie. Agenesis of cerebellar vermis and corpus callosum is frequently associated. Large head with prominent occiput and positive transillumination test on skull are highly suggestive of Dandy-Walker malformation.
Arnold-Chiari malformation, a common cause of congenital hydrocephalus, is of two types:
a. Type II is characterized by—(a) elongation of fourth ventricle, (b) kinking of brainstem, and (c) displacement of inferior vermis, pons and medulla into cervical canal leading to obstruction of subarachnoid pathways and hydrocephalus. Usually associated with myelomeningocele, these cases presents with progressive hydrocephalus in infancy.
b. Type I is less severe, characterized by downward displacement of cerebellar tonsils into cervical
TABLE 18.26: Common causes of hydrocephalus
Congenital
• Congenital aqueduct stenosis
• Arnold-Chiari malformations type I and II
• Dandy-Walker malformation
• Vein of Galen malformation
Acquired
• Post-infectious—meningitis, intrauterine infections
• ICSOL—tumors, tuberculoma, hematoma
• Subarachnoid hemorrhage
• Achondroplasia
• Pseudotumor cerebri, e.g.
hypervitaminosis A• #8593;CSFproduction, e.g. choroid plexus papilloma
canal and usually presents with headache, neck pain, bladder involvement and progressive spastic paraplegia in older children or adults.
Post-inflammatory exudates in meningitis are commonest causes of communicating/acquired hydrocephalus.
Hydrocephalus in Hurler syndrome is due to fibroid tissue proliferation in the subarachnoid spaces, while in achondroplasia, it is due to underdeveloped occipital skull and posterior fossa (platybasia).
Clinical manifestations of hydrocephalus depend on the severity of obstruction and rate of rise in ICP. While few cases are asymptomatic due to slower accumulation of CSF, a typical case presents with:
• Progressive enlargement of head is the most prominent sign of hydrocephalus in infancy before sutural closure, with bulging anterior fontanel, widening of sutures, dilated veins over scalp, prominent forehead and downward deviation of eyes, i.e. Sunset sign (Fig. 18.8). Skull may be translucent in severe hydrocephalus with cortical thinning, e.g. Dandy-Walker malformation. Macewan sign, i.e. a cracked-pot sound on percussion of skull, indicates sutural separation in older children, though it is of no diagnostic value in infants with open anterior fontanels. Head size may be normal in mild or early hydrocephalus, developing after the developmental closure of skull sutures.
• Raised intracranial pressure (ICP) with headache, irritability, vomiting, papilledema and diplopia. Papilledema may not be obvious in infancy as raised ICP is released outwards due to open sutures. Optic atrophy due to compression of optic nerve/chiasma may develop in untreated cases. Systemic indicators of raised ICP include bradycardia, hypertension and irregular respiration, due to brain-stem compression or autonomic disturbances.
Pyramidal tract involvement, e.g. spastic paraplegia is common, due to stretching and disruption of the corticospinal fibers, passing in vicinity of dilated lateral ventricles.
Gradual change in personality and deterioration in academic achievement might be an early indicator of slowly progressive hydrocephalus with raised ICP.
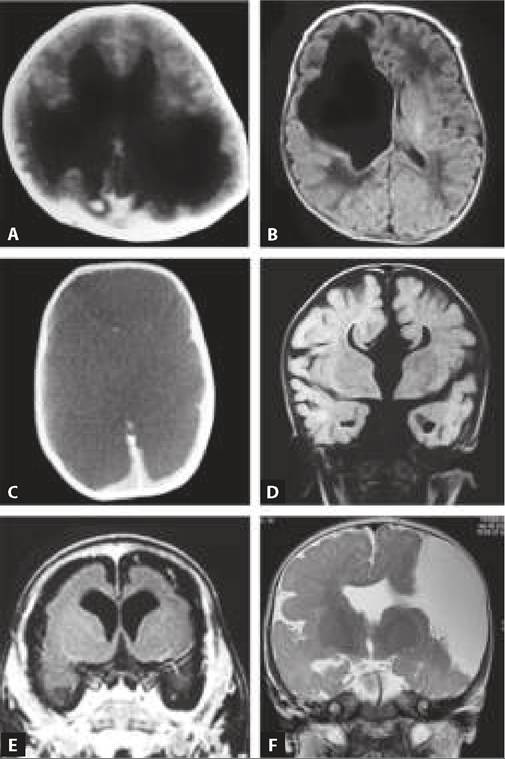
Fig. 18.8: Hydrocephalus: Sunset sign.

