Diagnosis Based on the Use of Ante-mortal Tests
9.3.1 The Intradermal Tuberculin Tests
The intradermal tuberculin test is one of two, the other being the IFN-γ assay, of the standard ante-mortal diagnostic procedures for detecting M.
bovis infections in cattle accepted by the Office International des Epizooties (OIE) for BTB surveillance and eradication purposes. The most common tuberculin tests used currently are the caudal fold test (CFT), the single intradermal test (SIT) and the single intradermal comparative cervical tuberculin test (CCT) done in the skin of the neck. Should an animal be suffering from BTB, the resulting reaction is the consequence of a cell- mediated hypersensitivity response causing a local infiltration of a succession of different types of T lymphocytes. It is characterized by the development of an inflammatory edema limited by a meshwork of fibrin deposited around the collagen bundles of the reticular dermis, to the area where the tuberculin was administered (Doherty et al. 1996). The test result of the skin tests is based on the measurement of the increase in the skin thickness caused by this localized delayed-type hypersensitivity response 72 h after intradermal injection of bovine tuberculin. The reaction is characterized by the presence of local erythema, swelling, heat, pain, and edema. The CFT is assessed by palpation of the injection site. The comparative test (CCT), when tuberculin derived from Mycobacterium avium is simultaneously injected at a different site on the neck to the bovine tuberculin, is assessed on the extent of the difference between the two reactions. Depending on the nature of the reaction, and the increase in the thickness of the skin at the injection site, the reaction will be classified as positive, negative, or inconclusive (suspicious), thus giving an indication of the BTB status of the specific animal and, by implication, of the herd to which it belongs. Because of the lack of Se and Sp of the tuberculin tests, it is essentially a herd test, and individual animals cannot be tested with confidence.The tuberculin skin test has only been validated for use in cattle and perhaps, for diagnostic use, in South Africa in African buffaloes (Syncerus caffer). Using these tests in other species of wildlife, in particular, is risky since their reactions and responses have not been validated, and the results may be erroneous leading to incorrect and unreliable diagnoses (OIE 2017).
Superficially, using the intradermal tests appears to be a simple matter, but because of the complex nature of the disease, it is a major challenge making a diagnosis in all instances. The procedure is influenced by the relative and variable lack of Se and Sp of the intradermal tests and a host of other factors including the time since infection, how the test was executed, host factors, environmental variables, and the characteristics and potency of the tuberculin used in each case.
It is not possible to detect all infected animals in a BTB-infected herd by only using the intradermal tuberculin test, and this creates major problems. When attempting to achieve disease-free status, the test is combined with other tests and abattoir surveillance to detect those cases that do not respond to tuberculin. Even with all the combined diagnostic procedures, some infected cattle may still not be detected and remain in the herd. Not identifying and removing all positive cattle make it most likely that the disease will eventually re-emerge, a situation that requires ongoing surveillance also in disease-free herds, if the disease is to be adequately controlled. In countries certified BTB-free, abattoir surveillance is used on an ongoing basis to monitor the situation.
9.3.1.1 Tuberculin
Tuberculin, initially known as Koch’s old tuberculin (OT), and then as the heatconcentrated synthetic medium (HCSM) tuberculin, is now known as purified protein derivative or PPD, and is prepared from heat-killed cultures of M.
