HEALTH DETERMINATION OF ECONOMIC INEQUALITY
17.3.1 Overview
How might the distribution of health determine the distribution of income? The most obvious effect is through physical and mental capacity for work. We begin this section by considering how health may impact productivity and wages.
We then turn to the relationship between health and the quantity of work. Labor supply may be reduced at both the extensive margin, with illness in middle age tilting the balance in favor of early retirement, and the intensive margin, with part-time work becoming a more attractive proposition for some with a debilitating illness. In high-income countries, the employment effect on earnings will be directly cushioned by DI, but resultant moral hazard will indirectly contribute to the effect. Earnings losses may be exacerbated by discrimination, but legislation designed to prevent this may increase the impact on employment by constraining wage flexibility. Labor supply may be constrained by current sickness and influenced over the longer term by any downward revision of life expectancy following the onset of a major illness.In addition to the immediate impact of ill-health on earnings, there may be important lifetime effects operating through education, occupation, and marriage. Illness in childhood can constrain opportunities for education and its efficiency in producing knowledge and skills. With few education qualifications, a frail young adult will be limited in his or her choice of occupation. The less healthy may also be constrained in their choice of partners. If there is sorting, such that the least healthy marry others of less than average health or remain unmarried, then the contribution of health to inequality in household incomes will be even greater than its contribution to inequality in individual incomes. Ill-health may not only directly constrain the work effort of the disabled person, but it may also indirectly affect the labor supply of the spouse, who may face conflicting demands on his or her time to both replace lost earnings and provide informal care.
Health may impact the distribution of wealth, both directly and indirectly, through income and the accumulation of savings. Because the latter effect is cumulative, the contribution of health to inequality in wealth should be even greater than that to inequality in incomes. The healthy, expecting to live for longer, may save a larger fraction of their higher incomes, further increasing wealth disparities by health. When health insurance is incomplete and medical care must be paid for from an individual’s own resources, illness can directly deplete wealth.
In the subsequent subsections, we consider the potential effects of health on income through wages, work, human capital, occupation, and household formation or spousal earnings. In each case, we elucidate the potential mechanisms and evaluate the evidence relevant to establishing the extent to which health differences contribute to economic inequality.
17.3.2 HealthandWages
Individuals in poor health have substantially lower earnings than those in good health. Figure 17.3 shows mean gross earnings of employees in the bottom two categories of SAH as a percentage of the mean in the two top categories for China, the Netherlands, and the USA, as estimated from the data sources in Section 17.2. Although there are discrepancies at the youngest and oldest age groups, mainly due to the small sample of individuals working and in less than good health in the Netherlands at these ages, among those working between the ages of 30 and 60, the earnings of individuals in the worst health are 15—40% below those in the best health in the three countries. In the middle age range, the health gradient in earnings is largest in the Netherlands, which may reflect both qualification for partial DI, which acts as an earnings subsidy, and the high rate of part-time employment. The relative earnings of the least healthy individuals decline most rapidly with age in China, where lower pension coverage leaves many with little option but to continue working despite deteriorating earnings capacity.
17.3.2.1 Productivity
Deterioration in health will often decrease labor market productivity and earnings capacity. But the multidimensionality of health and variation in the capacities and skills required for different occupations are reasons to expect a great deal of heterogeneity in the response of wages to health problems. A mobility-impeding disability obviously constrains the productivity of a manual worker much more than it does that of an office worker. Technology, particularly that which enables remote work and reduces the need for commuting, is making the productivity of workers who draw more on their brains than their brawn even less contingent on physical functioning. But the productivity of such workers is dependent on retaining cognitive functioning and is potentially vulnerable to mental health problems. Thus, the estimated effects of health on wages, derived from measures of different dimensions of health for individuals with different demographic and occupation characteristics, should display substantial variability.
The relationship between productivity and physical health is likely to be strongest in developing countries where there is a preponderance of low-skilled manual work.[63] Identifying the economic returns from health investments has been the motivation for macro studies, revealing a strong positive correlation between economic growth and initial population health (Barro, 2003, 2013),[64] and micro studies of the relationship between wages and health across individuals in developing countries (Strauss and Thomas, 1998). Our focus is not on the impact of health on average income. Rather, we are interested in the extent to which the distribution of health affects the dispersion in incomes.
In low-income settings, the relationship between health and productivity can sustain, exacerbate, and, in theory, even generate inequality. The crux of the argument is that health constrains productivity, and wages provide the means, through nutrition, to sustain health.
A negative shock to either health or wages can generate a downward spiral into a nutrition-based poverty trap (Dasgupta, 1993, 1997). The theory of nutritionbased efficiency wages (Bliss and Stern, 1978; Dasgupta and Ray, 1986; Leibenstein, 1957; Mirlees, 1975; Stiglitz, 1976) generates the prediction of increased inequality as a result of the interdependence of nutritional status and productivity. As nutrition rises above the critical threshold of physiological sustenance, the marginal increases in productivity rise substantially, and diminishing returns eventually set in. This nonconvexity results in involuntary unemployment because the savings in labor costs from employing the poorly nourished unemployed at lower wages would be more than offset by the resulting loss in productivity. Individuals with initially fewer assets, who can invest less in health, are more likely to be involuntarily unemployed (Dasgupta and Ray, 1986). The poor are more likely to be malnourished and sick, and because they are sicker, they are more likely to be unemployed and so fall into destitution. Thus, inequality is exacerbated.The relevance of this theory has been challenged by the observation that one of its central assumptions—that poor households are constrained to spend almost all their resources on food—is inconsistent with the observed behavior of the poor (Banerjee and Duflo, 2011). Starvation is not perennially present even in very low-income countries (Strauss and Thomas, 1998). Ill-health may, however, be a source of a poverty trap and a contributor to inequality. For the income- and asset-poor with little formal or informal insurance options, the loss of productivity and earnings precipitated by illness results in reduced consumption opportunities and consequently nutritional deprivation, which further harms health and constrains productivity. The economic impact of illness is likely to be greatest on poor individuals because their livelihoods rest most on their health and because they have fewer assets that can be used to protect consumption and maintain nutritional status when illness strikes.
Even if health shocks were evenly distributed across the population, their differential effects would increase economic inequality.There is a vast body of evidence concerning the impact of health and nutrition on productivity and wages in low- and middle-income countries. The main motivation for this research is to evaluate the case for investment in health and nutrition programs as an instrument of development policy. Reviewing this literature would take us well beyond the scope of this chapter. In any case, a number of reviews already exist (Commission on Macroeconomics and Health, 2001; Deolalikar, 1988; Schultz, 2005, 2010; Strauss and Thomas, 1998; Thomas and Frenkenberg, 2002). Strauss and Thomas (1998) conclude that there is no robust, consistent evidence from nonexperimental studies that ill-health reduces productivity and wages, although it does reduce labor supply. In interpreting this conclusion, one needs to bear in mind that the wage response to ill- health can only be studied among employees. This misses the large informal sector of the economy in which the productivity of self-employed, mainly agricultural, workers could be expected to depend on health (Dasgupta, 1997). Evidence of an effect of nutrition, as opposed to health, is stronger. Strauss and Thomas (1998) are convinced that the positive impact of nutritional status (height and body size) on wages and micronutrients (particularly iron) clearly raises productivity. Calorie intake, when accurately measured, is found to have a positive effect on wages, at least among those initially malnourished.
17.3.2.2 Discrimination
Not all disabilities impede productivity; at least, not in all occupations. Nonetheless, equally productive disabled individuals may be paid less than their able-bodied counterparts because they are perceived to be less productive, or simply because of prejudice.
Discrimination against the disabled, as against other minority groups, comes in two varieties. What economists refer to as taste discrimination would be more commonly recognized as prejudice, and it arises from a preference of employers, or other employees, to keep disabled workers at a distance.
Since Becker (1957), this has been modeled as a marginal cost, on top of the wage, that a prejudiced employer incurs in employing a member of the minority group. Such an employer will only hire a disabled person at a wage below his or her marginal product. Whether this discriminatory behavior is sustainable in a competitive market depends on the prevalence of prejudice relative to the supply of disabled labor (Becker, 1957). Under competitive conditions, nonprejudiced firms can undercut their prejudiced rivals, and discrimination will be competed away (Cain, 1986), unless prejudice arises from customers (Kahn, 1991).This model was developed with the central purpose of explaining and understanding the consequences of discrimination against ethnic minorities. Although some disabilities, or rather handicaps, may still carry a social stigma, most are unlikely to make others, or at least a majority of others, uncomfortable. Stereotyping, or statistical discrimination (Aigner and Cain, 1977; Arrow, 1973;Phelps, 1972), seems a more probable source of bias against disabled individuals. In making appointments and wage offers, it is optimal for an employer to supplement information obtained from a noisy signal of productivity, such as a test score or qualifications, with knowledge of the average productivity of a group to which the applicant is observed to belong. Presuming disabled individuals are, on average, less productive, a disabled person would be offered a lower wage than a nondisabled applicant who performed no better with respect to the assessment criteria.
This theory does not help us explain earnings differentials between the disabled and nondisabled over and above those attributable to productivity differences. But it can explain part of the reason for the productivity deficit. If test scores or qualifications are a noisier signal of productivity for the disabled, perhaps because the tests are designed to discriminate between able-bodied applicants, then employers will put less weight on these criteria and more on the observed disability. Faced with a lower return, this group will invest less in human capital. Inequality will be greater than it would be if employers where blind to disability status, or legislation successfully forced them to act as if they were.
Besides its inability to explain earnings differentials beyond those attributable to productivity, the relevance of statistical discrimination as an explanation for health-related wage differences depends upon the extent to which these differences exist across easily recognizable disabilities with known average productivity differentials. A blind man is easily recognized and categorized. Someone with a heart condition is not. Even if all health conditions were observable, perhaps because applicants were required to declare them, how much would employers know about even average productivity specific to them? Rather than responding to an immediately recognizable disability group, employers might have only a partial, perhaps unconsciously biased, understanding of the productivity implication of an incompletely comprehensible health condition.
Empirical identification of discrimination against the disabled is difficult because disability, being an impairment of functioning, will certainly reduce productivity in many jobs. Getting hold of data that make it possible to control for real differences in productivity, and so isolate wage differences attributable to discrimination, is a tall order. Studies that control for little or no differences in health (Kidd et al., 2000) cannot credibly claim to identify discrimination against the disabled. But controlling for impaired functioning while comparing wage differences between the disabled and nondisabled seems to be like asking to have one’s cake and eat it. One approach is to concentrate on the wage differences between individuals with easily observed disabilities, such as blindness, paralysis, or loss of a limb, which may be more likely to evoke prejudice, and others who may be completely able-bodied or disabled by an unobservable condition, such as a back pain or heart problems. US data from the 1970s and 1980s reveal that one-third to one-half of the wage differential between these groups is unexplained by wage determinants, including a battery of health indicators intended to capture differences in functional impairments (Baldwin and Johnson, 1994; Johnson and Lambrinos, 1985). This finding is indicative of substantial discrimination only if the controls are sufficient to mop up any productivity differentials. DeLeire (2001) suggests another approach which involves assuming there are no unobserved productivity differences between individuals who report a health problem but no work limitation arising from this and others reporting no health problem. In that case, all of the wage difference between these two groups can be attributed to discrimination. This can be taken as indicative of the discrimination against those with a work-limiting disability under the further assumption that the degree of discrimination is independent of the productivity loss arising from disability. Under these assumptions, only 7—11% of the wage difference not explained by observable characteristics between US males with a work-limiting disability and those with no disability could be attributed to discrimination.[65] It is difficult to hazard a guess as to whether this estimate lies closer to the truth than the larger earlier one, given that both rest on rather strong assumptions.
