Drug Susceptibility Testing Definition and Description
The field of DST is rife with technical jargon that merits a brief overview. Box 10.1 defines common DST vocabulary found throughout the chapter.
AST is the cornerstone of the practice of infectious diseases and the foundation of many multidisciplinary laboratories, namely clinical laboratories, national reference centres, hospital laboratories and basic research groups.
The outcome of AST on a microorganism is a determination whether the microbe is susceptible or resistant to an antimicrobial agent. A physician may be interested in susceptibility results to assist in correct antimicrobial administration, while infection control programmes may emphasize antimicrobial resistance to predict the spread of resistance. The Clinical Laboratory Standards Institute (CLSI) defines resistance as ‘a decrease in susceptibility compared to a sample of drug-naive wild strains' (Desmond et al., 2011). In technical‘Corresponding author: jaryd.sullivan@mail.mcgill.ca © CAB International 2020. Paratuberculosis: Organism, Disease, Control, 2nd Edition (eds M.A. Behr et al.)
Box 10.1. Vocabulary.
Antibiotic: A chemical compound within the subset of antimicrobials that inhibits the growth of bacteria.
Antibiotic resistance: The innate or acquired ability of bacteria to resist the effects of an antibiotic. Resistance is typically concerning at clinically relevant antibiotic concentrations. This concept is largely determined in vitro and is distinct from therapeutic failure, wherein an antibiotic fails to eliminate the infection.
Antimicrobial: A synthetic or naturally derived compound that inhibits the growth of bacteria, viruses or fungi.
Antimicrobial susceptibility testing (AST): Laboratory testing on microorganisms to determine resistance and susceptibility levels to antimicrobials.
CLSI: The Clinical and Laboratory Standards Institute is a US-based organization that develops clinical and laboratory standards, practices and guidelines.
Critical concentration: The lowest concentration of drug that inhibits 95% of wild strains that have never been exposed to drugs.
Drug susceptibility testing (DST): Subset of AST used in the field of mycobacteriology.
EUCAST: The European Committee on Antimicrobial Testing is a European-based society that develops laboratory standards for clinical microbiology and infectious diseases.
Inoculum: Volume/concentration of microorganism used in an AST assay.
Indeterminate (I): A microorganism that is deemed neither susceptible nor resistant according to established minimum inhibitory concentration (MIC) boundaries. These MICs do not suggest withholding the drug but emphasize appropriate adjustment of the dose. NB Some use ‘I’ to indicate Intermediate, but this use of I is discouraged by the CLSI because it implies a strength phenotype only, and excludes technical errors.
Isolate: A microbe isolated from a patient sample.
Microorganism: Categorical term encompassing bacteria, fungi and viruses. Commonly shortened to microbe.
Minimum inhibitory concentration (MIC): The lowest concentration of an antimicrobial that inhibits microbial growth. Typically denoted as MIC90 for inhibition of 90% of growth.
Resistance pattern: Summary of antimicrobial testing results for an isolate.
Resistant (R): A patient isolate should not be susceptible to dosage normally recommended to treat that type of infection and species.
Susceptible (S): A microorganism that is not resistant to antimicrobials at clinically relevant concentrations. A patient isolate should be susceptible to dosage normally recommended to treat that type of infection and species.
terms, a microorganism is considered to be resistant if greater than 0.1% of the inoculum grows through the critical concentration of the drug. In accordance, EUCAST defines resistance with a similar definition but with greater emphasis on standard dosing regimen. For example, EUCAST categorizes a microorganism as resistant when ‘there is high likelihood of therapeutic failure even when there is increased exposure' (Kahlmeter, 2019, p.
17). Therefore, strains are drug resistant even with a modified dose and dosing interval or parental administration.Mycobacteria DST is a variant of AST where resistance is established if the antimicrobial critical concentration permits more than 1.0% of inoculum growth compared with drug-naive wild strains (Desmond et al., 2011). Mycobacterium tuberculosis DST has been shown to predict clinical outcomes in trials and meta-analyses, so it would appear that the 99% threshold is useful (Kim, 2005; Lew et al., 2008). Whether these modified standards apply to MAP and other non-tuberculous mycobacteria (NTM) - is unknown. Determining the resistance pattern could help guide appropriate treatment options, identify a possible mechanism for failed antimicrobial therapy and maintain surveillance for emerging drug resistance in populations (see Box 10.2, for example).
Traditionally, DST examines whether a particular drug can inhibit the growth or metabolism of a bacterium in vitro. Classical DST relies on macroscopic observation of growth in drug and drug-free media through colony-forming unit (CFU) counts on agar or optical density
Box 10.2. S vs R vs I.