bovis (bovine PPD) and M. avium (avian PPD). Tests utilizing tuberculin remain the most acceptable diagnostic techniques used internationally for the diagnosis of BTB and their use has been sanctioned by the OIE, for use in the intradermal tests, and for the INF-γ assay.Tuberculin is a complex mixture of poorly defined proteins (both secreted and somatic), lipids, sugars, and nucleic acids that include a mixture of antigens that are common to several mycobacterial species (Monaghan et al. 1994; Van Pinxteren et al. 2000). Tuberculin currently is a mixture of refined, heat-treated products of the growth and lysis of specific strains of M. bovis (strain AN5) and M. avium (strain D4ER and TB 56) internationally produced commercially by different companies and institutions. The culture broths of the two mycobacteria contain more than 800 individual proteins that, dependent on several factors, vary in concentration. Commercially available tuberculin consists of a mixture of small, water-soluble proteins, following removal of the high-molecular-weight proteins. Bovine PPD is usually available at a concentration of 2000 IU/ml for cattle for routine diagnostic purposes, while that of avian PPD is 2500 IU/ml. The use of higher concentrations of up to 5000 IU/ml of bovine PPD is required for cattle with a decreased sensitization and in national eradication programs when there is a need to increase the Se of the test. Though the protein content in different batches of PPD may be similar, the correct protein concentration does not predict adequate and a similar biological activity. The variable concentration of specific proteins determines the potency of specific batches of tuberculin that may vary between manufacturers and between batches from the same manufacturer (Downs et al. 2017). The potency of each of the different batches must be assessed, usually in rabbits and periodically in cattle under conditions in which the tuberculin will be used (Good and Duignan 2011).
There have been numerous attempts to improve the performance of PPD and its use in tuberculin skin tests (TSTs), but a formulation that would satisfy all the requirements of a good test has yet to be developed (Schiller et al. 2010a).Tuberculin should be produced according to the standards determined by the OIE and the European Union (EU) and should be of a specified potency. However, tuberculins of varying and lower concentrations are available in the market. Consistency of the potency of the tuberculins used in a specific country is critical as it has an impact on the consistency of test performance and interpretation of the test results. For this reason, attention should be given to the quality of the product in addition to ensuring that there is evidence that the potency of each batch was evaluated and certified (Good and Duignan 2011). For best practice, regulatory authorities in specific countries should ensure that tuberculin from the same manufacturer is used for the duration of control and eradication campaigns.
9.3.1.2 Tuberculin Skin Tests (TSTs)
An ideal screening test must be able to identify all tuberculous animals tested in a group, and it must not identify non-diseased animals as tuberculous. Thus an ideal diagnostic test would detect a signal that is uniquely and specifically associated with an M. bovis infection, that is present in the animal throughout the course of the infection, and that can be detected in a reproducible manner (Anon 1994). An additional feature of the skin test, is also the requirement that it should differentiate between animals that are naturally infected, and those vaccinated with a Bacillus Calmette-Guerin (BCG) vaccine (Buddle et al. 1995; Whelan et al. 2010).
While the tuberculin skin tests have been the mainstay of the immunological diagnosis of TB in humans and many animal species (particularly cattle), there is a marked variation in the nature and extent of the response to tuberculin between the various species.
The induced reaction is also not fully specific since various other mycobacteria and other closely related bacteria share many of the epitopes of M. bovis and thus also those contained in PPD. However, in spite of these limitations, using these tests resulted in the eradication of BTB from a number of countries and for them to sustain a BTB-free status.Fig. 9.4 Injecting tuberculin intradermally when using the caudal fold tuberculin test (photo by Dr. C. Daborn)
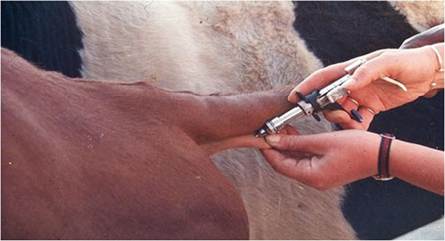
In cattle, there are three types of skin test: the single intradermal tuberculin test (SIT) and the single intradermal comparative cervical tuberculin test (CCT) that are done in the skin of the neck, and the caudal fold test (CFT) (Fig. 9.4). Depending on the specific situation, they may be used serially or as stand-alone tests. The caudal fold test is favored in the USA, Canada, Australia, and New Zealand, while the other two are routinely used in Europe, the UK, some of the African countries, and elsewhere. Generally, the SIT is used as the initial screening test, as it has the highest Se of the three. It is, however, important to select a specific test to be used in a country, dependent on the varying Se and Sp required for the environment, prevalence of the disease in the population, and the conditions under which the tests are to be conducted (Leslie and Hebert 1965; Awah-Ndukum et al. 2012).