17.3.2.3 Nonwage Costs and Nonpecuniary Benefits
The previous two subsections considered wage variation arising from health-related differences in (perceived) productivity. The employer was assumed powerless to correct productivity differentials. A richer model of the demand for disabled labor relaxes this assumption. The productivity of someone bound to a wheelchair is contingent on adjustments made to the workplace—ramps, elevators, adjustable desk, etc. Installation of such facilities involves incurring a fixed cost that pays off through raising the marginal product of disabled workers (Acemoglu and Angrist, 2001). Treatinglabor as a quasi-fixed factor, with the simplifying assumption that there are fixed costs associated with employing disabled but not able-bodied workers, and supposing that workplace modifications close the productivity gap between disabled and able-bodied workers, the wage paid to the former will be lower by the amount of the (discounted) fixed costs (Acemoglu and Angrist, 2001). Wage differentials need not reflect only productivity differences or discrimination. Even with perfect measures of productivity, an empirical test of discriminatory behavior would be difficult. A second implication of this model is that employers are likely to be particularly apprehensive about appointing disabled workers. Fixed costs incurred up-front must be compared with expectations of future marginal products and wages. A risk-averse employer will opt for labor with a higher proportion of variable costs.
11
Health-related wage variation could also arise from a willingness of employees to trade wage for nonwage benefits. The onset of a chronic condition would be expected to increase the value attached to employer-provided health insurance (Currie and Madrian, 1999). A worker suffering from a long-term illness would be more likely to accept a wage cut, or to forgo a pay rise, for fear of not being able to obtain insurance in a better paying job. Note that such health-related wage differentials do not imply differences in well-being. The individual is choosing to accept a lower price for his labor in return for obtaining a lower price for health insurance. Nevertheless, this would be an additional mechanism through which health differences may contribute to inequality in measured income, at last in countries with employment-based health insurance.
17.3.2.4 Evidence
Theory identifies mechanisms through which ill-health may reduce wages. But how large is the effect? Is health-induced variation large or small relative to overall wage inequality? The usual econometric demons—selection, omitted variables, reverse causality and measurement error—hinder attempts to answer these empirical questions. Evaluation of the evidence largely comes down to assessing the extent to which these problems have been overcome or avoided. Ill-health is likely to be a major reason for labor-force withdrawal (see next section). Estimation of the impact of health on wages from a cross section of workers or a balanced panel of individuals in continuous employment will overlook those whose wage opportunities were reduced most by ill-health and decided to stop working. Correction of this selection bias requires modeling employment, in addition to wages, with health allowed to impact both. With panel data, there may also be health-related attrition: those experiencing a marked deterioration in health might be more likely to drop out of the sample. Recognizing that individuals can influence their health through lifestyle, for example, leads to the realization that the same unobservable factors, such as time preferences, risk attitudes, and schooling quality, that influence job choices and thus wages may also condition investments in health. If panel data are available, then differencing can be used to purge the time-invariant unobservables correlated with health, or efficiency gains may be sought by using averages of assumed exogenous time-varying covariates to instrument health (Hausman and Taylor, 1981). Neither of these solutions is sufficient to remove bias if there is direct dependence of health on the wage. This is implied by Grossman’s seminal model of health determination (Grossman, 1972a,b), according to which the wage influences both the costs of, and the returns to, investments in health (see Section 17.4.1). Correcting or avoiding the threat of simultaneity bias requires identification from exogenous variation in health that does not arise from wage differences. Prices of medical care and, in a developing country context, the local disease environment have been used as instruments for measuring health (Strauss and Thomas, 1998). However, it can be difficult to find variation in prices that is not endogenous to the choice of medical care provider, and geographic variation may be a rather weak instrument (Currie and Madrian, 1999). Disease exposure is often correlated with weather and agricultural conditions that would be expected to impact wages directly.
Currie and Madrian (1999) provide a comprehensive review of the US evidence on the health impact on wages (and on labor supply) up to the end of the twentieth century. They note three main deficiencies in this evidence base. First, estimates are sensitive to the measure of health, and variability in the measures adopted impedes comparability across studies. We would add that this sensitivity does not merely reflect inconsistency in the measurement of health but is due to intrinsic heterogeneity in the effect depending on the nature of the health condition. Second, few studies attempted to correct for the potential endogeneity of health, and those that did relied on rather dubious exclusion restrictions. Third, most of the evidence available referred to white (US) males. Picking up from where Currie and Madrian (1999) left off, in the remainder of this subsection, we focus on the evidence published since 1999, using data from high-income countries. The latter two criticisms have, to an extent, been addressed in the more recent literature. The increasing availability of panel data, particularly on older populations that experience the most variability in health, as well as population level administrative data, has reduced reliance on instruments to deal with endogeneity. Although many studies still tend to focus on males, there are many exceptions, and the evidence comes from a wider spread of countries. All studies cited are summarized in Table 17.3 for evidence relating to the USA and Table 17.4 for studies that use data from European and other high-income countries.
A fixed effects estimate obtained from retrospective life history data collected in the first wave (1992-1993) of the US Health and Retirement Study (HRS) suggests that a work limitation lasting at least 3 months reduces the wage rate by 4.2% for males and twice that for females aged 50-60 (Pelkowski and Berger, 2004). Given that 7-9% of individuals in this age range report such a health condition, these estimates suggest that ill-health makes a substantial, though not dramatic, contribution to wage inequality. Using 25 years of longitudinal data from the US Panel Study of Income Dynamics (PSID), Charles (2003) obtains a fixed effects estimate (corrected for selection into employment) only half as large for men for a similar measure of ill-health experienced by almost one-third of the sample at some time during the panel. This would suggest a much more modest contribution of ill-health to wage inequality. The lower estimate obtained by Charles may be attributable not only to the use of panel data, rather than retrospective, but also to estimation using a younger sample. An analysis of the same dataset and health measure, taking account of simultaneity as well as selection and unobservable heterogeneity, finds that below the age of 35 and above the age of 62 there is little difference between the wage profiles of individuals in good and bad health
Table 17.3 US evidence of health effects on labor market outcomes
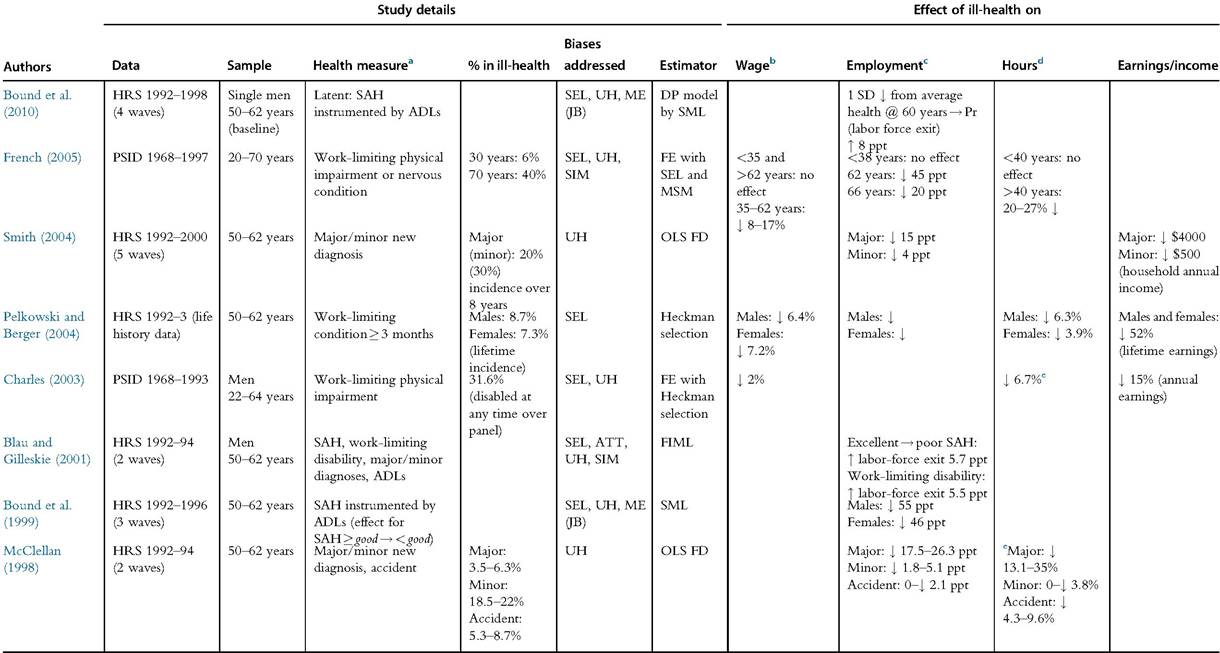
Notes: Table excludes earlier (pre-1998) studies Summarizedin tables presentedin Currie andMadrian (1999). JB,justification bias; ME, measurement error; SIM, simultaneity bias; SEL, selection bias; UH, unobservable heterogeneity (OVB bias). See Table A2 for explanation other acronyms, including those of datasets and variables.
aEffects on outcomes are with respect to this health measure.
b Impact on hourly wage for those in employment.
cImpact on probability of employment unless otherwise stated.
dRelative impact on annual work hours.
eAssuming average annual work hours of 1800.
