Notifiable Diseases
In the UK most of the legal powers conferred onto the Ministry of Agriculture are contained in the Diseases ofAnimals Act, 1950, which has now been incorporated into the Animal Health Act, 1981.
This enables the Ministry to record and control the movements of livestock, to regulate imports, to enforce quarantine and to establish and finance national disease eradication programmes. it is the orders made under this Act which make it a legal requirement for all owners of livestock to keep detailed records of the movements of their animals, to identify cattle by means of an ear-tag, to report all cases of abortion and sudden death in cattle, and to dip their sheep when there is evidence of scab (mange). There are many other regulations of a similar nature.The Act also states that any person in charge of an animal suspected of suffering from a notifiable disease must report it immediately to the police or to an inspector of the Ministry. Diseases are classed as notifiable when regulations have been made to control their entry into the country or to eradicate them. Current examples include:
Anthrax
Brucellosis
BsE (bovine spongiform encephalopathy)
Enzootic bovine leucosis
Foot-and-mouth
Tuberculosis
Warble fly
There are other exotic notifiable diseases of cattle, for example, rinderpest (cattle plague) and contagious bovine pleuropneumonia, which are not described in this book. Rinderpest was eradicated from the UK in 1877 by a quarantine and slaughter policy and pleuropneumonia in 1898.
Anthrax
Anthrax is an infection caused by the bacterium Bacillus anthracis. in cattle it causes an acute septicaemic illness, resulting in very rapid death. i have only once been called to a live affected animal. It was extremely ill, swaying on its legs and died before I could treat it. In the typical case, after death, dark blood often runs from the nose, mouth and possibly the anus and vulva.
In the UK any animal found dead without an obvious cause must be reported to the Ministry of Agriculture. At no expense to the owner of the animal, the Ministry will send a local veterinary inspector to take samples and test for anthrax. A small cut is made in an ear vein (Plate 11.1), a swab is taken and one side of a microscope slide is coated with a film of blood. This is taken back to the laboratory, a special stain is added to the blood film and the slide is examined microscopically for the presence of anthrax bacteria. The carcase must not be moved or interfered with in any way until the results of the tests are available. With the use of McFadyean’s old methylene blue stain, anthrax will be recognised as large blue square-ended rods (bacilli) surrounded by a pink-staining capsule.
The spores of anthrax are extremely resistant (see Chapter 1) and they are infectious to man and other animals. If anthrax is confirmed, the carcase must be destroyed on the farm by burning it together with any soil, bedding or any other material contaminated with the animal’s blood or faeces.
The disease is now relatively rare, with the total confirmed cases in the UK numbering approximately ten to twelve per year. The most common source of anthrax was imported meat and bone meal which used to be incorporated into animal feedingstuffs. In 1977 there was a minor epidemic (139 cases) originating from this source.
Disease can occur in man, either as ‘boils’ arising from an infected scratch, or as pneumonia if the spores are inhaled. The latter used to be known as ‘Wool-sorter’s Disease’, because dockers unloading hides and fleeces were occasionally exposed to skins which had been taken from anthrax carcases. Anyone at risk is now treated with penicillin or given anthrax vaccine.
Foot-and-mouth Disease
This is a highly infectious virus disease which can spread very rapidly to other cloven-hoofed animals (pigs, sheep and goats) and to adjacent farms. Once infection has entered a herd, the incubation period can be as little as two days, that is to say there may be only two days between exposure to the virus and clinical signs being seen, and this accounts for the very rapid spread of the disease.
An infected cow excretes virus in her urine, faeces, milk, saliva and even on her breath! The virus can survive on the ground for up to 30 days in winter, but only three to five days in summer.
Plate 11.1. Testing for anthrax: a blood sample is collected from a small cut in the ear vein, stained and examined under the microscope.

Plate 11.2. Foot-and-mouth: typical blisters on the tongue.
One of the first signs in an affected herd is that a significant number of cows show a dramatic drop in yield together with a high temperature. Within 24 hours the virus produces large ‘vesicles’, that is fluid-filled blisters, some 20-40 mm in diameter. These are most commonly seen on the tongue (Plate 11.2) and between the claws of the feet (Plate 11.3), although they may also occur on the teats. The blisters soon burst, leading to areas of exposed raw and painful tissue. You should imprint these pictures carefully in your mind in case you are unfortunate enough to see such cases in the future. There may be so many vesicles present that if the tongue is grasped almost all of its covering falls off in your hand (as shown in Plate 11.4). This makes affected animals drool (Plate 11.5) and they also become very uncomfortable on their feet, stepping from one to the other, and possibly kicking or shaking their legs.
If the disease is allowed to progress, affected animals will lose weight rapidly and milk production will suffer. Most adult animals will survive and develop a degree of immunity - although many of them


Plate 11.4. Foot-and-mouth: so many blisters may be present in the early stages that the skin of the tongue simply falls off in your hand.
Plate 11.3. Foot-and-mouth: blisters between the claws.
will remain permanently infected and will be a risk to other animals. Mortality may be very high in younger animals (50-60%) due to heart lesions. There is no specific treatment.
Fortunately there are few other diseases in cattle which show similar classic signs, although the recent increase in ‘soda grain’ feeding has led to a few false alarms! Whole (i.e. uncrushed) grain can be mixed with solid sodium hydroxide and some water to achieve predigestion of the grain husk. If it is not mixed thoroughly, large lumps of sodium hydroxide may be eaten and this can lead to severe mouth ulcers and a very sick animal. However, usually only one or two animals are

Plate 11.5. Foot-and-mouth: affected animals drool, are off their food and are uncomfortable on their feet.
affected, there are no lesions on the feet and affected cattle do not have a high temperature. If sufficient sodium hydroxide is eaten, the whole of the inside of the mouth may slough off, and because of the changes within the rumen, death may occur due to shock. It is interesting to note that one of the
local ‘treatments’ for foot-and-mouth disease in southern Africa is to smear the inside of the animal’s
mouth with sodium hydroxide or salt. This is said to reduce the rate of virus shedding and to speed recovery.
Sources of infection
Because Great Britain has an eradication policy for the control of the disease, determining possible sources of infection is extremely important. Imported live animals represent the greatest potential danger and so countries of origin are strictly monitored to confirm that they are totally free from any risk of foot-and-mouth. After arrival, animals may be quarantined and submitted to regular veterinary inspections. Imported carcases and other animal products can also carry infection. Again, the countries of origin are carefully monitored, as is the hygiene at their processing plants.
For example, only boneless meat may be imported from infected countries, because if any infected animals were slaughtered the virus is most likely to die in meat which has ‘set’, whereas it can survive for much longer periods in bones. Infected countries may also have restrictions specifying that meat may only be imported from zones within the country that are free of foot-and-mouth. Infection from imported meat can reach farms via waste foods being fed to pigs, and there are strict regulations relating to the storage of swill and to ensure that it is cooked in approved equipment for at least one hour prior to feeding.The virus is so infectious that air-borne spread is also a possibility. Many of the outbreaks of foot-and-mouth have started along the south and east coasts of England where migrating birds may have carried infection from the Continent. The outbreak which occurred on the Isle of Wight in 1981 was shown to have been carried by the wind alone and there is considerable meteorological data to support this. By a careful examination of the direction and speed of the wind, and of the prevailing temperature and humidity, it is now possible to predict mathematically the climatic conditions which might enable foot-and-mouth virus to blow across from Europe. This provides a useful forecast for times when extra vigilance is required.
At the time of writing the countries of the European Union are all considered free from foot-and-mouth, so there is relatively free movement of cattle from these countries into the UK. However, the movement of cattle from Eastern Europe into the EU and increasing EU membership from Eastern European countries represent a real threat.
Control of foot-and-mouth
Control is based on identification and slaughter of infected herds, plus restrictions on the movement of all livestock within a 10 mile radius, known as the infected area. Much larger controlled areas may be established if the disease is thought to be spreading. Slaughtered carcases, plus bedding and other infected material, must either be burnt or buried under six feet of earth.
The farm must be thoroughly disinfected and cannot be restocked for a further six weeks.Because of the rapid spread of infection, early identification of disease is vital and I would remind readers that it is their legal obligation to report even suspected cases of foot-and-mouth to the Divisional Veterinary Officer immediately. Failure to do so has in the past resulted in prosecution of stock owners, with quite heavy penalties being imposed.
Following the 1967-1968 outbreak of foot-and-mouth in Cheshire, one of the worst on record when 400,000 animals were slaughtered over nine months, stocks of vaccine were accumulated to carry out a ‘ring vaccination’ of animals around an infected area, should the disease ever get totally out of control. There are at least four good reasons why it is hoped that these measures will never be used.