The intensity of the reaction at the caudal fold and the neck sites differs as the sensitivity of the skin to tuberculin increases from the back toward the front and from the bottom to the top of a bovine. The skin of the hindquarters is three times less sensitive to tuberculin than that of the neck, and higher doses of PPD are used in the caudal fold test to compensate for this difference (OIE 2009; Schiller et al. 2010a). Even on the neck, although the Sp has not been determined, the tests have higher Se when they are done closer to the head and then have a higher probability of detecting reactors (Casal et al.
2014). Where the CFT is used, responder cattle are removed from infected herds, with or without using the CCT (Good and Duignan 2011).The Se and Sp of a test are used to assess its accuracy as a diagnostic tool. The Se of a test is the proportion (as a %) of the number of diseased animals that give a positive test result, and the Sp is the proportion of non-diseased animals that give a negative test result (Martin 1984). Negative test results in diseased animals are referred to as “false negatives,” whereas positive test results in non-diseased animals are “false positives” (Table 9.1).
The Se and Sp of the CCT are, respectively, between 68-95% and 96-99.9%, but they may vary substantially (Monaghan et al. 1994; Karolemeas et al. 2012). This low Se has the disadvantage of allowing the disease to persist in up to 29% of infected herds, thus allowing recurrent breakdowns, onward transmission of the infection to other herds, and spillover to local wildlife hosts to occur (Norby et al. 2004; Karolemeas et al. 2012). The choice of using either the single intradermal test (SIT) or the comparative cervical test (CCT) significantly influences the
Table 9.1 Interpretation criteria for TSTs (OIE 2009)
Test procedure Diagnosis Interpretation Purpose of the test
SIT—increase in skin thickness
| ≥4 | Positive | Standard | Surveillance |
| 2-4 | Inconclusive | Confirmation of breakdowns | |
| ≤2 | Negative |
CCT—difference between bovine and avian increase in skin thickness
| ≥4 | Positive | Standard | Surveillance |
| Inconclusive | Confirmation of breakdowns | ||
| ≤2 | Negative | ||
| 2-4 | Positive | Strict | Infected herds |
| >1 | Positive | Severe | High prevalence regions |
interpretation of the results. Hence the outcome of the assessment and the decision as to which test is used should not just be a financial consideration; rather the suitability of a specific test should be based on local circumstances (Awah-Ndukum et al. 2012; Bezos et al. 2014). This is of particular importance in areas where large numbers of non-specific reactors occur (see below). The problem of false-positive tuberculin reactions due to significant cross-reactivity with atypical mycobacteria, reduces the diagnostic value of the SIT, and, depending on the types and levels of exposure to environmental mycobacteria, the proportion of false positives may be as high as 12% (Schiller et al. 2010a). To deal with this lack of Sp of the SITs, cattle can be retested with the CCT to enhance the Sp of the test and to reduce the number of false positives (Fischer et al. 2005; Good and Duignan 2011).
The lack of diagnostic accuracy associated with false positive and inconclusive reactions are the major problems with the TSTs. This is partially because tuberculin itself is a poorly defined cocktail of antigens that does not discriminate clearly between individuals infected with TB, and reacts to non-specific antigens, particularly those produced by other mycobacteria. Using the CCT 42-60 days after initial screening by SIT increases the Sp. However, testing has less Se if used in this way, as small reactions to bovine PPD, by the way the test is interpreted, are not classified as positive, and prior exposure to environmental mycobacteria may mask an M. bovis infection (Thom et al. 2008; Awah-Ndukum et al. 2012) resulting in many infected animals to be classified as negative.