Table 17.4 European and rest-of-world evidence of health effects on labor market outcomes
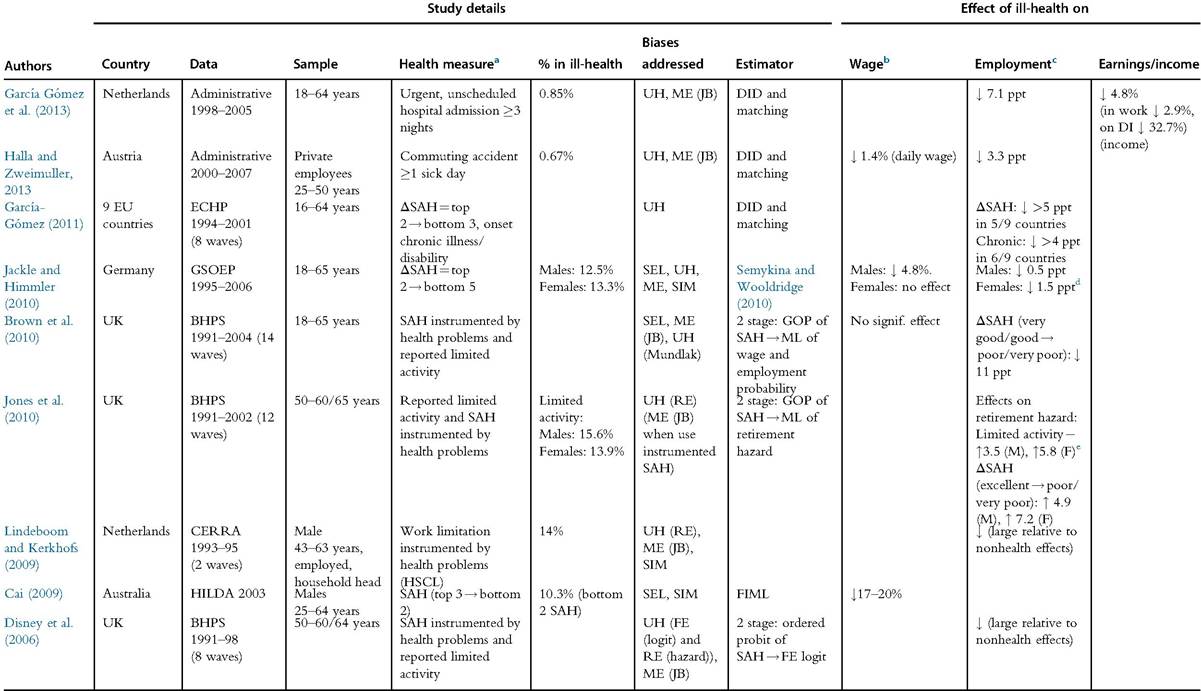
Continued
Table 17.4 European and rest-of-world evidence of health effects on labor market outcomes—cont'd
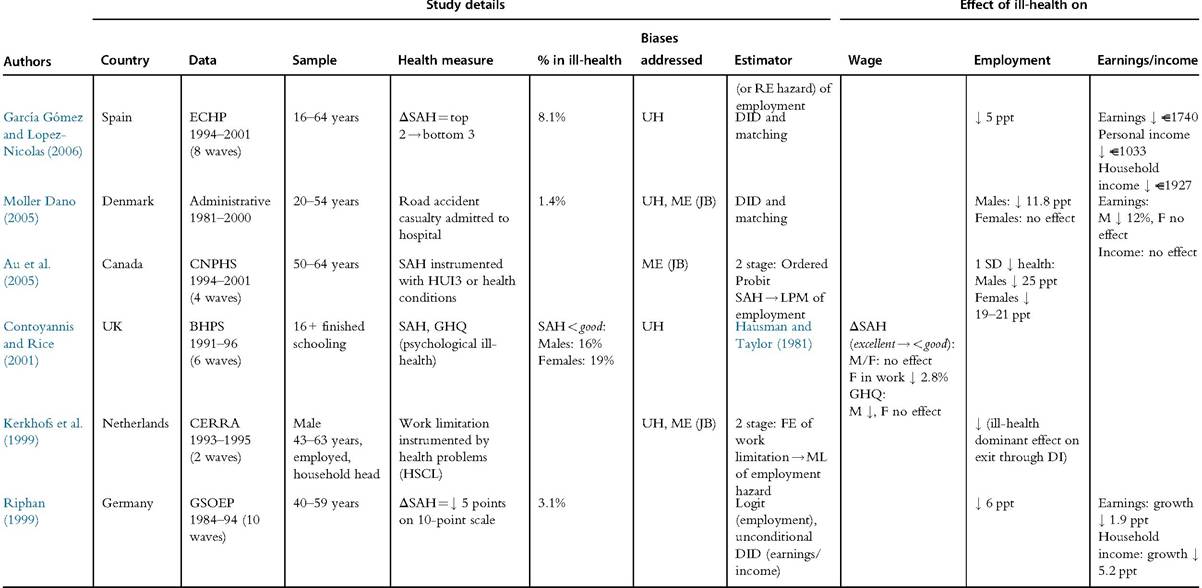
Notes: Table excludes studies published pre-1999. JB, justification bias; ME, measurement error; SIM, simultaneity bias; SEL, selection bias; UH, unobservable heterogeneity (OVB bias). See Table A2 for explanation other acronyms, including those of datasets and variables.
aEffects on outcomes are with respect to this health measure. b Impact on hourly wage for those in employment.
cImpact on probability of employment unless otherwise stated.
dEstimates from one of estimators used to correct for selectivity bias. Estimates from other estimators vary greatly, reaching effects of 16—19% points.
eDespite the large impact of a health shock on the retirement hazard, few individuals experience such a shock, and early retirement is simulated to be only 11% above what it would be in the absence of the shocks incurred.
(French, 2005). But in the prime ages of working life, individuals with a work limitation can command wages around 8-17% below the wages of those in good health.
Using UK panel data and the Hausman and Taylor (1981) estimator, Contoyannis and Rice (2001) find a significant effect of psychological health, but not general SAH, on wages for males, but no interpretation of the magnitude of the effect is given. For females in full-time employment, there is a significant effect of SAH; moving from less than good health to excellent health is estimated to result in a rather modest wage increase of less than 3%.
A cross-section analysis of data on Australian men that attempts to allow for full simultaneity finds a large effect of SAH on wages (Cai, 2009). But the instruments used (health conditions and behavior) are of dubious validity, and exploitation of the panel dimension of the data using a fixed effects estimator results in a large reduction of the estimate and loss ofits significance.[66] Jackle and Himmler (2010) also resort to instruments in order to deal with endogeneity arising from more than correlated time-invariant unobservables in their analysis of German panel data. They assume that past doctor visits determine health but not labor-force participation or wages conditional on this. The rationale is that past medical care is the investment response to previous health shocks and need not be correlated with current labor market outcomes given current health. This may be so, but it does not allow for the possibility that individuals visit a doctor to obtain a sick note to justify work absence. For males, a worsening in reported health from excellent to poor is estimated to result in a 4.8% drop in the hourly wage. For females, there is no significant effect.
Although differences in health indicators and estimators still make it difficult to compare estimates, we tentatively conclude that ill-health does reduce wages in high-income economies, but the effect is more likely modest than substantial. Because most studies estimate the wage response to ill-health while controlling for occupation, this conclusion refers to the degree to which the wage adjusts within a given job. A larger wage effect may arise through ill-health induced changes in occupation. We examine this effect in Section 17.3.5.
17.3.3 HealthandWork
As would be expected, employment rates vary a great deal with health. This is illustrated in Figure 17.4 for China, the Netherlands, and the USA. In the two high-income countries, already in young adulthood, individuals reporting poor health are much less likely to be working than their contemporaries reporting better health. The difference in employment by health widens until middle age, after which early retirement begins to reduce labor-force participation of even those in good health and the employment gap narrows.[67] The relationship between employment and health is different in China in two respects. First, there is little or no difference in employment by health in young adulthood. Second, while a gap opens up at older ages, it never becomes as wide as that observed in the Netherlands and the USA. This is partly an artefact of self-assessed health being reported in four, rather than five, categories in the Chinese survey. But this is not the whole story. In the USA around the age of 50, the employment rate difference between those reporting fair health and those reporting excellent or very good health is about twice as large as the difference between those reporting poor health and those reporting very good health in China at the same age. The relationship between employment and health is weaker in China. This is not what one would expect given the differences in the structures of the economies and the greater role of manual labor in China. It may be that the more generous social protection in the high-income countries allows individuals experiencing health problems to more easily withdraw from the labor market.
In this section, we consider a number of mechanisms through which health may impact on employment, including the incentive effects of DI.
17.3.3.1 Incapacity and Involuntary Unemployment
The impact of ill-health on work may seem obvious. If you are sick, you cannot work. For relatively short term, acute illnesses, this is a reasonably adequate description of the effect. But it is an effect that could only explain temporary interruptions to earnings and income. Any substantial contribution of the distribution of health to the distribution of income is unlikely to operate through short-term sickness. A few chronic medical conditions are completely incapacitating. But most reduce capacity for work to some degree. Ill-health may reduce productivity, but it is unlikely that the marginal product is pushed to zero in all possible jobs. The wage could fall below the level at which work is considered worthwhile, but that is a choice rather than a fait accompli.
This reasoning rests on the assumption that wages are perfectly flexible. Evidence of a moderate impact of health on wages (see Section 17.3.2.4) may reflect institutional constraints on wage flexibility. Equal pay and antidiscrimination laws typically make it illegal for employers to pay disabled workers less than their able-bodied colleagues doing the same job. This may succeed in constraining health-related wage inequality but exacerbate disparities in employment.
The 1990 Americans with Disabilities Act (ADA) compels employers to accommodate disabled workers through adjustments to the workplace and outlaws discrimination against the disabled in hiring, firing, and pay. In theory, the impact on employment of the disabled is ambiguous. The threat of legal action for discrimination in hiring would tend to increase employment, while increased accommodation and hiring costs would reduce employment. Acemoglu and Angrist (2001) argue that the negative effects are likely to dominate. Before and after legislation, trends in employment are consistent with this prediction (Acemoglu and Angrist, 2001; DeLeire, 2000). Employment of disabled individuals was also reduced immediately after the introduction of the UK Disability Discrimination Act in 1996, which imposed similar obligations on employers as the ADA, before it recovered somewhat (Bell and Heitmueller, 2009). Digging deeper into the effect in the USA, Hotchkiss (2004) reveals that it is not due to individuals always classified as disabled being more likely to leave employment or less likely to enter employment. Rather, it is due to nonparticipants in the labor market reclassifying themselves as disabled after the passing of the legislation. Whether antidiscrimination legislation makes it more difficult for disabled individuals to obtain work may still be an open question. What seems clear is that there is no evidence that major legislation makes it easier for disabled individuals to gain employment.
17.3.3.2 Disability Insurance
Any illness-induced reduction in the offer wage makes labor-force participation less financially attractive. Ifthe decline in health is sufficient to qualify for DI, then financial disincentives to work are compounded. Qualification for DI is not unambiguous (Diamond and Sheshinski, 1995). It is typically not determined by the presence of a precisely defined medical condition but is assessed on the basis of the vague concept of “capability of performing paid work,” perhaps taking account of workplace conditions and occupation. There is subjectivity in whether a person considers himself incapable of work, as well as whether the adjudication officer agrees. Financial incentives can tilt the balance in favor of applying for DI. For a given degree of work incapacity, withdrawal from employment is more likely when social protection is available to cushion the resulting loss of income (Autor and Duggan, 2006; Bound and Burkhauser, 1999; Gruber, 2000; Parsons, 1980).
By increasing the likelihood of labor-force withdrawal but compensating for the resulting income loss, the existence and generosity of DI may simultaneously strengthen the relationship between health and earnings, and it may weaken the relationship between health and income.[68] For a given distribution of health, income would be expected to be more equally distributed in countries with generous DI. But the equalizing effect of social protection may be weakened by a moral hazard effect that is stronger for individuals with lower earnings potential. If, as is usually the case, the replacement rate is decreasing with predisability earnings, the financial disincentive to continue in employment will be greatest for lower-paid workers. As a result of these differential incentives, onset of a given disability is more likely to result in employment withdrawal and loss of earnings (only partially replaced by DI) of lower-paid workers. This differential moral hazard effect will tend to increase income inequality relative to the hypothetical situation in which the financial incentives arising from DI have no impact on employment. But in the complete absence of DI and the income protection it provides, income inequality would be likely to be even greater. In addition to the strength of the differential moral hazard effect, the extent to which DI reduces income inequality will depend on the incidence of disability. The equalizing effect will be greater if, as is likely, the poor are more likely to become disabled. The lower paid are more likely to both benefit from social DI and respond to its financial disincentives to work.
DI rolls have been rising over much of the past 30 years in many high-income countries (OECD, 2010; Wise, 2012). Steep downward trends in mortality rates, accompanied by a compression of disability, if not disease, into fewer years before death (Crimmins and Beltran-Sanchez, 2011; Cutler et al., 2013; Milligan and Wise, 2012), suggest that this is not because populations are becoming less healthy. Looser eligibility criteria and increased returns from claiming DI relative to those available from work are considered to be the chief culprits (Autor and Duggan, 2006; Bound and Burkhauser, 1999; OECD, 2010; Wise, 2012). We will not evaluate the evidence concerning the strength ofthe moral hazard effect of DI (Bound and Burkhauser, 1999) but concentrate on the proposition that it interacts with increased economic inequality arising from structural changes in the economy to reduce labor-force participation of low-skilled, low-paid workers (Autor and Duggan, 2003, 2006).