• First, once Britain becomes an infected country, it will lose many of its export markets.
• Second, because there are a variety of different strains of foot-and-mouth, the vaccine in use may not be totally effective.
• Third, vaccinated animals can become carriers, shedding infection to other stock.
• Finally, and by no means least important, to give full protection, vaccination would have to be carried out each year, and in the long term this would be much more expensive than the current slaughter policy.

Plate 11.6. An aborted calf. This was at approximately the sixth month of pregnancy.
Brucellosis
Brucellosis is caused by an infection by the bacterium Brucella abortus. Its preferred sites in the body for growth are the uterus, udder, testicles and joints, although the uterus is by far the most important. Infection can only become established in animals of breeding age and although it is usually contracted by licking aborted calves or eating contaminated pasture, it can also be spread by an infected cow swishing her contaminated tail and flicking droplets of Brucella bacteria onto the eyes or noses of ‘clean’ animals.
Inside the cow Brucella grows in the placenta, especially on the cotyledons, leading to damage and loss of function. This then causes death of the calf and subsequent abortion, most commonly at the seventh or eighth month of pregnancy (Plate 11.6 shows a foetus aborted at about six months of pregnancy). Most cows abort once only, although they often shed infection for two weeks or more after subsequent normal calvings. Following abortion, infected cows frequently develop a chronic uterine infection. This endometritis leads to difficulties and delays in getting them back into calf. It also causes a uterine discharge, so that aborted cows may remain important sources of infection for several weeks.
Disease can spread very rapidly in a non-infected herd, and abortion ‘storms’, with a major part of the herd aborting, were once common. This led to a tremendous loss of calves and of milk in the first year and to production problems in the future because of the difficulty of getting cows back into calf again. The financial consequences were often disastrous. As dry cows are usually run together in a group, if one animal aborts there is a strong chance that infection will quickly spread to the others. This is because of the inquisitive nature of cows and the likelihood of their licking or sniffing the aborted foetus.
Other forms of brucellosis
In man, the infection is known as undulant fever, because it causes intermittent bouts of flu-like symptoms, with aching joints, severe lethargy and psychological depression. Because the Brucella bacteria grow inside the body cells (most bacteria live in the tissue fluid between cells) they are very difficult to kill with antibiotics and a course of treatment for six to twelve months may be necessary. (Pseudomonas, Chapter 7, and tuberculosis also grow inside cells.) Farmers, vets and slaughtermen are most at risk. Although milk can carry Brucella, it is not a common feature of infected cows and in any case the bacteria are destroyed by pasteurisation. Humans are usually infected by splashes from handling contaminated cows, the classic case being a heavily infected retained placenta following abortion.
Brucellosis can also occur in horses and dogs where it may cause chronic joint or tendon infections, for example fistulous withers in horses. Bulls may develop brucellosis in the testicles and could spread infection during service, although most infected bulls become sterile and would therefore be culled.
Control of brucellosis
In 1967 a voluntary register of non-infected herds was started in the UK and eradication began in 1971. Initially all calves between three and six months old were vaccinated free of charge with a live ‘Strain 19’ vaccine and in more severely affected herds the killed ‘45/20’ product was used in adult animals. Although a few carriers persisted, vaccination dramatically reduced the incidence of abortion storms and therefore decreased the spread of infection within herds. This policy was combined with a ‘test and remove’ regime. All breeding stock were subjected to blood tests at intervals of four months. Infected animals were identified and removed on each occasion. Milk ring tests on bulk milk supplies from each farm gave further assistance in detecting infected herds.
Current testing involves a monthly milk ring test on bulk milk, biennial blood testing of all bulls and of female cattle over two years old which are not in the milking herd, and abortion investigations. On 1 October 1985 the whole UK was designated as being Officially Brucellosis Free (OBF). This meant that 99.8% of all the herds in the country were free, but since then sporadic cases have occurred. For example, in 1985 there were still 69 herds from which Brucella had been cultured, the majority of these being associated with an outbreak in Somerset. Extensive movement of cattle, especially through dealers’ premises, is thought to be a major factor in the spread of the disease. The last cultural isolation of Brucella in the UK was from an imported heifer in Anglesey in October 1993. Blood-test-positive animals occur from time to time, but these are subsequently shown to be false positives.
The early identification of infected cows is vital, especially as vaccination was discontinued on 1 November 1978. This means that the national herd is now highly susceptible. For this reason, farmers have a legal obligation to report all cases of abortion or premature calving to their local Divisional Veterinary Officer. Affected animals should be isolated to prevent possible spread of infection to others and samples of blood, milk and placenta and/or uterine discharge may be taken and tested for brucellosis. If you wish the laboratory to check for other causes of abortion, including leptospirosis, then ideally the whole foetus and part of the placenta should be submitted as fresh as possible. Other causes of abortion are listed in Appendix 2 and discussed in Chapter 8.
Warble Flies
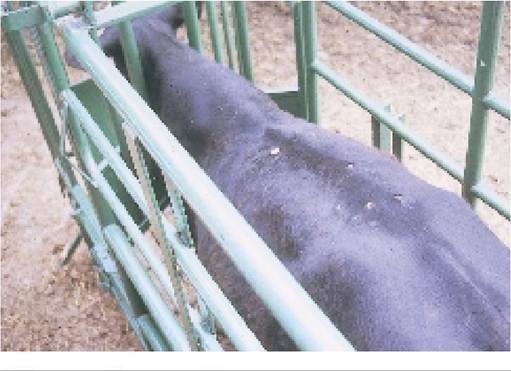
There are two species of warble fly, Hypoderma bovis and H. lineatum. They have very similar life cycles which are shown in Figures 11.1 and 11.2. Adult flies lay their eggs on the skin of the animal’s abdomen and legs during May to August, with H. lineatum attacking primarily the front legs and H. bovis the hindquarters of the animal. The eggs hatch into small larvae which burrow through the skin and into the tissues. They then migrate upwards through the other organs, some having a ‘rest’ stage in the oesophagus (H. lineatum) or around the spine (H. bovis) before arriving under the skin of the back from January onwards. There they make small breathing holes through the skin and the larva stays in one place, feeds and begins its slow transition towards the pupa stage. From the end of March to May the warbles may be seen as lumps under the skin of the back (Plate 11.7). Eventually they emerge as large white fleshy grubs, falling to the ground to pupate, that is to finish their development into adult flies in four to six weeks.
Damage caused by warbles
This is of four kinds. Firstly the noise of the adult fly frightens cattle, and herds of dairy cows may become restless and start ‘gadding’. This obviously depresses milk production and growth and can lead to physical injury, especially to the udder and teats. Secondly the presence of large numbers of warbles under the skin in the spring is very uncomfortable and this also reduces production. Third the air holes made by the warbles render this part of the hide useless for leather and the back is the most valuable part
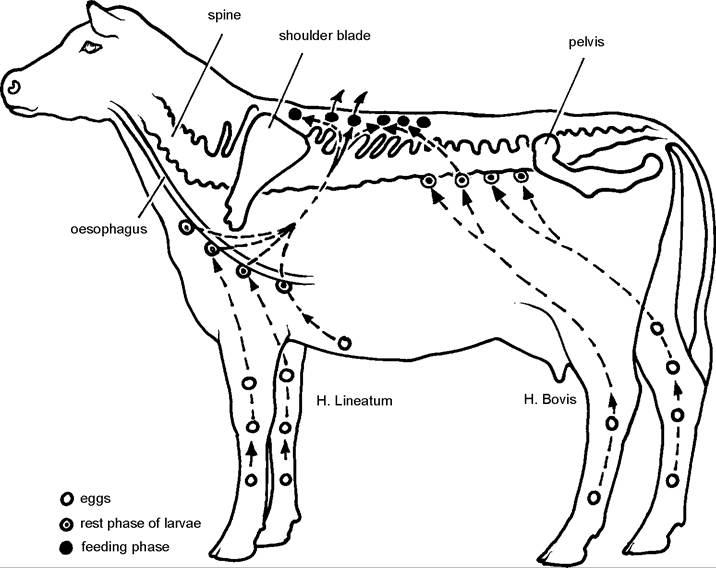
Figure 11.1. Life cycle of warble fly. Hypoderma Iineatum lays its eggs on the animal's front legs and its larvae have a rest phase in the oesophagus, whereas H. bovis lays its eggs on the hindquarters and the larvae ‘rest' adjacent to the spine. Both types of larvae arrive under the skin of the back from January onwards where they undergo a feeding phase before falling to the ground to pupate.
