ECONOMIC DETERMINATION OF HEALTH INEQUALITY
17.4.1 Overview
If, as one would expect, health is a normal good, then the financially better-off will demand more of it. Whether this inflated demand is realized will depend on how health-enhancing and health-depleting goods are allocated.
If medical care is delivered through the market, then the rich will be both willing and able to afford more effective treatment when illness strikes. But few countries, particularly high-income ones, leave the distribution of health care entirely to the market. Public provision of care to the poor and elderly, or even universal provision of care to the entire population, should constrain health differences that arise from variation in the individual’s willingness and ability to pay for medicine. But other goods that are beneficial to health, such as quality housing, safe neighborhoods, and education, are at least partially allocated by the market and provide an opportunity for income to “buy” health. The direction of the relationship is not, however, unambiguous. Whether inequality in health reflects economic inequality will depend on the extent to which the greater demand of richer individuals for health is offset by their higher demand for the pleasures of alcohol, smoking, and rich foods that higher income makes affordable.Whether the better-off should be expected to be in better health will also depend on the source of their economic advantage. If it arises from higher earnings potential, then the health effect is ambiguous. This insight emerges from Grossman’s (1972a) healthcapital model according to which health is demanded for a direct utility benefit—feeling sick is uncomfortable—and a production benefit—less time is lost to sickness and so more is available for work. Health is produced by investment in medical care, exercise, healthy eating, and so on. In the pure investment version of the model, which incorporates the production benefit only, a wage increase has two conflicting effects on health.
A higher wage implies a higher value for a given increase in productive time, which would lead higher-waged individuals to invest more in health. But the marginal cost of the time input into health investment also increases. More earnings are lost visiting the doctor, jogging, and so on. The net effect is positive, provided that market goods, such as medical care and nutritious food, are used in the production of health in addition to the individual’s own time input (Grossman, 2000). But in the pure consumption version of the model, which confines attention to the direct utility benefit of health, the fact that the time cost of producing health is less than the total cost is not sufficient to create a positive substitution effect from a wage increase. The relative intensity with which time is used in the production of health must be less than the relative time input into the production of other commodities that generate utility. Otherwise, a wage increase implies a rise in the relative price of health. Maintaining one’s health is likely to be more timeintensive than many other activities that generate sources of utility, and thus, a negative pure wage effect certainly cannot be ruled out.Empirically determining the extent to which economic advantage bestows health advantage is complicated greatly by the multitude of mechanisms, identified in the previous section, through which health impacts economic circumstances, as well as the plethora of unobservables, such as risk attitudes, time preferences, and genetics, that can influence investments in health and other human and financial capital. Fixed effects methods deal with the latter problem but are powerless against the former simultaneity problem, and early attempts to tackle both problems tended to rely on instruments of questionable validity.[90] Since the beginning of the twenty-first century, researchers have increasingly studied changes in the health response due to more plausibly exogenous sources of variation in income or wealth, such as sudden policy reforms, stock market volatility, or windfall gains.
The weakness of this strategy is that it employs a form ofeco- nomic variation that, while exogenous, does not correspond to the variation that can plausibly impact health. The problem is exacerbated by the fact that health does not respond immediately to a change in demand. Even if a windfall gain from a stock marketboom, inheritance, or lottery win does induce a rise in an individual’s desired level of health, achieving this improved health will take years of investment in preventive medical care, diet, and so on. Even long panels may be insufficient to observe this process. There is a greater chance of identifying the income effect on health determinants than on health itself.