The falling relative wages and employment opportunities experienced by low-skilled workers in the USA and other high-income countries since the 1980s increases the attractiveness of DI for this group (Autor and Duggan, 2003; Black et al., 2002). Dependence of DI awards on ability to engage in gainful employment results in DI applications tending to rise in an economic downturn (Autor and Duggan, 2006) and suspicion that some governments deliberately use DI to disguise long-term unemployment. After the loosening ofthe Social Security Disability Insurance (SSDI) eligibility criteria in the USA in the mid-1980s, the sensitivity of applications to adverse economic conditions increased by at least twofold, and high school dropouts became twice as likely to exit the labor force on the occurrence of a negative shock to the economy (Autor and Duggan, 2003). The effect is compounded by the indexing of the SSDI benefit formula to average wage growth. As a result, the replacement rate has increased for individuals whose wage growth lagged the average, as has been the case for low-paid workers in the USA over the past 30 years (Autor and Duggan, 2003, 2006). The replacement rate was further increased by rising real expenditures on Medicare, the health insurance program for the elderly that SSDI beneficiaries are given entitlement to before reaching the age of 65. Taking into account these fringe benefits, the DI replacement rate for a 50- to 61-year-old male at the 10th percentile of the earnings distribution increased from 68% in 1984 to 86% in 2002 (Autor and Duggan, 2006). At the 90th percentile, the increase was much more modest, from 18% to 22%. As would be expected given these differential incentives, SSDI enrolment rates are much higher and have increased much more rapidly for low-skilled individuals. For male high school dropouts aged 55-64, the rate increased by 5% points between 1984 and 2004 to reach almost 20% (Autor and Duggan, 2006). The increase was only 1% point (to reach 3.7%) for the college educated.
In the USA, reduced earnings prospects relative to the average and increased DI replacement income relative to those reduced earnings, separately and in combination, have reduced the incentives for low-skilled workers with health problems to continue working. Increased reliance of this disadvantaged group on DI may be both a consequence of rising economic inequality and, given the replacement ratio is less than one, a contributor to it. This process may also operate in Europe, which also witnessed increased wage inequality and, at times, rising DI rolls since the 1980s.
17.3.3.3 Preferences
In addition to an indirect effect through DI, ill-health may shift the reservation wage directly by changing preferences for consumption relative to leisure. The direction of the effect is ambiguous. Ill-health would be expected to increase the disutility of work. But it may also reduce the marginal utility of a number of leisure activities, such as sport. The direction of the effect on the marginal utility of consumption is even more difficult to predict. A disabled person may derive less, or no, pleasure from some goods, including sports equipment or travel, but become more dependent on others, such as pharmaceuticals, heating, and private as opposed to public transport. Comparing the relationship between subjective well-being and consumption—proxied by permanent income— for older Americans with and without chronic illness, Finkelstein et al. (2013) infer that the marginal utility of consumption decreases with ill-health. If we assume that the increased disutility of work dominates, such that the marginal utility of leisure rises, this gives a clear prediction that the marginal rate of substitution of leisure for consumption rises when health falls. The reservation wage rises and labor-force withdrawal becomes more likely.[69] More direct evidence suggests that a work-limiting health problem is equivalent to aging around 4 years in the extent to which it increases the willingness of older (58 +) Americans to trade consumption for leisure (Gustman and Steinmeier, 1986a,b).[70]
While these estimates support the plausible proposition that ill-health shifts preferences away from work, one should be careful not to overlook the multidimensionality of health. A physical disability may reduce the marginal utility of many leisure pastimes as much as, or more than, it raises the disutility of work. A chronic illness such as diabetes may have little or no impact on preferences for leisure relative to consumption. The empirical content of a prediction that preferences for work increase with a characteristic we conveniently refer to as health is blurred if that characteristic, or at least the means of measuring it, is not well defined. In the social sciences, we are rather attached to the concept of health, despite finding it difficult to define what we mean by it (Twaddle, 1974). Estimates of the impact of ill-health on work-leisure preferences are likely to vary with the dimensions of health examined and the indicators used to measure them.
17.3.3.4 Life Expectancy
Expected longevity is an additional mechanism through which differences in health may contribute to observed differences in income and wealth in a cross section. In the standard life cycle model of consumption with no bequest motive in which there is dissaving before death, a longer length of life is predicted to increase labor supply (and saving) at any given age (Chang, 1991; Hammermesh, 1984). This is basically a wealth effect. Increased lifespan implies greater lifetime potential income. The resulting increase in demand for consumption prompts a rise in labor supply.[71] We may refer to this as the horizon effect. Individuals in poor health work less because they do not have to provide for an extended old age. For a given degree of functional impairment, illnesses that are life-threatening, or at least life-shortening, should be observed to reduce earnings by more than chronic disabilities that present no threat to longevity (McClellan, 1998).
Recognizing that the length of life is uncertain and annuity markets are incomplete gives rise to an offsetting effect. Through the mortality risk on savings, or the prospect of dying before being able to enjoy the fruits of one’s savings, variation in survival probability affects the marginal return on savings and, consequently, the marginal rate of substitution between consumption and leisure (Chang, 1991; Kalemli-Ozcan and Weil, 2010). Through this uncertainty effect, a reduction in the probability of death raises the return on and, thus, level of savings, making it possible to reduce labor supply, perhaps by retiring earlier, even when there is a longer expected length of life to be provided for. The chances of this uncertainty effect dominating the horizon effect decrease with the initial mortality rate (Kalemli-Ozcan and Weil, 2010). In high-income countries, one expects ill-health and reduced longevity to be associated with lower earnings (and wealth).
17.3.3.5 Evidence
Apart from the ambiguous effects of preferences and longevity, theory gives the clear prediction that ill-health reduces work effort. Under reasonable assumptions for high- income economies, the effects of preferences and longevity go in the same direction. But what is the size of the overall effect of ill-health on employment?[72]
Most studies address this question using samples of older individuals. Effectively, they estimate the impact of health on (early) retirement. In general, health is found to be an important determinant of retirement (Currie and Madrian, 1999; Lindeboom, 2012). How important depends on the measure of health and estimator adopted, as well as the context.
Estimating the effect of health on employment is complicated by econometric obstacles similar to those confronted when trying to identify the impact of health on wages, only the measurement error problem becomes particularly thorny. Most studies have relied on survey data and self-reported measures of ill-health. One would expect the reporting of health to be endogenous to employment. Put most crudely, individuals who have decided not to work may lie about their capacity to work either to reduce the stigma attached to voluntary inactivity or because they are claiming DI. But the phenomenon need not be so blatant. The threshold of functioning at which an individual considers himself to be incapable of work may be influenced, possibly subconsciously, by financial incentives to work, job stimulus, length of working life, contact with others claiming DI, and so on. Reported ill-health may reflect motivations for not working. This so-called justification bias has been a major concern in the literature (Bound, 1991). The evidence tends to suggest that it leads to substantial overestimation of the effect of ill-health on employment (Bazzoli, 1985; Bound et al., 2010; Lindeboom, 2012; Lindeboom and Kerkhofs, 2009), although there are dissenting findings (Dwyer and Mitchell, 1999; Stern, 1989).
Replacing reported work incapacity with more objective indicators of chronic illnesses or future mortality reduces the risk of justification bias but increases classical measurement error and may result in underestimation of the effect (Bound, 1991). Instrumenting reported work limitations with more objective health indicators is arguably a better approach (Bound, 1991; Bound et al., 2010; Stern, 1989) but requires that the indicators are free of the justification bias, which may be a strong assumption given these are often also self-reported.
All studies from North America and Europe that attempt to deal Withjustification bias by treating self-reported health as endogenous confirm that health is an important determinant of labor-force participation (Au et al., 2005; Blau and Gilleskie, 2001; Bound et al., 1999; Brown et al., 2010; Disney et al., 2006; Dwyer and Mitchell, 1999; Jones et al., 2010; Kerkhofs et al., 1999; Lindeboom and Kerkhofs, 2009; Sickles and Taubman, 1986; Stern, 1989).[73] Health also emerges as a strong determinant of retirement in structural life cycle models of older US males (Bound et al., 2010; French, 2005; Sickles and Yazbeck, 1998). Boundet al. (2010) find that, although responding to justification bias by instrumenting self-reported health with objective indicators greatly reduces the health effect, this effect remains very large. Before the early retirement age, an older single male in bad health is five times more likely to withdraw from the labor force than an equivalent in good health.[74] When US workers reach 62, the age at which Social Security pensions can first be claimed and financial incentives shift in favor of retirement, the probability of withdrawal rises from 0.1 to 0.17 for those in poor health and from 0.025 to 0.049 for those in good health. In absolute terms, those in poor health react more to the financial incentives such that the difference in employment probabilities widens when it becomes financially more advantageous to retire. Ill-health and financial incentives interact. Financial incentives appear to tilt the balance toward considering a health problem to be incapacitating. From a low level of health, marginal deteriorations in health have a large effect. At age 62, when the health of a worker in poor health decreases by one-half of a standard deviation, the probability of that worker’s labor-force exit increases from 0.17 to 0.27; this change is 10 times larger than the change in probability for a comparable worker in average health.
Extending the scope of analysis beyond older US males, French (2005) finds a very strong health effect that varies across the lifecycle. Below the age of 40, there is no difference in the employment rate of men in good and bad health. At 40, an incapacitating physical or nervous condition is estimated to reduce employment probability by 5% points for a stereotypical male. The effect reaches a peak of 60 points at age 58 before declining to 45 points at age 62 and 20 points at age 66. In responding to these very large effects, one needs to bear in mind that they are not corrected for justification bias. Despite the very large estimated health effect, the author argues that it is modest in terms of the proportion of the total decline in older male labor-force participation that can be attributed to population health. The percentage of males reporting an incapacity rises from 20% at age 55 to 37% at age 70. Applying the estimated health effect, this decline in health can explain only 7% of the 74% fall in labor-force participation between these ages. This may be so, but the estimates of both French (2005) and Bound et al. (2010) imply that ill-health can account for a substantial fraction of labor-force withdrawal before the early retirement age of 62.
Establishing a substantial effect of health on employment only takes us part way toward our objective of gauging the contribution of health to the distribution of income. We need to know the earnings and, ultimately, income consequences of illness-induced loss of employment. Reviewing the earlier US evidence, Currie and Madrian (1999) conclude that ill-health has a large negative effect on earnings, which operates mainly through reduced hours of work, including nonparticipation, rather than reduced wages.
From the US HRS life history data, Pelkowski and Berger (2004) find that 7—9% of individuals over the age of 50 have experienced a work limitation at some time that, on average, is estimated to result in the loss of half of their potential future earnings. By far the greatest part of this substantial loss is from the reduced likelihood of working, which falls to around half of its counterfactual value. Taken at face value, these estimates suggest that health is a major determinant of earnings differences. Caution should be exercised in their interpretation, however. A major concern is the retrospective nature of the data, which may be vulnerable to recall, as well as justification, bias. There could be a tendency to report health events that did have labor market consequences and to recall changes in labor outcomes that coincided with periods of illness.
Charles (2003), using the US PSID, finds that annual earnings of initially employed individuals fall, on average, by 15% around the time of onset of disability. Given that almost one-third of the panel experiences a work limitation at least once, this suggests that ill-health is an important contributor to cross-sectional inequality in earnings. But earnings do not remain as depressed as they are immediately following the onset of ill-health. Some illnesses recede and disabilities can be adapted to through retraining. Within 2 years of the onset of disability, about half of the earnings loss is recovered. Subsequently, earnings continue to trend upward, rather slowly, toward the level at which they would have been without the worker having experienced the disability. These findings suggest that Pelkowski and Berger (2004) substantially overestimate lifetime earnings losses by extrapolating from the contemporaneous impact of ill-health on earnings.
While the PSID study provides valuable insight into the impact of ill-health on earnings, it is weakened by reliance on self-reported work limitation with no correction for justification bias. The steepest drops in earnings occur in the period between 1 and 2 years prior to the reporting of a work limitation. One interpretation is that health is declining and impeding labor outcomes prior to the point at which a health problem is reported. But another is that decreasing returns to and motivation for work lead to the reporting of a disability, perhaps to justify entry to DI.