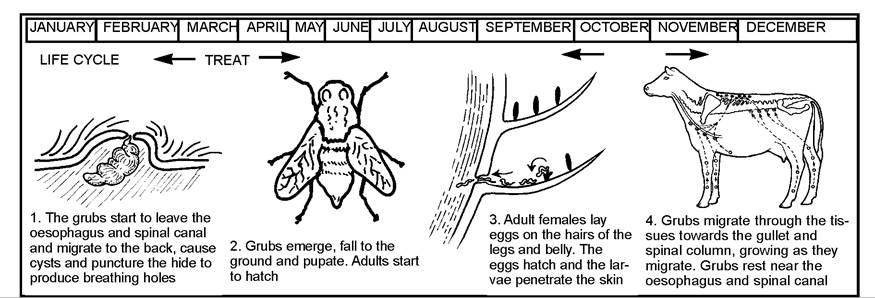
Figure 11.2. Warble fly migration and treatment period.
of the hide. Finally, occasional larvae migrating through the body enter the spine and cause paralysis, although this is more common when treatment is applied incorrectly.
Treatment and control
Plate 11.7. Warble fly larvae emerging from the back at the end of their feeding phase in March/April. They now fall to the
Traditionally the animal’s back was scrubbed with derris to kill the emerging larvae; this has now been superseded by organo-phosphorus pour-on preparations such as 20% phosmet, and by the avermectins. The OPs are about 98% effective if applied during the autumn (Figure 11.2) but less efficient for spring treatments. Organo-phosphorus preparations cannot be used between 20 November and 15 March. Although the vast ground and pupate into adult flies. majority of larvae migrating through
the spine cause no damage, if they are killed by organo-phosphorus compounds when at this site, they can stimulate a hypersensitivity reaction by the animal. This causes inflammation, swelling and pressure on the spine and may lead to paralysis of the hind legs. Several cases of treatment outside the recommended time periods have resulted in animals having to be sent for slaughter. It is interesting to note that the avermectin group (ivermectin, moxidectin etc) can be used at any time during the winter and as such is an extremely useful drug to administer to cattle which are being housed later in the year, for example in December, because it kills lice, mange, warbles, lungworms and intestinal worms, including the inhibited stages of type II Ostertagia larvae.
In 1978 legislation was introduced in the UK to make it compulsory to dress all obvious warble-infested cattle in the spring and this was accompanied by a vigorous advertising campaign to encourage voluntary autumn treatments, since these are more effective. There is now a legal obligation for stock-owners and others to report all suspected cases of warble-fly infestation. There are movement restrictions and compulsory treatment regulations for infected and adjacent herds and a compulsory herd inspection and treatment at the owner’s expense if these regulations are infringed.
In the first five years of eradication, the incidence of infested cattle was reduced from 34% (1979) to 0.02% (1983) with Anglesey having a significant pocket of infection. From 1983 most of the infection was in the south-west of England, and the percentage of herds affected decreased rapidly each year:
| Year | % of herds infected | Number of affected cattle |
| 1978 | 40 | — |
| 1979 | 34 | — |
| 1982 | 0.02 | 705 |
| 1984 | 0.01 | — |
| 1986 | 0.0009 | 34 |
| 1989 | — | 2 |
No live warble larvae have been found on British cattle since 1990 and the final stages of eradication were carried out by means of serological surveys (blood testing). In 1991 there were four blood-test-positive animals from 300,000 examined, and by 1993 this had fallen to zero. The UK is now declared officially free from warbles. All imported cattle must be treated on arrival.
Enzootic Bovine Leucosis (EBL)
This is a virus infection of cattle which produces tumours in the lymph nodes. Affected animals develop hard swellings under the skin, approximately the size of a flattened grapefruit, and the skin moves freely over them. Weight loss is quite marked. Other clinical signs may be seen, for example chronic bloat due to an enlarged lymph node in the chest compressing the oesophagus, or roaring breathing from pressure on the trachea. There is no treatment and affected animals slowly die.
A word of caution, however. There are other causes of tumour development in the lymph nodes and other organs, for example sporadic bovine leucosis. This is a different viral condition, and blood samples need to be taken to confirm the diagnosis. A skin form of lymphosarcoma is shown in Plate 10.17.
Transmission of infection
Calves are born free of disease but become infected via the colostrum during the first few hours of life. In infected animals the virus is found only in the lymphocytes. Lymphocytes are one of the types of white blood cells and are the main constituent of lymph nodes. The DNa of the virus actually becomes incorporated into the nucleus of the lymphocyte cell, and in so doing it alters its chromosome pattern and therefore the genetic content of the lymphocyte. This is a ‘natural’ form of genetic engineering.
Transmission to in-contact animals can only occur following transfer of infected blood cells and this can be via colostrum, blood-sucking insects, contaminated injection needles or even sputum, as sputum contains white blood cells. Only 0.0005 ml of blood is needed, an amount far too small to be seen with the naked eye. Even so, the risk of spread from one animal to another by physical contact is very low and by far the most important method of transmission is from the cow to the calf by colostrum. This means that provided infected animals can be identified and removed, control and eradication should be easy.
Control of EBL
The disease was made notifiable in the UK in 1977 and in the following year imported cattle and their progeny, a total of 9000 animals, were blood sampled. Evidence of infection was found in 67 Canadian Holstein animals and in two others but even then only 20% of the calves from the infected cows were carrying EBL. A register of EBL-free herds was established in January 1982, based on two consecutive clear blood tests, and this became a self-financing part of the Government Cattle Health Scheme in 1987. All cattle tumours found at meat inspection or at post-mortem must be reported to the Ministry of Agriculture and tested for EBL. Because of the low rate of transmission of infection and the accuracy of the blood test, it is likely that EBL will soon be eradicated from Great Britain. In 1995 there were only seven animals from seven herds, and in 1996 six animals from five herds.
Tuberculosis
This is a bacterial infection caused by Mycobacterium bovis and was once one of the major diseases of cattle, especially when milking cows were tied in byres (shippons) in close contact with one another. It was estimated that well over 40% of all such animals were infected. Many developed tuberculosis in the udder. This led to infected milk and hence to human tuberculosis, known as consumption. Tuberculosis in man, especially children, was extremely common. In the UK in the 1930s some 15,000 people each year were said to be infected, with over 2000 dying and others remaining debilitated for life. Although animal reservoirs of infection did play a part, tuberculosis in man was due primarily to the poor standards of housing and hygiene at the time which permitted a greater spread of infection within the community. Pasteurisation of milk prior to sale was a major measure which reduced the spread of TB from animals to man.
It is now very unlikely that clinical tuberculosis will ever be seen, although it should always be considered in cows with gross thickening of the udder, or in cows which progressively go thin and cough up blood and pus (Plate 11.11).
Eradication of tuberculosis
A voluntary scheme to establish a register of free herds was started in 1935 and by 1950 there was a sufficient pool of clean stock to introduce compulsory eradication. This was generally very successful and by 1960 the whole country had reached the Attested Herd status. Testing is based on the comparative intradermal test. Two sites, one above the other, are located on the side of the neck by means of a scissor mark. The skin thickness at each point is measured using a pair of special calipers (Plate 11.8) and then a small volume (0.1 ml) of tuberculin is injected (Plate 11.9). The injection is made into the skin and not under it, that is intradermally and not subcutaneously. Tuberculin is an extract of tuberculosis bacteria and if an animal has been previously exposed to TB it reacts to tuberculin by producing a nodule at that point.
The test is a ‘comparative’ measurement, with injections of avian and bovine tuberculin being necessary. This is because there are conditions other than bovine tuberculosis which can occasionally give a reaction to bovine tuberculin. These include avian TB and skin TB, neither of which is harmful to cattle or man, and Mycobacterium phlei (an infection found on certain grasses), M. kanasii and Johne’s disease (M. johnei, Chapter 13). Only M. johnei produces disease in cattle. Skin TB nodules are most commonly seen on the neck (Plate 10.18), legs or chest. The nodules are under the skin, not in it. It has been suggested that they may also be a sign of bovine immunodeficiency virus (BIV) (see Chapter 14), but as they are so common in the UK, this seems unlikely. Since the introduction of purified protein derivatives (PPD) of tuberculin, these cross-reactions have become much less important.
Plate 11.10 shows a beef cow which has reacted to the TB test. Note how the swelling at the bovine injection site (the lower one) is considerably larger than at the avian, indicating a positive reaction to the test. This animal is classified as a reactor. After the test the cow was isolated and when slaughtered, small caseous nodular lesions were found within the carcase, from which TB was cultured. The whole herd then had to be retested at intervals of 60 days until two clear tests were achieved.