Many chronic health problems are also unlikely to be provoked by sudden changes in income or wealth, but they may, in part, result from long-term exposure to unhealthy living conditions experienced by the poor. The time lag in such an effect, along with the obvious endogeneity issues, make its identification challenging. Most of the existing evidence does not relate to such long-term relationships, and this lack of applicable data must be kept in mind when interpreting the evidence from shorter-term variation that tends to show no, or a weak, effect of income or wealth on health, at least in higher-income countries.
In this section, we begin our review of the evidence by examining the impact of income and wealth on health in adulthood. Most of this evidence comes from high- income countries. We then turn to mechanisms and look at the evidence that economic resources impact health behavior and utilization of medical care. The penultimate subsection examines the evidence for an impact of household economic circumstances on child health. Much of this evidence has been collected from low- and middle-income countries, or it refers to low-income populations in high-income countries.[91]
17.4.2 Income and Wealth Effects on Adult Health
17.4.2.1 CausalityTests
Perhaps the most influential examination of the economic determinants of health conducted since the turn of the century is the study by Adams et al.
(2003). Adams and colleagues recognize the difficulty of finding plausibly exogenous instruments for economic ircumstances that provide variation relevant to mechanisms of causation. So, they concentrate on the less demanding task of testing for the absence of causal income and wealth effects (and other dimensions of SES) on health among elderly (70+) Americans (see Table 17.5 for details of this study and other evidence relating to the USA). Their focus on an elderly sample neatly sidesteps the reverse causality from health to earnings that would likely occur in a sample of working-age individuals, and this complication is further avoided by adopting the concept of Granger (1969) causality and testing whether, conditional on lagged health, current health is uncorrelated with lagged income (wealth). This involves imposition of an assumption that there is no contemporaneous impact of income (or wealth) on health. The authors argue this plausible and strive to weaken itTable 17.5 US evidence of income and wealth effects on adult health and health behavior
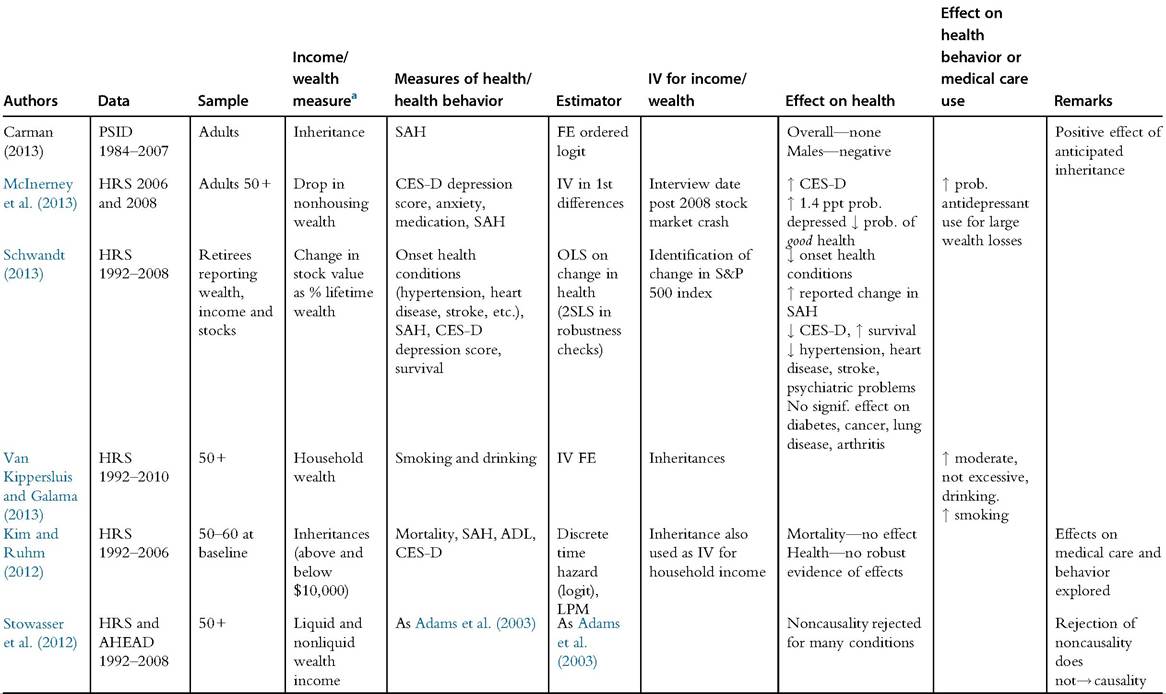
Table 17.5 US evidence of income and wealth effects on adult health and health behavior—cont'd
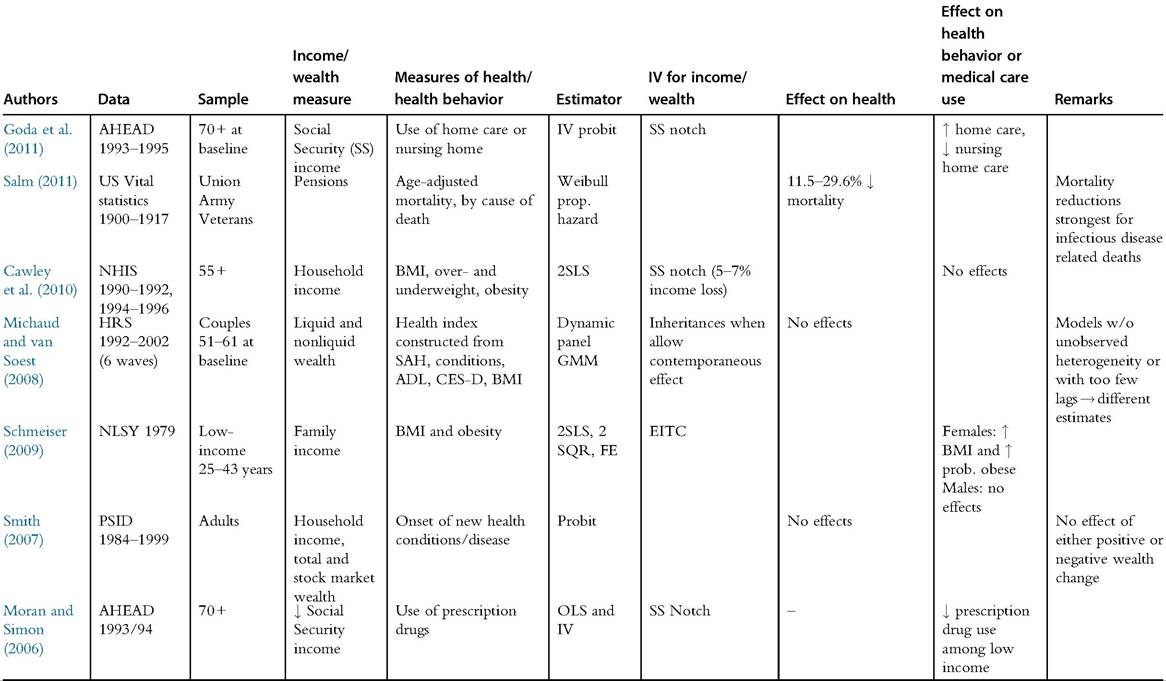
Table 17.5 US evidence of income and wealth effects on adult health and health behavior—cont'd
Note: See Appendix for explanation of dataset, variable, and estimator acronyms. aEffect on health/health behavior is with respect to health measure defined in this column.
further by conditioning on a battery of health conditions that are presumed, in a medical sense, to be precursors of the illness that income (wealth) is hypothesized to affect.
In this study, the null stating that lagged income (wealth) does not predict health is not rejected for most conditions, including acute, sudden-onset conditions and mortality.
The authors interpret this result as consistent with the absence of a causal effect of income and wealth on most health outcomes.[92] The hypothesis of no causal effect of wealth is rejected for the incidence of mental health problems, and the results for chronic and degenerative diseases are mixed. The authors argue that, because the treatment of mental and chronic illnesses are often not (fully) covered by Medicare, the ability of the individual to pay for such care may be a causal factor in the determination of these conditions.[93]Stowasser et al. (2012) revisit the analysis by applying the same Granger causality tests to the original data source extended to a longer observation period, younger cohorts at a given age and younger ages (50+ rather than 70+). The last extension generates some variation in health insurance status that was not present in the older, Medicare-eligible sample included in the original study. With these changes, the null that health is conditionally independent of lagged income and wealth is rejected for a much larger number of conditions, leaving only a minority of conditions for which it is not rejected. This result is problematic for the approach because rejection ofthe null can arise either due to a true causal effect or a common correlation with omitted unobservables. So, while the original study tends toward the conclusion of no causal effect of income or wealth on health, analysis of more data leaves one in the unfortunate situation of being unable to make any conclusions about the existence of the causal effect.
17.4.2.2 Causal Effects
Panel data methods can be used to deal with time-invariant unobservable determinants of health and income that cloud the conclusions that can be drawn from Granger causality analysis, although this is not straightforward because it uses the nonlinear estimators appropriate for modeling categorical health measures when dynamics and long-term relationships are taken into account.