Besides its vulnerability to justification bias, another limitation of the reported work capacity measure is that it focuses on functional impairment and does not discriminate other dimensions of health, such as longevity. This is not sufficiently recognized in part of the literature, which tends to presume that the ideal measure of health would be one that accurately informs of work capacity (Bazzoli, 1985; Bound, 1991; Lindeboom, 2012). Implicitly, the assumption is that there is only one mechanism through which health impacts employment—physical and mental capacity to perform work-related tasks. Recognizing the other mechanisms identified in the preceding subsections, health conditions that differ with respect to their implications for current functional impairment, prospects of recovery, survival chances, and so on can be expected to have differential impacts on work.
McClellan (1998) makes an interesting distinction between three types of health outcomes. Major health events, such as a severe heart attack or a stroke, imply both acute and long-term functional impairment and reduced life expectancy. Onset of a chronic illness, such as a heart condition or diabetes, does not dramatically affect current functioning but may affect labor supply through expectations given prospects of a degenerative disease and long-term impairment. At the other extreme, accidents have an immediate impact on functioning but are less likely to have any effect on preferences or health expectations in the long term. Using the first two waves of the US HRS, McClellan finds evidence consistent with the nature of the health event having an independent effect on employment over and above that of the degree of functional limitation arising from it. For a given change in functioning (measured by Activities of Daily Living (ADL)), the reduction in the employment probability is 40 points greater when it is precipitated by a major health event. The employment probability falls by 14% and 35% points for males incurring a new chronic illness with moderate and major reductions in functioning, respectively. Accidents are not significantly associated with a decline in employment. McClellan interprets this as indicative of employment effects being muted when the health event does not have consequences for long-term health expectations.[75]
Smith (2004) extends this type of analysis by using more waves of the HRS to look at longer term effects. Onset of a major health condition (i.e., cancer, heart disease, lung disease) is associated with an immediate reduction of 15% points in the employment probability of males among whom just over half were working at baseline. After 8 years, those contracting such an illness are 27 points less likely to be working. The short- and long-term effects for those succumbing to a minor chronic illness (i.e., hypertension, diabetes, arthritis, heart attack, angina, and stroke) are reductions of 4% and 11% points, respectively. The average loss in annual household income immediately following the onset of a major chronic illness is $4000, which rises to $6250 after 8 years. Cumulating these losses gives a total loss of income over 8 years of $37,000. The cumulative income loss associated with a minor condition is almost $9000.
Although this evidence of sustained reductions in employment and income appears to contradict that of Charles (2003), it does not once the older age of the HRS sample is recognized, and the heterogeneity in the effects estimated by Charles is scrutinized. Men that become chronically disabled, defined as reporting a work limitation in every period after the initial onset, experience an estimated initial earnings loss of 21% with little or no recovery over time. The initial loss is also greater and the recovery absent for older men. So, both studies find substantial permanent losses of income for older males succumbing to a chronic condition.
Bound et al. (1999) focus on the implications of the dynamic evolution of health for the continued labor-force participation of older (50+) US workers. They find that it is health deterioration, rather than the health level arrived at, that most affects labor-force exit. Employment is not simply dependent on current functional capacity because there can be adaptation to impairments. A drop to any given level of health implies lower expectations of future health that may have an independent effect on the decision to continue in employment. Disney et al. (2006) take the same approach with British data and find a different pattern of behavior. Controlling for past health, lower current health still increases the likelihood of job exit. But for any given level of current health, a lower level of past health also raises the probability of retirement. A possible interpretation of this result is that individuals take time to revise their health expectations downward. Only when health is persistently lower is the decision made to retire, which may be difficult to revoke.
Cross-country comparisons can be useful for exploring the extent to which the employment and income responses to ill-health appear to be influenced by employment and social policies. Garcia-GtSmez (2011) compares the likelihood of continuing in employment following a sustained drop in SAH in nine EU countries. She finds the employment effects are largest in Ireland, a country in which DI claimants are not allowed to engage in any form of paid work, followed by Denmark and the Netherlands, where replacement rates are highest and, as in Ireland, there is no quota on the percentage of employees that must be registered disabled. In France and Italy, the two countries that impose the highest quotas on disabled employees, there is no significant impact on employment. These findings suggest, but do not confirm, that the employment (and income) effect of ill-health is highly contingent on policies influencing both the demand and supply of disabled labor.
Rather than attempt to identify the health effect from data on self-reported general health, which is difficult to interpret and potentially endogenous, or reported work incapacity, which is possibly even more endogenous due to justification bias, three European studies have concentrated on more narrowly defined health events that are abrupt and unforeseen and so more plausibly exogenous to lifecycle planning of health and labor supply (Garcia Gomez et al., 2013; Halla and Zweimuller, 2013; Moller Dano, 2005). Unlike structural models that aim to estimate the endogenously determined lifecycle profiles of health and labor supply (Bound et al., 2010; French, 2005; Sickles and Yazbeck, 1998), the objective of these studies is to exploit some unanticipated shift in the health profile to estimate the response of employment and income. Two of the studies use accidents (Halla and Zweimuller, 2013; Moller Dano, 2005), and the third relies on urgent and unscheduled hospital admissions (Garcia Gomez et al., 2013). Implementation of this strategy is made feasible by the availability of population, or near population, data from administrative registers providing sufficient observations of relatively rare health events for which matches can be found from millions of control observations. Use of administrative records greatly reduces measurement error and avoids the justification bias that plagues estimates based on reported health. All three of the studies combine matching, which deals with observable differences, with taking difference-indifferences to eliminate correlation of the health event with time-invariant unobservables.
These studies consistently find that a health shock reduces the probability of employment. The estimates range from a 3.3% point reduction as a result of a commuting accident in Austria (Halla and Zweimuller, 2013), through a 7.1 point drop due to an acute hospital admission in the Netherlands (Garcia Gomez et al., 2013), to a 11.8 point fall following a road accident experienced by men in Denmark (Moller Dano, 2005). That the estimates differ in magnitude is to be expected given the narrow definition of the health events from which they are identified. Commuting accidents mostly give rise to musculoskeletal impairments, and diseases of the circulatory, digestive, and respiratory systems are all important causes of acute hospital admissions. Such different conditions would be expected to have different effects. A focus on specific health events that occur suddenly enhances the internal validity of these studies, but generalization to other forms of health deterioration cannot be presumed. There is no avoiding the multidimensionality of health and the consequent heterogeneity in its effects.
These studies confirm that ill-health causes employment to fall, a conclusion that could be made with less certitude from more weakly identified estimates. A less predictable finding is that the effect is persistent. All three studies find that the probability of employment remains reduced by a health shock for at least 5 years following its occurrence. This contrasts with what Charles (2003) finds for prime working-age US men. The difference is most likely attributable to the lack of incentives for DI recipients in continental Europe to move off the roll.
In Austria and the Netherlands, but not in Denmark, the impact on employment is greater for women. In the same two countries, the effects are greater on older persons and blue collar (Austria) or low-income (the Netherlands) workers. This is consistent with evidence from the UK showing that older poor individuals are more likely exit the labor force by entering disability insurance (Banks, 2006). It is also consistent with
22
There is no significant impact of a road accident on the employment probability of women. US evidence from the PSID that earnings losses from ill-health are larger and more sustained for nonwhites and the poorly educated (Charles, 2003), characteristics associated with working in industries and occupations in which productivity is more contingent on physical health and that identify low-skilled workers for whom, as observed in Section 17.3.3.2, labor market opportunities have deteriorated and dependence on DI has increased. The less privileged may not only be more likely to be struck by ill-health, but their employment and incomes are also more contingent on their health. Ill-health may increase economic inequality through both its skewed incidence and its differential effect.
In the Netherlands, an acute hospital admission results in an average reduction of around 5% in personal income 2 years after the health shock, with little or no recovery over the following 4 years (Garcia Gomez et al., 2013). For individuals who remain in employment, income falls by only 3%, indicative of very modest reductions in wages and hours of work at the intensive margin. Those moving onto DI experience an income loss of one-third, which is broadly consistent with the DI replacement rate. Although this is a substantial drop, the moral hazard effects of providing more complete income protection are likely to be large in a country where at one time 10% of the working-age population was on DI. But Denmark does offer even greater insurance, with an average 12% average drop in male earnings maintained for 6 years after a road accident offset by a rise in transfer income such that there is no significant change in total income (Moller Dano, 2005). This does not imply that there is complete insurance. Presumably, the 12% who lose employment do experience income losses, but this is not reported. For women, there is no significant drop in earnings or loss of income. These findings are consistent with the income consequences of ill-health being muted in a country, such as Denmark, with a generous welfare state. But one should keep in mind that it is the effect of a road accident that is estimated. According to McClellan (1998), accidents should have the mildest economic consequences because the induced health change may be temporary, and longer term functioning and survival expectations may be little affected. This is the limitation of the described approach. Although one can be confident that the estimate does accurately capture the effect of the health change studied, the rarity of the narrowly defined event reduces the relevance of the evidence to the broader question of the extent to which the overall variation in health contributes to observed economic inequality in the population.
17.3.4 Early-Life Health Determinants of Later-Life Economic Inequality The focus on the income effects of ill-health in adulthood until this point risks missing much of the action. A rapidly growing literature, to which Janet Currie and James Heckman are leading contributors, argues that early-life—even prebirth—and childhood conditions, including health, explain much of the variation in economic outcomes across adults (Almond and Currie, 2012; Cunha et al., 2006; Currie, 2009; Heckman, 2007; Heckman et al., 2006). It has been estimated that a staggering 50% of inequality in the present value of lifetime earnings in the USA can be explained by factors known at age 18 (Cunha and Heckman, 2009). Although most, such as parental occupation, are not directly health-related, exposure to health risks in the womb, infancy, and childhood is a potentially important component of these economically significant conditions. Ill-health in early life may directly constrain health capital in later life and impede the accumulation of nonhealth human capital. Both effects would reduce earnings potential.
One may distinguish three broad mechanisms through which early-life health may impact on economic outcomes in adulthood, differentiated by the life stage in which they become manifest. Nutritional deprivation and exposure to health risks in utero and in infancy can directly impair cognitive functioning and lead to childhood health problems that interfere with the acquisition of cognitive, and possibly noncognitive, skills. A second route is through education. Ill-health in childhood and adolescence may restrict opportunities to acquire education, and impaired cognitive functioning arising from insults to health in infancy may reduce the efficiency of schooling in producing educational qualifications. The third mechanism operates through health capital, as opposed to other forms of human capital. Ill-health may persist from childhood to adulthood. More dramatically, exposure to health risks in the womb may do lasting physiological damage, which becomes manifest with the onset of disease in middle age. Earnings may subsequently fall, as is clear from the evidence reviewed in the previous section.
In the following subsections, we discuss each of these three broad mechanisms by which infant and childhood health may constrain economic success in adulthood. This takes us into territory that has traditionally been the domain of psychology and epidemiology but in which economists are increasingly daring to venture. We end the section by summarizing and evaluating the evidence on the extent to which adult economic outcomes are determined by early-life health conditions. We do not provide detailed reviews of the rapidly growing literatures, which have already been provided by researchers with far greater expertise (Almond and Currie, 2011, 2012; Cunha et al., 2006; Currie, 2009). Our focus is on what the literature has to say about the contribution of health to income inequality and to understanding the association between income and health in adulthood.