Plate 11.8. Tuberculosis testing. Two sites are identified by means of scissor marks and the skin thickness measured.
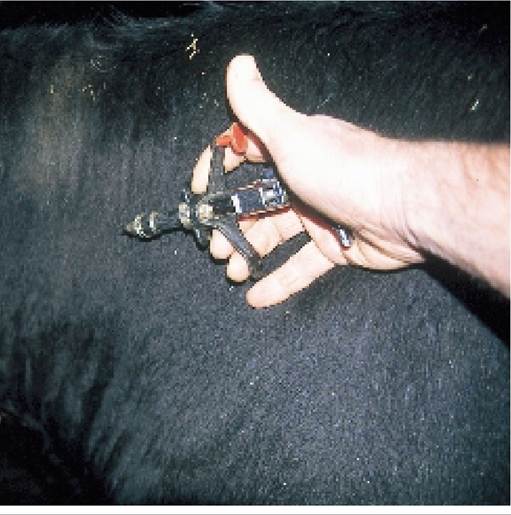
Plate 11.9. Tuberculosis testing. Asmall volume (0.1 ml) of tuberculin is injected into the skin, avian at the top and bovine at the bottom site.
Of the cattle which are classified as inconclusive reactors (IRs) at the initial skin test, only 1.0% have TB. The majority pass when retested after 60 days.
Although the skin test has its imperfections, it is rapid, cheap and easy to carry out and is likely to be used for the foreseeable future. Its major problems are:
False negatives In the advanced stages of TB the cow becomes desensitised by a heavy challenge of infection. This is known as the anergic state and is typified by the cow shown in Plate 11.11. Because she was in a herd under movement restrictions, she was tested for TB to allow casualty slaughter on account of her chronic nasal haemorrhage. She passed the intradermal TB test - but was found to be heavily infected with TB two days later at the abattoir!
It is also possible that cattle slaughtered very soon after infection (especially lung infection) may have small lesions at post-mortem, but do not react to the intradermal test.
False positives In a proportion of animals which fail the test (viz they are classified as reactors), no TB is found at post-mortem. These are known as no visible lesion (NVL) reactors.
There are two possible reasons for false positives, namely:
• TB is present in the carcase, but is not found at post-mortem.
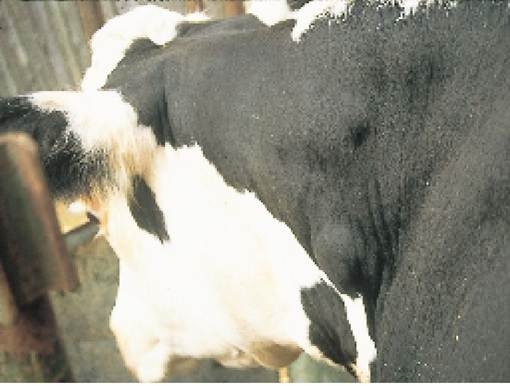
Plate 11.10. Tuberculosis testing. This animal is a reactor and TB lesions were seen at post-mortem. Note how the bovine (lower) reaction is much greater than the avian.
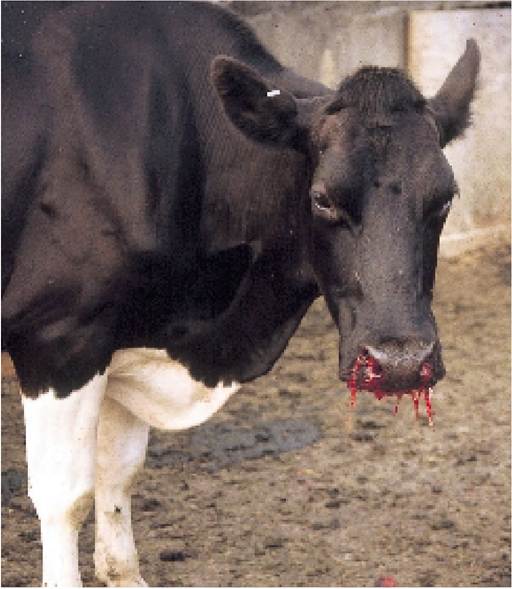
Plate 11.11. Tuberculosis testing - an anergic animal. Because she was so heavily infected with TB in her lungs (leading to bleeding from the nose), the intradermal TB test did not work.
Detailed dissections of such reactor carcases have shown that the TB nodule present might be as small as a pinhead, but even this is enough for a few of them to be shedding infection to other cows. • The animal has been exposed to TB but has since recovered. She will continue to give a positive
reaction to the test for a considerable period of time. This probably accounts for 70% of the NVL reactors.
As in the UK only 50 cattle each year are found to have TB at the abattoir, the skin test must be reasonably effective!
Tuberculosis in badgers
In 1970, despite the falling incidence of cattle reactors in most areas of the country, the level of infection in parts of Gloucestershire, Avon and a few other counties in the UK remained unchanged at around 0.1%. This was associated with the high incidence of TB in badgers in these areas. It may well be that cattle infected the badgers initially, but in areas of heavy badger density, and where they are living in close confinement, tuberculosis in badgers is rife. The Cotswold hills provided an ideal habitat and in the mid 1970s 27% of badgers examined in this area were found to be infected, rising to 33% in 1996! Compared with cattle, badgers have relatively little resistance to TB. Once infected, disease spreads rapidly and especially in the final stages, badgers excrete large numbers of bacteria in their urine, faeces and saliva. Unfortunately, because of their different immune system, the intradermal (= tuberculin) test used in cattle does not work in badgers and even blood samples are not particularly accurate. Cultural examination of urine, faeces and sputum can be used, but isolation of TB from faeces is difficult because so many other bacteria are present and because all TB cultures have to be incubated for several weeks.
Badgers like to dig in sandy soil and prefer to have a rocky roof to their sett, so wooded escarpments form their favourite habitat (Plate 11.12). On the other hand, as 60% of their diet consists of earthworms, they like to forage over short grazed pasture, in other words, where cattle might graze. Dry summers used to reduce the number of available earthworms and consequently the number of badgers. However, the increase in the quantity of forage maize being grown now more than compensates for this.
There are thought to be two main methods of transmitting infection to cattle, pasture contamination and contamination of feedingstuffs. The former is especially common because badgers have a specific ‘latrine’ area on pasture some distance away from their woodland sett and of course cattle will sniff and lick any unusual objects including badger urine and faeces. Second, badly affected badgers become weak and are no longer able to dig and forage for their food. This drives them towards farm buildings for eas-
ier access to feedingstuffs and hence TB contamination of cattle feed- ingstuffs can occur.
As the incidence of TB in badgers is very much higher than in cattle, it seems most probable that infection flows from badgers to cattle and not cattle to badgers. In the long term the elimination of infected setts must be beneficial to badgers as well as to cattle and man. However, elimination also has its problems. Because infected setts can become repopulated quite quickly by other badgers and as TB can live in the soil for up to two months, there is a risk that a repopulated sett will become reinfected. Similarly if you have a sett on your farm and no TB in the cattle, then you are legally bound to leave that sett intact. In any case, eliminating could lead to repopulation - and possibly with infected badgers!

Plate 11.12. A badger sett, typically found in sandy soil in a wooded area.
The motor vehicle is one of the main ‘predators’ of the badger. It has been estimated that 50,000 deaths each year are caused by road accidents. This represents 50% of all adult badger deaths - and should be compared with the 1000 badgers per annum eliminated by the culling of infected setts! In TB infected areas of the country road traffic deaths are commonly submitted for post-mortem and around 25% of badgers are infected with TB. This should be compared with the finding that in 1996 32% of all badgers trapped on the basis of being in contact with infected herds were positive. This must surely be further strong evidence supporting the link between TB in badgers and cattle.
From the mid 1970s control of TB in badgers was carried out by gassing infected setts with cyanide, but in 1982 trapping was introduced because it was said that death following exposure to cyanide was inhumane. Since then there have been numerous changes in badger trapping, testing and elimination policies, due primarily to political pressure from badger protection groups, who consider that the case against badgers is unproven.
After 1975, with the introduction of unrestricted gassing of those badger setts associated with TB-infected cattle, there was a sharp reduction in the number of new infected herds. For example, in the counties of Gloucestershire and Avon the number of new herds having ‘reactors’ to the intradermal tuberculin test fell from 123 herds per annum in 1976 to around 40 per annum (range 36-48 over the years 1980-1988) by 1988 (Figure 11.3). Not all ‘reactor’ herds are confirmed by visible lesions or culture (although it is estimated that at least 70% of unconfirmed cases do have TB) and so the number of confirmed infected herds each year fell from 68 in 1976 to around 20 (range 17-26) by 1988.