Fig. 18.9: Hydrocephalus: CT scan showing dilated ventricles with periventricular oozing of CSF.
• Other indicators, e.g. disturbances in growth, sexual development and fluid/electrolyte homeostasis may develop in chronic cases due to the pressure of dilated third ventricle on hypothalamus.
Diagnosis is based on clinical findings, supported by following investigations to identify the cause:
• Neuroimaging with USG (till AF is open), CT scan or MRI to identify the severity, and specific cause of hydrocephalus, as well as exact location of lesion. In obstructive hydrocephalus, only the ventricular system proximal to the block dilates, whereas in nonobstructive type, entire ventricular system is uniformly dilated (Fig. 18.9). Congenital hydrocephalus can also be detected antenatally on USG.
• CSF examination for underlying infection, which should be treated before shunt surgery to avoid complications, e.g. shunt-block or infection.
D/D of hydrocephalus includes other causes of large head,
e. g. (a) thick cranium, e.g. hemolytic anemia, rickets, etc., (b) subdural hematoma/effusion, (c) hydranencephaly, and (d) megalencephaly.
Megalencephaly, defined as Brain weightvolume ratio gt;2 SD for age, is usually accompanied by Macrocephaly, i.e. head circumference gt;2 SD for age. Megalencephaly may be primary (benign familial) or secondary, seen in genetic syndromes, e.g. Sotos syndrome, neuronal storage disorders (Ch 18.12), Hurler syndrome and neurofibromatosis.
Management of hydrocephalus aims to control intraventricular pressure by surgical or medical means and treatment of primary cause.
Medical therapy to reduce CSF production with acetazol amide, furosemide and glycerol, is only a temporary measure to arrest further progress of hydrocephalus, indicated in—(a) mild/slowly progressive hydrocephalus, (b) hydrocephalus with CSF infection, till shunt surgery is possible, (c) hydrocephalus due to increased CSF production, e.g. choroid papilloma, and
(d) as adjuvant to shunt surgery.
Surgical intervention with creation of a mechanical shunt to facilitate CSF drainage is cornerstone of treatment in moderate to severe hydrocephalus. Although various shunt procedures draining ventricular system extracranially (into peritoneum, atrium, jugular veins) or intracranially (to the ventricle distal to block site) have been used, ventriculoperitoneal shunt (VP) continues to be the procedure of choice in most cases. Commonly used VP shunts have non-return, pressurelimited valves, which drain excess CSF into peritoneal cavity whenever intraventricular pressure rises above a critical level.
Shunt surgery should be deferred till normalization of CSF in subarachnoid hemorrhage or meningitis, as high protein content of CSF may block the shunt. These cases may be temporarily treated by placing a temporary reservoir in the ventricle through which repeated CSF tapping can be done.
Complications o f shunt surgery include—(a) shunt block, (b) shunt infection, usually caused by Staph. epidermidis, (c) shunt displacement/extrusion, (d) shunt fracture, (e) peritonitis and (f) skin/subcutaneous infection or abrasion over the shunt track.
To avoid the complications of shunt, endoscopic third ventriculostomy is being done increasingly in which an endoscope is passed through laternal ventricle and a perforation is made in the floor of third ventricule to allow drainage of CSF directly from ventricles to the subarachnoid space.
Prognosis depends on the cause and size of ventricles, along with thickness of cortical mantle at the time of operative intervention. Hydrocephalic children are at risk for developmental disabilities, visual field defects, optic atrophy and intellectual and motor handicaps.
18.11
More on the topic HYDROCEPHALUS:
- Ventricles
- NEURAL TUBE DEFECTS
- PEARLS AND PERILS
- Selected parasite
- Open fetal surgery
- Dehydration
- Cerebellum and Hindbrain
- LJUNGAN virus infection
- Stenosis
- Defects of Tubular Bone or Spinal Growth Present at Birth