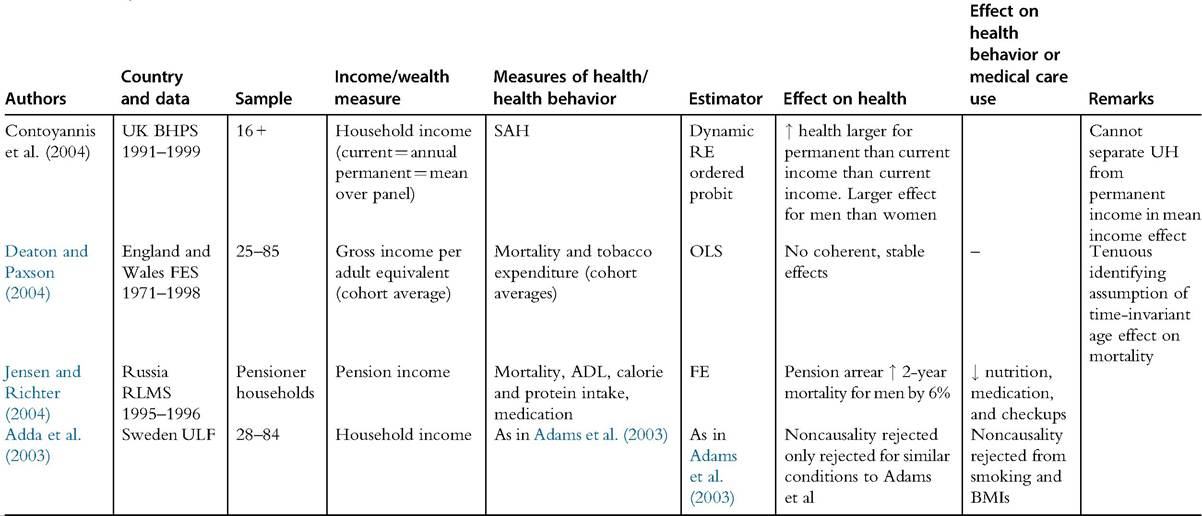
Estimating a dynamic random effects model of SAH with British data, Contoyannis et al. (2004) find that health varies with income averaged over time but not with current income (see Table 17.6 for all studies providing evidence from Europe). This result might be interpreted as indicating that health responds to changes in permanent income but not to transitory income shocks. As such, it is consistent with the above-mentioned argument that sudden income surprises observed over aTable 17.6 European evidence of income and wealth effects on adult health and health behavior
Continued
Table 17.6 European evidence of income and wealth effects on adult health and health behavior—cont'd
Note: See Appendix for explanation of dataset, variable, and estimator acronyms. aEffect on health/health behavior is with respect to health measure defined in this column.
short period may not provide variation in economic circumstances relevant to the determination of health. Sustained differences in income that influence long-term behavior seem more relevant to the evolution of health. However, caution is called for because it is not possible to separate the effect of individual income averaged over a panel from that of time-invariant correlated unobservables.
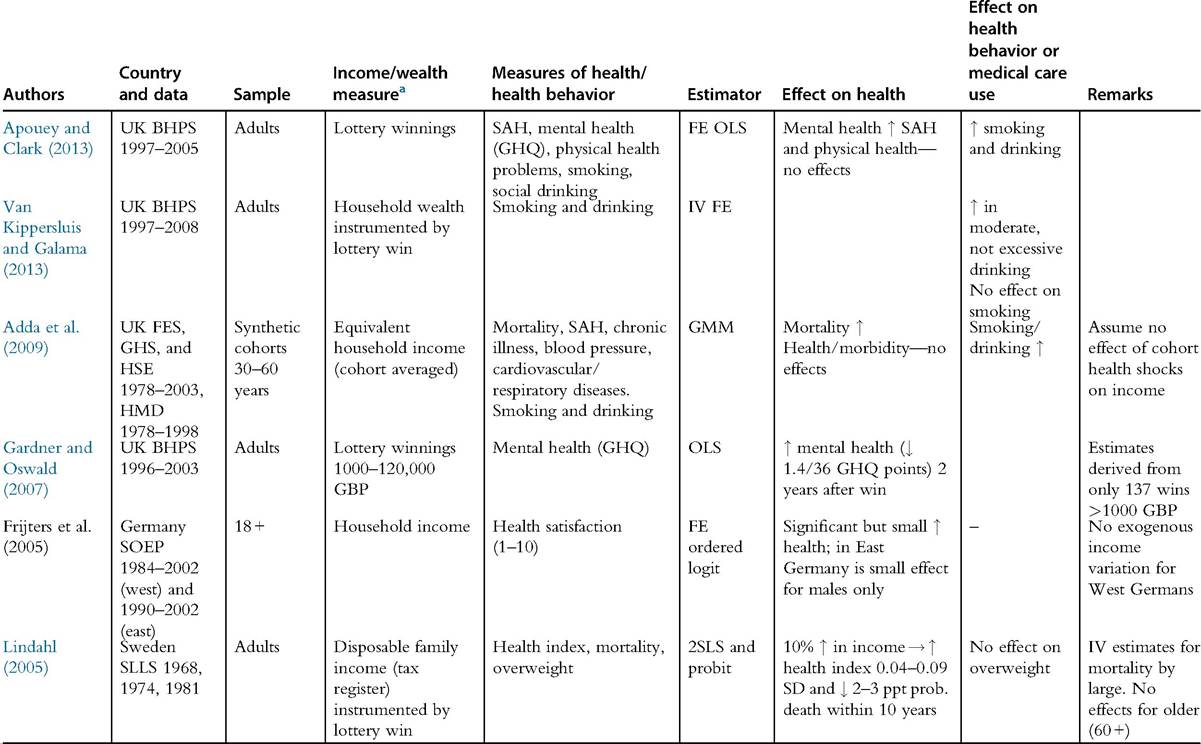
Frijters et al. (2005) exploit the largely exogenous income variation generated by the reunification of Germany in 1990 that resulted in sudden large income gains for nearly all residents of the former East Germany. Reverse causality cannot be eliminated because the East German component of the panel only started in 1990, and so reunification cannot be used as an instrument. Fixed effects models of reported health satisfaction reveal positive effects of income on health in the West, but, surprisingly, in the East where the income variation was much greater, these effects are only observed for males. However, all estimated effects are very small. Taking into account that the estimates are potentially upwardly biased by the failure to eliminate reverse causality, this study suggests that income does not have a substantial causal impact on health (satisfaction) in Germany.