Gassing of infected setts was banned in 1982 and was replaced by the ‘clean ring’ trapping and elimination strategy which eliminated all infected setts within a mile of infected cattle. In 1986 this was again changed and the Dunnet strategy was implemented which only permitted trapping and testing of badgers on the farm which had TB infected cattle. If the sett happened to be in an adjacent neighbour's field, trapping was not permitted! Since then there has been a steady increase in TB, with approximately 180 new reactor herds in 1997 and a further increase in 1998. This change in the incidence of reactor herds in Gloucestershire is shown in Figure 11.3.
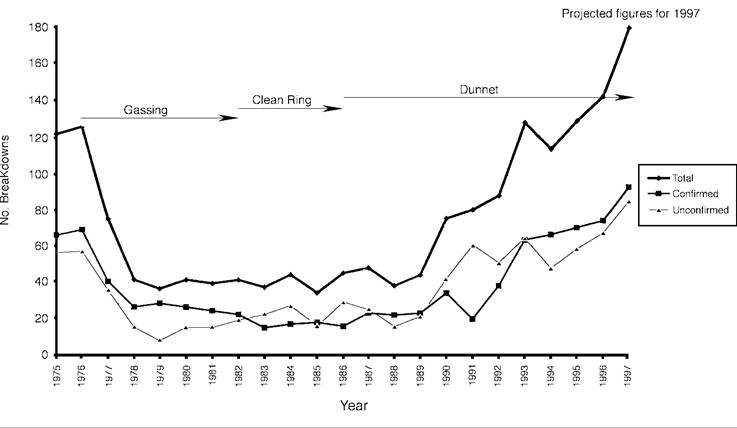
Figure 11.3. The incidence of new TB reactor herds in Gloucestershire and Avon from 1975 to 1997.
The future
Although there has been a limited trial of an oral administration system it will be many years before a vacine for badgers or cattle is available. Freedom from TB for cattle, badgers and man must be a logical long-term aim.
The massive increase in UK badger numbers (76% increase from 1985 to 1995) must have a contributory effect: as population densities increase, so will the rate of spread of infection to cattle. Some farms are already having to harvest their maize early in the autumn because of severe badger damage. Perhaps a limited cull will be permitted in the future.
In 1998 the report of the Krebs Committee in the UK proposed a field trial aimed at resolving the issue as to whether badgers are involved in the spread of TB to cattle. The trial, planned to last for at least
five years, was to be carried out (approximately 20,000 acres) would be subdivided into three treatments, namely
• in one area all the badgers would be totally eliminated for the five year period
• in the second area, badgers would only be eliminated if they were associated with farms where there is TB in cattle
• in the third area, only the badger numbers would be monitored. There would be no culling, irrespective of the incidence of TB in the cattle.
in TB ‘hot spots’. Each trial area of 100 square kilometres

The results of this trial are awaited with interest.
In the interim the only practical steps are to reduce the amount of contact between badgers and cattle. This can be achieved by keeping cattle away from badger setts by means of electric fencing and perhaps using fencing 150 mm above ground level to redirect badger tracks away from pasture land. Any bedding discarded by badgers from their setts in the spring, as in Plate 11.13, should be burnt (wear gloves when handling it, as it may be infected). Submit all dead badgers for post-mortem examination to ascertain whether or not they are infected with TB (Plate 11.14). Finally, make sure that feed stores and cattle food and water troughs are not accessible to badgers. This means that they should be at least 800 mm high with smooth, solid walls, with perhaps a protruding
Plate 11.13. The bedding discarded from badger setts in the spring, as seen here, is best burnt, as it could be infected with TB.

Plate 11.14. If you have TB in your herd, then it would be a wise precaution to submit any dead badgers found for a test for tuberculosis.
lip at the top. As mentioned previously, in the terminal stages badgers infected with TB are no longer able to forage for food and are therefore more likely to take the easy way out and eat cattle food, especially cereals. With even their saliva being infected, this represents a serious danger to the cattle and explains why young stock which have never been out to graze are sometimes infected with TB.
Attempt to minimise spread of TB from badgers to cattle by:
• fencing cattle away from badger setts
• burning potentially infected bedding discarded from the sett in the spring
• ensuring cattle water and feed troughs are not accessible to badgers
• submitting all dead badgers for post-mortem examination and testing
TB has been found in foxes, moles, ferrets and rats, but at a lower incidence and it is not known if these animals were shedding tuberculosis. If not, they are unlikely to act as a source of infection for cattle. Farmed deer have occasionally shown a high incidence TB, and there is concern this might spread to wild deer. Unfortunately for the badger, it is the only significant excretor of infection and as such, is likely to be a major reservoir for cattle. Until the problem has been resolved, TB in cattle may be controlled, but it will not be eliminated. In the longer term, it must be in the interests of man, cattle and the badger itself to have a healthy badger population.
Bovine Spongiform Encephalopathy (BSE)
First reported in 1986, BSE became one of the greatest issues ever to strike the British cattle industry, although it was the politics surrounding the disease, rather than the disease itself, which led to such massive economic losses. It was not until the end of 1998 that the world-wide export ban imposed by the EU on beef produced in the UK was lifted, and even then there were stringent restrictions, with only fully traceable animals under thirty months of age eligible for export. All the available evidence suggests that this epidemic will have virtually died out soon after the year 2004.
Clinical signs
The disease is seen primarily in mature dairy cows, three to six years old, with a variety of clinical signs including:
• weight loss, partly due to poor rumination
• incoordination: affected animals walk with stiff hind legs and may almost fall if rushed around a sharp bend
• excessive licking of the nostrils, first one side then the other, and sometimes biting the flanks and grinding the teeth
• ears flicking to and fro, and the skin over the chest and flanks twitching and fluttering repeatedly, as if flies were landing on it
• general apprehension, for example cows may appear nervous when entering a narrow doorway into the milking parlour; they may over-react with jumping and pricked ears at the sound of a hand-clap (Plate 11.15); and they occasionally kick violently and aggressively in the milking parlour. Aggression, such as attacking farm staff in the yard, is a rare feature and only occurs when the animal has been separated from the others and feels threatened
• in the terminal stages affected cows become recumbent with a characteristic ‘dog-sitting’ posture as shown in Plate 11.16.
If the condition were to progress, cows would be so uncoordinated that they would become recumbent and would eventually die from inability to eat and drink, and from self-inflicted injuries. There is no treatment.
No animal is ever allowed to progress to this stage in the UK, as it is a legal requirement that any animal showing any suspect signs of BSE is reported to the Ministry of Agriculture. The compensation paid to farmers is sufficient to encourage them to do so.
After a Ministry veterinary officer has confirmed the tentative diagnosis of BSE from clinical signs, the animal is destroyed by lethal injection and the head is taken away for examination.
Despite the quite characteristic clinical signs, there is as yet no test available in the live animal and confirmatory diagnosis can only be carried out by a microscopic examination of the brain at post- mortem.
Causes
BSE is one of a family of transmissible spongiform encephalopathies (TSEs), all of which are caused by closely related infections. The infectious agent has yet to be identified but it is most probably a prion, a subcellular protein particle, which replicates by becoming incorporated into the host cell. TSEs are not a new phenomenon: they have been in existence for many years. Examples (and the year in which they were first identified) include:
• Scrapie in sheep (1732)
• Kuru in man (1900)
• Creutzfeldt-Jakob disease (CJD) in man (1920)
• Transmissible mink encephalopathy (TME) (1947)
• Chronic wasting disease in eland and kudu (1967)
• Bovine spongiform encephalopathy
(BSE) (1986)
• Feline spongiform encephalopathy
(FSE) (1990)
All these diseases have a similar epidemiology, namely a very long incubation period of several years, after which ‘spongy’ vacuoles appear in specific areas of the brain (the brain stem) and lead to nervous signs. The average incubation period for BSE is around five years, although it can be as little
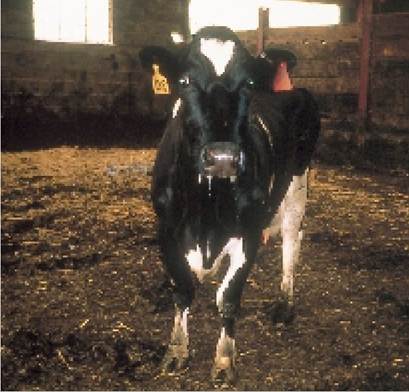
Plate 11.15. An animal with BSE over-reacts to a hand-clap, as in this cow. Note the startled look in her eyes and erect ears. She has also lost weight.