17.3.4.1 Health, Cognitive, and Noncognitive Capabilities
There is abundant evidence that cognitive functioning is a strong predictor of wages (Cawley et al., 2001; Herrnstein and Murray, 1994; Jencks, 1979). We are interested in whether cognitive functioning measured during childhood determines economic success later in life and whether childhood cognitive function is in part determined by health in infancy. Case and Paxson (2008) provide indirect evidence of the first relationship. Using longitudinal data from the UK, they show the strong positive correlation between earnings and adult height.[76] This relationship is well established, but it falls greatly in magnitude and becomes insignificant when cognitive functioning in childhood, which is shown to be a strong predictor of wages, is controlled for. The change resulting from the cognition control is consistent with early-life nutrition producing both cognition and height and only the former impacting on earnings. After dealing with bias arising from cognition measured in adolescence being a product of (endogenously chosen) schooling, Heckman et al. (2006) find that cognitive functioning is an important determinant of schooling, employment, occupation, and wages.
So, cognitive functioning in childhood has economic consequences. Do we know that cognition itself is contingent on health in infancy? Through animal experiments, neuroscience has identified the biological and neurological processes that link undernutrition, as well as nutrient deficiency and exposure to toxins, in utero and infancy to impeded development of the brain (Grantham-McGregor et al., 2007). Birth weight, which is an indicator of exposure to health risks in utero, particularly nutritional deprivation, is the most frequently used indicator of the health of humans at birth. Epidemiological studies confirm that low birth weight is associated with low IQ (Breslau et al., 1994), along with a host of other child health problems including asthma (Nepomnyaschy and Reichman, 2006), behavioral problems including attention deficit hyperactivity disorder (ADHD) (Hayes and Sharif, 2009; Loe et al., 2011), slower motor and social development (Hediger et al., 2002), and depression (Costello et al., 2007). While consistent with the neuroscience, one cannot read too much into a simple correlation because low birth weight could reflect the behavior of the pregnant mother correlated with later investments in the child that influence cognitive functioning. Variation in birth weight within siblings and twins has been used to reduce the risk of such bias. This approach has produced evidence that the smaller sibling or twin tends to have a lower IQ at age 7 in Scotland (Lawlor et al., 2006) and on entrance to the military in Norway (Black et al., 2007). The latter finding is more difficult to interpret because IQ in young adulthood could reflect differential investment in education.
In low- and middle-income countries, where the nutritional and micronutrient deficiencies are obviously much more pronounced, there is clearer evidence from randomly assigned nutrition supplementation programs that better nutrition improves cognitive functioning and raises educational attainment (Grantham-McGregor et al., 1991, 2007; Pollitt et al., 1993; Walker et al., 2005). Currie (2009) cites evidence showing that even in the US children of mothers included (not randomly) in a nutritional program during pregnancy achieve higher test scores.
Heckman and his collaborators present evidence demonstrating that noncognitive skills developed in childhood are as important, possibly even more important, than cognitive functioning in explaining economic outcomes in adulthood (Cunha and Heckman, 2009; Heckman, 2007; Heckman et al., 2006). Noncognitive capabilities refer to personality traits, such as self-esteem, perseverance, dependency, consistency, patience, and optimism, which may be considered to be determinants or aspects of preferences over risk and the timing of consumption. Currie (2009) points out that some noncognitive skills are closely related to, or are highly contingent on, mental health conditions. She cites a number of studies presenting evidence that child behavioral problems, such as ADHD and aggression, are strong predictors of lower cognitive functioning, educational attainment, and economic outcomes. Most of the studies control only for observables, but Currie and Stabile (2006) use sibling fixed effects and find that children in both the USA and Canada with high ADHD scores at younger ages had lower cognitive functioning (math and reading test scores) at age 11 and were more likely to be admitted into special education and to have repeated a grade. Given that behavioral mental health problems are so prevalent in children, they are potentially an important part of the link between child health and adult economic circumstances.
23
Although the evidence base does need strengthening, we believe that there are sufficient conceptual grounds for expecting health in infancy and early childhood to emerge as an important constraint on the formation of cognitive and noncognitive skills that are increasingly recognized as important determinants of labor market success. Within the framework developed by Cunha and Heckman (2008), the importance of these skills in the generation and reproduction of economic inequality derives from the fact that they are malleable. Skills are produced through parental investments, the level and efficiency of which are likely to depend on the socioeconomic environment of the child’s family and neighborhood. Heckman (2007) hypothesizes that there may be complementarities between investments in health and cognition. Bad luck of the draw that leaves a child with a deficit of one may make it more difficult to raise the other through investments. An early-life health shock could leave a child frail, with limited capacity to respond to the stimuli that can raise cognitive functioning. Facing a higher price for a marginal gain in functioning, parents may invest less in the development of the child’s skills. Thus, sickly kids may be doubly penalized with a deficit in both health and human capital.
17.3.4.2 Education
Education is a potential conduit that links income to health not only over the life cycle but also across generations. Health problems in childhood may directly constrain the acquisition of education, as well as weaken incentives for investment in schooling, with long-run consequences for income. Ifthe children of poorer and less healthy parents are more likely to experience illness, then the interference of health capital in the acquisition of other forms of human capital could contribute to the intergenerational transmission of income (Currie, 2009). Health determination of income distribution may operate with a very long lag.
According to life course epidemiology (Kuh and Ben-Shlomo, 1997; Kuh and Wadsworth, 1993; Wadsworth and Kuh, 1997), childhood illness, which may arise from social deprivation, not only has a permanent effect on health, but it also interferes with education. As a result, occupational opportunities are limited in young adulthood, which may further reduce adult health, and lifetime earnings potential is constrained. Health and income in adulthood are correlated because they are both determined by childhood illness.
The most straightforward way in which health may impact education is through the interruption of schooling. In low-income countries, this could be an important constraint. In high-income countries, it seems less relevant. Currie (2009), citing Grossman and Kaestner (1997), notes that differences in school absence rates between healthy and unhealthy US kids are too small to lead to a strong correlation between health and educational attainment. Any impact of child ill-health on knowledge and skills acquisition more likely operates through the channel examined in the last subsection constrained cognitive functioning and impaired efficiency of learning.
Using a cohort of Britons born in 1958 and controlling for childhood socioeconomic status (SES), Case et al. (2005) find that a health problem in childhood is correlated with lower educational attainment. But poor health and low education could both result from parents who make little investment in the human capital of their offspring. A partial solution is to go one stage back in the child’s development when parental behavior can exercise less influence and examine the association between birth weight and educational attainment. We noted above the evidence of the impact of birth weight on cognition. If this is the channel, we now need to establish the next link in the chain, to educational outcomes. There are many epidemiological and social science studies showing that children with very low, or even low, birth weight tend to perform poorly in school (Case et al., 2005; Currie and Hyson, 1999; Hille et al., 1994; Kirkegaard et al., 2006; Saigal et al., 1991). The causality of the relationship is given credence by sibling and twin difference studies of sufficiently large samples from high-income countries across three continents. These studies show lower educational attainment by the children who were smaller at birth (Behrman and Rosenzweig, 2004; Black et al., 2007; Johnson and Schoeni, 2011; Lin and Liu, 2009; Oreopoulos et al., 2008; Royer, 2009). There is, however, variation in the magnitudes of the estimates. For example, using US PSID data, Johnson and Schoeni (2011) find that low birth weight increases the probability of dropping out of high school by one-third, with part of the effect appearing to operate through impaired cognitive functioning. Royer (2009), using data on twins who both became mothers in California, finds a rather small average effect.[77] A claimed feasible 250 g increase in birth weight would raise schooling by only 0.04 of a year.
A couple of US studies only find significant or substantial effects for children born into poor families or neighborhoods (Conley and Bennett, 2001; Currie and Moretti, 2007). This is consistent with wealthier parents being able to compensate for a health disadvantage in early life, when poorer parents lack the means to invest in medical care or other health and educational inputs. Other studies conducted with British (Currie and Hyson, 1999), Norwegian (Black et al., 2007), and Canadian (Oreopoulos et al., 2008) data find no evidence of this heterogeneity. Hasty attribution of this discrepancy to the equalizing effect of universal health care coverage in Europe and Canada, but not in the USA, would be foolhardy. The 1958 British cohort would have had access to only rudimentary medical interventions for the treatment of low weight babies by today’s standards (Almond and Currie, 2012). But it could be that little treatment was available for both rich and poor low-birth-weight babies in 1950s Britain. The pertinent question is whether the gradient observed in the more recent US data arises from differential access to effective medical care and possibly other corrective interventions. It may also be that the incentives parents have to make investments that compensate for poor child health differ between the rich and the poor. A particularly tight budget constraint may not allow investment in all offspring. It can then be optimal to concentrate investments on the child with the best chance at the expense of the child the parents observe to be frail and likely to struggle in life in any case (Almond and Currie, 2012).[78]
There is emerging evidence of a link between measures of school performance, or educational attainment, and in utero exposure to health risks through disease (Almond, 2006; Kelly, 2011), radiation (Almond et al., 2009), and maternal alcohol consumption (Nilsson, 2009). This is arguably a more convincing strategy to identify the effect of early- life health on education than that of twin differences because it uses variation in infant health risks that is external to the family environment and so is more plausibly exogenous to factors that also impact on schooling. Even more convincing is evidence that treatment of children for disease raises school attendance (Bleakley, 2007; Miguel and Kremer, 2004).
The evidence is convincing that health status at the time of birth impacts positively on educational attainment. How does this effect operate? Does fetal distress permanently damage cognitive functioning, which interferes with knowledge acquisition and skills development throughout school? Or do children who are frail at birth subsequently develop health conditions and illnesses at preschool ages that delay development and place the child at a disadvantage throughout his or her schooling? Or do health problems in the preschool and early school years lead to additional health problems in later school life at ages when qualifications must be obtained? Currie et al. (2010) are able to address these types of questions by using rich Canadian data following children from birth into young adulthood. Controlling for sibling fixed effects, birth weight, and congenital and perinatal abnormalities, which always have effects, major physical health conditions and injuries in the preschool (0-3) and early school (4-8) years impact on educational attainment only because they raise the probability of experiencing similar conditions in later school years. The process is different with respect to mental health conditions. Behavioral problems at all ages, including the preschool years, directly reduce educational attainment. From this and other evidence, Almond and Currie (2012) conclude that there is an important effect of early-life health on human-capital acquisition and later-life outcomes. Exposure to adverse conditions in utero appears to exert a stronger effect than postnatal health, although mental health conditions identified in the preschool years have lasting effects.
Besides a technological effect of childhood ill-health on the acquisition of education, if the reduction in health is permanent, then there may be an incentive effect operating through life expectancy. A longer life may raise education by lengthening the period over which the return on this investment can be reaped (Ben-Porath, 1967). This further strengthens the extent to which dispersion in health implies dispersion in earnings potential. There is an inequality increasing concentration of health and human capital in the same individuals.
17.3.4.3 Fetal Origins Hypothesis
Early-life health potentially determines later-life economic outcomes not only via education and skills acquisition but more directly through health problems that interfere with productive work in adulthood. The fetal origins hypothesis, proposed by David Barker, is that chronic diseases, principally coronary heart diseases but also related diseases such as type 2 diabetes, originate in nutritional deprivation in gestation and infancy (Barker, 1992, 1995; Barker et al., 1993). Nutrition-induced stresses placed on the fetus at critical stages of development alter the physiology of vital organs, particularly the heart, which makes them susceptible to failure in middle and old age, inducing the onset of chronic disease.[79] Metabolism can also be detrimentally affected by in utero nutritional deprivation such that the risk of obesity is raised.
One cause of fetal stress that has been exploited to estimate long-term economic effects is in utero exposure to the 1918-1919 Spanish flu (Almond, 2006), which has been shown to increase the incidence of stroke, diabetes, and hearing, seeing, and mobility impairments (Almond and Mazumder, 2005), as well as cardiovascular disease (Mazumder et al., 2010). As is clear from the evidence reviewed in Section 17.3.3.5, chronic illnesses such as these have negative impacts on employment and earnings. Economic consequences of the fetal origins hypothesis are a topic that is increasingly receiving attention (Almond and Currie, 2011, 2012; Currie, 2009). We discuss some of the evidence in Section 17.3.4.4.