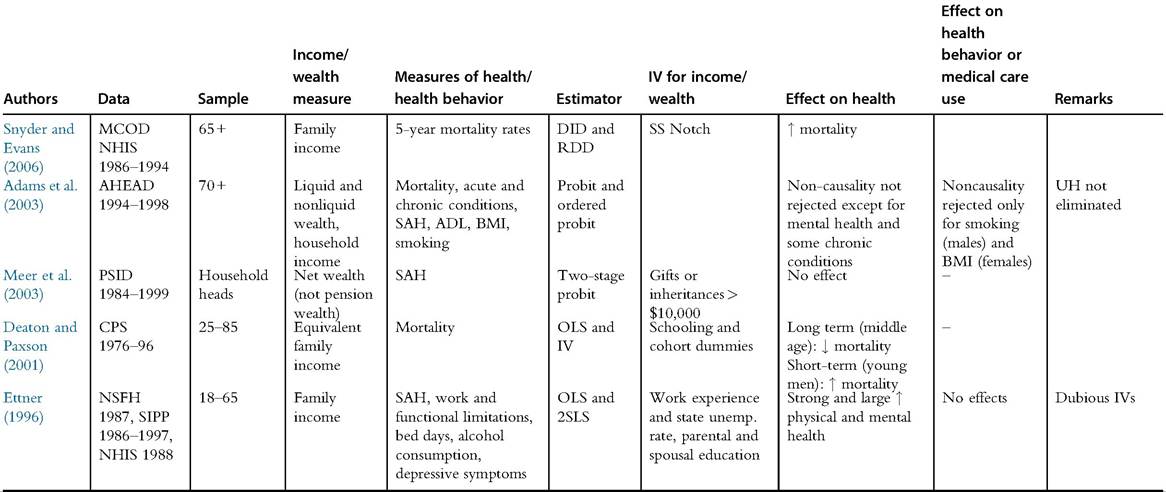
Using data aggregated at the level of birth cohorts, Deaton and Paxson (2001) find strong negative effects of income on all-cause US mortality in the period 1976—1996. The effects appear strongest in middle age and in young men. But these findings are not uncontroversial. It is difficult to rule out reverse causality in cohort models, and the authors’ use of education as an instrument for income is easily criticized. Moreover, the same authors do not find any coherent or stable effects of cohort income on cohort mortality in England and Wales (1971-1998) (DeatonandPaxson, 2004). Theyconclude that the observed correlated cohort income growth and mortality decline in both countries does not necessarily reflect a causal effect of the former on the latter, but it more plausibly arises from technological advances and the emergence of new diseases, such as AIDS, that affect age groups differentially. In this case, the main identifying assumption of the cohort approach—that age effects on mortality are constant through time—is invalid. This rather negative conclusion has not kept others from adopting a similar approach. Adda et al. (2009) study the health effect of permanent income innovations arising from structural changes in the UK economy in the 1980s and 1990s that are assumed to be exogenous. They find that cohort incomes have little effect on a wide range of health outcomes, but they do lead to increases in mortality: a 1% increase in income is estimated to lead to 0.7-1 more deaths per 100,000 persons among the prime-aged (30-60) population in any given year. This result is in sharp contrast to Deaton and Paxson’s finding of no mortality effect for the UK, and a negative effect of income on mortality for the USA. The authors claim their finding is consistent with substantial evidence that population health is countercyclical (Ruhm, 2000, 2003), although they are identifying the health effect of permanent income shocks, not transitory changes.
The countercyclicality of health is consistent with accumulating evidence from the USA of deterioration in individual health coinciding with the receipt of income. Evans and Moore (2011) find that mortality increases immediately following the arrival of monthly Social Security payments, regular wage payments for military personnel, tax rebates, and dividend payments. The increase in mortality is large and occurs for many causes of death connected to short-term behavior—like heart attacks and traffic accidents—but not for cancer deaths, which suggests that the effects derive from increased risky behavior. For example, the daily mortality of seniors is half a percentage point higher in the week after Social Security pay checks arrive compared to the week before. Mortality in younger populations is even more responsive to income receipt. Dobkin and Puller (2007) find elevated drug-related hospital admissions (23%) and within-hospital mortality (22%) in California in the first few days of the month for recipients on federal DI programs paid on the first of the month.
Health deterioration in response to payment of a given level of income is not necessarily inconsistent with health improvement arising from a permanently higher level of income. Higher income may afford both a smoother consumption profile and a lifestyle that is freer of health-threatening binging on alcohol or drugs. Although the evidence on the health response to the receipt of income rightly makes one wary of the health consequences of increased intermittent cash payments to certain groups, it tells us nothing about how the level of income impacts health.
Identification ofthe health effect of windfalls arising from prizes, lottery wins, investment returns, or inheritances is attractive because the gains are unanticipated and so are more plausibly exogenous to the evolution of health. Smith (2007) exploits large wealth gains accumulated by US stockholders during the stock market run-ups of the late 1980s and 1990s to estimate effects on the onset of major and minor chronic conditions, while conditioning on baseline health, income, and wealth. He does not deal with unobserved heterogeneity and so uses the language of prediction, not causation. Wealth changes (positive or negative) do not predict health changes.
Using the same PSID data but instrumenting wealth by inheritances, Meer et al. (2003) also find no significant effect on health. The same negative result emerges from three studies that test for a response of health to inheritance-induced changes in wealth using data on older (50+) individuals from the HRS (Carman, 2013; Kim and Ruhm, 2012; Michaud and van Soest, 2008). Allowing for a rich lag structure and unobserved heterogeneity, Michaud and van Soest (2008), as was noted in Section 17.3.7, find a significant effect of health on wealth, but they find no evidence of a causal effect of (contemporaneous or lagged) wealth on either SAH or chronic conditions.[94] Carman (2013) finds that health is only correlated with inheritances that are anticipated, the exogeneity of which may be doubted.
In stark contrast, Schwandt (2013) provides evidence of a positive wealth effect on health among relatively well-off retirees observed in the US HRS. In this admirably careful and detailed study, the author constructs a claimed exogenous measure of wealth shocks from the rate of change in the S&P 500 stock market index over a 2-year period applied to the household’s share of lifetime wealth held in stocks. The use of this measure presumes that it is the proportionate, and not the absolute, change in wealth that potentially impacts health. Thus, a psychophysiological response to a relative change in wealth, perhaps operating through stress, will generate more health variation in relatively wealthy, stock-holding retirees with health insurance than will a change in absolute wealth, given that the absolute change in wealth is not large enough to influence their ability to purchase health-preserving goods, such as medical care. Schwandt (2013) estimates that a shock (positive or negative) corresponding to 5% of lifetime wealth, which is within the range observed in the data, is positively associated with a change of 1-2% of a standard deviation in a variety of health measures, including onset of new health conditions, reported change in self-assessed health, mental health, and, for negative wealth shocks, even survival. Consistent with the hypothesis of a mechanism operating through stress, the study shows a significant impact on hypertension and, to a lesser extent, heart disease, stroke, and psychiatric problems, but no significant effect on conditions that are likely to evolve more gradually, such as diabetes, arthritis, cancer, and lung disease, although this may also be attributable to the lower incidence of some of the latter conditions. A further clue to a possible mechanism is provided by comparing the estimated health effects of a wealth shock with the cross-sectional correlation of health and wealth. For aggregate health conditions, mental health, hypertension, and heart disease, the magnitude of the estimated effect is greater than the respective correlation. For chronic conditions that take longer to develop, the opposite is true. This is consistent with an abrupt change in wealth of the otherwise well-off triggering a health change that is quite different in nature and aetiology from the health differences by wealth observed in that population.
