Chronic Progressive Nephropathy
This disease has been referred to by a variety of other terms, including "glomerulosclerosis," “progressive glo- merulonephrosis,” and "old rat nephropathy,” among others.
Chronic progressive nephropathy (CPN), the preferred term used herein, is an extremely common life-limiting disease of aged rats. The prevalence of CPN in older rats varies but may exceed 75% in susceptible strains. A variety of predisposing factors play a role in the development of CPN. (i) Age: lesions are usually most extensive in animals at least 12 months of age. (ii) Sex: CPN is more common and more severe in males. (iii) Strain: the prevalence is usually significantly higher and more severe in Sprague-Dawley and Fischer 344 rats compared to other rat strains. (iv) Diet: high-protein diets are an important contributing factor, although total dietary restriction, rather than protein content, may be more important in reducing the progression of CPN. (v) Immunological factors: mesangial deposition of IgM has been observed in affected glomeruli, consistent with noncomplement-fixing immune complexes, but CPN does not appear to be primarily an immunologically mediated disease. (vi) Endocrine: prolactin levels have been implicated as a contributing factor. (vii) Microbial status: axenic rats tend not to develop CPN, living much longer than microbe-associated rats.Pathology
Clinical signs associated with CPN include proteinuria, weight loss, and in advanced cases elevated plasma creatinine levels consistent with renal insufficiency. The renal cortices are usually pitted and sometimes irregular, with variable degrees of enlargement and pallor in some affected animals. On cut surface, there may be irregularities and linear streaks in the cortex and medulla, with varying degrees of brown pigmentation (Fig. 2.62). Microscopic changes are consistent with a chronic glomerulopathy.
Glomerular changes vary from minimal thickening of the basement membranes to marked thickening of glomerular tufts, with segmental sclerosis and adhesions to Bowman's capsule (Fig. 2.63). Proteinaceous casts are often present in dilated tubules in the cortex and medulla (Fig. 2.64). Eosinophilic, PAS- positive and iron-positive resorption droplets are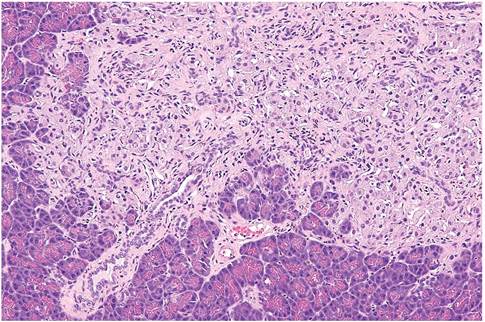
FIG. 2.61. Pancreatic islet fibrosis in an aged rat.
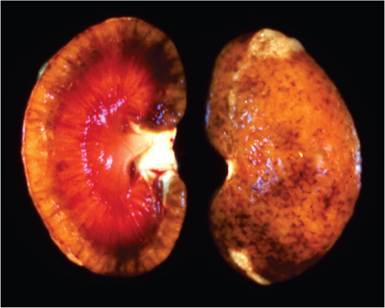
FIG. 2.62. Chronic progressive nephropathy in an aged rat. Note the
granular appearance to cortical surface, linear streaks on cut surface, and irregular pigmentation.
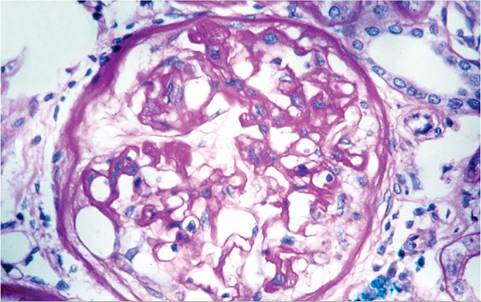
FIG. 2.63. Chronic progressive nephropathy in an aged rat. Note the thickening and splitting of Bowman's capsular basement membrane, thickening of glomerular capillary basement membranes, and glomerular synechiae (PAS stain).
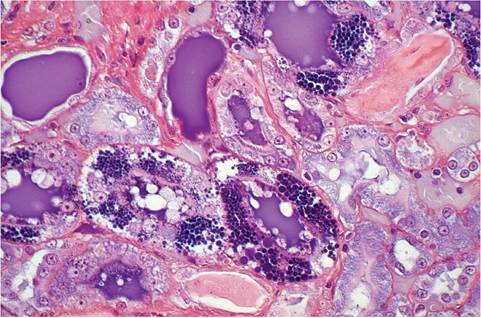
FIG. 2.65. Chronic progressive nephropathy. Note the proteinaceous
casts in dilated tubules and the variable-sized granules (resorption droplets) in the cytoplasm of tubular epithelial cells (PTAH stain).
frequently present in epithelial cells lining affected nephrons (Fig. 2.65). Tubules are frequently dilated and lined by flattened epithelial cells, contracted and lined by poorly differentiated, cuboidal, basophilic epithelial cells, or sclerotic. There may be varying degrees of thickening and splitting of Bowman's capsular and proximal tubular basement membranes, interstitial fibrosis, and interstitial mononuclear cell infiltration. Macrophages and myofibroblasts appear to play an important role in the development of the interstitial fibrosis. In advanced cases, there may be secondary hyperparathyroidism, with mineralized deposits in tissues such as kidney, gastric mucosa, lungs, and the media of larger arteries. CPN contributes to hypertension, and is often associated with polyarteritis. Hypercholesterolemia, hypoproteinemia, and elevated blood urea nitrogen consistent with renal insufficiency/failure may be evident in advanced cases. Elevated serum cholesterol and marked proteinuria (>300 mg/dl of urine) are useful diagnostic parameters. In advanced CPN, urine proteins electro- phoretically mimick serum protein profiles. Animals with severe disease appear to cope well, but may rapidly decompensate and die.
More on the topic Chronic Progressive Nephropathy:
- BIBLIOGRAPHY FOR AGE-, MISCELLANEOUS-, ENVIRONMENTAL- AND DRUG-RELATED DISORDERS
- Glomerulonephropathy