26
17.3.4.4 Economic Consequences of Early-Life Ill-Health
The previous three subsections establish that ill-health in early life and childhood constrains the acquisition of nonhealth human capital and directly impinges on adult health. With these disadvantages, one expects adults who were sick, or exposed to health risks as infants and children to be less well-off.What is the evidence that frailty of health at the beginning of life leads to economic disadvantage later in life?
Analyses of the 1958 British birth cohort establish that low birth weight is not only associated with lower educational attainment but also with lower employment, greater likelihood of being engaged in manual labor, and lower wages (Case et al., 2005; Currie and Hyson, 1999). Sibling and twin fixed effects studies produce evidence that lower birth weight reduces wages in Minnesota (Behrman and Rosenzweig, 2004) and reduces employment and earnings in the USA (Johnson and Schoeni, 2011).[80] It also reduces earnings (but not employment) in Norway (Black et al., 20 07).[81] In addition, low birth weight increases welfare dependency in Canada (Currie et al., 2010; Oreopoulos et al., 2008) and may (Currie and Moretti, 2007) or may not (Royer, 2009) increase the likelihood of living in a poor neighborhood of California.
Johnson and Schoeni (2011) find that only around 10% of the effect of low birth weight on earnings operates through years of schooling.[82] The fact that most of the health effect does not operate via human capital is consistent with the findings of other studies (Luo and Waite, 2005; Persico et al., 2004; Smith, 2009). Using the 1970 British Cohort Study, Conti et al. (2010a,b) do not find any selection into postcompulsory schooling on the basis of child health for males and only a weak effect for females, although there is very strong selection on cognitive and noncognitive skills. There is a direct effect of child health on wages for males, but the weak wage effect for females does run via education.
The health measures employed by Conti et al. are height and head circumference at age 10. Although these measures should pick up nutritional deprivation at early ages, they will miss many other child health conditions. Estimating the long-term economic impact of child health, more generally defined, is made difficult by the scarcity of suitable longitudinal data and the challenge of measuring the general health status of children. Using the US PSID, Smith (2009) estimates that an adult retrospectively reporting excellent or very good health in childhood earns 24% more than his or her sibling who reports less than good health in childhood. There are no differences in education, so again most of the effect, if we are prepared to label the earnings difference as such, does not appear to operate through human capital.
In an intriguing paper, Almond (2006) finds dramatic effects of in utero exposure to the 1919 Spanish flu on economic outcomes. Earnings of male workers were reduced by 5-9%. Applying standard estimates of the return to education to the impact on schooling (length reduced by 5 months, on average, and high school graduation probability down by 13-15%), the indirect effect through education explains around one-half of the earnings effect. So, although there is support for the pathways model of life course epidemiology that proposes that the infant health effect operates (partly) through education (Hertzman et al., 2001; Kuh et al., 2003), this does not tell the full story. There appears to be a substantial direct effect of fetal conditions on earnings.
Welfare payments, which include DI, are higher for those exposed to the flu. There is also evidence of a substantial effect through occupation. For men, exposure results in a drop of around 6% on a hierarchical index of occupational status. Total income is reduced by about 6.4% for men, and the probability ofbeing poor is increased by as much as 15% points.[83] Identification of these effects from prebirth conditions cuts through the endogeneity problems that plague the evidence on the economic consequences of ill-health reviewed in Section 17.3.3.5. The limitation is that the link between health and economic outcomes is less transparent. The identification requires a leap of faith that it is the Spanish flu and not some other peculiarity of the 1919 birth cohort that is responsible for the effects.[84]
Subject to this caveat, this study has important implications for the interpretation of income distribution and its association with health. Sizable differences in incomes, and in its education and occupation determinants, appear to be attributable to differences in health conditions at the very beginning of life. Policies that can improve the early-life conditions of the most vulnerable infants can potentially compress the distribution of income decades later by ensuring that there are fewer physically frail individuals who can become the most economically deprived. Almond (2006) draws attention to the tremendous racial disparity in early-life conditions in the USA, where nonwhites are exposed to twice the infant mortality rate of whites. His estimates suggest that this health inequality may not only be a consequence of current economic inequality but also a potentially important cause of future economic inequality.
Overall, the evidence points to the health environment in which a child is conceived and delivered exerting a lifelong effect on economic opportunities. Currie (2009) notes that it is difficult to gauge the magnitude of the effect, given the variety of health risks and measures that have been employed by researchers and the differing study contexts. However, the evidence would seem sufficient to conclude that it is not a negligible effect. A further tentative conclusion is that the effect of health risks in infanthood on economic outcomes, via adult health, is stronger than the effect that operates via educational attainment. This is sometimes claimed as support for the fetal origins hypothesis. Strictly, it is not. The hypothesis claims a direct causal link between fetal health and the onset of chronic disease in middle age. Yet, a number of the studies purported to find evidence consistent with the hypothesis examine younger adults, and the health measures used often do not identify the cardiovascular conditions that are triggered by fetal stress according to the theory. Adult health can also be related to health conditions in childhood because illness is persistent and cumulative, which is a feature of the accumulation model of epidemiology (Kuh et al., 2003; Riley, 1989).
It is safe to conclude that health in early life is relevant to economic circumstances in adult life. Establishing precisely why and to what extent is a challenging research agenda to be tackled by both economists and epidemiologists.
17.3.5 HealthandOccupation
The life course model identifies entry into the labor market as an important stage at which the relationship between health and SES is strengthened (Kuh and Wadsworth, 1993). Frail young adults face a narrower choice of entry-level jobs both because their education has been constrained by ill-health and because persistent health conditions directly impede productivity or provoke discrimination. The evidence reviewed in the previous section suggests that the direct productivity effect is stronger than the education effect. The income gradient in health may then partly reflect selection of the less healthy into lower-paid jobs, as well as sickness impeding movement up the career ladder.
This mechanism has been the focus of the epidemiological literature that has considered the extent to which causality runs from health to SES. The literature generally concludes that health-related occupation selection and social mobility are of insufficient magnitudes to make important contributions to the observed socioeconomic gradient in health (Chandola et al., 2003; Power et al., 1996, 1998). In this literature, SES is typically measured by occupation, social class, or employment grade. What is found is that, althoughjob changes are related to health, movements of the more healthy into “better jobs” are insufficient to explain the observed health disparity across the occupational hierarchy (Chandola et al., 2003). The same need not follow with respect to the explanation of health differences across more economic dimensions of SES, such as earnings or income (Adda et al., 2003). As is hopefully clear by now, ill-health can impact on income through many channels other than occupation, and thus, even if this is not an important mechanism, it certainly does not follow that the income (rather than the occupation) gradient in health is mainly attributable to causality from income to health, rather than vice versa. Researchers from the economics discipline are generally more sympathetic to the selection hypothesis (Deaton, 2002, forthcoming; Smith, 2004). In particular, they recognize and emphasize the potential evolution of an individual’s career and health based on his early-life health and other experiences, as discussed in the previous section (Case and Paxson, 2011).
The health-related selection of occupation need not necessarily steepen the income gradient in health. If productivity varies with health, and productivity is unobservable, then wages will vary with health only if the latter is observable (Strauss and Thomas, 1998). Ifhealth is not observable, then the healthy would be expected to sort into occupations in which productivity is less difficult to observe. Particularly in low-income countries, the healthy may stick to self-employment in which there is no issue of productivity verification and earnings are not set at some average over higher and lower levels of productivity. But such occupations may offer lower earnings potential, perhaps because there is less capital per unit of labor. Wage differences by health would be more compressed than in a situation in which there was no sorting.
The evidence reviewed in Section 17.3.2.4 generally provides estimates of the impact of health on the wage rate conditional on occupation. But there could be an additional effect on earnings through occupation itself. The evidence on job change after the onset of a health condition is relatively sparse. Now rather old data reveal that around one quarter of males and one-fifth of females in the USA with a work-limiting health problem report having moved to jobs more compatible with their conditions (Daly and Bound, 1996). Older workers and high school dropouts are less likely to change jobs. Charles (2003) argues that older workers are less likely to retrain for the purpose of accommodating a disability, because they have less time remaining to reap a return on this investment. He finds evidence consistent with this hypothesis in the US PSID. The low-educated may be less likely to adapt because they lack the general human capital that raises the efficiency of specific investments. It is more difficult to move from manual to nonmanual labor if basic reading and writing skills are lacking. This may partly explain why lower-educated, lower-skilled, and lower-paid workers are more likely to exit the labor force when struck down by a disability (Banks, 2006; Garcia Gomez et al., 2013; Halla and Zweimuller, 2013) and, in the USA, are less likely to recover earnings lost after the initial onset of a disability (Charles, 2003).
17.3.6 Health and Household Income
The impact of health on the distribution of household incomes may differ from that on the distribution of individual incomes for two principal reasons. First, health may affect the formation and dissolution of households. Second, the illness of one household member may provoke a response from the labor supply of others.
Poor health may make it more difficult to find a partner. Limitations in functioning, caring needs, and reduced expected longevity may make a disabled or chronically ill person a less attractive proposition in what some economists refer to as the marriage market. On top of the direct effect, there may be a reinforcing indirect effect operating through the impact of health on human-capital accumulation and earnings potential; marrying a sicker person, on average, means marrying a poorer person. The marriage vows of “in sickness and in health” appear to recognize the threat that illness poses to marriage. Ifless healthy people do have fewer opportunities to find and keep a partner, then one would expect that there will be health-related sorting. Then lower than average earnings of a disabled or sickly person will be compounded, not compensated, by the earnings of his or her spouse.
Although the idea that health influences marriage prospects has been around for some time (Carter and Glick, 1976; Sheps, 1961), there is little convincing evidence with which to judge its empirical validity. In part, this is because of the difficulty of separating healthy selection into marriage from the potentially beneficial effect of marriage on health (Goldman, 1993). Longitudinal data are required. Fu and Goldman (1994) find little evidence that health predicts the marriage behavior of young American adults. For US women there is evidence of health selection, however. Among young women not in full-time employment, those in better health are more likely to marry and less likely to break up (Waldron et al., 1996), and in a Californian sample of siblings, the sister with the lower birth weight is 3% points less likely to be married when she gives birth (Currie and Moretti, 2007).
Recognition of potential health gains from marriage introduces the possibility that there is negative health selection into the institution. The less healthy have more to gain frommarriage. LillardandPanis (1996) find evidence of such adverse selection among US men; the less healthy (re)marry sooner and remain married for longer. However, there is also selection on unobservables correlated with good health, and this dominates so that married men are healthier than their unmarried counterparts.
Within a household, ill-health of one partner could provoke two conflicting motivations for labor market activity of the other partner. On the one hand, reduced earnings of the disabled partner will generate an income effect that will motivate the spouse to replace those lost earnings through increased work effort. This is the added worker effect that is familiar in the unemployment literature. On the other hand, the disabled person’s productivity may be reduced not only in the labor market, but also within the household. Limitations in functioning may reduce capacity to wash, dress, and feed oneself.Meeting these caring needs will place demands on the spouse’s time. A priori, one cannot say which effect will dominate.
There appears to be a gender difference in the relative magnitude of the two effects, but the direction of this bias is not always consistent. Most US evidence finds that women are more likely to participate in employment when their husbands fall ill, but, if anything, male spouses are less likely to participate (Berger, 1983; Berger and Fleisher, 1984; Charles, 1999; Van Houtven and Coe, 2010). Coile (2004) finds no effect on the female spouse and only a small increase in the employment of men whose wives fall ill, however. The employment response of the spouse has also been found to depend on the type of health condition and the initial labor supply of the spouse (Blau and Riphahn, 1999; Siegel, 2006).