41
Zooming in on the October 2008 stock market crash, McInerney et al. (2013) present further evidence from the HRS on the impact of large wealth losses on mental health.[95] The crash reduced wealth and increased depressive symptoms, as well as the use of antidepressants. The effects are nontrivial: for instance, a loss of $50,000 in the value of nonhousing wealth is estimated to increase the likelihood of feeling depressed by 1.4% points (8% in relative terms). Although one may expect some recovery from these immediate and substantial declines in mental health as result of adaptation, the evidence from Schwandt (2013) would suggest that the mental stress may provoke the onset of risk factors for physical illness.
The main threat to identifying the short-term health effect of a wealth shock arising from share prices is the possibility that health risks differ systematically with the fraction of wealth held in stocks. Schwandt (2013) provides some analysis that suggests this is not driving his results. However, a dynamic model of joint decisions over financial and health investments, which has a good fit with the relationships observed in PSID data, does predict that individuals facing greater health risks will diversify by holding less risky financial investments (Hugonnier et al., 2013). This model also predicts that investments in health rise steeply with wealth. While resting on strong behavioral assumptions, it provides insight into the joint evolution of health and wealth and could potentially be useful for pinpointing strategies for convincingly identifying the wealth effect on health.
A few European studies find evidence of positive health effects resulting from lottery wins. Using a Swedish panel and instrumenting a measure of permanent income (average income over 15 years) with average lottery winnings, Lindahl (2005) estimates that an income increase of 10% generates a fall in morbidity and a rather spectacular 2-3% point decrease in the probability of dying within 5-10 years. One may be sceptical of the credibility of such a large effect, which exceeds even the raw correlation between income and mortality. Using British data, Gardner and Oswald (2007) find that 2 years after a win of between £1000 and £120,000, the GHQ index of mental health increased by 1.4 points, on a scale of 36 points. The effect is only significant for males and, surprisingly, for higher-income individuals. Using a few more waves ofthe same data, Apouey and Clark (2013) find that lottery winnings have no significant effect on SAH, but a large positive effect on mental health.
Although the exogeneity of windfalls is certainly valuable, one may question the relevance of the resulting evidence to an understanding of the large differences in morbidity and mortality between the rich and the poor that are likely to arise from sustained differences in health behavior, and perhaps access to medical care, over many years. Economic shocks observed in data with a limited longitudinal span are potentially useful in identifying short-term health responses, but they can tell us little or nothing about the mechanisms responsible for the gradient in health conditions that emerge over the life cycle.
Pension policies have provided a final source of income variation from which researchers have attempted to identify effects on health. Jensen and Richter (2004) study the effect of losses in pension income in Russia during a major crisis period (1995-1996) (Table 17.6). Delayed pension payments had a dramatic impact on living standards, with income declining by up to 24% and poverty rates tripling to over 50%. For males, the loss of pension income increased the likelihood of death within 2 years by 5.8% points, and raised functional impairment (ADL) and the probability of experiencing chest pain. These effects are likely to have materialized from substantial and significant reductions in both calorie and protein intake, as well as reduced use of medication for chronic conditions and preventive checkups. There were no effects on women’s health or mortality.
Back in the USA, Snyder and Evans (2006) report evidence suggesting that reduced pension income raises health (Table 17.5). They exploit a notch in Social Security payments that resulted in those born after January 1,1917, receiving sharply lower retirement incomes than contemporaries with identical earnings histories born slightly earlier. There was little time to adjust to the income loss because the legislative changes happened late in their working lives. In any case, most of those affected did not realize the impact of the changes until after retirement. The authors find that the decrease in pensions reduced mortality and rationalize this surprising result by a claimed positive health effect of increased postretirement (part-time) work effort in response to the income loss.
The contradictory evidence from the USA and Russia is most plausibly attributable to differences in how the level of income around pensions fluctuated. There is evidence of large mortality reductions (particularly for the poor) resulting from increases in pensions paid to US Union Army veterans at the beginning of the twentieth century (Salm, 2011), when both incomes and health were obviously much lower than in the period studied by Snyder and Evans.
17.4.3 Income and Wealth Effects on Health Behavior
The evidence reviewed in the previous section does not support a strong, or even any, causal effect of income, or wealth, on health. But this may simply reflect the difficulty of observing, even in moderately long panels, the health consequences of changes in health behavior and utilization of medical care that may only materialize in the long term. In this and the following section, we assume that there are health effects of smoking, drinking, forgoing effective health care, and so on, and we examine whether there is evidence that economic circumstances impact on these health determinants.
Particularly in the USA, more affluent individuals are generally less likely to smoke, drink heavily, be overweight, or use illegal drugs, and they are more likely to exercise and engage in preventive care (Cutler and Lleras-Muney, 2010; Cutler et al., 2011a,b). But simple correlations obviously tell us nothing about the presence or direction of causality. Some of the evidence reviewed by Cawley and Ruhm (2011) shows that income and/or wealth increases consumption of tobacco and alcohol. This holds for the response to income shocks in the UK captured by cohort income (Adda et al., 2009) and lottery winnings (Apouey and Clark, 2013) (see Table 17.6). In the USA, Kim and Ruhm (2012) find that wealth gains from inheritances only raise moderate drinking and have no effect on smoking (Table 17.5).
The evidence for income and wealth effects on obesity is mixed but certainly does not support a strong causal effect in either direction. Kim and Ruhm (2012) find some indication of wealth gains reducing the likelihood of being overweight, which is consistent with Swedish evidence based on lottery winnings (Lindahl, 2005). Cawley et al. (2010) use US National Health Interview survey data and the Social Security notch as an IV for income and find no impact of income on weight or obesity. Exploiting variation across US states in the generosity of the Earned Income Tax Credit (EITC), Schmeiser (2009) finds no effect of income on weight for men and a positive effect for women: an additional $1000 per year is associated with a gain of no more than 1.80 pounds (0.82 kg).
Galama and van Kippersluis (2010) extend Grossman’s (1972a,b) health-capital model with the aim of understanding how health behavior may differ by wealth. They distinguish between healthy consumption, which reduces the rate of depreciation of health (e.g., good housing, vitamins, muesli) and unhealthy consumption, which increases health depreciation (e.g., cigarettes, excessive alcohol, etc.). Wealth has a positive effect on healthy consumption both because of a pure wealth effect and because higher wealth raises health investment, which is assumed to exhibit diminishing returns, so that depreciated health is more expensive to replace through medical care.[96] The effect on unhealthy consumption is ambiguous because the wealth and price effects go in opposite directions. The wealthy are less inclined to run down their health because of the higher marginal cost of replacement. The model predicts that, under arguably plausible assumptions, the wealthy will be more likely to engage in moderately unhealthy consumption (wealth effect dominates) and less likely to partake in severely unhealthy consumption (price effect dominates).
