Mycobacterium bovis Infection in Humans
The occurrence and prevalence of human TB due to M. bovis are difficult to determine accurately and probably remain under-reported owing to the diagnostic limitations of the main method used for diagnosing human TB in Ghana.
In a previous work in which 70 pulmonary TB patients attending a health-care facility in Accra were sampled, 3% were identified as infected with M. bovis using biochemical methods for characterization of the mycobacteria (Addo et al. 2007). Ongoing population-based prospective studies of human TB cases in the Accra Metropolis and a rural district of northern Ghana, using conventional culture followed by molecular characterization, identified 15 M. bovis and 1 M. caprae strains from 1794 isolates (from sputum) giving an M. bovis prevalence of 0.8% in the study population. The spoligotype patterns of the identified animal strains are shown in Fig. 15.2. The prevalence that was reported, however, seems lower when compared to the prevalence of up to 10% found in neighboring countries (Mawak et al. 2006), but it is within the estimated range for Africa based on the review of Muller et al. (2013).The National Tuberculosis Control Program of the Ghana Health Service guides TB control in humans in Ghana. In the year 2013, close to 16,000 new TB cases were notified making it the 19th most burdened country with TB in Africa. It was found that in that year, 9% of the over 7000 patients registered died before completing treatment (Kurbatova et al. 2012). This figure, however, may not be a true reflection
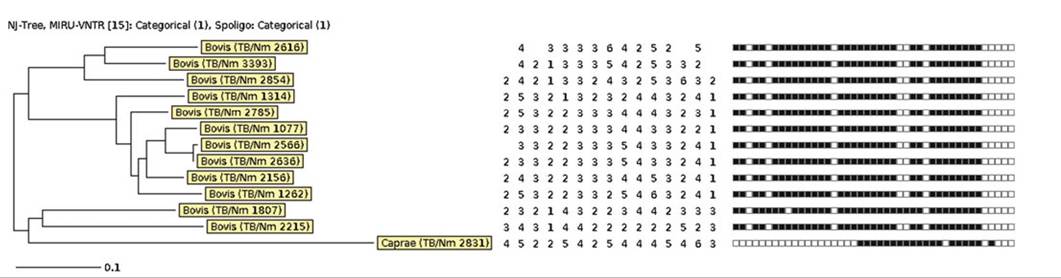
Fig. 15.2 Dendrogram constructed using the Neighbour-Joining (NJ) algorithm for 12 MIRU-VNTR typed M. bovis (identified by Spoligotyping) isolates and an additional M. caprae isolate. Figure was plotted using the MIRU-VNTRplus on-line tool.
The respective Spoligotype patterns are displayed alongside the dendrogramD. Yeboah-Manu and A. Asante-Poku
of the actual prevalence since there are many patients that do not report to health facilities for treatment. Thus, the real TB burden in Ghana is likely to be substantially higher than the official WHO estimates indicate. This notion is confirmed by preliminary data of the just-ended national TB prevalence survey, which shows a prevalence of about 264 cases per 100,000 human populations (National Tuberculosis Report 2014: unpublished data). In addition, anecdotal evidence in Korle-Bu Teaching Hospital (KBTH), Accra (the highest referral health facility in Ghana), indicates that TB is the cause of death in one out of seven post-mortems conducted (MOH/GHS 2003). Reports from the National Tuberculosis Control Program (NTP) in Ghana indicate that about 23% of TB cases are co-infected with HIV and that as many as 50% of patients with chronic cough could be HIV-positive (MOH/GHS 2007).
Due to the lack of appropriate laboratory infrastructure, drug susceptibility testing is not routinely performed in Ghana; therefore, the actual extent of drug-resistant TB is unknown. Current TB control measures in Ghana (like in most other developing countries) are primarily based on sputum smear microscopy, which has a diagnostic sensitivity of only 50% (Muvunyi et al. 2010). However, TB control activities in the past years have improved greatly due to activities being supported by funds from the Global Fund Initiative that include early case detection, detection among vulnerable groups, increasing access to WHO-recommended rapid and more sensitive diagnostics such as XpertMTB/RIF (Cepheid), and the line probe assay, MTBDRplus (Hain Lifescience).