Plate 11.16. More advanced cases of BSE become recumbent and adopt a dog-sitting position.
as two or three years, with the youngest confirmed case being twenty months old.
All TSEs are progressive and always fatal. There is absolutely no treatment. Animals should be destroyed as soon as the diagnosis has been made. Death from TSEs in man is most unpleasant.
Epidemiological studies of the occurrence of BSE strongly indicate that it is associated with the feeding of meat and bone meal. Changes in the production of meat and bone meal in the early 1980s led to its being manufactured without the use of solvents and on a continuous production line, rather than on a batch basis. The lower incidence of BSE in Scotland is thought to be due to the fact that they continued with solvent and high temperature processing for much longer, although experimentally, solvents have
had litle effect on the viability of the BSE agent. It is now known that temperatures probably in excess of 140°C are needed to destroy the agent, preferably under steam.
At the same time as these changes occurred in the rendering industry there was a considerable increase in sheep production, and therefore sheep slaughtering, in the UK and a switch towards the use of meat and bone meal because of high world soya prices. It remains unknown whether BSE is a mutation from scrapie in sheep or whether it is an infection which has always been present in cattle and the relaxation of offal processing in the early 1980s led to it recycling to produce very high levels of disease. Using mouse infectivity titrations, the BSE agent does not resemble any of the known strains of sheep scrapie and it would appear that there is only one strain of BSE.
Control measures
In June 1988 BSE was made a notifiable disease. After this date all animals suspected of having the disease were incinerated and removed from the human food chain. In July 1988 a ban was imposed to prohibit the use of ruminant meat and bone meal (rM+BM) in ruminant rations. In June 1990 the use of certain bovine offals in human food was prohibited: brain, spinal cord, spleen and tonsils of animals over six months old, plus the thymus and intestine of calves less than six months old, all of which were termed specified bovine offals (SBOs). Then in September 1990 these SBOs were also banned from use in rM+BM for any livestock diets and had to be stained at the abattoir and then incinerated. Because such small quantities of brain (1.0 g) were found to be infective to cattle, later the whole head (excluding the tongue and lower jaw) became included and it was all known as specific bovine material (SBM). It had proved impossible for all traces of brain to be completely removed from the skull and there was concern that in attempting to remove it, nervous tissue might leak onto meat which would be used for human consumption.
These measures led to a dramatic reduction in the incidence of BSE from 1993 onwards (the average incubation period being 5 years). However, there were still far too many animals ‘born after the ban’, i.e. after July 1988, which developed BSE. At that stage it was realised that only a very low dose (1.0 g) of BSE infected brain tissue was needed to be ingested by a calf to cause disease. Despite the ban on feeding rM+BM it was found that some infective material was still getting into cattle diets. This was occurring because of:
• cross-contamination in feed mills. At this stage rM+BM was still being used in horse, pig and poultry food
• failure to keep SBOs totally separate at abattoirs, knacker yards and hunt kennels, so that even non-ruminant derived meat and bone meal (nrM+BM) was found to contain traces of ruminant SBOs
There was considerable tightening up of feed mill and abattoir practices to prevent this cross-contamination. Then in November 1994 a ban was imposed to prohibit the use of all mammalian (viz in addition to ruminant) M+BM to any ruminants. In March 1996 this was further strengthened by banning the feeding of any mammalian M+Bm to any livestock species and it is now an offence even to leave it in the mill! This was monitored by careful checks on animal feed using an ELISA test, able to detect very low levels of mammalian M+bM. Consequently it was not until August 1996 that all traces of meat and bone meal were removed from all ruminant feeds and it will be the year 2000 and beyond before we can be sure if this was totally effective.
Birth records and double tagging
A second part of the BSE control measures involves records of animal births and movements. All cattle born since 1 July 1996 have an individual passport which goes with them from farm to farm until they reach slaughter. It is illegal to trade in animals which do not have passports, none can be sold for human consumption, and to attempt to do so would result in a heavy penalty. Movement records had been a statutory requirement for many years, but as a result of the BSE episode, the following records have become mandatory for cattle in the UK:
• all movements to be recorded within 36 hours of the movement occurring
• births of dairy calves and their individual ear-tag to be recorded within seven days of birth
• births of beef calves and their individual ear-tag to be recorded within 30 days of birth
• the identity (ear number) of the dam to be recorded in each case
• deaths reported within seven days
• replacement of ear-tags to be recorded and reported within 36 hours
• all calves to be double-tagged, viz they must have a tag in each ear
The idea behind such comprehensive recording was to allow tracing of animals which had possibly been exposed to BSE and to confirm their age at slaughter for human consumption.
Cohort and offspring cull
In an attempt to reduce the incidence of BSE even faster, and in so doing win political approval to restart UK beef exports, it was decided to cull and incinerate those animals which were most likely to develop BSE later in life. This consisted of two groups, namely
• the birth cohorts. These were animals born on a farm at the same time (defined as within the same year) as a cow which later developed BSE. These animals were thought to be at special risk because, as calves, they would have eaten the same food as the BSE animal.
• the offspring cohorts. In 1998 it was decided to cull all offspring born to BSE cases after 1 August 1996. This represented a considerable tracing exercise, with approximately another 1000 animals found, culled and incinerated.
Progress of control measures
The incidence of BSE reached its peak in late 1992/early 1993, when 1000 cases were being reported each week. By October 1998 there had been over 172,500 confirmed cases of BSE slaughtered and incinerated, 37,187 of which had been born after the July 1988 meat and bone meal ban. By June 1997 67% of dairy herds and 15.8% of suckler beef herds had had at least one case. However, the weekly incidence had decreased by a factor of ten to less than 100 cases a week and by October 1998 the number of animals born after the ban was also showing a sharp decline:
Year of birth
Number of cases to October 1998
| July-Dec 1988 & 1989 | 24,483 |
| 1990 | 5,524 |
| 1991 | 4,254 |
| 1992 | 2,350 |
| 1993 | 1,057 |
| 1994-95 | 110 |
Despite the characteristic clinical signs and the considerable experience of the veterinary personnel carrying out the clinical examinations, approximately 15% of all animals slaughtered as suspect BSE eventually proved to be negative, with listeriosis being one of the main diagnoses in negative cases. As the incidence of BSE fell, so the error rate of diagnosis increased, reaching almost 20% by 1997. By this time around 20,500 animals had been slaughtered as suspect BSE cases but were subsequently found to be negative at post-mortem.
It is impossible to explain why other European countries, supposedly virtually BSE-free, failed to identify similar numbers of suspect animals, that is animals which showed typical signs of BSE but which were found to be negative on post-mortem examination. After the UK, Switzerland reported the second highest number of confirmed cases (228) and Ireland the third (188), but in both cases the numbers are nothing to match the incidence (172,000) in the UK. Considerable concern was also raised about possible under-reporting in other European countries when a survey of cattle exported from the UK prior to 1989 was published in 1997. This survey compared the actual numbers of BSE cases reported in cattle exported from the UK with the predicted incidence, that is the incidence that would have occurred in those cattle if they had remained within the UK. The figures reported were:
| Predicted incidence to Jan 1997 | Reported incidence | |
| UK | n/c | 165,323 |
| Switzerland | n/c | 228 |
| Ireland | 911 | 188 |
| Portugal | 262 | 61 |
| France | 32 | 28 |
| Germany | 243 | 5 |
| Italy | 50 | 2 |
| Denmark | 29 | 1 |
n/c = not calculated
In addition, as many thousands of tons of both infected meat and bone meal and cattle concentrates were exported from the UK prior to 1989, it is impossible to speculate why this apparently did not produce BSE in any European country apart from Switzerland.
Maternal transmission
There is little firm evidence for significant maternal transmission. Studies of field cases of BSE show:
• the incidence of BSE in the offspring of BSE dams was not higher than the national average
• when one case had occurred, an individual farm was no more likely to get further cases of BSE than any other farm
A similar trend was found when offspring from BSE and non-BSE dams were purchased from farms and reared to seven years old. Most of these animals had been reared for several weeks on the farm of origin and had therefore been exposed to potentially BSE contaminated feed. Although initial results suggested a maternal transmission rate of around 10% when the calf was born within six months of the cow developing BSE, extrapolation to the field situation showed that if maternal transmission of BSE existed, it was at a very low level and certainly not sufficient to have a significant influence on the course of the epidemic.