Van Kippersluis and Galama (2013) test these predictions with wealth gains instrumented by lottery winnings in British (BHPS) data (Table 17.6), as in Apouey and Clark (2013), and by inheritances in US (HRS) data (Table 17.5), as in Kim and Ruhm (2012). Unlike the earlier studies, they use fixed effects models to deal with unobserved heterogeneity and find robust evidence that wealth increases the probability of drinking alcohol, but it has no effect on the number of drinks and heavy drinking. This is consistent with the direct wealth effect dominating for behavior that is moderately unhealthy, although indulgence in a glass of good claret over dinner may actually be beneficial to one’s health. Their results for smoking are inconclusive: a lottery win in the UK does not increase smoking, which is inconsistent with Apouey and Clark (2013), but inheritance receipt in the USA does immediately increase both the prevalence and intensity of smoking, which is inconsistent with Kim and Ruhm (2012), who look at longer term effects, and also with the prediction of the theory.
Income opens consumption opportunities. For unhealthy consumption to explain income-related health inequality, tobacco, alcohol, fatty foods, and so on would have to be grossly inferior goods. There is no evidence of this. This is not to say that health behavior is not an important contributor to the social, as opposed to economic, gradient in health. On the contrary, health behavior can account for a large proportion ofthe differences in health across education groups (Cutler and Lleras-Muney, 2010; Cutler et al., 2011a,b). But it is likely to be the preferences and knowledge of higher education groups, and not their wealth, that lead them to adopt healthier lifestyles.
17.4.4 Income Effects on Medical Care
As pointed out earlier, the potential for medical care to contribute to health differences by income is constrained in many high-income countries by the dominance of public health insurance. The income gradient in utilization of medical care should be stronger in countries, such as the USA, that give the market greater more influence on the financing of the health system. But public health care seldom completely crowds out private care, and even within the European social health insurance and national health service systems, specialist care is often distributed in favor of the better-off (Van Doorslaer et al., 2000, 2004, 2006). But while the income elasticity of demand for medical care has been the subject of numerous studies, the literature provides surprisingly little evidence of a causal effect of income on utilization.4
The Kim and Ruhm (2012) study using the US HRS finds that wealth gains from inheritances raise utilization of many types of medical services and out-of-pocket spending. Using a sample of the old (70 +) US population whose drug expenses were not covered by Medicare at the time, Moran and Simon (2006) find a large and statistically significant effect of income instrumented by the Social Security notch on prescription drug utilization, though only for households that have low education and do not have high income (< 75th percentile) (Table 17.5). Their estimates of income elasticity are all above 1. Goda et al. (2011) extend the analysis to estimating the impact of income on utilization of long-term care, which is also not fully covered by Medicare, and they find that a positive permanent income shock lowers nursing home use but increases the utilization of paid home care services. It is important to bear in mind that the estimated positive income effects on both drug and long-term care utilization pertain only to the elderly who had been low-wage workers, because the Social Security notch had only a weak impact on the pensions of older cohorts who had been higher earners.
These three studies of the older US population confirm what one would expect. Medical care is a normal good. Where universal public health insurance coverage is absent, individuals who can afford more and better health care will purchase it.
44 Virtually every textbook in health economics devotes a chapter to the demand for medical care, including estimates of income elasticity (e.g., Sloan and Hsieh, 2012). We do not cover the literature on the effect of income on the demand for health insurance, which would take us some distance from the income-health nexus. It is well-known that uptake of insurance is very much income-related.
17.4.5 Income Effects on Child Health
In Section 17.3.4, we conclude that early-life health conditions have an economically significant effect on economic well-being in adulthood. Currie (2009) proposes that child health is a potentially important contributor to the intergenerational transmission of education and economic status. The idea is that less educated, poor parents are more likely to give birth to and rear less healthy children. Childhood ill-health interferes with humancapital acquisition and directly constrains health capital in adulthood, which further reduces earnings potential. A cycle of poverty is propelled by childhood ill-health. Poverty begets childhood illness, which generates poverty later in life. If true, this would give health a role not only in the creation of inequality, through health shocks that increase income dispersion, but in its perpetuation across generations. Whether parental income does constrain child health is therefore an important question to be addressed not only from a health perspective but also from that of economic inequality.
We focus here on the evidence that parental economic circumstances constrain child health and skip consideration of the mechanisms through which an effect may arise. Almond and Currie (2012) use Cunha and Heckman’s (2007) model of investment in cognitive and noncognitive skills of children to provide a framework for thinking about the evolution of children’s human capital, including health. Further development of this model to formally incorporate health may provide insight into the impact of parental income on child health.
From a review of the evidence, Currie (2009) concludes that, while there is little doubt that children from less privileged backgrounds are less healthy, there is insufficient evidence to conclude that, in a high-income country context, this arises from a causal effect. Identification of a causal effect of parental income on child health should, nonetheless, be easier than the identification of the (own) income effect on adult health. The reason is that reverse causality is less of an issue because children generally do not earn income, at least in high- income countries. This has been one of the main motivations for researchers to examine the impact of parental income on child health. Of course, reverse causality is not entirely eliminated, because the illness of a child may interfere with his or her parents’ work activity, and correlated unobservables remain a substantial problem.
17.4.5.1 Evidence from High-Income Countries
The correlation between family income and children’s general health strengthens as children grow older in the USA (Case et al., 2002) and Canada (Currie and Stabile, 2003), suggesting that the disadvantages associated with parental income accumulate as children age. The steepening of the gradient with age can be due to poorer children being hit by more health shocks and/or having more difficulty recovering from illness, given constrained access to medical care. In the USA, the strengthening of the gradient is due to a combination of these effects (Case et al., 2002; Condliffe and Link, 2008), whereas in Canada, consistent with its universal health care system, it is only due to poor children becoming sick more frequently (Currie and Stabile, 2003).[97]
These findings are not generally confirmed for other countries. Khanam et al. (2009) find that there is a gradient in Australia that strengthens with age when similar covariates to those used by Case et al. (2002) are included. However, the gradient disappears when they include a richer set of controls, in particular maternal health, suggesting that there may be no causal effect. Reinhold andJiirges (2012) find that the parental income gradient in child health in Germany is as strong as it is in the USA, but it does not steepen as children grow older, which could be attributed to the constraining effect of universal health care.