Estimates of the Se and Sp of the TST vary substantially as the test results may be influenced by several factors at the time the test is performed (Table 9.2) (Martin 1984; Monaghan et al. 1994; Awah-Ndukum et al. 2012). Current TSTs thus have considerable limitations when used to test individual animals for which it is an inadequate procedure. The values for the ante- and postmortal Se and Sp of the various tests have been assessed by Nunez-Garcia et al. (2018) and should be used as a guideline for selecting appropriate tests when developing control strategies.
The herd-level sensitivity [Se (Herd)] of a test depends on the individual level Se and Sp of the test, the number of animals tested in a herd, and the proportion of these animals that are actually infected. As the number of animals tested from a given herd
Table 9.2 Common causes of false-positive and false-negative responses in the TSTs for BTB
| Test result | Reason for the inappropriate response and interpretation |
| Falsenegative | Early infection |
| Anergy due to advanced, generalized M. bovis infection | |
| Temporary desensitization associated with short-interval, repeat testing | |
| Stress associated with poor nutrition, transportation, pregnancy, parturition | |
| Concurrent parasitic or viral infections | |
| Use of immunosuppressive drugs | |
| Tuberculin administered incorrectly, insufficient amounts of tuberculin, inadequate preparation of the injection site, inexperienced operators, inappropriate animal handling | |
| Low potency of tuberculin, expired product, product stored under inappropriate conditions, manufacturing errors | |
| Falsepositive | Exposure to or infection with several non-tuberculous environmental mycobacteria |
| Bacillus Calmette-Guerin (BCG) vaccination or vaccination against Johne’s disease | |
| Passive immunity (in young calves) | |
| Skin tuberculosis caused by unidentified acid-fast mycobacteria | |
| Infection with other bacterial species | |
| Variation in the pressure applied to manual calipers |
increases, the probability of detecting at least one infected animal (to declare the herd “diseased”) is assumed to be greater than it is to identify an individual infected animal. However, testing a large number of animals to improve the Se increases the likelihood of obtaining false-positive results and reduces the Sp, particularly as the prevalence of the disease decreases in a herd or country (Anon 1994). The Se of the test in high-risk groups too may differ from those in the general population. By using different cut-off points when interpreting the reaction to a TST, the number of test positives may vary between the tests, and this may cause an inconsistency when determining the actual number of TB-infected animals (Anon 1994; Buddle et al.
2009).
In those countries where the SIT or CCT are used, interpretation of the tests is done in accordance with the guidelines of the OIE and, in the European countries, also the relevant EU trade directive (Directive 64/432/EEC). Because of specific local conditions, and other reasons, the OIE recommendations for the interpretation of the tests may have to be modified in specific countries, or regions of countries, to increase the Se and Sp of the tests to acceptable levels. There is no point, as an alternative, to just increase the potency of tuberculin, since there is then an increase in the number of cross-reactions with other mycobacteria, and thus, in the number of false positives (Ritchie 1959).
Cattle that were recently infected also do not react to any of the tests, since it takes from 3 to 6 weeks for them to develop a sufficient cell-mediated immune response that can be detected by the test (Good and Duignan 2011). Sensitized cattle react stronger during the early stages of the infection, and the response decreases over time as the disease progresses. The waning of the delayed cellular immune response causes this decline in responsiveness because midway through the course of the diseases, the immune response gradually switches to a predominantly humoral response. The extent of the immunological response may vary substantially within and between species, age cohorts, testing histories, and between sexes. Coinfections with liver fluke, Johne's disease (Alvarez et al. 2008), and bovine viral diarrhea virus also diminish the reaction (Byrne et al. 2018). Animals may be unresponsive, or anergic (Lepper et al. 1977), during the early stages of the infection, when lesions heal, and particularly in the advanced, generalized stages of the disease when they shed large numbers of M. bovis into the environment (Perla 1927).