If organisms are highly resistant to an antibiotic, it is unlikely that the antibiotic can provide clinical benefit, as seen in Panel A (Fig. 10.1). However, the MIC distribution may follow a distribution closer to that seen in Panel B, where organisms that are not S have an MIC that is increased, but to a lesser extent. In the example of M. tuberculosis, resistance to isoniazid is a heterogeneous phenotype. Resistance due to katG deletions cannot be overcome, as isoniazid is a pro-drug, for which bacterial KatG is required for activation. Resistance attributed to promoter mutations in inhA leads to so-called ‘low-level resistance'. Here, the provision of an MIC result that is one to two dilutions higher than the standard threshold, coupled with a genetic test detecting the mutation, can inform the clinician that the resistance can be overcome with a higher dose of the antibiotic.
Hence, results from DST should be interpreted appropriately with biological context and possible mechanism of action of the drug - DST means more than just reading S vs R in a microbiology report.(OD600nm) readout in liquid culture. Indeed, these methods are slow and dated for modern medicine, however, they remain the gold standard according to the CLSI guidelines.
Researchers and clinical labs have developed methodologies for DST that measure the metabolism of bacteria rather than visible growth as a means to circumvent the issue of slow-growing mycobacteria. Resazurin Microtiter Assay (REMA) and Bactiter Glo™ are two assays that monitor metabolism through intracellular redox potential and ATP synthesis, respectively (Niles et al., 2008; Necchi et al., 2018). Additionally, the Mycobacteria Growth Indicator Tube (MGIT) design was modified from the original BACTEC™ blood culture system from BD Diagnostic Systems to culture bacteria from patient samples (Automated Blood Culture System, 2014). Each MGIT™ tube contains an inorganic dye, which fluoresces upon exposure to CO2 produced from metabolically active mycobacteria. MGIT™ culture systems could be described as the backbone of clinical mycobacte- riology labs in many countries due to the ease of use and automated system.
The gold standard for M. tuberculosis frontline drug DST remains the agar proportion method for isoniazid (INH), rifampicin (RIF) and ethambutol (EMB), and the radiometric proportion method for pyrazinamide (PZA) - despite the arrival of new methods with shorter incubation times. In light of these standards, the CLSI recognizes growth on solid media is time consuming and recommends broth culture with a shorter incubation time for industrialized countries. The Centres for Disease Control and Prevention also recommends broth culture for DST. The goal is to report results of primary DST within 15-30 days of receiving the patient sample. Unfortunately, countries lacking the facilities for automated culture systems must rely on standard agar growth.
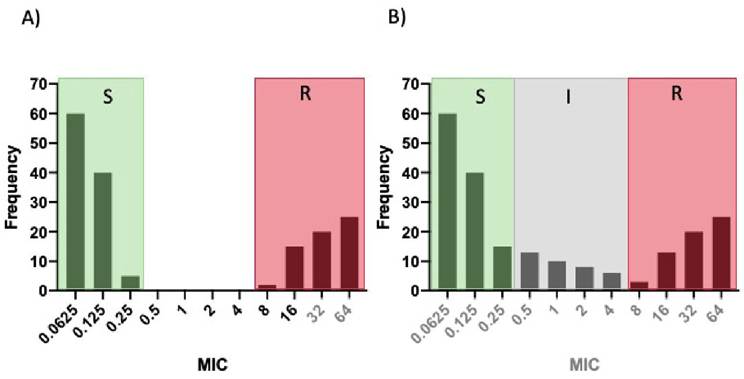
Fig. 10.1. Histogram of hypothetical minimum inhibitory concentration (MIC) distribution for a microorganism. (A) Categorical distribution. (B) Graded distribution.
10.3
More on the topic Drug Susceptibility Testing Definition and Description:
- Drug Susceptibility Testing for MAP, Why Bother?
- MAP Drug Susceptibility Testing: Where Are We in 2019?
- Drug Susceptibility Testing and Antimicrobial Resistance in Mycobacterium avium subsp. paratuberculosis
- Definition and the Ordering of Guardians Definition of the child
- Evidence for Disease Susceptibility Differences in Deer
- Drug-Induced Hemolytic Anemia
- Drug resistance
- Evidence for Disease Susceptibility Differences in Goats
- Adverse Drug Reactions
- DRUG FEVER
- Evidence for Disease Susceptibility Differences in Cattle
- Genetic Testing
- Injecting drug users
- Genetics of Host Susceptibility to Paratuberculosis
- Testing of patients and blood donors