There is evidence from Germany (Riphan, 1999), Spain (Garcia Gomez and Lopez- Nicolas, 2006), and the Netherlands (Garcia Gomez et al., 2013) that ill-health reduces household income by more than the fall in the personal income of the person experiencing the health shock. For example, the Dutch study finds that an acute hospital admission reduces household income by 50% more than the reduction in income of the person admitted to hospital.
17.3.7 HealthandWealth
The impact of health on economic inequality may go beyond wage and income distributions to wealth distribution.[85] If ill-health reduces income through one or more of the mechanisms identified in the previous subsections, then opportunities to accumulate wealth over a lifetime will be constrained. Because the effect is accumulated, permanent differences in health will create greater variance in wealth than in income. In addition, ill- health may force depletion of wealth to pay for medical or nursing care. Less obviously, health may affect wealth through life expectancy and consequent saving incentives. The horizon and uncertainty effects of increased longevity both raise saving, while they have contradictory effects on labor supply (see Section 17.3.3.4). Those expecting to live for longer will accumulate more wealth both to provide for an extended old age and because they face a lower risk of dying before having the opportunity to enjoy their savings.
Consistent with these mechanisms, the relationship between health and wealth is particularly strong. PSID data reveal that the median wealth in 1994 of a household whose head was in excellent health 10 years earlier was 268% greater than the median wealth of a household whose head had been in poor health (Smith, 1999). This wealth inequality grew both with the lapse of time since the difference in heath was recorded and with age, consistent with differential rates of wealth accumulation by health. A number of US studies have examined whether the strong positive relationship between health and wealth is due to causality from health to wealth, causality from wealth to health, or simply a spurious correlation.
The much-cited paper by Adams et al. (2003) analyzes panel data on a sample of the US population aged 70+ (Asset and Health Dynamics among the Oldest Old— AHEAD). Their focus on the elderly eliminates differential earnings as a mechanism through which health may contribute to differences in wealth accumulation. The null of no causation from both current and previous health, indicated by 19 conditions and SAH, to the change in wealth is rejected.[86] The authors’ rigorous analysis leads them to emphasize that, although the result is consistent with a causal effect from health to wealth, they cannot rule out the possibility that it reflects model misspecification and/ or time-invariant unobservable factors driving the evolution of both health and wealth.
Michaud and van Soest (2008) overcome both limitations and provide even more conclusive evidence of a causal effect from health to wealth. They use the HRS and allow for causality operating contemporaneously and with lags in both directions, along with unobservable heterogeneity. Health is measured by an index constructed from principal components analysis of SAH, major and minor conditions, ADL, depression score, and body mass index. The health of both the husband and the wife are found to impact on household wealth. The effect of the wife’s health is immediate, but that of the husband’s health is delayed.[87] This assumption is due to a gender difference in the type of ill-health that impacts on wealth. Forboth sexes there is a delayed impact of physical ill-health. But only the mental health of females has an impact on wealth that is immediate. Evidence of the causal impact of health on wealth is stronger for households that lack health insurance coverage, particularly those in which the wife succumbs to mental ill-health, suggesting that depletion of assets to pay for medical care is an important part of the effect.
Although the Michaud and van Soest study gives us good reason to believe that there is an effect of health on wealth, at least in the older US population, its use of a health index has the disadvantage of not producing an estimate of easily interpretable magnitude. Without allowing for unobservables that condition the evolution of both health and wealth, Smith (2004) estimates, using HRS data, that the income loss, medical expenses, and consequent forgoing of interest arising from the onset of a major health condition (see Section 17.3.3.5) accumulate over 8 years to an average loss of wealth of almost $50,000. Most of this lost wealth is due to reduced earnings. Consequently, the wealth loss is considerably lower ($11,350) for the older AHEAD cohort analyzed by Adams et al. The wealth loss resulting from the onset of a minor health condition is also much smaller ($11,500). Recognizing that one-fifth of Americans aged 50+ experience the onset of a major health condition over an 8-year period and a further 30% incur a minor condition, Smith argues that the consequent wealth losses represent substantial effects of health on the distribution of wealth. Consistent with Michaud and van Soest (2008), the magnitude of the effect that does not operate though earnings losses is larger when the wife experiences the illness (Wu, 2003). This effect relationship is explained by assets being run down to pay for general living expenses when the wife is no longer fit to perform household chores. Accordingly, it is not observed when the husband’s health deteriorates.
Overall, the evidence is convincing that health constrains the accumulation of wealth, and illness speeds its depletion. The magnitude of the effect is likely to differ with the nature of the health condition and the means of financing both pensions and medical care.[88] [89] In the USA, for which most evidence is available, the effect seems substantial. Variation in both health levels and rates of health depreciation with age may make substantial contributions to interhousehold inequality in wealth holdings. 17.3.8 Summary Understanding the effects of health on income and wealth is important for the explanation of distributions of income and wealth and the interpretation of the economic gradient in health. We have identified a number of pathways through which health potentially impacts income and wealth, and the evidence suggests that many of these are empirically important. Ill-health can lead to a fall in wages at the margin, but wages are more likely to drop through job changes. In high-income economies, policies that constrain wage flexibility, such as effective minimum wage laws and antidiscrimination legislation, which has been strengthened considerably in relation to disability in Europe and the USA from the 1990s onward, can limit the downward pressure on wages, but this effect often comes at the cost of reducing employment opportunities for disabled individuals. Legislation frequently obligates employers to adapt workplace and employment conditions to accommodate disabled workers, and the responses of employers may vary across sectors and occupations. Changes toward a more disability-friendly workplace are evident to those of us working in white collar and professional occupations. Employers faced with difficulties in recruiting skilled workers may offer an accommodating work environment and flexible hours to secure a competitive advantage. In lower-paid sectors, employment decisions have become more short-term, however, and firms may be even less willing to invest in accommodating low-skilled workers with health problems. Although we are not aware of any evidence of such a heterogeneous employer response, it is a hypothesis worthy of investigation, not least because it implies that increasing general labor market inequality would generate an even greater increase in inequality between disabled workers with different skill sets. Policy further conditions the labor market response to ill-health through DI, which protects incomes but increases the impact on employment through a sizable incentive effect. From the perspective of public finances, the moral hazard of DI is a legitimate and substantial concern. However, the increased responsiveness of employment to ill- health does not necessarily imply welfare loss. For individuals suffering health conditions that make work extremely uncomfortable, DI may, indeed should, allow these workers to withdraw from the labor force. In lower-income economies with less social protection, ill-health may have a smaller impact on employment, and perhaps even on money income, but it could contribute more to inequality in well-being, because the necessity to continue working with a disability reduces worker utility, both immediately through the discomfort of work and in the long term through reduced health. This point serves as a reminder that, although the focus of this chapter is on the relationship between two central dimensions of well-being, income and health, we are ultimately interested in the implications of this relationship for the distribution of well-being itself. The impact of ill-health on household income can be substantially larger than that on the earnings of the disabled person, because of a spillover effect on the labor supply of the spouse. In addition, illness may reduce the likelihood of forming and maintaining marriage partnerships, although the evidence on this point is mixed. Through these two mechanisms, the contribution of ill-health to inequality in household incomes need not be less and may even be greater than its contribution to inequality in personal incomes. Beyond DI, policy can attenuate the contribution of ill-health to inequality in household disposable incomes through the tax and benefit system. High marginal tax rates, resulting from tax credits and other income-tested transfers, will moderate any increased inequality in gross household earnings arising from the distribution of health. Perhaps the most important conclusion emerging from the literature, and emphasized by others (Almond and Currie, 2012; Currie, 2009; Heckman, 2007), is that ill-health can have a very long reach from exposure to health risks in childhood to constrained economic opportunities in adulthood. By constraining human-capital acquisition through education and skills formation, as well as persistent and delayed effects on health in adulthood, early-life and childhood health experiences can be important determinants of both income distribution and the observed income gradient in adult health. A good deal of evidence supports the mechanisms through which health may impact income and wealth, but inferring the magnitude of each effect is far from easy. This is because, even with respect to a particular mechanism, there is not a single effect but many. Health is not unidimensional. Different dimensions of health will impact income and wealth through different routes and to different degrees. Using a general measure of health, such as self-assessed health, may provide some average effect over different types of health problems, but the usefulness of this average is questionable. Relatedly, measurement error in health variables has been a substantial obstacle to obtaining credible estimates of health on labor market outcomes. But this problem is receding. Longitudinal surveys, such as the HRS and its equivalents, increasingly contain detailed measures of specific health conditions, allowing researchers to exploit the timing of illness onset in order to identify the economic consequences of intrinsically interesting changes in health with precise medical meanings. Also promising is the increasing access of researchers to linked administrative registers on hospital admissions, social insurance, and tax files, which drastically reduce measurement error and provide very large samples from which the effects of specific medical conditions can be identified. Ill-health reduces income and wealth. The contribution of health to economic inequality depends upon how it is distributed. If health variation is random, then it adds to the dispersion of income (wealth). In this case, the additional economic inequality may not be considered socially objectionable. Losing income as a consequence of illness may be seen as unlucky but not unjust, and insurance may be called for on grounds of efficiency. The consequences for economic inequality—both the nature of the impact and its normative interpretation—are quite different if ill-health is not distributed by the roll of the dice, however. The next section examines whether income and wealth exert causal effects on health. Irrespective of whether such effects exist, if individuals with lower potential incomes are more likely to fall sick, then the income distribution is skewed even more to the disadvantage of the poor. For example, assume that low education both reduces income and increases the likelihood of sickness. The poor are more likely to get sick, and because they are sick, they become even poorer. The income distribution gets stretched by the unequal incidence of illness and its impact on income. Economic inequality is generated by biases that place the socially underprivileged at a health disadvantage and then impose an economic penalty for this status. Thus, inequality is more likely to be considered morally objectionable than it would be if it arose from even-handed luck in the distribution of illness. In addition to the uneven incidence of illness, the effect of health on economic inequality is likely exacerbated by heterogeneity in the impact of health on income across the income distribution. The employment and earnings of low-skilled, low-paid workers is more contingent on their health than is the case for higher-paid professionals. Not only do the socially disadvantaged face a higher incidence of illness, but they are also more economically vulnerable to it. DI provides a safety net, but its disincentive effects are stronger for the low-paid, and they are more responsive to these incentives, because labor market opportunities have been deteriorating for this group since the 1980s. As a result, the loss of employment following ill-health is both a contributor to economic inequality and a consequence of it. We conjecture that ill-health contributes to economic inequality not merely by adding noise to the distribution of income (wealth) but by further reducing the incomes (wealth) of those who would be located toward the bottom of the distribution in any case. This could occur even without low income or wealth reducing health. We now turn to the question of whether there is a causal effect from the economic to the health domain of well-being. 17.4.
More on the topic HEALTH DETERMINATION OF ECONOMIC INEQUALITY:
- HEALTH DETERMINATION OF ECONOMIC INEQUALITY
- ECONOMIC DETERMINATION OF HEALTH INEQUALITY
- Atkinson Anthony, Bourguignon François. Handbook of Income Distribution. Volume 2B. North Holland, 2014. — 2366 p.,
- INTRODUCTION
- INEQUALITY OF OPPORTUNITY: MEASUREMENT ISSUES AND EMPIRICAL RESULTS
- Socioeonomic polarization
- Inequality, Credit Market Imperfections and Human Capital
- THE APPLICABILITY OF THE INSTITUTIONAL APPROACH
- The Motivations for Social Ownership
- PREPARING THE GROUND FOR EMPIRICAL ANALYSIS