It is generally accepted that the SIT is more Se but less Sp than both the CFT and the CCT, and in certain countries as many as 12% more cattle reacted to the SIT compared to the CCT (Anon 1994; Good and Duignan 2011). When applied to animals exposed to a high risk of infection, the SIT is effective in detecting preclinical cases (Buddle et al. 2009), and in many countries BTB was eradicated by rapidly removing tuberculin-positive reactors using this test. However, as the prevalence of the disease becomes lower, not all infected animals react to the injection of tuberculin, irrespective of whether the SIT or CCT is used. This phenomenon may be due to the presence of anergic reactors, animals that react equally to the bovine and avian PPD, animals in the advanced stages of the disease, lesions confined to single organs such as the udder, lesions that became inactive (latent), or peri-parturient cows (Ritchie 1959). Non-specific responses, that appear to be a worldwide problem, also complicate the caudal fold test.
Interpretation of the SIT According to the OIE-formulated guidelines for the interpretation of the tuberculin skin tests, a general approach when doing the SIT is to consider an increase of ≥4 mm as a positive reaction, whereas an increase of ≤2 mm, with no local signs, is defined as negative. An indeterminate reaction (IR) (inconclusive or suspicious) is recorded in the absence of local signs of a reaction, when the increase in skin thickness is between 2 and 4 mm (Vekemans et al. 1999).
Interpretation of the test is not only dependent on an increase in the thickness of the skin. The characteristics of the reaction at the site where the tuberculin has been injected should also be taken into consideration after visual assessment and by palpation. Non-specific reactions, such as those caused by the so-called skin lesions caused by environmental mycobacteria, result in the development of a hard, localized swelling. Those reacting to M. bovis usually have a diffuse, poorly circumscribed thickening of the skin characterized by the presence of edema, pain, heat, and, when severe, superficial necrosis of the skin in the central portion of the reaction site, distention of the lymphatics draining the area, and enlargement of the prescapular lymph node. A number of factors influence the Se and the outcome of the test (Table 9.2).
Depending on the required Se and objectives of the investigation, the skin tests can be interpreted according to standard, strict, or severe criteria (Table 9.1). Because of various factors, that may differ from country to country, the criteria for interpreting the skin reaction may differ and may have to be adapted for a specific
Fig. 9.5 The typical site in the middle of the neck for doing the single intradermal tuberculin test, manifesting a positive response

country. An example of this type of adaptation for different situations that can be used as a guideline in Africa, can be found in the South African BTB test manual (DAFF 2016). What is critical to remember though is that these criteria may have to be adapted over time based on the experience gained in each specific country as its campaign progresses. Good record keeping and monitoring the human resources and reagents are critical for quality control and consistency when interpreting the test results.
Single Intradermal Tuberculin Testing Technique Assessing the outcome of an SIT test in the skin of the neck involves measuring the skin thickness (after clipping the hair) using a spring-loaded caliper that will consistently exert the same pressure on the skin when measuring, and then injecting PPD-B tuberculin (0.1 ml of 2000IU at 1 mg/ml) intradermally. Normally, the tuberculin is injected on one side of the neck, halfway between the juncture of the head and neck, and the skin fold in front of the shoulder, halfway between the top and bottom of the neck (Fig. 9.5). The injection site should have a normal skin texture and be without lumps (DAFF
2016). Tuberculin can be injected using a number of different types of syringe: the McLintock (UK) and the Dermojet (France) syringes are used most frequently. A small, pea-like swelling should be present at the site of the injection to confirm that the intradermal injection was successful. The skin thickness at the injection site is remeasured 72 h later, using the same caliper used to initially measure the skin thickness, to determine the increase in skin thickness. The site should also be palpated to assess the nature of the reaction.
The Single Intradermal Comparative Cervical Tuberculin Test (CCT) The CCT is applied by injecting avian and bovine PPD (0.1 ml of 2500 IU of each, at 1 mg/ml) 12-15 cm apart on the same side of the neck. The difference between the increase in skin thickness at the two sites after 72 h is used to determine the status of the animal (OIE 2009). Should the increase in the avian PPD be equal or greater than that of the bovine PPD, the animal is considered to be negative. The interpretation, should the bovine reaction exceed the avian reaction, is based on different cutoff points, referred to as standard, strict, or severe, to increase the likelihood of detecting more positive cases in a given situation (Table 9.1).