BSE and human health
This was the aspect of BSE which had the least proof and yet politically produced the most devastating consequences for the cattle industry throughout Europe and even throughout the world. The concern was that tissues from BSE-infected cattle could enter the human food chain and lead to CJD in man. There was no definitive evidence that this was occurring, but near panic broke out when in March 1996 the CJD Surveillance Unit in Edinburgh announced that ten cases of a variant form of human CJD (nvCJD) had been identified in an age group under 45 years old. Because no other explanation was readily available it was assumed that these nvCJD cases were associated with the consumption of BSE-infected beef or beef products (Will R.G. & others (1996), The Lancet, vol 347, p. 921).
In March 1996 this caused the collapse of the beef industry in Europe and a considerable depression in beef consumption worldwide, brought about in no small part by EU governments grossly over-reacting and imposing a worldwide ban on the export of all UK beef and beef products. At the same time all animals over 30 months of age (both clean beef and barren cows) were considered to be unfit for human consumption and the Government paid compensation to the farmers for them to be slaughtered and rendered or incinerated. By October 1998 over 2.5 million animals had been destroyed in this way and at the same time the Government was paying farmers to slaughter male animals within the first few weeks of life.
It should be remembered that this took place despite the fact that almost all the available evidence suggested that by that stage of the epidemic there were so many controls in place that meat was quite safe to eat. For example:
• Even in affected animals the BSE agent had only ever been found in the brain and spinal cord, and all affected animals had been slaughtered and incinerated since June 1988.
• Even when meat and milk from animals clinically affected by BSE was injected into the brains of mice, no BSE was reproduced.
• From June 1990, all specified offal (bovine brain, spinal cord, thymus, spleen and intestine) had been removed from the food chain.
• From March 1996, no animal over 30 months old was permitted to enter the human food chain.
• In animals known to be incubating the disease following a very heavy (100 g) experimental challenge of infection, the agent had been identified only from the small intestine - which at this stage was being discarded - in all animals under 30 months old. All other tissues were ‘safe’, including the brain and spinal cord.
• From December 1997, it even became illegal to sell beef ‘on the bone’ because of the risk that, in animals incubating BSE, the dorsal root ganglia (part of the nervous system) might contain the BSE agent.
The latter measure was considered by many people to be an ‘over-kill’ in terms of food safety. It had been calculated that even if the beef was not deboned, there was only a 5% chance that one person in the UK might develop nvCJD. This equates to a risk of one in 600 million, and should be compared to other UK risks, for example being struck by lightning (1:10 million), murdered (1:100,000) or dying from a smoking related illness (1:200). Despite all these additional safeguards, the worldwide export ban on UK beef was retained until 1998.
Experiments did show a similarity between mice injected with BSE and nvCJD, whereas mice infected with classical CJD were different. This is by no means proof that BSE was the cause of nvCJD, however. If there had been any risk, ever, it had occurred prior to June 1988, at the time before BSE had been made a notifiable disease, or possibly before specified offal had been removed from the
| Summary of BSE legislation | |
| June 1988 | BSE made a notifiable disease and all animals showing clinical signs removed from the food chain and incinerated |
| July 1988 | Feeding of ruminant M+B to ruminants prohibited |
| June 1990 | SBO from all healthy cattle removed from the human food chain |
| September 1990 | SBO from all cattle banned from inclusion in any livestock diets |
| November 1994 | Ban on feeding ruminants mammalian M+B from any source |
| March 1996 | Total ban on feeding all livestock mammalian M+B from any source |
| July 1996 | Compulsory registration of all calf births, with passports issued |
| August 1996 | No further traces of M+B detected in routine compulsory screening of rations. |
| 1997-99 | Cull of cohorts from BSE farms: - birth cohorts = animals born at the same time as BSE case. - offspring cohorts = calves born to BSE dams |
food chain in June 1990. Transmission has never been shown possible in milk, even when milk from confirmed cases of BSE was injected into the brains of mice. Despite this, and as an additional safety precaution, milk from suspect BSE cows is always discarded.
In spite of these reassurances, there were still certain high profile pseudoscientists predicting that there would be a cataclysmic outbreak of nvCJD and that we were about to ‘lose a generation of the nation’s children’. It has to be accepted that this is a possibility and it will be ten to twenty years after publication of this book before we can be sure it did not happen. With only thirty-five cases of nvCJD having occurred at the time of writing (March 1999), which is more than ten years after BSE was made notifiable, this seems highly improbable. In fact nvCJD case number 20 occurred in a person who had been a strict vegetarian since 1985, i.e. one year before the first case of BSE had been reported. By this stage even the national press was starting to doubt whether there was any connection, and possibly part of the increase in nvCJD cases was simply due to more surveillance. Other suggestions included a genetic link (consistent DNA pattern found in many patients), surgical intervention (nvCJD prions had been found in an appendix following routine removal), blood transfusions (nvCJD present in white cells) and vaccines prepared from bovine products. If nvCJD did originate from cattle, it is much more likely to have been transmitted by injection - i.e. from vaccines or blood - than by ingestion of food.
Salmonellosis
Many aspects of disease caused by salmonella have been covered already, for example in the young, bucket-fed calf (Chapter 2) and in the weaned animal (Chapter 3). This section deals with the disease in the adult cow and discusses some of the possible sources and the human health aspects. Salmonellosis is not a notifiable disease, but must be reported under the Zoonosis order.
There are many different strains of salmonella (almost 2000 in total) called serotypes. In the 1960s the commonest serotype in cattle was Salmonella dublin, but from mid 1970 onwards S. typhimurium became much more common and, in addition, a whole range of ‘exotic’ strains were encountered, with names like:
S. agona S. newport S. virchow
S. enteriditis S. heidelberg S. seftenburg
and many others. S. dublin is found almost entirely in cattle and the source of infection must therefore be direct or indirect contact with other cattle. S. typhimurium and the exotics, on the other hand, are much more widespread. Infection occurs in a whole range of animals, including man, which means that the possible sources of infection are much more variable.
Clinical signs
Salmonella particularly affects the intestine and scouring is therefore the most frequent clinical sign in animals of all ages. Dysentery is often seen, viz a profuse diarrhoea sometimes with blood, and often mixed with large pieces of ‘fleshy mucus’. This is the damaged lining of the gut being shed. Lactating cows completely stop milking, their eyes become dull and sunken due to dehydration, and they run a very high temperature. The dung will contain millions of salmonella bacteria and hence isolation is vital to reduce the risk of infecting other cows. Ideally use a loose-box with no drainage to the outside and particularly avoid surface drains which run across an open yard.
Infection with salmonella does not always cause scouring, however. Abortion, especially from mid pregnancy onwards, may be the only clinical sign seen, and salmonella can be recovered in very large numbers from the afterbirth. S. dublin especially may be involved and sometimes abortion may precede an attack of acute diarrhoea and death. S. dublin may also cause pneumonia, joint ill or even meningitis with nervous signs, and cattle of any age may be affected. I have also seen S. typhimurium isolated from an aborted cow showing no other symptoms and with no further cases occurring in the herd. This makes it very difficult when advising farmers what action they ought to take following the confirmation of salmonellosis in their herd. Even calvings induced with cortisone or prostaglandin may be sufficient stress to precipitate clinical salmonellosis in a carrier cow.
Treatment
Treatment is largely symptomatic, aimed as much at treating the symptoms as eliminating the disease. Kaolin and chlorodyne may physically help to control the scouring. Sick animals should be encouraged to drink by giving them warm water. Animals not drinking can be orally dosed with electrolyte, or given intravenous fluid therapy if severely dehydrated. Antishock treatments (such as the non-steroidal anti-inflammatory flunixin) help enormously and are certainly worth giving to very sick animals. Multivitamins may assist in the healing phase, especially if the rumen (the major source of B vitamins for the cow) is not working properly.
The use of antibiotics in the treatment of salmonellosis has been called into question on two counts: firstly because of the risk of antibiotic-resistant strains of salmonella spreading into the human population, and secondly because antibiotics may prolong excretion rates and produce more carrier animals. However, I consider that antibiotics are justified on both economic and welfare grounds. A septicaemic animal with a high temperature cannot be left to die and provided that an adequate dose of the correct antibiotic is administered for a reasonable period of time to a cow in isolation, personally I believe that the risk to the human population is extremely low. Although care should always be exercised, it has been suggested that most antibiotic resistance in man is likely to be due to the misuse of antibiotics in humans, rather than from any excessive use in animals.
Progress of a herd outbreak
Disease due to 5. typhimurium and the exotics appears to be much more common in the autumn and this is thought to be because warmth and humidity predispose to the survival and spread of the organism. The isolation of salmonella from one cow, whether she is scouring or following an abortion, should certainly cause alarm and lead to increased vigilance, but possibly no other immediate action is needed, apart from treatment and separating her from the remainder of the herd. Ideally, faecal swabs should be taken from her until at least two consecutive negative results have been obtained. The cow can then be released from isolation.