The UK evidence is mixed, with Currie et al. (2007) and Case et al. (2008) arriving at different conclusions from analyses of the same survey. Currie et al. (2007) find a significant family income gradient in child general health that increases between ages 0—3 and 4—8 and decreases afterward. Case et al. (2008) add 3 years of data and find that the gradient keeps increasing until age 12. Analyses of a rich data set from one region of England reveal a gradient that does not increase between birth and age 7 and almost disappears with an expanded set of controls, including parental behaviors and health (Burgess et al., 2004; Propper et al., 2007) Using a nationally representative sample, Apouey and Geoffard (2013) find a gradient thatpersists up to the age of17 but no evidence that utilization ofhealth care, housing conditions, nutrition, or clothing are important mechanisms for generating it.
In North America and Europe, children from poorer households are less healthy. Whether this arises from an effect of parental income or some other characteristic of the family associated with both income and child health cannot be established from the studies cited above. Using reform-induced variation in the US Earned Income Tax Credit (EITC), Hoynes et al. (2012) estimate that increased maternal income reduces the incidence of low birth weight and increases mean birth weight. For single low-educated mothers, an increase of $1000 in the EITC generates a 6.7-10.8% reduction in the incidence of low birth weight (see Table 17.7 for this and other studies providing causal evidence in this and next subsection). The effect appears to be mediated through slightly greater use of prenatal care and much more substantial reductions in smoking and drinking during pregnancy.[98] These estimates suggest sizeable gains in infant health from income increases among low-income populations.[99] A much more
Table 17.7 Evidence of income effects on child health and related health behavior
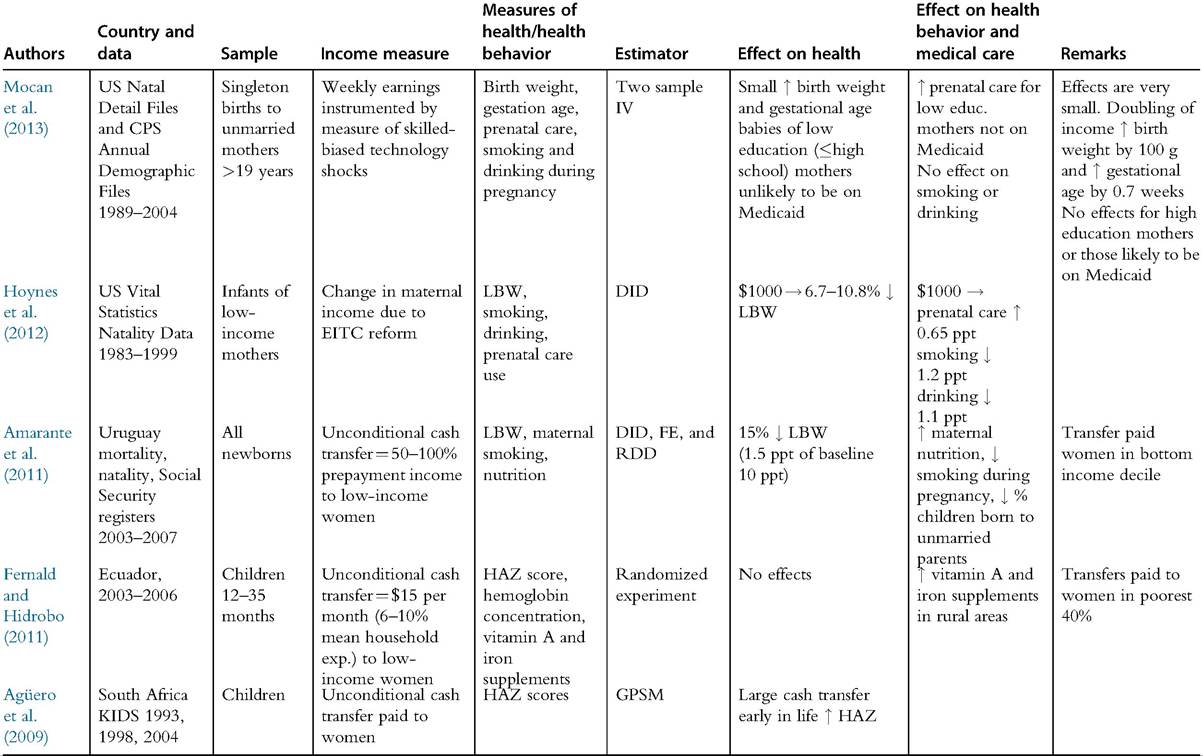
Table 17.7 Evidence of income effects on child health and related health behavior—cont'd
| Authors | Country and data | Sample | Income measure | Measures of health/health behavior | Estimator | Effect on health | Effect on health behavior and medical care | Remarks |
| Paxson | Rural | Children | as Fernald and | Hemoglobin | Randomized | Poorest quartile: ↑ | ↑ deworming | as Fernald and |
| and | Ecuador | 36-83 | Hidrobo (2011) | level, HAZ, | experiment | hemoglobin | treatments | Hidrobo (2011) |
| Schady | 2003-2006 | months | fine motor | Other quartiles: no | ||||
| (2010) | control, deworming | effects | ||||||
| treatment | ||||||||
| Case | South Africa | Children | Pension receipt | height | OLS | ↑ height of black and | ||
| (2004) | Langeberg Survey 1999 | colored kids | ||||||
| Duflo | South Africa | Children | Woman's receipt of | HAZ and | 2SLS | ↑ HAZ and WHZ of | No effect on boys. | |
| (2000, | SALDRU | 6-60 | pension | WHZ scores | (IV = pension | girls by 1.2 SD after 2 | No effect of | |
| 2003) | 1993 | months | eligibility) | years | pension paid to male on either girls or boys. |
Note: See Appendix for explanation of dataset, variable, and estimator acronyms.
modest effect is estimated from data on 14 million US births between 1989 and 2004 that uses a census division year-specific index of skill-biased technological change to instrument mothers’ earnings (Mocan et al., 2013). For low-educated (i.e., no more than high school diploma) unmarried mothers who are unlikely to be on Medicaid (public health insurance for low-income households), increased earnings raise utilization of prenatal care, as well as birth weight and gestational age. The fact that there are no significant effects on births to high-educated mothers and to all mothers who are likely to be covered by Medicaid suggests that low income constrains access to maternity care for those lacking insurance coverage. However, the effects are very small. A doubling of earnings would raise birth weight by only 100 grams and gestational age by only two-thirds of a week.