Serial Tuberculin Skin Testing To increase the specificity of a TST, sequential or serial testing may be used. An example of sequential testing is the use of the CFT or SIT to initially screen a herd. Then all responders, or those that inconclusively reacted to the bovine PPD, are tested with the CCT after an interval of 42-60 days. Only those animals that continue to react are then classified as positive. This sequential testing procedure greatly increases the specificity of the overall diagnostic procedure, although there is potential for a reduction in sensitivity because of the likelihood of false-negative results with the second test (Radunz and Lepper 1985).
Another approach in serial testing is to use the SIT or CCT as herd-screening tests, and then to subject all negative reactors to a second test, commonly the IFN-γ assay. Although both the TST and the IFN-γ assay detect a cell-mediated immune response, they are known to detect different sets of reactors that partially overlap (Wood et al. 1991). One or the other test will identify a certain, but different, percentage of the reactors. This process increases the Se of the overall diagnostic procedure, because animals reacting to either of the tests are considered to be positive, and they then in combination identify a larger number of infected animals. The process still remains inadequate, as the Se of the IFN-γ assay is only about 85% and its use does not contribute substantially to detecting all the positive reactors (Praud et al. 2015).
The application of the TST followed by a serological test, as an ancillary test, is a unique form of sequential testing. It appears that infected animals are stimulated by the initial intradermal test to increase antibody production, and they are then more likely to test positive with the subsequent serological test (Dowling and Schleehauf 1991). Using different serological techniques, up to 75% positive reactors out of a group of false negatives were detected by collecting blood for commercially available serological assays 15 days after the TST was done. This is a useful procedure when there is a need to identify anergic animals that are likely to be supershedders when the CCT with its low sensitivity is used, and in those cases where the INF-γ assay cannot be done due to resource limitations (Casal et al. 2014).
The Use of TSTs in Africa Because of limited financial resources and the cost of TSTs, and because the disease is not considered to be of importance to livestock or humans, few countries in Africa use tuberculin testing to assess the prevalence and distribution of BTB in their livestock population. For these reasons, TSTs on the continent are mostly used for research or limited surveillance purposes (Bedard et al. 1993).
There are a number of major impediments that limit the use of TSTs, particularly when testing in remote rural African areas. Doing the tests in these areas in which transhumant and extensive management practices prevail, is challenging. Under these circumstances, given the poor, or non-existing roads, the lack of infrastructure, and the reluctance of cattle owners to return their cattle to the testing site to evaluate the reactions, it becomes almost impossible to use tuberculin skin testing as a diagnostic tool. Further impediments include the limited availability of tuberculin, the lack of trained human resources to do the tests, and the lack of suitable handling facilities in which to restrain the animals for testing. It is possible that physiological and operational problems including stress associated with poor nutrition and exertion also cause a poor immunological response and render the tests less sensitive (Buddle et al. 2009). Concurrent parasitic infections also significantly undermine the reactivity to tuberculin in tropical Africa (Awah-Ndukum et al. 2012). The presence of external parasites and other parasitic conditions of the skin caused by Demodex, Filarioidea, and Besnoitia spp. further limit the ability to use the skin test (Martrenchar et al. 1993) because of the diffuse lesions that they cause in the skin that interfere with accurately measuring the increase in skin thickness.
The large number of non-specific reactors is a further major problem impacting the use of TSTs in Africa. In some instances as many as 50% of the animals tested are non-specific reactors (Carmichael 1937; Warren et al. 2006; Asiak et al. 2007; Michel 2008; Durnez et al. 2009; Muller et al. 2009; Katale et al. 2013; Zahran et al. 2014). To deal with these problems in some of the tests, cut-off points of ≥2 mm or ≥3 for CCT were used to limit the number of non-specific reactors (Muller et al. 2009; Muma et al. 2013). Because of the extent of non-specific reactors in the various countries, it has been recommended that the SIT should not be used as a preliminary screening test, but that the CCT should be routinely used. This, however, increases the cost of testing, which further limits the use of TSTs because of the inadequate financial resources available in most of the African countries.