However, if the disease starts to spread, careful control measures will be needed. The precise details will depend on the management and design of your unit, and the action necessary should be discussed with your vet. As a general rule, calves from infected cows should be given ample colostrum and then penned individually to prevent the spread of infection. Nutritional stress, for example a sudden change in diet for either the cows or calves, should be avoided, because stress can precipitate an outbreak of disease. Separation of the different age groups of cattle is important, and any possible measures to prevent faecal contamination of food should be taken.
Salmonellosis often strikes batch-calving herds, with disease being seen as a severe scouring just after calving or following abortion. In such herds control measures should include:
• Calve each animal in isolation in a clean box. With the stress of calving, a cow which has been carrying salmonella may start shedding infection in her dung. Ideally every cow should remain isolated until faecal swabs are negative, even if not scouring. This is unlikely to be feasible in most herds.
• Vaccinate. A dead vaccine given at six weeks and three weeks prior to calving will provide good protection against both the enteric (i.e. scouring) and abortion forms of the disease and, through the transfer of antibodies in the colostrum, it reduces the excretion of salmonella and thereby reduces salmonella problems in calves. In the event of an outbreak, the whole herd should be vaccinated, irrespective of their stage of lactation or pregnancy.
• Minimise faecal contamination of food. This might entail keeping dogs, chickens, pigeons etc. away from feed stores and troughs and reducing the contamination of food by tractor wheels, e.g. by scraping passages more thoroughly. Do not walk on cattle food with dirty boots.
• Do not use dirty water from yard drains etc. for the irrigation of land currently being grazed.
• Feed diets which will not produce digestive upsets and which will lead to firm dung. The latter helps to reduce faecal contamination of feed.
• Minimise overcrowding and keep buildings well ventilated. Infection is more likely to spread if cattle are tightly packed into humid buildings.
• If possible, get the dry cows well away from the milking cows to minimise any chance of faecal contamination between the two groups. As it is the cow at calving who is most susceptible to salmonella, reducing her risk of contracting and spreading infection is all important.
• Dose for liver fluke in areas where fluke infection is a possibility, since even quite low fluke infestations appear to increase the likelihood of disease from S. dublin.
Sources of infection
From the early 1990s a specific strain of S. typhimurium, DT104, has become increasingly important both in man and in all species of farmed livestock. For example, in 1995 it accounted for over 30% of all salmonella incidents in cattle and was second in importance to S. enteritidis, PT4, in man. The DT104 strain is characteristically resistant to the antibiotics ampicillin, chloramphenicol, streptomycin, sulphonamides and tetracyclines, and a few strains are also resistant to trimethoprim. It is more pathogenic (i.e. causes more severe symptoms) than most other strains, with deaths occurring in around 40% of clinically affected cows and almost 50% of calves. This strain is also a greater risk to man and so careful hygiene measures are required.
By means of extensive swabbing, infected farms have been shown to have a widespread distribution of the organism. For example, it may be found in cubicles, feed passages, on tractors, cars, boots, drains, in rats and mice and often household pets. Sheep and pigs may also be carriers. With such an extensive reservoir it is difficult to instigate any effective control measures apart from vaccination.
The most common source of infection in calves is undoubtedly other calves which have been obtained via markets or through dealers’ premises. The reasons for this are given in Chapter 2 and clearly calves which repeatedly pass through such premises present an even greater risk. However, disease outbreaks in dairy herds are often not associated with recent purchases and other sources of infection need to be identified.
Exotic salmonella species may be found in imported feedstuffs, especially fishmeal. Current importations are routinely screened at the docks. Unfortunately no legislation exists for impounding such imports and by the time that the laboratory culture results are available, many consignments will already have been incorporated into feedingstuffs and are being fed to livestock. At least the monitoring is able to identify commonly infected sources, however. For example one type of South American fishmeal once featured prominently in the results. Pelleting and other heat treatments destroy many of the salmonellae during processing, so that the number of contaminated finished feeds will be very much lower.
Home-produced animal protein food, for example, from chicken offal, was also once a high risk, but the Protein Processing Order (1981) made it compulsory for all such material to be heat treated before its incorporation into feedingstuffs and this should no longer present any risk. The legislation would be considerably strengthened if compulsory powers of sampling were included, however.
Sewage is a further possible source of salmonella, from both human and animal origin. Human carriers are not uncommon and seagulls or other birds feeding on effluent discharged directly into estuaries, or from inadequately supervised septic outflows, have been shown to contaminate grazing land. Sewage sludge is a possible source, although there are strict codes of practice governing its use and the subsequent grazing of treated land, and most of the salmonellae die from desiccation within a week of being spread onto the pasture, especially in the summer. Some may persist for a considerable time, however, particularly those protected in the moist environment of a dung pat. Although survival periods of up to six months have been recorded for both S. dublin and S. newport, it is doubtful whether there would then be a sufficiently large dose to lead to disease, since experiments feeding 100,000 S. dublin bacteria daily to healthy cattle failed to produce any symptoms. It does indicate a further possible source, however, and pasture contamination may be important in producing carrier animals which can develop disease following stress at a later date. This is particularly the case for S. typhimurium DT104. During periods of flooding, salmonellae may be deposited directly onto pasture and be ingested by grazing animals. The importance of hygiene and disposal of faeces during an outbreak of disease cannot be overstressed.
Many wild animals have been shown to be carriers of salmonella and they can contaminate animal feed. Salmonella-infected rats, mice or birds can contaminate stored feedingstuffs and it would be impossible to tell if infection came in with the original imported fishmeal or whether it was due to subsequent contamination either on the farm or at the mill. Clearly vermin control is important in this context.
Dogs or foxes may also be involved. They could drag an aborted foetus or its placenta from an adjacent field, or they may simply carry infection on their feet. This is why the placenta and foetus should always be carefully disposed of by burning or burying. One of the major problems in trying to identify the source of salmonella during an outbreak is that exposure to infection may have occurred some considerable time in the past. It is only under subsequent stress that disease then develops, and by that stage the original source of infection may have long since gone.
Salmonellosis in man
With the increase in incidence in animals, there has been a corresponding rise in human infections of S. typhimurium and the exotics; human infection with S. dublin is very rare. Symptoms of salmonellosis are seen as food poisoning, with fever, severe abdominal pain, vomiting and diarrhoea. The elderly and very young children are particularly susceptible and deaths may occur. As with cattle, symptomless human carriers can develop and these people could be a risk to livestock, either directly or through inadequate sewage treatment.
The reverse, that is the spread of salmonella from animals to man, occurs most commonly through improperly cooked meat, improperly stored food or through drinking unpasteurised milk. For example, in Scotland, where consumption of unpasteurised milk was once common, there were 21 outbreaks with 1146 confirmed human cases (including 8 deaths) for the three year period 1980-82 inclusive. In 1983, legislation was introduced to enforce pasteurisation of all milk prior to sale and in the next three year period, 1983-85 inclusive, this reduced the human incidence of salmonellosis in Scotland to 15 outbreaks, but involving only 101 persons, all of whom were directly related to the farming community. It is expected that similar legislation will eventually follow in England.
The incidence of human cases from milk is relatively low, however. The dramatic increase of almost 300% in human S. enteriditis infection from 1987 to 1990 is well documented, and was of course associated with eggs and poultry meat. In the 1990s S. typhimurium DT104 became increasingly important and in 1994 there were 2500 human cases. As this organism has such a widespread distribution on infected farms, infection of farm personnel is almost impossible to avoid. However, clinical signs of disease are only likely to be seen in children and the elderly. Basic hygiene procedures are necessary to minimise the risks.
More on the topic Notifiable Diseases:
- Chapter 11 NOTIFIABLE DISEASES, SALMONELLOSIS AND ZOONOSES
- The various cardiovascular diseases observed in HIV-infected patients and widely described in the literature have been predominantly coronary and peripheral arterial diseases (PAD) and remain poorly known.
- BIBLIOGRAPHY FOR NONINFECTIOUS DISEASES
- other Orbiviral diseases
- INTERSTITIAL LUNG DISEASES
- THE CLOSTRIDIAL DISEASES
- WHY STUDY WILDLIFE DISEASES
- VECTOR-BORNE VIRAL DISEASES
- OTHER CLOSTRIDIAL DISEASES IN WILDLIFE
- BIBLIOGRAPHY FOR PARASITIC DISEASES