17.4.5.2 Evidence from Low- and Middle-Income Countries
One would expect health in general, and child health in particular, to be more contingent on income in low-income settings where the nutritional needs to sustain health are often not met and universal health insurance coverage is absent, with most medical care paid for out-of-pocket. Indeed, the economic gradient in health is particularly steep in low- and middle-income countries and is evident in critical indicators, such as infant mortality (Commission on the Social Determinants of Health, 2008). The evidence that the gradient in child health does derive, at least in part, from the causal impact of economic circumstances on health is much more clear-cut than that from high-income countries (see Table 17.7 for studies cited in this section).[100] [101] Duflo (2000, 2003) examines whether the extension of pensions to black South Africans in the early 1990s had an impact on the nutritional status of children. An effect may have been anticipated because more than a quarter of black children under five lived with a pension recipient by the end of the period studied. The analysis reveals that pensions paid to women have substantial positive effects on the weight and height of girls but no significant effects on the nutritional status of boys, and pensions paid to males have no effect.4 The effects are very large. Payment of a pension to a woman is estimated to raise both weight and height of girls by 1.2 standard deviations over a 2-year period (Duflo, 2003). The income gain was also large with pension benefits being around twice the median per capita income in the rural areas at the time. These results suggest that income can have very large positive effects on child health in low-income settings, but whether this effect materializes crucially depends on who receives the income.[102] Consistent with this, an unconditional cash grant paid to child caregivers (mostly women) in South Africa has been demonstrated to significantly boost child height (Agtiero et al., 2009). On the basis of the observed relationship between adult height and earnings, the projected discounted return to the grant is estimated to be as much as 50%. The evidence is mixed for income effects on child health in poor populations, as obtained from unconditional cash transfer programs in Latin America, however.[103] Ecuador’s Bono de Desarrollo Humano (BDH) pays $15 per month—equivalent to 6-10% of average household expenditure in the target group—to mothers of children below the age of 17 in the poorest two-fifths ofthe population, but this additional income has been found to have no significant impact on the health (height and hemoglobin concentrations) of children aged 1-3 years (Fernald and Hidrobo, 2011), and among older children aged 3-7 years, there are only modest effects (on hemoglobin and deworming treatments) for the poorest (Paxson and Schady, 2010).[104] Uruguay’s PANES program targets poorer households, restricting payment of the generous monthly cash transfer—equivalent to 50% of average preprogram income for recipient households and up to 100% of income for households with a recent birth—to households in the bottom decile. It is estimated to reduce the incidence of low birth weight by 1.5% points relative to a baseline of 10% (Amarante et al., 2011). This effect appears to materialize through improved maternal nutrition, reduced smoking during pregnancy, a large reduction in the proportion of children born to unmarried parents, and a modest reduction in maternal labor supply. The larger health impact relative to that of the general cash transfer in Ecuador is plausibly explained by the greater magnitude of the payment and its direction to (relatively) poorer households. 17.4.6 Conclusion In this section, we set out to determine the extent to which differences in economic circumstances contribute to health inequality across individuals. Do the poor experience worse health because they are poor? Answering this question is difficult because worse health would be expected to be associated with lower income even without being caused by it. This has driven researchers to search for phenomena that generate variation in income or wealth without being caused by or associated with health. In high-income countries, this research enterprise has tended to produce evidence indicative of no impact of income on health in adulthood, or effects that are small in comparison to the observed income-health gradient, suggesting that the association does not derive from financial resources impinging on health. An exception is US evidence of deterioration in health, particularly as reflected in indicators related to stress and mental status, in response to stock market losses. To an extent, the general finding of little or no effect is plausible. Variation in health arises from differences in the health stock with which we are endowed (genetics), the extent to which we look after this endowment (lifestyle and living conditions), the opportunities to repair it when it gets damaged (medical care), and luck. Financial resources cannot influence the first and last determinants. Most high-income countries offer universal health care coverage irrespective of ability to pay, which greatly weakens the economic impact on the third determinant. That leaves lifestyle and living conditions. Most research concentrates on the former, and, within this, on what we do that is bad for our health, rather than what we do that is good for it. It would be perverse if greater ability to afford indulgencies in unhealthy behavior, such as smoking and drinking, explained why the better-off are in better health. In fact, the rich tend to lead less unhealthy lives, but that is not because they are economically privileged. More likely, it has to do with their education advantage. The ability of money to buy health in the developed world is limited. Mental health appears to respond to economic circumstances, with losses producing larger deteriorations in mental well-being than gains generate improvements. But there is little evidence that physical health problems are provoked by worsened personal finances. However, we suspect that there is much that current research is missing. Identification of the effect of one stock variable (financial wealth) on another (health capital) is far from easy. There is a risk that identification strategies that focus on very local effects of windfall gains from lottery wins, inheritances, or tax/benefit reforms throw away effects that accumulate over the life cycle together with the bathwater containing the common unobservables. The determinant that is more permanent—living conditions—tends to get overlooked in research conducted by economists. This includes housing and features of the built and social environment that vary with the economic status of neighborhoods: pollution, leisure facilities, open spaces, food quality, and crime. Money can afford improved housing quality and relocation but it takes a very large economic shock to achieve this. Chronic poverty can entail damp walls, confined spaces, disruptive neighbors, polluted air, and a threat of violence that gradually, or perhaps suddenly, take a toll on health. The health experience of the chronically poor has no influence on the estimated impact of wealth on health in some research, such as that identifying variation in inheritances or stock prices. Other evidence, such as that based on lottery wins, does potentially capture exposure among the poor, but the sudden and often moderate gains in cash involved may not be sufficient to substantially change living conditions, and even if they are, the observation period is unlikely to be sufficiently long to detect impacts on chronic health problems that may only slowly respond to material circumstances. We are hesitant to conclude that lack of evidence of an impact of wealth on adult physical health in much of the developed world means that there is no effect. One can be more confident that the worse health of poorer children, which is unfortunately still observed in many high-income countries, is not simply a reflection of health constraining earnings. It may also arise from the fact that poorer parents are also less educated, and this lower level of education impacts child health. As would be anticipated, the strongest evidence that economic conditions determine inequalities in (child) health comes from the developing world. But even here more income does not necessarily bring better health. Money may be able to buy health when nutritional status is low and many cannot afford medical care, but the money must be given to those that value health highly. There is some evidence that women prioritize child health more than men. 17.5.
More on the topic ECONOMIC DETERMINATION OF HEALTH INEQUALITY:
- PRELIMINARIES: DIMENSIONS, INDICATORS, AND WEIGHTS
- Constitutional change
- The place and role of knowledge of life safety basics in the modern world
- Chapter 79 A New Macroeconomic Architecture for the Stock Market: A General-System and Cybernetic Approach
- Concluding remarks
- Freeing the Labor Market from its Distortions
- Intragenerational equity
- THE PRECAUTIONARY PRINCIPLE
- Introduction
- Bovine TB Control Strategies