The Use of TSTs in Wildlife in Africa For the purpose of control, wild animals are categorized as those animals that do not live under human supervision or control and do not have their phenotype selected by humans, captive wild animals, and feral animals. There is a long list of wild animals, either free-living or in captivity, that have been subjected to a variety of diagnostic procedures for BTB. However, only the intradermal test (both the SIT and CCT) and the IFN-γ assay used in African buffaloes (Michel et al. 2011) come close to being validated for the purpose (Cousins and Florisson 2005).
The CCT, done on the neck, was assessed in lions in the Kruger National Park (KNP), South Africa. By only using the reaction at the site where bovine PPD was injected, it detected 85% of positive animals (as confirmed by culture), and it was 5% more sensitive than the CCT. To obtain a sufficient reaction to the intradermal injection of both bovine and avian PPD in lions, doubling the dosage used in cattle, and an increase in skin thickness of ≥2 mm as the cut-off point, rendered the highest Se and Sp. The extensive infection of lions in the KNP with mycobacteria other than M. bovis is the most likely reason why the CCT was less Se, as it also influenced and masked the response to bovine tuberculin. Although these results can be used as a guideline for interpreting a TST in lions, the test has not been validated, and under different circumstances, the response may be different (Keet et al. 2010).
A substantial amount of work has been done in South Africa to develop a variety of tests for some of the more iconic species such as white (Ceratotherium simum) and black (Diceros bicornis) rhinoceroses, elephants, lions, and greater kudus, but most are not close to being validated for the purpose. Validation of tests for diagnostic purposes is a tedious process, and the methodology is contained in the OIE’s Manual of Diagnostic Tests and Vaccines (OIE 2017). The OIE makes provisions for validation of tests in wildlife given the small numbers of animals that are dealt with and available for the validation process. The procedures for test validation in wildlife are contained in Chapter 3.6.7 of the Manual and can be accessed online (http://www.oie.int/standard-setting/terrestrial-manual/access- online/).
Given the likely importance of wildlife in the epidemiology of BTB in Africa, there is no doubt that some effort is needed to validate the available tests to allow assessment of the epidemiological role of wildlife in the various countries in which wildlife maintenance hosts have been identified. It is clear that not only wildlife maintenance hosts are important when dealing with BTB. The tests should also be available for spillover hosts, particularly those that are farmed with, those in zoological collections, and other free-ranging wildlife as they may yet be determined to play a significant role in the epidemiology of the disease, its control, and its final eradication from the continent.
From a practical perspective, developing diagnostic tests for wildlife species should focus on one-off, rapid, ante-mortal tests. The need to assess the reaction of the TSTs after a few days, prohibits their use in wildlife as a general diagnostic technique, because of their impracticality, the time and effort required to do the tests, and the cost of immobilizing animals for a second time (Fitzgerald and Kaneene
2012).
9.4
More on the topic Diagnosis Based on the Use of Ante-mortal Tests:
- Post-mortal Diagnosis of BTB in Nigerian Abattoirs
- Application and Interpretation of Findings From PCR-Based Diagnostic Tests
- Immunity and Immune-Based Diagnostic Tests
- Diagnosis Based on Clinical Signs
- Immune-Based Diagnosis of Paratuberculosis
- Simple and non-invasive tests, confirmatorytests, follow-up tests
- Mortal Combat
- Tests Used in Prevalence Studies
- The Tests
- Cell-Mediated Tests
- Evaluation of Diagnostic Tests Under Local Conditions
- Memory and Learning Tests
- Sensory-Perceptual and Motor Tests