All forms of human TB are dealt with by the National Tuberculosis Control Program (NTP). The main control strategy of human TB by the NTP is case detection mainly by direct smear microscopy and treatment by the directly-observed-treatment- short-course (DOTs) strategy (MOH/GHS 2003). Thus, determining drug resistance is not routinely done and most efforts are focused on diagnosing pulmonary TB by sputum analysis.
Nevertheless, current efforts have been maximized to include recent WHO-recommended diagnostics such as XpertMTB/Rif (Kurbatova et al. 2012) and line probe assays (Asante-Poku et al. 2015) in some regional hospitals. In addition, the NTP receives support from the main biomedical research institute in the country for culture, phenotypic drug-resistance, and molecular genotyping expertise to support case management of retreatment cases and epidemiological studies. The main challenge impeding human TB control is late case reporting and low detection rates due to stigmatization (Weiss et al. 2006).Control of BTB and Challenges Facing the Veterinary Services in Ghana
In Ghana, the control of BTB in animals is the responsibility of the Veterinary Services Department (VSD) of the Ministry of Agriculture. The VSD is also responsible for public health through controlling diseases communicable from animals to human beings by:
• Ensuring that meat and other products of animal origin are safe for human consumption
• Controlling animal movement by ensuring that only healthy animals are permitted to be moved from one area to another to prevent disease spread in the country • Ensuring that all animals entering the country are quarantined and only those found healthy allowed passage into the country
The above measures are assumed to be in place to control the transmission of zoonotic diseases, which includes BTB. However, there are a number of challenges for the VSD to carry out its mandate effectively. For example, lack of logistics including reagents and well-equipped laboratories, and the situation that routine surveillance of BTB by the Surveillance System Component (SSC) is not done. Likewise, movement of animals in accordance with the Economic Community of West-African States protocol that allows free movement of animals and humans across borders limits cross-border control and restriction of movement of cattle across borders.
The acclaimed and effective test-and-slaughter protocol, however, is capitalintensive and cannot be supported financially by the Ghanaian Government.
The VSD, therefore, has a policy of examining cattle slaughtered at various abattoirs for the presence of granulomatous lesions suggestive of bovine tuberculosis infection in an effort to control the spread of the disease from cattle to humans. Cattle with localized infections at post-mortem, that is, infection in one organ and/or its associated lymph node only, has the affected part trimmed off and the carcasses passed for human consumption. However, in animals with generalized infection, that is, infection throughout the entire carcass, the whole carcass is deemed unwholesome for human consumption and is therefore condemned.BTB is a potential zoonotic disease that can infect a variety of wild animals including African buffaloes (Syncerus caffer) (Katale et al. 2012) that are a known BTB maintenance host and are present in both the Mole and Digya National Parks in Ghana. It is currently not known whether any of the wildlife species are infected with M. bovis in Ghana. The presence of multiple hosts including wild animals (Addo et al. 2007) and inefficient diagnostic techniques and the absence of defined national control and eradication programs impede the control of bovine TB in Ghana (Katale et al. 2012).
Finally, not much has been done regarding public education of the zoonotic importance of BTB and raising awareness within communities to prevent the disease. For most rural herdsmen in Ghana, consumption of raw milk and milk products and close association between animals and farmers are common practices, which all enhance exposure to both the alimentary and respiratory routes of infection with M. bovis.
15.6
More on the topic Mycobacterium bovis Infection in Humans:
- Zoonotic Tuberculosis in Zambia
- Control of BTB in Ethiopia
- Introduction
- Conclusion and Recommendations
- Diagnosis of Bovine Tuberculosis in Zambia
- Conclusion
- Prevention and Control of BTB in Sudan
- Prevention and Control of BTB
- The Burden of TB in Africa
- 3 SELECTED SOCIO-ECONOMICALLY IMPORTANT WILDLIFE RELATED PATHOGENS AND DISEASES IN EUROPE